
Vocal Fold Motion Impairment in Neurodegenerative Diseases
by
 , , ,
, , ,
Rumi Ueha
1,2,* ,
,
Cathrine Miura
2,
Naoyuki Matsumoto
2,
Taku Sato
2,
Takao Goto
2 and
Kenji Kondo
2 1
Swallowing Center, The University of Tokyo Hospital, Tokyo 113-8655, Japan
2
Department of Otolaryngology and Head and Neck Surgery, Faculty of Medicine, The University of Tokyo, Tokyo 113-8655, Japan
*
Author to whom correspondence should be addressed.
J. Clin. Med. 2024, 13(9), 2507; https://doi.org/10.3390/jcm13092507
Submission received: 30 March 2024
/
Revised: 20 April 2024
/
Accepted: 24 April 2024
/
Published: 24 April 2024
(This article belongs to the Special Issue Review Special Issue Series: Current Advances in Clinical Neurology)
Abstract
:Vocal fold motion impairment (VFMI) is the inappropriate movement of the vocal folds during respiration, leading to vocal fold adduction and/or abduction problems and causing respiratory and vocal impairments. Neurodegenerative diseases (NDDs) are a wide range of disorders characterized by progressive loss of neurons and deposition of altered proteins in the brain and peripheral organs. VFMI may be unrecognized in patients with NDDs. VFMI in NDDs is caused by the following: laryngeal muscle weakness due to muscular atrophy, caused by brainstem and motor neuron degeneration in amyotrophic lateral sclerosis; hyperactivity of laryngeal adductors in Parkinson’s disease; and varying degrees of laryngeal adductor hypertonia and abductor paralysis in multiple system atrophy. Management of VFMI depends on whether there is a presence of glottic insufficiency or insufficient glottic opening with/without severe dysphagia. VFMI treatment options for glottic insufficiency range from surgical interventions, including injection laryngoplasty and medialization thyroplasty, to behavioral therapies; for insufficient glottic opening, various options are available based on the severity and underlying cause of the condition, including continuous positive airway pressure therapy, botulinum toxin injection, tracheostomy, vocal fold surgery, or a combination of interventions. In this review, we outline the mechanisms, clinical features, and management of VFMI in NDDs and provide a guide for physicians who may encounter these clinical features in their patients. NDDs are always progressive; hence, timely evaluation, proper diagnosis, and appropriate management of the patient will greatly affect their vocal, respiratory, and swallowing functions as well as their quality of life.
1. Introduction
Neurodegenerative diseases (NDDs) encompass a wide range of disorders characterized by progressive loss of neurons and deposition of altered proteins in the brain and peripheral organs [1,2]. These conditions tend to develop slowly, with symptoms becoming evident in the later stages of life. NDDs can manifest with a range of symptoms, including memory loss, abnormal movements, balance impairments, and swallowing difficulties, as well as potential complications such as voice and breathing disorders, which may emerge either at the onset or throughout disease progression [1,3].
Voice disorders can arise from various neurological conditions that affect the corticospinal pathway, cerebellum, basal ganglia, and upper and/or lower motor neurons [4]. A comprehensive examination of voice disorders in neurological diseases, emphasizing acoustic analysis, underscored the significant role of neurodegenerative diseases in affecting voice quality, especially in movement disorders such as Parkinson’s disease (PD), essential tremor, and spasmodic dysphonia [4,5].
Vocal fold motion impairment (VFMI) is also often encountered in NDDs [6,7,8,9]. VFMI is characterized by inappropriate movement of the vocal folds during breathing, leading to difficulties in vocal fold opening or closing. VFMI refers to a condition in which there is a disturbance in the movement of the vocal folds, but the terms vocal fold movement impairment [10], vocal cord (fold) paralysis [11,12], vocal cord (fold) dysfunction [13,14], and paradoxical vocal fold motion [15] are used as synonyms and analogues.
There are several reviews of voice disorders in NDDs but few reviews of VFMI in NDDs. Many physicians may have limited experience with NDDs and may be largely unaware of VFMI in these patients. Since VFMI related to NDDs is not widely recognized, even among otolaryngologists who assess vocal fold function, physicians may not readily attribute VFMI findings on endoscopic evaluation to NDDs as the underlying pathology. Recognizing VFMI as an early sign of NDDs may prompt otolaryngologists to expedite referrals to neurologists. In addition, if neurologists recognize hoarseness or respiratory difficulties in patients with NDDs, they should anticipate the potential for VFMI and encourage an early laryngeal assessment by otolaryngologists, particularly given the risk of respiratory deterioration.
To inform healthcare professionals about VFMI in patients with NDDs, we have compiled this review article. In this review article, we describe the clinical features and mechanisms of VFMI in NDDs and, additionally, provide insights into therapeutic approaches. Notably, we used the term vocal fold dysfunction to describe a condition in which the vocal folds move differently than expected, vocal fold dysmotility to describe a condition in which the vocal folds have reduced movement, and vocal fold immobility to describe a condition in which the vocal folds hardly move.
2. Diagnosis and Etiology of Vocal Fold Motion Impairment
Laryngological examination using a flexible laryngoscopy is an important tool for diagnosing VFMI, since it can visualize the vocal fold movement during breathing and phonation [16,17]. VFMI, including vocal fold immobility, vocal fold hypomobility, and vocal fold dysmotility, describes the qualitative findings of vocal fold motion without assuming a specific cause. These terms are preferred for describing physical exam results, especially through flexible laryngoscopy. The terms vocal fold paralysis and vocal fold paresis indicate a neurological cause for the abnormality seen during examination [16]. Laryngeal electromyography is a valuable tool in the evaluation and management of VFMI, providing prognostic information and guiding treatment decisions, as well as monitoring recovery in patients with VFMI. Laryngeal electromyography can differentiate between neuropathic patterns in the laryngeal muscles and other causes of vocal fold immobility, such as arytenoid dislocation [18,19,21]. Laryngeal ultrasonography can be a useful tool for screening and evaluating vocal fold motion impairment, but its accuracy is still debated compared to the standard of flexible laryngoscopy, especially in adult populations [20,22].
