
The Relationship between Tumor Budding and Tumor Deposits in Patients with Stage III Colorectal Carcinoma
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Pathohistologically Assessment
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Sobin, L.; Wittekind, C. (Eds.) International Union against Cancer (UICC). TNM Classification of Malignant Tumours, 5th ed.; John Wiley & Sons, Inc.: New York, NY, USA, 1997; ISBN 0-471-18486-1. [Google Scholar]
- Sobin, L.; Wittekind, C. (Eds.) International Union against Cancer (UICC). TNM Classification of Malignant Tumours, 6th ed.; John Wiley & Sons, Inc.: New York, NY, USA, 2002; ISBN 978-0-471-22288-0. [Google Scholar]
- Sobin, L.; Gospodarowicz, M.; Wittekind, C. (Eds.) International Union against Cancer (UICC). TNM Classification of Malignant Tumours, 7th ed.; John Wiley & Sons, Inc.: New York, NY, USA, 2009; ISBN 978-1-4443-3241-4. [Google Scholar]
- Brierley, J.; Gospodarowicz, M.; Wittekind, C. (Eds.) International Union against Cancer (UICC). TNM Classification of Malignant Tumours, 8th ed.; John Wiley & Sons, Inc.: New York, NY, USA, 2017; ISBN 978-1-119-26357-9. [Google Scholar]
- Burke, H.B. Outcome Prediction and the Future of the TNM Staging System. JNCI J. Natl. Cancer Inst. 2004, 96, 1408–1409. [Google Scholar] [CrossRef] [PubMed]
- Rogers, A.C.; Winter, D.C.; Heeney, A.; Gibbons, D.; Lugli, A.; Puppa, G.; Sheahan, K. Systematic Review and Meta-Analysis of the Impact of Tumour Budding in Colorectal Cancer. Br. J. Cancer 2016, 115, 831–840. [Google Scholar] [CrossRef] [PubMed]
- Puppa, G.; Sonzogni, A.; Colombari, R.; Pelosi, G. TNM Staging System of Colorectal Carcinoma: A Critical Appraisal of Challenging Issues. Arch. Pathol. Lab. Med. 2010, 134, 837–852. [Google Scholar] [CrossRef] [PubMed]
- Maguire, A.; Sheahan, K. Controversies in the Pathological Assessment of Colorectal Cancer. World J. Gastroenterol. 2014, 20, 9850–9861. [Google Scholar] [CrossRef] [PubMed]
- Athanasakis, E.; Xenaki, S.; Venianaki, M.; Chalkiadakis, G.; Chrysos, E. Newly Recognized Extratumoral Features of Colorectal Cancer Challenge the Current Tumor-Node-Metastasis Staging System. Ann. Gastroenterol. 2018, 31, 525–534. [Google Scholar] [CrossRef] [PubMed]
- Landau, M.A.; Zhu, B.; Akwuole, F.N.; Pai, R.K. Histopathological Predictors of Recurrence in Stage III Colon Cancer: Reappraisal of Tumor Deposits and Tumor Budding Using AJCC8 Criteria. Int. J. Surg. Pathol. 2019, 27, 147–158. [Google Scholar] [CrossRef] [PubMed]
- Demirović, A.; Krušlin, B. Recommendations for Histopathology Report of Colorectal Carcinoma Specimens. Rad. Hrvat. Akad. Znan. I Umjet. 2017, 530, 67–72. [Google Scholar] [CrossRef]
- Riffet, M.; Dupont, B.; Faisant, M.; Cerasuolo, D.; Menahem, B.; Alves, A.; Dubois, F.; Levallet, G.; Bazille, C. New Histoprognostic Factors to Consider for the Staging of Colon Cancers: Tumor Deposits, Invasive Tumor Infiltration and High-Grade Budding. Int. J. Mol. Sci. 2023, 24, 3573. [Google Scholar] [CrossRef]
- Zlobec, I.; Lugli, A.; Baker, K.; Roth, S.; Minoo, P.; Hayashi, S.; Terracciano, L.; Jass, J.R. Role of APAF-1, E-cadherin and Peritumoural Lymphocytic Infiltration in Tumour Budding in Colorectal Cancer. J. Pathol. 2007, 212, 260–268. [Google Scholar] [CrossRef]
- Hase, K.; Shatney, C.; Johnson, D.; Trollope, M.; Vierra, M. Prognostic Value of Tumor “Budding” in Patients with Colorectal Cancer. Dis. Colon. Rectum 1993, 36, 627–635. [Google Scholar] [CrossRef] [PubMed]
- Ueno, H.; Mochizuki, H.; Hashiguchi, Y.; Hatsuse, K.; Fujimoto, H.; Hase, K. Predictors of Extrahepatic Recurrence after Resection of Colorectal Liver Metastases. Br. J. Surg. 2004, 91, 327–333. [Google Scholar] [CrossRef]
- Lugli, A.; Karamitopoulou, E.; Zlobec, I. Tumour Budding: A Promising Parameter in Colorectal Cancer. Br. J. Cancer 2012, 106, 1713–1717. [Google Scholar] [CrossRef] [PubMed]
- Ueno, H.; Murphy, J.; Jass, J.R.; Mochizuki, H.; Talbot, I.C. Tumour ‘budding’ as an Index to Estimate the Potential of Aggressiveness in Rectal Cancer. Histopathology 2002, 40, 127–132. [Google Scholar] [CrossRef]
- Berg, K.B.; Schaeffer, D.F. Tumor Budding as a Standardized Parameter in Gastrointestinal Carcinomas: More than Just the Colon. Mod. Pathol. 2018, 31, 862–872. [Google Scholar] [CrossRef] [PubMed]
- Thiery, J.P.; Acloque, H.; Huang, R.Y.J.; Nieto, M.A. Epithelial-Mesenchymal Transitions in Development and Disease. Cell 2009, 139, 871–890. [Google Scholar] [CrossRef]
- Hanahan, D.; Weinberg, R.A. Hallmarks of Cancer: The Next Generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Xu, F.; Li, S.; Zhong, A.; Meng, X.; Lai, M. The Tumor Microenvironment: An Irreplaceable Element of Tumor Budding and Epithelial-Mesenchymal Transition-Mediated Cancer Metastasis. Cell Adhes. Migr. 2016, 10, 1–13. [Google Scholar] [CrossRef]
- Priya, R.; Yap, A.S. Making a Choice: How Cadherin Switching Controls Cell Migration. Dev. Cell 2015, 34, 383–384. [Google Scholar] [CrossRef]
- Mashita, N.; Yamada, S.; Nakayama, G.; Tanaka, C.; Iwata, N.; Kanda, M.; Kobayashi, D.; Fujii, T.; Sugimoto, H.; Koike, M.; et al. Epithelial to Mesenchymal Transition Might Be Induced via CD44 Isoform Switching in Colorectal Cancer. J. Surg. Oncol. 2014, 110, 745–751. [Google Scholar] [CrossRef]
- Yabata, E.; Udagawa, M.; Okamoto, H. Effect of Tumor Deposits on Overall Survival in Colorectal Cancer Patients with Regional Lymph Node Metastases. J. Rural. Med. 2014, 9, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Lord, A.C.; D’Souza, N.; Pucher, P.H.; Moran, B.J.; Abulafi, A.M.; Wotherspoon, A.; Rasheed, S.; Brown, G. Significance of Extranodal Tumour Deposits in Colorectal Cancer: A Systematic Review and Meta-Analysis. Eur. J. Cancer 2017, 82, 92–102. [Google Scholar] [CrossRef] [PubMed]