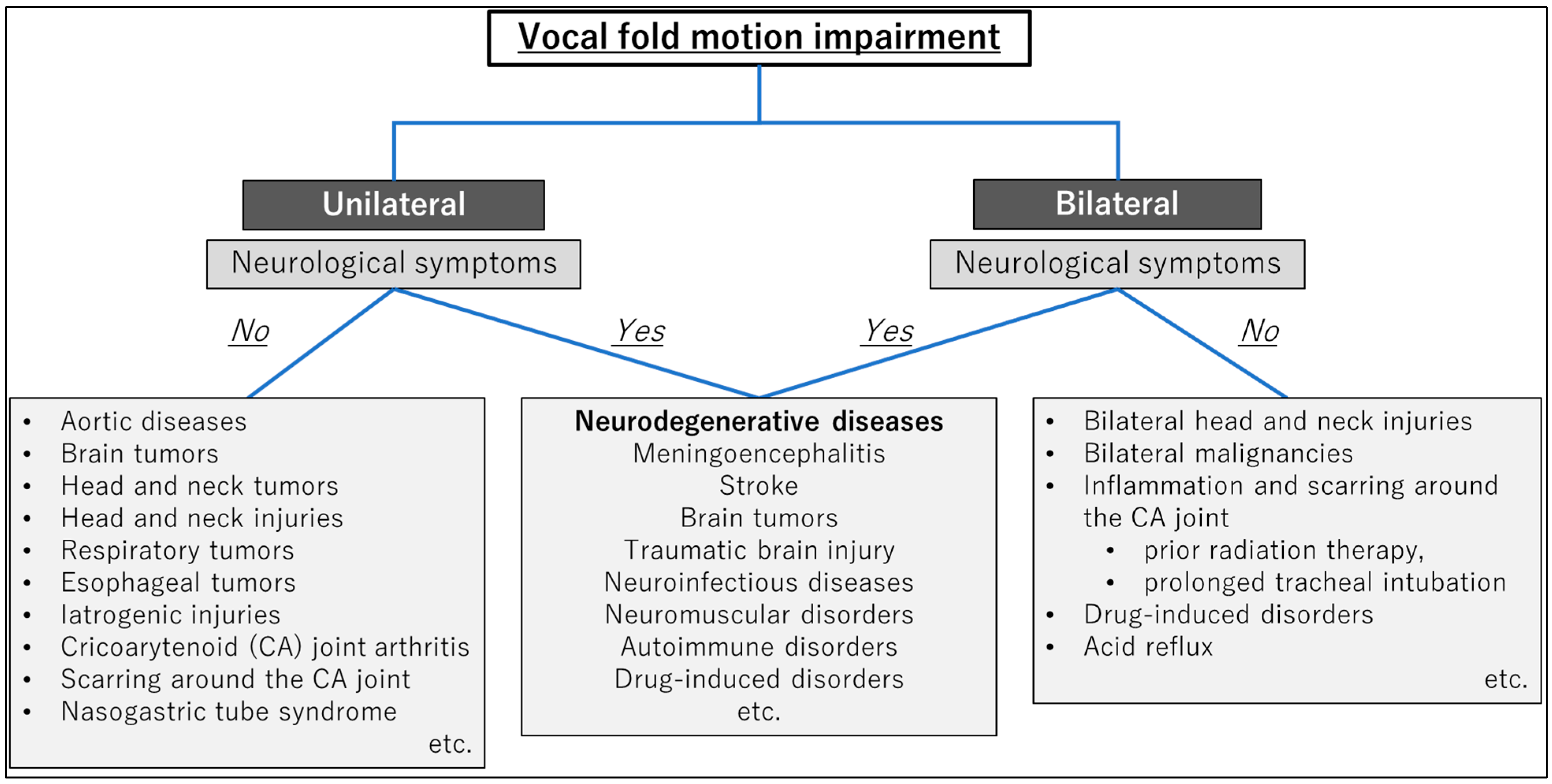
VFMI can occur in unilateral or bilateral vocal folds, and the etiology includes the following [23,24,25,26,27]:
- Neurological conditions;
- Malignancies;
- Mechanical/structural causes;
- Trauma;
- Iatrogenic injuries;
- Other potential causes.
The etiologies of VFMI are summarized in Figure 1. Neurological conditions like stroke, neurodegenerative diseases, and Guillain–Barré syndrome may result in VFMI [23]. Scarring or inflammation around the cricoarytenoid joint can cause mechanical vocal fold immobility [26]. Tumors or malignancies in the neck and laryngeal region can compress or infiltrate the nerves controlling the vocal folds [17]. VFMI can be triggered by factors like exercise, strong odors, acid reflux, and stress, though the underlying causes are not well understood [25].
3. Vocal Fold Motion Impairment in Neurodegenerative Diseases
NDDs are classified into the following categories based on their background mechanisms: dementia-type diseases, demyelinating diseases, parkinsonism-type diseases, motor neuron diseases, and prion diseases [2,3,28,29]. Dementia-type diseases include various disorders like Alzheimer’s disease, frontotemporal dementia, chronic traumatic encephalopathy, and dementia with Lewy bodies (DLB). This entails progressive deterioration in distinct brain regions, resulting in neuronal demise in multiple areas [3,30]. Demyelinating diseases are a group of neurological disorders characterized by damage or loss of the myelin sheath, which protects the surrounding nerve fibers in the central and peripheral nervous systems. Some demyelinating diseases, such as multiple sclerosis (MS) and neuromyelitis optica spectrum disorder (NMOSD), can be considered both demyelinating and neurodegenerative because of their impact on axons and neurons [31,32]. Parkinsonism-type diseases are a group of NDDs characterized by motor symptoms, such as bradykinesia, tremor, rigidity, and postural instability. Parkinsonism-type diseases include PD, DLB, progressive supranuclear palsy (PSP), and multiple system atrophy (MSA). Neuronal loss is associated with the accumulation of misfolded proteins, such as α-synuclein in PD and MSA and tau protein in PSP [33,34]. Motor neuron diseases are a subset of neurodegenerative disorders that primarily affect motor neurons and lead to progressive muscle weakness and atrophy. These include amyotrophic lateral sclerosis (ALS), spinal muscular atrophy (SMA), and primary lateral sclerosis (PLS). ALS is associated with the accumulation of the TDP-43 protein, whereas SMA stems from mutations in the survival motor neuron gene [35,36]. Prion diseases are caused by abnormal folding of prion proteins, which leads to extensive brain degeneration, including spongiform changes, neuronal loss, and accumulation of protein aggregates [37]. Prion diseases include Creutzfeldt–Jakob disease (CJD), Gerstmann–Sträussler–Scheinker syndrome, and kuru in humans, as well as scrapie in sheep and goats [38].
Among the NDDs, VFMI is frequently encountered in ALS, PD, MSA, PSP, and MS. Laryngoscopy can assess the movement and function of the vocal folds and identify abnormalities, such as incomplete glottic closure, vocal fold paralysis, or bowing of the vocal folds. Stroboscopy provides a detailed view of vocal fold vibration during phonation, helping to identify subtle abnormalities in vocal fold movement and closure. The following outlines the characteristics of VFMI under each condition.
3.1. Amyotrophic Lateral Sclerosis (ALS)
ALS is a neurodegenerative disease that affects motor neurons and leads to progressive muscle weakness and atrophy. Patients with ALS can experience various vocal fold abnormalities, including paradoxical adduction patterns, aperiodic vocal fold vibrations, hyperadduction of the ventricular folds, and hypoadduction of the vocal folds. These abnormalities can lead to symptoms of dysphonia, dysarthria, and dysphagia, which are prevalent in the bulbar form of ALS that primarily affects the brainstem and cranial nerves [39,40]. The exact pathophysiology of vocal fold dysmotility in ALS is not fully understood; however, it is thought to have multiple causes involving both infranuclear and supranuclear origins, resulting in the degeneration of the motor neurons that control the muscles of the larynx [41,42,43,44] (Figure 2).
Weakening of the upper airway muscles, including the vocal cord (fold) abductors, contributes to vocal fold movement impairment in ALS. VFMI in ALS can occur at any stage of the disease, and the symptoms range from hoarseness, hypophonia, and shortness of breath to acute dyspnea, laryngospasm, and stridor. Both unilateral and bilateral vocal cord (fold) dysfunction can manifest in ALS patients, contributing to a variety of laryngeal and respiratory symptoms. Involuntary vocal fold abduction dysfunction, including laryngospasm, can elicit dyspnea in ALS, with excessive saliva irritating the vocal folds, which is a commonly reported trigger [45].
Identification of these dysfunctions is important for the diagnosis and management of ALS, and comprehensive management strategies are essential to maintain quality of life, prevent complications, and improve patient outcomes [46]. When bilateral VFMI causes respiratory compromise in patients with ALS, tracheostomy to secure the airway should be considered, particularly when dysphagia is coexistent. However, because tracheostomy can impair patients’ swallowing function, continuous positive airway pressure or other measures are also an option, and shared decision making between the patients and medical professionals is performed to plan the best course of action.
3.2. Parkinson’s Disease (PD)
PD is characterized by neuromuscular impairments, including rigidity, tremor, and bradykinesia. Degeneration of the nucleus ambiguus, a region of the brainstem involved in motor control, may contribute to these symptoms. The pathogenesis of VFMI in PD is not completely understood, but it is thought to involve a combination of motor impairments, neuromuscular dysfunction, and degenerative changes in the brainstem nuclei responsible for laryngeal muscle control, which contribute to paralysis or weakness [47,48] (Figure 3).