- Ueno, H.; Mochizuki, H.; Hashiguchi, Y.; Ishiguro, M.; Miyoshi, M.; Kajiwara, Y.; Sato, T.; Shimazaki, H.; Hase, K. Extramural Cancer Deposits Without Nodal Structure in Colorectal Cancer: Optimal Categorization for Prognostic Staging. Am. J. Clin. Pathol. 2007, 127, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Lugli, A.; Kirsch, R.; Ajioka, Y.; Bosman, F.; Cathomas, G.; Dawson, H.; El Zimaity, H.; Fléjou, J.-F.; Hansen, T.P.; Hartmann, A.; et al. Recommendations for Reporting Tumor Budding in Colorectal Cancer Based on the International Tumor Budding Consensus Conference (ITBCC). Mod. Pathol. 2017, 30, 1299–1311. [Google Scholar] [CrossRef]
- Nagtegaal, I.D.; Quirke, P. Colorectal Tumour Deposits in the Mesorectum and Pericolon; a Critical Review. Histopathology 2007, 51, 141–149. [Google Scholar] [CrossRef]
- Jin, M.; Roth, R.; Rock, J.B.; Washington, M.K.; Lehman, A.; Frankel, W.L. The Impact of Tumor Deposits on Colonic Adenocarcinoma AJCC TNM Staging and Outcome. Am. J. Surg. Pathol. 2015, 39, 109–115. [Google Scholar] [CrossRef]
- Ueno, H.; Mochizuki, H.; Tamakuma, S. Prognostic Significance of Extranodal Microscopic Foci Discontinuous with Primary Lesion in Rectal Cancer. Dis. Colon. Rectum 1998, 41, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Prabhudesai, A.; Arif, S.; Finlayson, C.J.; Kumar, D. Impact of Microscopic Extranodal Tumor Deposits on the Outcome of Patients with Rectal Cancer. Dis. Colon. Rectum 2003, 46, 1531–1537. [Google Scholar] [CrossRef] [PubMed]
- Bouquot, M.; Creavin, B.; Goasguen, N.; Chafai, N.; Tiret, E.; André, T.; Flejou, J.-F.; Parc, Y.; Lefevre, J.H.; Svrcek, M. Prognostic Value and Characteristics of N1c Colorectal Cancer. Color. Dis. 2018, 20, 248–255. [Google Scholar] [CrossRef]
- Belt, E.J.T.; Van Stijn, M.F.M.; Bril, H.; De Lange-de Klerk, E.S.M.; Meijer, G.A.; Meijer, S.; Stockmann, H.B.A.C. Lymph Node Negative Colorectal Cancers with Isolated Tumor Deposits Should Be Classified and Treated As Stage III. Ann. Surg. Oncol. 2010, 17, 3203–3211. [Google Scholar] [CrossRef]
- Gopal, P.; Lu, P.; Ayers, G.D.; Herline, A.J.; Washington, M.K. Tumor Deposits in Rectal Adenocarcinoma after Neoadjuvant Chemoradiation Are Associated with Poor Prognosis. Mod. Pathol. 2014, 27, 1281–1287. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Choi, G. Clinical Implications of Lymph Node Metastasis in Colorectal Cancer: Current Status and Future Perspectives. Ann. Coloproctol. 2019, 35, 109–117. [Google Scholar] [CrossRef]
- Zhang, L.-N.; Xiao, W.-W.; Xi, S.-Y.; OuYang, P.-Y.; You, K.-Y.; Zeng, Z.-F.; Ding, P.-R.; Zhang, H.-Z.; Pan, Z.-Z.; Xu, R.-H.; et al. Tumor Deposits: Markers of Poor Prognosis in Patients with Locally Advanced Rectal Cancer Following Neoadjuvant Chemoradiotherapy. Oncotarget 2016, 7, 6335–6344. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Rehman, A.; Chung, Y.; Yi, K.; Wi, Y.C.; Kim, Y.; Jang, K.; Jang, S.M.; Paik, S.S. Clinicopathologic Significance of Extranodal Tumor Extension in Colorectal Adenocarcinoma with Regional Lymph Node Metastasis. Gastroenterol. Res. Pract. 2016, 2016, 5620765. [Google Scholar] [CrossRef] [PubMed]
- Koelzer, V.H.; Canonica, K.; Dawson, H.; Sokol, L.; Karamitopoulou-Diamantis, E.; Lugli, A.; Zlobec, I. Phenotyping of Tumor-Associated Macrophages in Colorectal Cancer: Impact on Single Cell Invasion (Tumor Budding) and Clinicopathological Outcome. OncoImmunology 2016, 5, e1106677. [Google Scholar] [CrossRef] [PubMed]
- Van Wyk, H.C.; Park, J.H.; Edwards, J.; Horgan, P.G.; McMillan, D.C.; Going, J.J. The Relationship between Tumour Budding, the Tumour Microenvironment and Survival in Patients with Primary Operable Colorectal Cancer. Br. J. Cancer 2016, 115, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Zlobec, I.; Lugli, A. Epithelial Mesenchymal Transition and Tumor Budding in Aggressive Colorectal Cancer: Tumor Budding as Oncotarget. Oncotarget 2010, 1, 651–661. [Google Scholar] [CrossRef]
- Prall, F. Tumour Budding in Colorectal Carcinoma. Histopathology 2007, 50, 151–162. [Google Scholar] [CrossRef] [PubMed]
- Shinto, E.; Mochizuki, H.; Ueno, H.; Matsubara, O.; Jass, J.R. A Novel Classification of Tumour Budding in Colorectal Cancer Based on the Presence of Cytoplasmic Pseudo-fragments around Budding Foci. Histopathology 2005, 47, 25–31. [Google Scholar] [CrossRef]
- Mitrovic, B.; Schaeffer, D.F.; Riddell, R.H.; Kirsch, R. Tumor Budding in Colorectal Carcinoma: Time to Take Notice. Mod. Pathol. 2012, 25, 1315–1325. [Google Scholar] [CrossRef]
- Graham, R.P.; Vierkant, R.A.; Tillmans, L.S.; Wang, A.H.; Laird, P.W.; Weisenberger, D.J.; Lynch, C.F.; French, A.J.; Slager, S.L.; Raissian, Y.; et al. Tumor Budding in Colorectal Carcinoma: Confirmation of Prognostic Significance and Histologic Cutoff in a Population-Based Cohort. Am. J. Surg. Pathol. 2015, 39, 1340–1346. [Google Scholar] [CrossRef] [PubMed]
- Kakar, S.; Chanjuan, S.; Mariana, B.; Driman, D.; Fitzgibbons, P.; Frankel, W.; Hill, K.; Jessup, J.; Krasinskas, A.; Washington, M.; et al. Protocol for the Examination of Specimens from Patients with Primary Carcinomaof the Colon and Rectum. 2023. Available online: https://documents.cap.org/protocols/ColoRectal_4.3.0.0.REL_CAPCP.pdf (accessed on 23 April 2024).
- Loughrey, M.B.; Webster, F.; Arends, M.J.; Brown, I.; Burgart, L.J.; Cunningham, C.; Flejou, J.-F.; Kakar, S.; Kirsch, R.; Kojima, M.; et al. Dataset for Pathology Reporting of Colorectal Cancer: Recommendations from the International Collaboration on Cancer Reporting (ICCR). Ann. Surg. 2022, 275, e549–e561. [Google Scholar] [CrossRef] [PubMed]
- Benson, A.; Venook, A.; Adam, M.; Chen, Y.; Ciombor, K.; Cohen, S.; Cooper, H.; Deming, D.; National Comprehensive Cancer Network. Colon Cancer Version 1.2024—January 29, 2024: NCCN Clinical Practice Guidelines in Oncology. Available online: https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf (accessed on 23 April 2024).
- Benson, A.; Venook, A.; Adam, M.; Chen, Y.; Ciombor, K.; Cohen, S.; Cooper, H.; Deming, D.; National Comprehensive Cancer Network. Rectal Cancer Version 1.2024—January 29, 2024: NCCN Clinical Practice Guidelines in Oncology. Available online: https://www.nccn.org/professionals/physician_gls/pdf/rectal.pdf (accessed on 23 April 2024).