In patients with PD, VFMI can manifest as hypophonia, monotone speech, vocal tremor, breathiness, and dysarthria [49]. In some cases, bilateral VFMI can occur. The prevalence of VFMI in patients with PD is relatively low compared with in that other neurodegenerative conditions [47]. However, bilateral VFMI, especially vocal fold abductor motion impairment, can be a life-threatening complication that may necessitate urgent interventions, such as tracheotomy or surgical treatments, to address airway obstruction [47,50]. Early recognition and appropriate management of VFMI in PD are important to improve voice quality, communication abilities, and overall quality of life for affected individuals.
3.3. Multiple System Atrophy (MSA)
MSA is a progressive neurodegenerative disorder characterized by autonomic dysfunction, parkinsonian disorder, and cerebellar dysfunction as the main symptoms. MSA is classified into parkinsonian (MSA-P) and cerebellar (MSA-C) variant types [9]. VFMI is a common issue in patients with MSA and is found in approximately half to two-thirds of the patients [9,51,52,53,54]. In particular, patients with MSA-P can develop VFMI earlier than patients with MSA-C because the spontaneous activity of intrinsic laryngeal muscles in patients with MSA-P can lead to an earlier onset of VFMI [9]. There are two plausible hypotheses for the pathophysiology of VFMI: (1) a severe loss of neurons in the nucleus ambiguus results in hypoactivity and neurogenic atrophy of the posterior cricoarytenoid muscle, which is the sole laryngeal abductor muscle, or (2) dystonia is induced by hyperactivity of the laryngeal adductor muscles [55,56] (Figure 3).
Patients with MSA often have sleep-related respiratory disorders, including high-pitched inspiratory stridor and sleep apnea. Upper airway obstruction can be caused by bilateral VFMI. VFMI is exacerbated during sleep, and airway narrowing can worsen [7]. Sudden death is frequently reported in patients with MSA, and VFMI is one of the most common causes of this [57]. In addition, diazepam should not be administered to patients with VFMI because it can aggravate glottic closure in patients with MSA [58]. The severity of VFMI impacts the overall survival of MSA patients, with unilateral or bilateral VFMI being statistically associated with decreased survival rates [9,59]. Therefore, early detection through laryngological assessment is crucial for managing VFMI in patients with MSA.
3.4. Progressive Supranuclear Palsy (PSP)
PSP is characterized by the gradual worsening of symptoms over time due to damage to certain brain areas, affecting functions such as walking, thinking, swallowing, and eye movements [60]. The exact cause of PSP has not been completely clarified, but it involves aggregation of tau proteins found in the brain, leading to neuronal damage [61]. This condition is often misdiagnosed as PD initially, but it progresses more rapidly than PD. The mechanism behind VFMI in PSP involves neurodegenerative processes that affect the central nervous system [62]. In patients with PSP, the development of bilateral VFMI is linked to the progression of the disease, leading to respiratory issues like inspiratory stridor. This dysmotility is a result of the neurodegenerative changes in the brain, particularly affecting areas involved in motor control and coordination [63]. In some instances, emergency tracheostomy is necessary to alleviate the respiratory symptoms associated with vocal fold paralysis in patients with PSP [64]. This highlights the importance of monitoring and managing VFMI in patients with PSP to prevent serious respiratory complications.
3.5. Multiple Sclerosis (MS)
MS is a neurological condition that can affect the nerves that innervate the laryngeal muscles, leading to VFMI [65,66,67]. This vocal fold dysmotility can result in difficulties in speech, breathing, and swallowing. The impact of multiple sclerosis on vocal fold paralysis emphasizes the intricate relationship between NDDs and laryngeal function.
4. Comparison of Patients with Vocal Fold Motion Impairment and PD or MSA
When comparing patients with VFMI and PD or MSA, VFMI is more frequently observed in MSA, and the irregular movement of the arytenoid cartilage may serve as a clinical marker to distinguish MSA from PD [8]. Airway narrowing due to VFMI is evidently more likely to occur in MSA [47]. In patients with MSA, the progression of VFMI and dysphagia was compared between patients with MSA-C and MSA-P. In MSA-C, worsening VFMI preceded the exacerbation of dysphagia, whereas, in MSA-P, severe dysphagia either preceded or occurred simultaneously with worsening VFMI [68]. Other differences in the clinical characteristics are summarized in Table 1. Compared with patients with PD, patients with MSA exhibited a longer duration from disease onset to VFMI, and their daily activities were more impaired at the onset of VFMI. At the onset of VFMI, dysphagia was notably severe in PD, while its severity varied among patients with MSA [47,68,69]. Inspiratory stridor was more prominent during the daytime in PD, while it predominated during sleep in MSA [47]. The effects of diazepam administration were entirely different between PD and MSA [58], and they also differed in their histological and laryngeal electromyographic findings [47,70].
5. Management and Treatment for Vocal Fold Motion Impairment
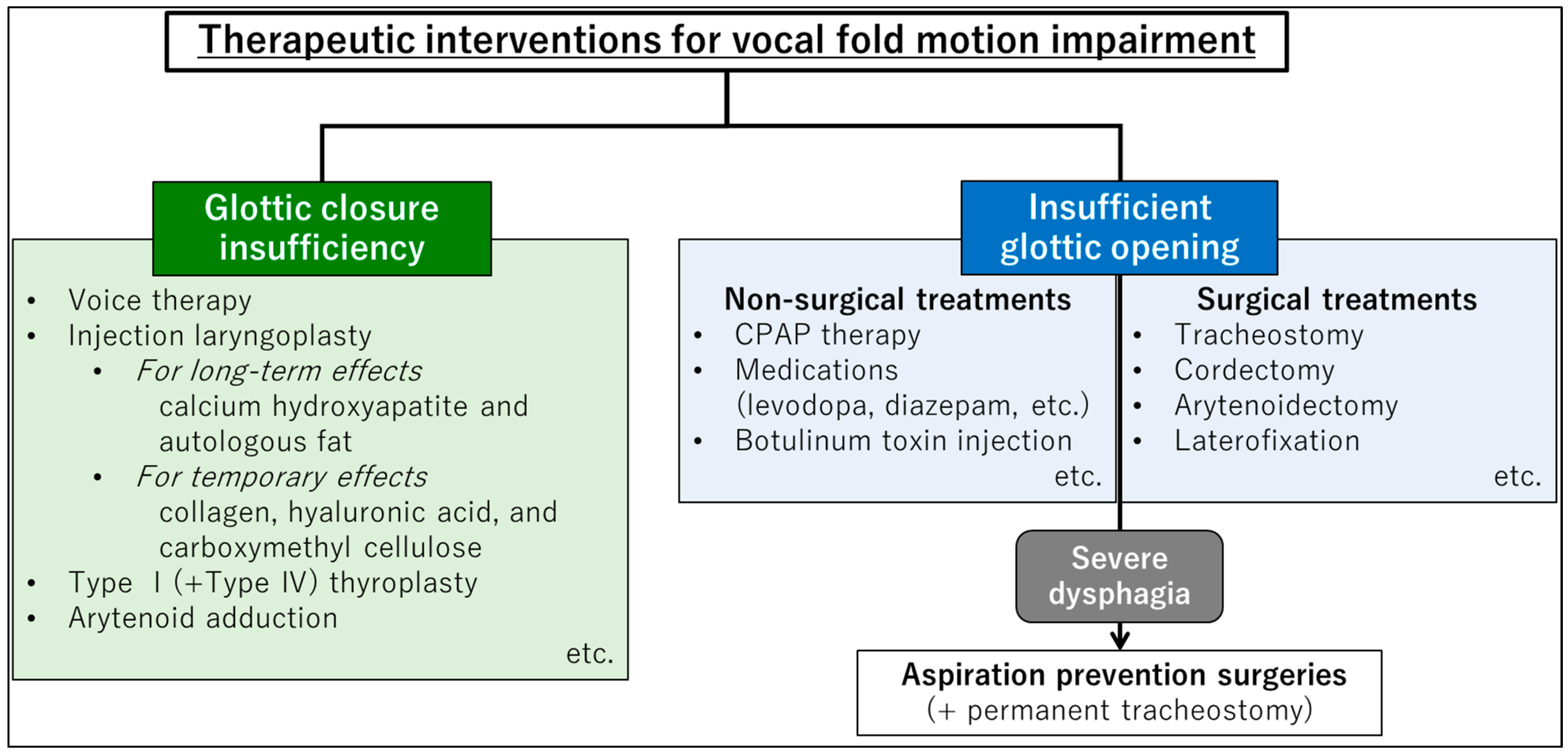
VFMI manifests with challenges in both glottal closure and opening, demanding distinct therapeutic strategies for each. Hereafter, we detail the therapeutic interventions targeting glottic closure insufficiency and insufficient glottic opening (Figure 4).