- Zlobec, I.; Berger, M.D.; Lugli, A. Tumour Budding and Its Clinical Implications in Gastrointestinal Cancers. Br. J. Cancer 2020, 123, 700–708. [Google Scholar] [CrossRef] [PubMed]
- Dawson, H.; Blank, A.; Zlobec, I.; Lugli, A. Potential Clinical Scenarios of Tumour Budding in Colorectal Cancer. Acta Gastroenterol. Belg. 2019, 82, 515–518. [Google Scholar] [PubMed]
- Ueno, H.; Ishiguro, M.; Nakatani, E.; Ishikawa, T.; Uetake, H.; Matsuda, C.; Nakamoto, Y.; Kotake, M.; Kurachi, K.; Egawa, T.; et al. Prospective Multicenter Study on the Prognostic and Predictive Impact of Tumor Budding in Stage II Colon Cancer: Results from the SACURA Trial. J. Clin. Oncol. 2019, 37, 1886–1894. [Google Scholar] [CrossRef] [PubMed]
- Haddad, T.S.; Lugli, A.; Aherne, S.; Barresi, V.; Terris, B.; Bokhorst, J.-M.; Brockmoeller, S.F.; Cuatrecasas, M.; Simmer, F.; El-Zimaity, H.; et al. Improving Tumor Budding Reporting in Colorectal Cancer: A Delphi Consensus Study. Virchows Arch. 2021, 479, 459–469. [Google Scholar] [CrossRef] [PubMed]
- Koelzer, V.H.; Assarzadegan, N.; Dawson, H.; Mitrovic, B.; Grin, A.; Messenger, D.E.; Kirsch, R.; Riddell, R.H.; Lugli, A.; Zlobec, I. Cytokeratin-based Assessment of Tumour Budding in Colorectal Cancer: Analysis in Stage II Patients and Prospective Diagnostic Experience. J. Pathol. Clin. Res. 2017, 3, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.-H.; Yan, Z.-C.; Liu, J.-Y.; Li, X.-Y.; Yang, M.; Fan, J.; Huang, B.; Ma, C.-G.; Chang, X.-N.; Nie, X. Association of Tumor Budding with Clinicopathological Features and Prognostic Value in Stage III-IV Colorectal Cancer. World J. Gastroenterol. 2024, 30, 158–169. [Google Scholar] [CrossRef]
- Wang, K.; He, H.; Lin, Y.; Zhang, Y.; Chen, J.; Hu, J.; He, X. A New Clinical Model for Predicting Lymph Node Metastasis in T1 Colorectal Cancer. Int. J. Color. Dis. 2024, 39, 46. [Google Scholar] [CrossRef]
- Kamall, G.H.; Ulusoy, C.; Nikolovski, A.; Kamall, S. Tumour Budding—An Additional Prognostic Factor in Colorectal Cancer Survival. Pol. J. Pathol. 2023, 74, 36–41. [Google Scholar] [CrossRef]
- Cyr, D.P.; Pun, C.; Shivji, S.; Mitrovic, B.; Duan, K.; Tomin, R.; Sari, A.; Brar, A.; Zerhouni, S.; Brar, M.S.; et al. Tumor Budding Assessment in Colorectal Carcinoma: Normalization Revisited. Am. J. Surg. Pathol. 2024, 48, 251–265. [Google Scholar] [CrossRef] [PubMed]
- Jurescu, A.; Dema, A.; Văduva, A.; Gheju, A.; Vița, O.; Barna, R.; Lăzureanu, C.; Cornianu, M.; Tăban, S.; Duță, C.; et al. Poorly Differentiated Clusters and Tumor Budding Are Important Prognostic Factors in Colorectal Carcinomas. Bosn. J. Basic. Med. Sci. 2021, 22, 164–177. [Google Scholar] [CrossRef] [PubMed]
- Lino-Silva, L.S.; Salcedo-Hernández, R.A.; Gamboa-Domínguez, A. Tumour Budding in Rectal Cancer. A Comprehensive Review. Contemp. Oncol. 2018, 22, 61–74. [Google Scholar] [CrossRef]
- Krištić, A.; Aralica, G.; Demirović, A.; Krušlin, B. Pathohistologic Prognostic and Predictive Parameters in ColorectalcancerTumor Budding. Rad. Hrvat. Akad. Znan. I Umjet. 2018, 533, 113–126. [Google Scholar] [CrossRef]
- Mirkin, K.A.; Kulaylat, A.S.; Hollenbeak, C.S.; Messaris, E. Prognostic Significance of Tumor Deposits in Stage III Colon Cancer. Ann. Surg. Oncol. 2018, 25, 3179–3184. [Google Scholar] [CrossRef]
- Koelzer, V.H.; Zlobec, I.; Berger, M.D.; Cathomas, G.; Dawson, H.; Dirschmid, K.; Hädrich, M.; Inderbitzin, D.; Offner, F.; Puppa, G.; et al. Tumor Budding in Colorectal Cancer Revisited: Results of a Multicenter Interobserver Study. Virchows Arch. 2015, 466, 485–493. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total (N = 90) | % | TB Grade | p * | |||||
|---|---|---|---|---|---|---|---|---|---|
| Bd1 (N = 23) | % | Bd2 (N = 20) | % | Bd3 (N = 47) | % | ||||
| Age | |||||||||
| <65 | 36 | 40.0% | 9 | 39.1% | 10 | 50.0% | 17 | 36.2% | 0.689 |
| ≥65 | 54 | 60.0% | 14 | 60.9% | 10 | 50.0% | 30 | 63.8% | |
| Mean (±SD) | 65.8 (±10.6) | ||||||||
| Gender | 90 | 100.0% | |||||||
| Male | 55 | 61.1% | 15 | 65.2% | 14 | 70.0% | 26 | 55.3% | 0.314 |
| Female | 35 | 38.9% | 8 | 37.8% | 6 | 30.0% | 21 | 44.7% | |