5.1. Treatments for Glottic Insufficiency
Treatment options for glottic insufficiency range from surgical interventions, including injection laryngoplasty and medialization thyroplasty, to behavioral therapies, such as voice therapy. These treatments aim to improve glottic closure to prevent aspiration and enhance vocal function.
Speech therapy, particularly techniques such as Lee Silverman Voice Treatment, can help improve vocal projection, intonation, and overall voice quality in patients with PD. This therapy focuses on increasing vocal loudness and clarity, enhancing communication skills, and addressing voice-related issues through one-on-one training sessions [78].
Injection laryngoplasty (augmentation laryngoplasty) is often helpful for hypoactive neurolaryngological disorders that result in glottal insufficiency and a weak voice. Injection laryngoplasty can be performed with a temporary injectable in an office setting that can address glottal closure, reduce glottal atrophy, and improve voice strength. Injectable materials are currently categorized as either temporary or long-term. Options for temporary materials include those derived from collagen, hyaluronic acid, and carboxymethyl cellulose, whereas calcium hydroxyapatite and autologous fat are available for long-term use. If temporary injection improves symptoms, longer term materials and more permanent interventions should be considered [79,80]. In cases of glottic insufficiency caused by unilateral vocal fold paralysis, surgical treatments using external approaches, such as type I (+IV) thyroplasty and arytenoid adduction, as well as injection laryngoplasty, are viable options [81]. Injection laryngoplasty is a minimally invasive procedure involving injections into the vocal folds under local anesthesia, whereas external approach surgeries are more invasive and permanent, suitable for cases wherein irreversible causes of severe glottal incompetence need to be addressed surgically [82].
5.2. Treatments for Insufficient Glottic Opening
Insufficient glottic opening refers to glottic narrowing due to vocal fold movement disorders such as bilateral vocal fold paralysis and bilateral abduction disorder. To treat insufficient glottic opening due to VFMI, various options are available based on the severity and underlying cause of the condition. Treatment approaches for managing VFMI in patients with NDDs include continuous positive airway pressure (CPAP) therapy, botulinum toxin (BTX) injection, tracheostomy, vocal fold surgery, or a combination of interventions can be considered [83,84]. If noninvasive interventions, such as drug therapy and CPAP, do not alleviate airway narrowing, surgical treatments should be performed.
CPAP has been shown to effectively manage glottic narrowing without surgical intervention in patients with bilateral vocal fold paralysis, particularly in patients with NDDs [83]. It involves wearing a mask over the nose and/or mouth, which delivers a continuous flow of air to keep the airway open and to prevent obstruction. CPAP reduces intratracheal negative pressure, thereby decreasing the transglottic pressure gradient through glottic stenosis during inspiration, reducing the likelihood of laryngeal adductor activation [8,85,86]. BTX injections can be used to temporarily weaken the function of the overactive vocal folds in cases of spasmodic dysphonia or adductor-type vocal fold paralysis. Although its effects diminish over the course of several months, BTX can improve airway narrowing and reduce the symptoms of dyspnea [87,88]. When glottic narrowing occurs in patients with PD due to VFMI, adjusting the dosage of levodopa may improve the symptoms [89].
Surgical treatments for insufficient glottic opening include various options aimed at improving airway patency. It should be noted that treatments to widen the glottis and secure the airway, other than tracheotomy, tend to worsen the quality of the voice because of glottic insufficiency after surgeries, and make the patient more susceptible to aspiration because the glottis does not close during swallowing.
- Tracheostomy is considered an essential intervention in managing bilateral VFMI, especially in situations where there is a risk of airway compromise due to the inability of the vocal folds to open properly during breathing. This surgical opening bypasses the narrowed portion of the airway, allowing for adequate breathing and preventing life-threatening obstruction of the airway [84,90].
- Arytenoidectomy is a surgical procedure in which the arytenoid cartilage, one of the cartilages in the larynx, is either completely or partially removed. This procedure is typically performed to address certain conditions affecting the larynx, such as insufficient glottic opening. However, this is not commonly performed on bilateral vocal folds because of the potential risks and impact on voice and swallowing functions [93,94].
- Laterofixation is a reversible method for the treatment of bilateral vocal fold paralysis in both adults and children. This procedure may be applied independently or in combination with other laryngeal microsurgery methods, unilaterally or bilaterally. Suture laterofixation is highlighted as an important option in the treatment of bilateral VFMI, and it avoids the long-term consequences of ablative procedures like arytenoidectomy [91,95,96].
5.3. Treatment for Insufficient Glottic Opening with Severe Dysphagia
When severe dysphagia is present, in addition to insufficient glottic opening, it is necessary to provide a means of nutrition (tube feeding, gastrostomy, etc.) as well as to secure the airway. Since tracheostomy worsens swallowing function, aspiration prevention surgery can be considered in patients with insufficient glottic opening and severe dysphagia. Although patients who undergo aspiration prevention surgeries eventually lose their vocal function, they are able to practice oral nutrition or oral intake by creating a structure preventing aspiration, which improves the patients’ quality of life [90,97,98,99,100].
6. Discussion
To inform healthcare professionals about VFMI in patients with NDDs, we have compiled this review article. Many physicians may have limited experience with NDDs and may be largely unaware of VFMI in these patients. Consequently, when examining patients who visit their clinic due to voice or respiratory problems, even if VFMI were found, physicians may not consider it as being related to NDDs. This review paper provides a comprehensive explanation of the pathophysiology and management of VFMI due to NDDs, offering advantages over previous literatures. Additionally, as clinically significant knowledge, it delineates differences in the management of VFMI between PD and MSA, which present similar findings.
When the vocal folds have trouble moving smoothly, voice, swallowing, and breathing are impaired, which not only reduces the patients’ quality of life, but can also be a critical and life-threatening issue. Patients with NDDs often experience progressive worsening of various symptoms over time and, aside from breakthrough molecular-targeted drugs, there are currently no viable drugs or therapies for alleviating these symptoms. Therefore, when VFMI is identified in a patient, it is essential to consider the progression of the disease and discuss appropriate measures to address it.
One must be aware that the management of bilateral severe VFMI in patients exhibiting parkinsonian symptoms is not the same for patients with PD and patients with MSA. In PD, airway narrowing is influenced by hyperactivity of the laryngeal adductor muscles and can be improved by the administration of diazepam, a drug that alleviates hypertonia. In contrast, in MSA, diazepam administration may worsen VFMI, resulting in the need for emergency measures for airway narrowing such as endotracheal tube insertion or tracheostomy.
In cases where VFMI (bilateral vocal fold abductor paralysis) induces airway narrowing, CPAP or tracheostomy may be necessary; nevertheless, neither CPAP nor tracheostomy can offer a permanent solution. Even when CPAP is used, the mask must be removed during meals, which may exacerbate respiratory disturbances during that time. Even if the airway is secured by tracheostomy, swallowing function may deteriorate with the placement of a tracheostomy tube. Consequently, if swallowing function is impaired, a tracheostomy tube for speaking cannot be utilized. In evaluating patients presenting with VFMI, it is important to account for the potential presence of underlying NDDs. Moreover, when addressing airway narrowing due to VFMI in patients with NDDs, it is appropriate to consider a broad perspective that encompasses not only current problem-solving but also future implications for vocal and swallowing functions, as well as the quality of life of patients. It is important to carefully consider the preferences of patients and their families when determining the appropriate course of action. Future studies are needed to evaluate the progression following treatment for VFMI in patients with NDDs. As for limitations, the details of the diagnostic and surgical procedures for VFMI were not included in this review article, and we refer the reader to more specialized books and articles for this information.
7. Conclusions
This review outlined the clinical examination approaches and management strategies for VFMI in patients with NDDs from the perspective of an otolaryngologist. To address VFMI in patients with NDDs, it is desirable to consider a broad perspective that encompasses future implications for vocal, respiratory, and swallowing functions, as well as patients’ quality of life. It is important to carefully consider the preferences of patients and their families while deliberating on the appropriate course of action.
Author Contributions
R.U.: developed the concept, collected the related papers, created all the figures and tables, and wrote the draft of the manuscript. C.M., N.M., T.S. and T.G.: collected the related papers and reviewed the manuscript. K.K.: reviewed the manuscript and provided appropriate advice on the content of the paper. All authors contributed to writing of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This study received no external funding.
Institutional Review Board Statement
The study protocol was approved by the Human Ethics Committee of the University of Tokyo (no. 2487, 2022179NI, 31 October 2022) and complied with the tenets of the amended Declaration of Helsinki.
Informed Consent Statement
Not applicable.
Data Availability Statement
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Checkoway, H.; Lundin, J.I.; Kelada, S.N. Neurodegenerative diseases. IARC Sci. Publ. 2011, 163, 407–419. [Google Scholar] [PubMed]
- Kovacs, G.G. Concepts and classification of neurodegenerative diseases. Handb. Clin. Neurol. 2017, 145, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Lamptey, R.N.L.; Chaulagain, B.; Trivedi, R.; Gothwal, A.; Layek, B.; Singh, J. A Review of the Common Neurodegenerative Disorders: Current Therapeutic Approaches and the Potential Role of Nanotherapeutics. Int. J. Mol. Sci. 2022, 23, 1851. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gamboa, J.; Jimenez-Jimenez, F.J.; Mate, M.A.; Cobeta, I. Voice disorders caused by neurological diseases. Rev. Neurol. 2001, 33, 153–168. [Google Scholar] [PubMed]
- Hecker, P.; Steckhan, N.; Eyben, F.; Schuller, B.W.; Arnrich, B. Voice Analysis for Neurological Disorder Recognition-A Systematic Review and Perspective on Emerging Trends. Front. Digit. Health 2022, 4, 842301. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kashima, H.K. Bilateral vocal fold motion impairment: Pathophysiology and management by transverse cordotomy. Ann. Otol. Rhinol. Laryngol. 1991, 100, 717–721. [Google Scholar] [CrossRef] [PubMed]
- Ueha, R.; Maeda, E.; Ino, K.; Shimizu, T.; Sato, T.; Goto, T.; Yamasoba, T. Sleep-Induced Glottis Closure in Multiple System Atrophy Evaluated by Four-Dimensional Computed Tomography. Front. Med. 2020, 7, 132. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gandor, F.; Vogel, A.; Claus, I.; Ahring, S.; Gruber, D.; Heinze, H.J.; Dziewas, R.; Ebersbach, G.; Warnecke, T. Laryngeal Movement Disorders in Multiple System Atrophy: A Diagnostic Biomarker? Mov. Disord. 2020, 35, 2174–2183. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tsuchiya, K.; Ueha, R.; Suzuki, S.; Goto, T.; Sato, T.; Nito, T.; Yamasoba, T. Heightened risk of early vocal fold motion impairment onset and dysphagia in the parkinsonian variant of multiple system atrophy: A comparative study. Clin. Park. Relat. Disord. 2020, 3, 100037. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kurita, S.; Hirano, M.; Matsuoka, H.; Tateishi, M.; Sato, K. A histopathological study of carcinoma of the larynx. Auris Nasus Larynx 1985, 12 (Suppl. S2), S172–S177. [Google Scholar] [CrossRef] [PubMed]
- Plasse, H.M.; Lieberman, A.N. Bilateral vocal cord paralysis in Parkinson’s disease. Arch. Otolaryngol. 1981, 107, 252–253. [Google Scholar] [CrossRef] [PubMed]
- Bawa, R.; Ramadan, H.H.; Wetmore, S.J. Bilateral vocal cord paralysis with Shy-Drager syndrome. Otolaryngol. Head Neck Surg. 1993, 109, 911–914. [Google Scholar] [CrossRef] [PubMed]
- Denipah, N.; Dominguez, C.M.; Kraai, E.P.; Kraai, T.L.; Leos, P.; Braude, D. Acute Management of Paradoxical Vocal Fold Motion (Vocal Cord Dysfunction). Ann. Emerg. Med. 2017, 69, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Alfonsi, E.; Terzaghi, M.; Cosentino, G.; Tassorelli, C.; Manni, R.; Pozzi, N.; De Icco, R.; Bertino, G.; Todisco, M.; Alvisi, E.; et al. Specific patterns of laryngeal electromyography during wakefulness are associated to sleep disordered breathing and nocturnal stridor in multiple system atrophy. Park. Relat. Disord. 2016, 31, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Hicks, M.; Brugman, S.M.; Katial, R. Vocal cord dysfunction/paradoxical vocal fold motion. Prim. Care 2008, 35, 81–103. [Google Scholar] [CrossRef] [PubMed]
- Rosen, C.A.; Mau, T.; Remacle, M.; Hess, M.; Eckel, H.E.; Young, V.N.; Hantzakos, A.; Yung, K.C.; Dikkers, F.G. Nomenclature proposal to describe vocal fold motion impairment. Eur. Arch. Otorhinolaryngol. 2016, 273, 1995–1999. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kandil, E.; Deniwar, A.; Noureldine, S.I.; Hammad, A.Y.; Mohamed, H.; Al-Qurayshi, Z.; Tufano, R.P. Assessment of Vocal Fold Function Using Transcutaneous Laryngeal Ultrasonography and Flexible Laryngoscopy. JAMA Otolaryngol. Head Neck Surg. 2016, 142, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.J.; Rosen, C.A.; Niyonkuru, C.; Munin, M.C. Quantitative electromyography improves prediction in vocal fold paralysis. Laryngoscope 2012, 122, 854–859. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.J.; Rosen, C.A.; Munin, M.C. Vocal fold motion outcome based on excellent prognosis with laryngeal electromyography. Laryngoscope 2016, 126, 2310–2314. [Google Scholar] [CrossRef] [PubMed]
- Nasser, H.M.; Askoura, A.; Hussein, A. Ultrasonography diagnostic validity in structural and functional laryngeal disorders. Egypt. J. Radiol. Nucl. Med. 2020, 51, 219. [Google Scholar] [CrossRef]
- Ho, G.Y.; Leonhard, M.; Volk, G.F.; Foerster, G.; Pototschnig, C.; Klinge, K.; Granitzka, T.; Zienau, A.K.; Schneider-Stickler, B. Inter-rater reliability of seven neurolaryngologists in laryngeal EMG signal interpretation. Eur. Arch. Otorhinolaryngol. 2019, 276, 2849–2856. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Izadi, S.; Zendejas, B.; Meisner, J.; Kamran, A.; Mohammed, S.; Demehri, F.; Staffa, S.; Zurakowski, D.; Hseu, A.; Cunningham, M.; et al. Diagnostic Accuracy of Laryngeal Ultrasound for Evaluating Vocal Fold Movement Impairment in Children. J. Pediatr. Surg. 2024, 59, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Zur, K.B. Vocal Fold Motion Impairment. Curr. Probl. Pediatr. Adolesc. Health Care 2018, 48, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Jabbour, J.; Martin, T.; Beste, D.; Robey, T. Pediatric vocal fold immobility: Natural history and the need for long-term follow-up. JAMA Otolaryngol. Head Neck Surg. 2014, 140, 428–433. [Google Scholar] [CrossRef] [PubMed]
- Malaty, J.; Wu, V. Vocal Cord Dysfunction: Rapid Evidence Review. Am. Fam. Physician 2021, 104, 471–475. [Google Scholar] [PubMed]
- Cohen, E.R.; Dable, C.L.; Iglesias, T.; Singh, E.; Ma, R.; Rosow, D.E. Clinical Predictors of Postintubation Bilateral Vocal Fold Immobility. Int. Arch. Otorhinolaryngol. 2022, 26, e524–e532. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lechien, J.R.; Hans, S.; Mau, T. Management of Bilateral Vocal Fold Paralysis: A Systematic Review. Otolaryngol. Head Neck Surg. 2024, 170, 724–735. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Rio, M.; Caballero, M.M.; Gorriz Saez, J.M.; Minguez-Castellanos, A. Diagnosis of Neurodegenerative Diseases: The Clinical Approach. Curr. Alzheimer Res. 2016, 13, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Logroscino, G.; Urso, D.; Savica, R. Descriptive Epidemiology of Neurodegenerative Diseases: What Are the Critical Questions? Neuroepidemiology 2022, 56, 309–318. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Walker, L.; McAleese, K.E.; Erskine, D.; Attems, J. Neurodegenerative Diseases and Ageing. Subcell. Biochem. 2019, 91, 75–106. [Google Scholar] [CrossRef] [PubMed]
- Sandi, D.; Fricska-Nagy, Z.; Bencsik, K.; Vecsei, L. Neurodegeneration in Multiple Sclerosis: Symptoms of Silent Progression, Biomarkers and Neuroprotective Therapy-Kynurenines Are Important Players. Molecules 2021, 26, 3423. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Huang, T.L.; Wang, J.K.; Chang, P.Y.; Hsu, Y.R.; Lin, C.H.; Lin, K.H.; Tsai, R.K. Neuromyelitis Optica Spectrum Disorder: From Basic Research to Clinical Perspectives. Int. J. Mol. Sci. 2022, 23, 7908. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Koziorowski, D.; Figura, M.; Milanowski, L.M.; Szlufik, S.; Alster, P.; Madetko, N.; Friedman, A. Mechanisms of Neurodegeneration in Various Forms of Parkinsonism-Similarities and Differences. Cells 2021, 10, 656. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Shin, H.W.; Hong, S.W.; Youn, Y.C. Clinical Aspects of the Differential Diagnosis of Parkinson’s Disease and Parkinsonism. J. Clin. Neurol. 2022, 18, 259–270. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Masrori, P.; Van Damme, P. Amyotrophic lateral sclerosis: A clinical review. Eur. J. Neurol. 2020, 27, 1918–1929. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nash, L.A.; Burns, J.K.; Chardon, J.W.; Kothary, R.; Parks, R.J. Spinal Muscular Atrophy: More than a Disease of Motor Neurons? Curr. Mol. Med. 2016, 16, 779–792. [Google Scholar] [CrossRef] [PubMed]
- Soto, C.; Satani, N. The intricate mechanisms of neurodegeneration in prion diseases. Trends Mol. Med. 2011, 17, 14–24. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Prusiner, S.B. Biology and genetics of prions causing neurodegeneration. Annu. Rev. Genet. 2013, 47, 601–623. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Onesti, E.; Schettino, I.; Gori, M.C.; Frasca, V.; Ceccanti, M.; Cambieri, C.; Ruoppolo, G.; Inghilleri, M. Dysphagia in Amyotrophic Lateral Sclerosis: Impact on Patient Behavior, Diet Adaptation, and Riluzole Management. Front. Neurol. 2017, 8, 94. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nichols, N.L.; Van Dyke, J.; Nashold, L.; Satriotomo, I.; Suzuki, M.; Mitchell, G.S. Ventilatory control in ALS. Respir. Physiol. Neurobiol. 2013, 189, 429–437. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Watts, C.R.; Vanryckeghem, M. Laryngeal dysfunction in Amyotrophic Lateral Sclerosis: A review and case report. BMC Ear Nose Throat Disord. 2001, 1, 1. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Arai, M.; Endo, S.; Oshima, G.; Yagi, Y. A case of amyotrophic lateral sclerosis with bilateral vocal cord paralysis necessitating tracheotomy. Rinsho Shinkeigaku 2011, 51, 765–769. [Google Scholar] [CrossRef] [PubMed]
- van der Graaff, M.M.; Grolman, W.; Westermann, E.J.; Boogaardt, H.C.; Koelman, H.; van der Kooi, A.J.; Tijssen, M.A.; de Visser, M. Vocal cord dysfunction in amyotrophic lateral sclerosis: Four cases and a review of the literature. Arch. Neurol. 2009, 66, 1329–1333. [Google Scholar] [CrossRef] [PubMed]
- Fukae, J.; Kubo, S.; Hattori, N.; Komatsu, K.; Kato, M.; Aoki, M.; Mizuno, Y. Hoarseness due to bilateral vocal cord paralysis as an initial manifestation of familial amyotrophic lateral sclerosis. Amyotroph. Lateral Scler. Other Mot. Neuron Disord 2005, 6, 122–124. [Google Scholar] [CrossRef] [PubMed]
- Gotesman, R.D.; Lalonde, E.; McKim, D.A.; Bourque, P.R.; Warman-Chardon, J.; Zwicker, J.; Breiner, A. Laryngospasm in amyotrophic lateral sclerosis. Muscle Nerve 2022, 65, 400–404. [Google Scholar] [CrossRef] [PubMed]
- Yunusova, Y.; Plowman, E.K.; Green, J.R.; Barnett, C.; Bede, P. Clinical Measures of Bulbar Dysfunction in ALS. Front. Neurol. 2019, 10, 106. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Isozaki, E.; Shimizu, T.; Takamoto, K.; Horiguchi, S.; Hayashida, T.; Oda, M.; Tanabe, H. Vocal cord abductor paralysis (VCAP) in Parkinson’s disease: Difference from VCAP in multiple system atrophy. J. Neurol. Sci. 1995, 130, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Merati, A.L.; Heman-Ackah, Y.D.; Abaza, M.; Altman, K.W.; Sulica, L.; Belamowicz, S. Common movement disorders affecting the larynx: A report from the neurolaryngology committee of the AAO-HNS. Otolaryngol. Head Neck Surg. 2005, 133, 654–665. [Google Scholar] [CrossRef] [PubMed]
- de Swart, B.J.; Willemse, S.C.; Maassen, B.A.; Horstink, M.W. Improvement of voicing in patients with Parkinson’s disease by speech therapy. Neurology 2003, 60, 498–500. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.H.; Lim, S.C.; Lee, J.K. Bilateral vocal cord paralysis in a patient with Parkinson’s disease. B-ENT 2012, 8, 141–142. [Google Scholar] [PubMed]
- Isozaki, E.; Naito, A.; Horiguchi, S.; Kawamura, R.; Hayashida, T.; Tanabe, H. Early diagnosis and stage classification of vocal cord abductor paralysis in patients with multiple system atrophy. J. Neurol. Neurosurg. Psychiatry 1996, 60, 399–402. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Higo, R.; Tayama, N.; Watanabe, T.; Nitou, T.; Takeuchi, S. Vocal fold motion impairment in patients with multiple system atrophy: Evaluation of its relationship with swallowing function. J. Neurol. Neurosurg. Psychiatry 2003, 74, 982–984. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Grimaldi, S.; Renaud, M.; Robert, D.; Lagier, A.; Somma, H.; Soulayrol, S.; Korchia, D.; Fluchere, F.; Lagha-Boukbiza, O.; Schaeffer, M.; et al. Prevalence and characterisation of vocal fold motion impairment (VFMI) in patients with Multiple system atrophy compared with Parkinson’s disease. Rev. Neurol. 2020, 176, 608–613. [Google Scholar] [CrossRef] [PubMed]
- Ueha, R.; Sato, T.; Goto, T.; Yamauchi, A.; Nativ-Zeltzer, N.; Mitsui, J.; Belafsky, P.C.; Yamasoba, T. Esophageal Dysmotility is Common in Patients with Multiple System Atrophy. Laryngoscope 2021, 131, 832–838. [Google Scholar] [CrossRef] [PubMed]
- Ozawa, T.; Sekiya, K.; Aizawa, N.; Terajima, K.; Nishizawa, M. Laryngeal stridor in multiple system atrophy: Clinicopathological features and causal hypotheses. J. Neurol. Sci. 2016, 361, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Yogakanthi, S.; Wools, C.; Mathers, S. Unilateral vocal cord adductor weakness: An atypical manifestation of motor neurone disease. BMJ Neurol. Open 2021, 3, e000205. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Papapetropoulos, S.; Tuchman, A.; Laufer, D.; Papatsoris, A.G.; Papapetropoulos, N.; Mash, D.C. Causes of death in multiple system atrophy. J. Neurol. Neurosurg. Psychiatry 2007, 78, 327–329. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Isozaki, E.; Hayashi, M.; Hayashida, T.; Tanabe, H.; Hirai, S. Vocal cord abductor paralysis in multiple system atrophy–paradoxical movement of vocal cords during sleep. Rinsho Shinkeigaku 1996, 36, 529–533. [Google Scholar] [PubMed]
- Lalich, I.J.; Ekbom, D.C.; Starkman, S.J.; Orbelo, D.M.; Morgenthaler, T.I. Vocal fold motion impairment in multiple system atrophy. Laryngoscope 2014, 124, 730–735. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, M.J. Progressive Supranuclear Palsy: An Update. Curr. Neurol. Neurosci. Rep. 2018, 18, 12. [Google Scholar] [CrossRef] [PubMed]
- Lyons, S.; Trepel, D.; Lynch, T.; Walsh, R.; O’Dowd, S. The prevalence and incidence of progressive supranuclear palsy and corticobasal syndrome: A systematic review and meta-analysis. J. Neurol. 2023, 270, 4451–4465. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Enver, N.; Borders, J.C.; Curtis, J.A.; Sevitz, J.S.; Vanegas-Arroyave, N.; Troche, M.S. The Role of Vocal Fold Bowing on Cough and Swallowing Dysfunction in Progressive Supranuclear Palsy. Laryngoscope 2021, 131, 1217–1222. [Google Scholar] [CrossRef] [PubMed]
- Wen, Y.; Yang, Q.; Jiao, B.; Zhang, W.; Lin, J.; Zhu, Y.; Xu, Q.; Zhou, H.; Weng, L.; Liao, X.; et al. Clinical features of progressive supranuclear palsy. Front. Aging Neurosci. 2023, 15, 1229491. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sakai, K.; Sumikawa, K. Anesthetic management of a patient with progressive supranuclear palsy. J. Anesth. 2006, 20, 312–313. [Google Scholar] [CrossRef] [PubMed]
- Holinger, L.D.; Holinger, P.C.; Holinger, P.H. Etiology of bilateral abductor vocal cord paralysis: A review of 389 cases. Ann. Otol. Rhinol. Laryngol. 1976, 85, 428–436. [Google Scholar] [CrossRef] [PubMed]
- Urquhart, A.C.; St Louis, E.K. Idiopathic vocal cord palsies and associated neurological conditions. Arch. Otolaryngol. Head Neck Surg. 2005, 131, 1086–1089. [Google Scholar] [CrossRef] [PubMed]
- Rontal, E.; Rontal, M.; Wald, J.; Rontal, D. Botulinum toxin injection in the treatment of vocal fold paralysis associated with multiple sclerosis: A case report. J. Voice 1999, 13, 274–279. [Google Scholar] [CrossRef] [PubMed]
- Ueha, R.; Naito, R.; Watanabe, Y.; Watanabe, T.; Naito, A.; Yamasoba, T. Dysphagia in patients with bilateral vocal cord paralysis caused by multiple system atrophy. Deglutition 2012, 1, 9. [Google Scholar]
- Hamdan, A.L.; Khalifee, E.; Tabet, G. Unilateral Vocal Fold Paralysis in Parkinson Disease: Case Report and Review of the Literature. J. Voice 2018, 32, 763–766. [Google Scholar] [CrossRef] [PubMed]
- Lapresle, J.; Annabi, A. Olivopontocerebellar atrophy with velopharyngolaryngeal paralysis: A contribution to the somatotopy of the nucleus ambiguus. J. Neuropathol. Exp. Neurol. 1979, 38, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Howell, R.J.; Webster, H.; Kissela, E.; Gustin, R.; Kaval, F.; Klaben, B.; Khosla, S. Dysphagia in Parkinson’s Disease Improves with Vocal Augmentation. Dysphagia 2019, 34, 862–868. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.I.; Lee, D.H.; Kim, H. Bilateral vocal cord paralysis during emergence from general anesthesia in a patient with Parkinson’s disease. Saudi J. Anaesth. 2020, 14, 112–114. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Palesse, N.; Marelli, A.; Legge, M.P. Bilateral abductor paralysis of the vocal cords in the course of neurological diseases: Report of 5 cases. Ital. J. Neurol. Sci. 1988, 9, 59–62. [Google Scholar] [CrossRef] [PubMed]
- Shiba, K.; Isono, S.; Nakazawa, K. Paradoxical vocal cord motion: A review focused on multiple system atrophy. Auris Nasus Larynx 2007, 34, 443–452. [Google Scholar] [CrossRef] [PubMed]
- Guindi, G.M.; Higenbottam, T.W.; Payne, J.K. A new method for laryngeal electromyography. Clin. Otolaryngol. Allied Sci. 1981, 6, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Guindi, G.M.; Bannister, R.; Gibson, W.P.; Payne, J.K. Laryngeal electromyography in multiple system atrophy with autonomic failure. J. Neurol. Neurosurg. Psychiatry 1981, 44, 49–53. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Isozaki, E.; Osanai, R.; Horiguchi, S.; Hayashida, T.; Hirose, K.; Tanabe, H. Laryngeal electromyography with separated surface electrodes in patients with multiple system atrophy presenting with vocal cord paralysis. J. Neurol. 1994, 241, 551–556. [Google Scholar] [CrossRef] [PubMed]
- Ramig, L.O.; Fox, C.; Sapir, S. Parkinson’s disease: Speech and voice disorders and their treatment with the Lee Silverman Voice Treatment. Semin. Speech Lang. 2004, 25, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.T.; Benyamini, L. Voice outcome after vocal fold injection augmentation with carboxymethyl cellulose versus calcium hydroxyapatite. J. Laryngol. Otol. 2020, 134, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Courey, M.S.; Naunheim, M.R. Injection Laryngoplasty for Management of Neurological Vocal Fold Immobility. Adv. Otorhinolaryngol. 2020, 85, 68–84. [Google Scholar] [CrossRef] [PubMed]
- Heman-Ackah, Y.D.; Ivey, C.M.; Alexander, R. Options for treatment of a small glottic gap. Laryngoscope Investig. Otolaryngol. 2023, 8, 720–729. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mortensen, M.; Carroll, L.; Woo, P. Arytenoid adduction with medialization laryngoplasty versus injection or medialization laryngoplasty: The role of the arytenoidopexy. Laryngoscope 2009, 119, 827–831. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Brake, M.K.; Anderson, J. Bilateral vocal fold immobility: A 13 year review of etiologies, management and the utility of the Empey index. J. Otolaryngol. Head Neck Surg. 2015, 44, 27. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Garrett, G.; Zealear, D. Current Treatment Options for Bilateral Vocal Fold Paralysis: A State-of-the-Art Review. Clin. Exp. Otorhinolaryngol. 2017, 10, 203–212. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zitsch, R.P., 3rd. Continuous positive airway pressure. Use in bilateral vocal cord paralysis. Arch. Otolaryngol. Head Neck Surg. 1992, 118, 875–876. [Google Scholar] [CrossRef] [PubMed]
- Blumin, J.H.; Berke, G.S. Bilateral vocal fold paresis and multiple system atrophy. Arch. Otolaryngol. Head Neck Surg. 2002, 128, 1404–1407. [Google Scholar] [CrossRef] [PubMed]
- Ongkasuwan, J.; Courey, M. The role of botulinum toxin in the management of airway compromise due to bilateral vocal fold paralysis. Curr. Opin. Otolaryngol. Head Neck Surg. 2011, 19, 444–448. [Google Scholar] [CrossRef] [PubMed]
- Lekue, A.; Garcia-Lopez, I.; Santiago, S.; Del Palacio, A.; Gavilan, J. Diagnosis and management with botulinum toxin in 11 cases of laryngeal synkinesis. Eur. Arch. Otorhinolaryngol. 2015, 272, 2397–2402. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.C.; Wu, M.N.; Liou, L.M.; Chang, Y.P. Levodopa reverse stridor and prevent subsequent endotracheal intubation in Parkinson disease patients with bilateral vocal cord palsy: A case report. Medicine 2016, 95, e5559. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ueha, R.; Nito, T.; Sakamoto, T.; Yamauchi, A.; Tsunoda, K.; Yamasoba, T. Post-operative swallowing in multiple system atrophy. Eur. J. Neurol. 2016, 23, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Sapundzhiev, N.; Lichtenberger, G.; Eckel, H.E.; Friedrich, G.; Zenev, I.; Toohill, R.J.; Werner, J.A. Surgery of adult bilateral vocal fold paralysis in adduction: History and trends. Eur. Arch. Otorhinolaryngol. 2008, 265, 1501–1514. [Google Scholar] [CrossRef] [PubMed]
- Czesak, M.A.; Osuch-Wojcikiewicz, E.; Niemczyk, K. Methods of surgical treatment of bilateral vocal fold paralysis. Endokrynol. Pol. 2020, 71, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Qayyum, A.; Mierzwa, K.; See, M.; Sharma, A.; Montgommery, P.Q. Laser arytenoidectomy for bilateral vocal fold palsy in Parkinson’s disease. J. Laryngol. Otol. 2005, 119, 831–833. [Google Scholar] [CrossRef] [PubMed]
- Mahmud, A.; Strens, L.H.; Tedla, M. Laser arytenoidectomy and posterior cordotomy in a patient with bilateral vocal cord paralysis due to multiple system atrophy. BMJ Case Rep. 2015, 2015, bcr2014206156. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Damrose, E.J. Suture laterofixation of the vocal fold for bilateral vocal fold immobility. Curr. Opin. Otolaryngol. Head Neck Surg. 2011, 19, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Hyodo, M.; Nishikubo, K.; Motoyoshi, K. Laterofixation of the vocal fold using an endo-extralaryngeal needle carrier for bilateral vocal fold paralysis. Auris Nasus Larynx 2009, 36, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Koyama, M.; Ueha, R.; Sato, T.; Goto, T.; Yamauchi, A.; Kaneoka, A.; Suzuki, S.; Nito, T.; Yamasoba, T. Aspiration Prevention Surgery: Clinical Factors Associated with Improvements in Oral Status Intake and Suction Frequency. Otolaryngol. Head Neck Surg. 2023, 168, 1146–1155. [Google Scholar] [CrossRef] [PubMed]
- Ito, H.; Nagao, A.; Maeda, S.; Nakahira, M.; Hyodo, M. Clinical Significance of Surgical Intervention to Restore Swallowing Function for Sustained Severe Dysphagia. J. Clin. Med. 2023, 12, 5555. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ueha, R.; Cotaoco, C.; Kondo, K.; Yamasoba, T. Management and Treatment for Dysphagia in Neurodegenerative Disorders. J. Clin. Med. 2023, 13, 156. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ueha, R.; Magdayao, R.B.; Koyama, M.; Sato, T.; Goto, T.; Yamasoba, T. Aspiration prevention surgeries: A review. Respir. Res. 2023, 24, 43. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
Figure 1.
Etiologies of vocal fold motion impairment. CA, cricoarytenoid.

Figure 2.
Pathophysiology of vocal fold motion impairment in amyotrophic lateral sclerosis.

Figure 3.
Pathophysiology of vocal fold motion impairment in Parkinson’s disease and multiple system atrophy. MSA, multiple system atrophy; PD, Parkinson’s disease; PCA, posterior cricoarytenoid muscle.
Figure 3.
Pathophysiology of vocal fold motion impairment in Parkinson’s disease and multiple system atrophy. MSA, multiple system atrophy; PD, Parkinson’s disease; PCA, posterior cricoarytenoid muscle.

Figure 4.
Therapeutic interventions targeting glottic closure insufficiency and insufficient glottic opening. CPAP, continuous positive airway pressure.
Figure 4.
Therapeutic interventions targeting glottic closure insufficiency and insufficient glottic opening. CPAP, continuous positive airway pressure.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Comparison of clinical findings in patients with Parkinson’s disease and multiple system atrophy who developed vocal fold motion impairment. PD, Parkinson’s disease; MSA, multiple system atrophy; VFMI, vocal fold motion impairment; TA, thyroarytenoid muscle; LCA, lateral cricoarytenoid muscle; PCA, posterior cricoarytenoid muscle.
Table 1.
Comparison of clinical findings in patients with Parkinson’s disease and multiple system atrophy who developed vocal fold motion impairment. PD, Parkinson’s disease; MSA, multiple system atrophy; VFMI, vocal fold motion impairment; TA, thyroarytenoid muscle; LCA, lateral cricoarytenoid muscle; PCA, posterior cricoarytenoid muscle.
| PD | MSA | |
|---|---|---|
| Age (year) [47,68,69] | 68.7 ± 9.2 | 62.8 ± 8.0 |
| Sex [47,68,69] | Male > Female | Male > Female |
| Onset to VFMI (year) [47,68,69] | 10.4 ± 5.6 | 7.6 ± 3.2 |
| Hoehn and Yahr scale [47,68] (Usually applied to PD) | Stage 5: 100% | Stage 3: 6.3% Stage 4: 43.7% Stage 5: 50% |
| Findings of VFMI [8,71,72,73,74] | Vocal fold abductor paralysis Glottic insufficiency | Vocal fold abductor motion impairment Paradoxical vocal fold movement |
| Degree of dysphagia at detection of VFMI [68] | Severe dysphagia in most cases | Varying degrees from normal to severe |
| Inspiratory stridor [47] | Daytime > Bedtime | Daytime < Bedtime |
| Diazepam test [58] | Improvement or no change in VFMI | VFMI worsening |
| Histology of the PCA [47,70] | No morphological abnormalities | Neurogenic muscular atrophy |
| Electromyography [75,76,77] | Hyperactivity of the laryngeal adductor muscles | Dystonic activation of TA and LCA Paradoxical activation of TA Reduced activity of PCA during sleep |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Ueha, R.; Miura, C.; Matsumoto, N.; Sato, T.; Goto, T.; Kondo, K. Vocal Fold Motion Impairment in Neurodegenerative Diseases. J. Clin. Med. 2024, 13, 2507. https://doi.org/10.3390/jcm13092507
AMA Style
Ueha R, Miura C, Matsumoto N, Sato T, Goto T, Kondo K. Vocal Fold Motion Impairment in Neurodegenerative Diseases. Journal of Clinical Medicine. 2024; 13(9):2507. https://doi.org/10.3390/jcm13092507
Chicago/Turabian StyleUeha, Rumi, Cathrine Miura, Naoyuki Matsumoto, Taku Sato, Takao Goto, and Kenji Kondo. 2024. "Vocal Fold Motion Impairment in Neurodegenerative Diseases" Journal of Clinical Medicine 13, no. 9: 2507. https://doi.org/10.3390/jcm13092507
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.