| Tumor location | |||||||||
| Right side | 21 | 23.3% | 6 | 26.1% | 2 | 10.0% | 13 | 27.7% | 0.67 |
| Left side | 35 | 38.9% | 10 | 43.5% | 9 | 45.0% | 16 | 34.0% | |
| Rectum | 34 | 37.8% | 7 | 30.4% | 9 | 45.0% | 18 | 38.3% | |
| Histological grade | |||||||||
| Low grade | 73 | 81.0% | 17 | 73.9% | 17 | 85.0% | 39 | 83.0% | 0.465 |
| High grade | 17 | 19.0% | 6 | 26.1% | 3 | 15.0% | 8 | 17.0% | |
| TD | |||||||||
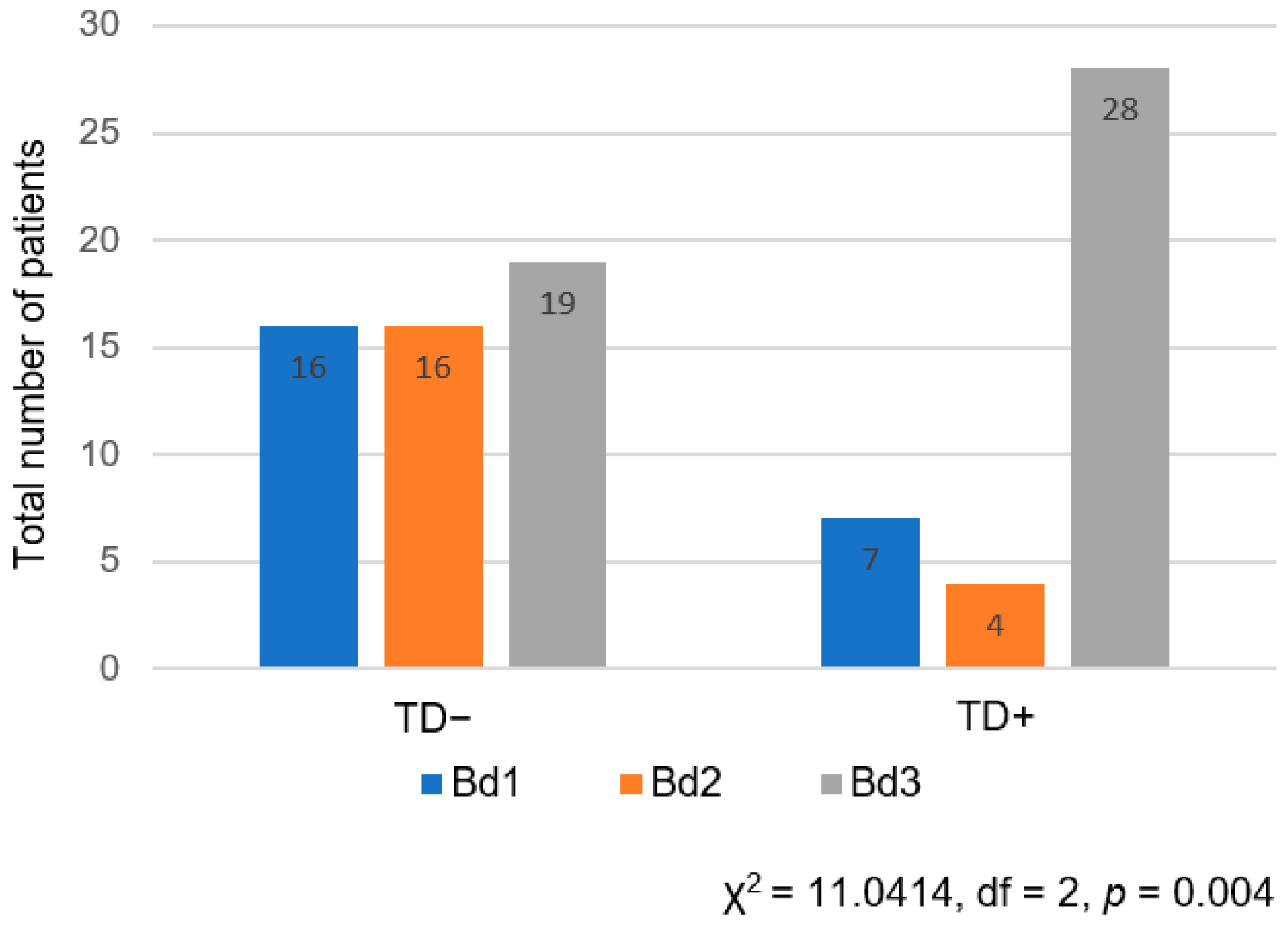
| Presence (TD+) | 39 | 43.3% | 7 | 30.4% | 4 | 20.0% | 28 | 59.6% | 0.002 |
| Absence (TD−) | 51 | 56.7% | 16 | 69.6% | 16 | 80.0% | 19 | 40.4% | |
| TB | |||||||||
| Presence | 85 | 94.4% | - | - | - | - | - | - | 1 |
| Mean No. (±SD) | 22.5 (±24.2) | - | - | - | - | - | - | ||
| Range | 0–138 | ||||||||
| Bd1 | 23 | 25.6% | - | - | - | - | - | - | |
| Bd2 | 20 | 22.2% | - | - | - | - | - | - | |
| Bd3 | 47 | 52.2% | - | - | - | - | - | - | |
| pT | |||||||||
| T1 | 1 | 1.1% | 1 | 4.3% | 0 | 0% | 0 | 0% | 0.214 |
| T2 | 7 | 7.8% | 1 | 4.3% | 1 | 5.0% | 5 | 10.6% | |
| T3 | 78 | 86.7% | 18 | 78.3% | 19 | 95.0% | 41 | 87.2% | |
| T4 | 4 | 4.4% | 3 | 13.1% | 0 | 0% | 1 | 2.2% | |
| pN | |||||||||
| N1 | 58 | 64.4% | 14 | 60.9% | 11 | 55.0% | 33 | 70.2% | 0.318 |
| N2 | 32 | 45.6% | 9 | 39.1% | 9 | 45.0% | 14 | 29.8% | |
| TNM Stage | |||||||||
| IIIA | 9 | 10.0% | 2 | 8.7% | 1 | 5.0% | 5 | 10.6% | 0.219 |
| IIIB | 69 | 76.7% | 16 | 69.6% | 17 | 85.0% | 36 | 76.6% | |
| IIIC | 12 | 13.3% | 5 | 21.7% | 2 | 10.0% | 6 | 12.8% | |
| Variables | Hazard Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Age, years, <65 vs. ≥65 | 1.31 | 1.1–1.08 | 0.001 |
| Gender, female vs. male | 0.281 | 0.27–1.56 | 0.092 |
| Histological grade, LG vs. HG | 0.9 | 0.45–1.82 | 0.107 |
| T1, T2 vs. T3, T4 | 3.5 | 3.32–37.4 | 0.002 |
| N1 vs. N2 | 8.55 | 2.65–8.64 | 0.009 |
| TNM, IIIA vs. IIIB, IIIC | 3.2 | 1.13–4.09 | 0.016 |
| EMVI− vs. EMVI+ | 1.92 | 1.417–8.85 | 0.016 |
| LVI− vs. LVI+ | 1.34 | 1.148–1.76 | 0.049 |
| PNI− vs. PNI+ | 0.49 | 0.27–0.89 | 0.980 |
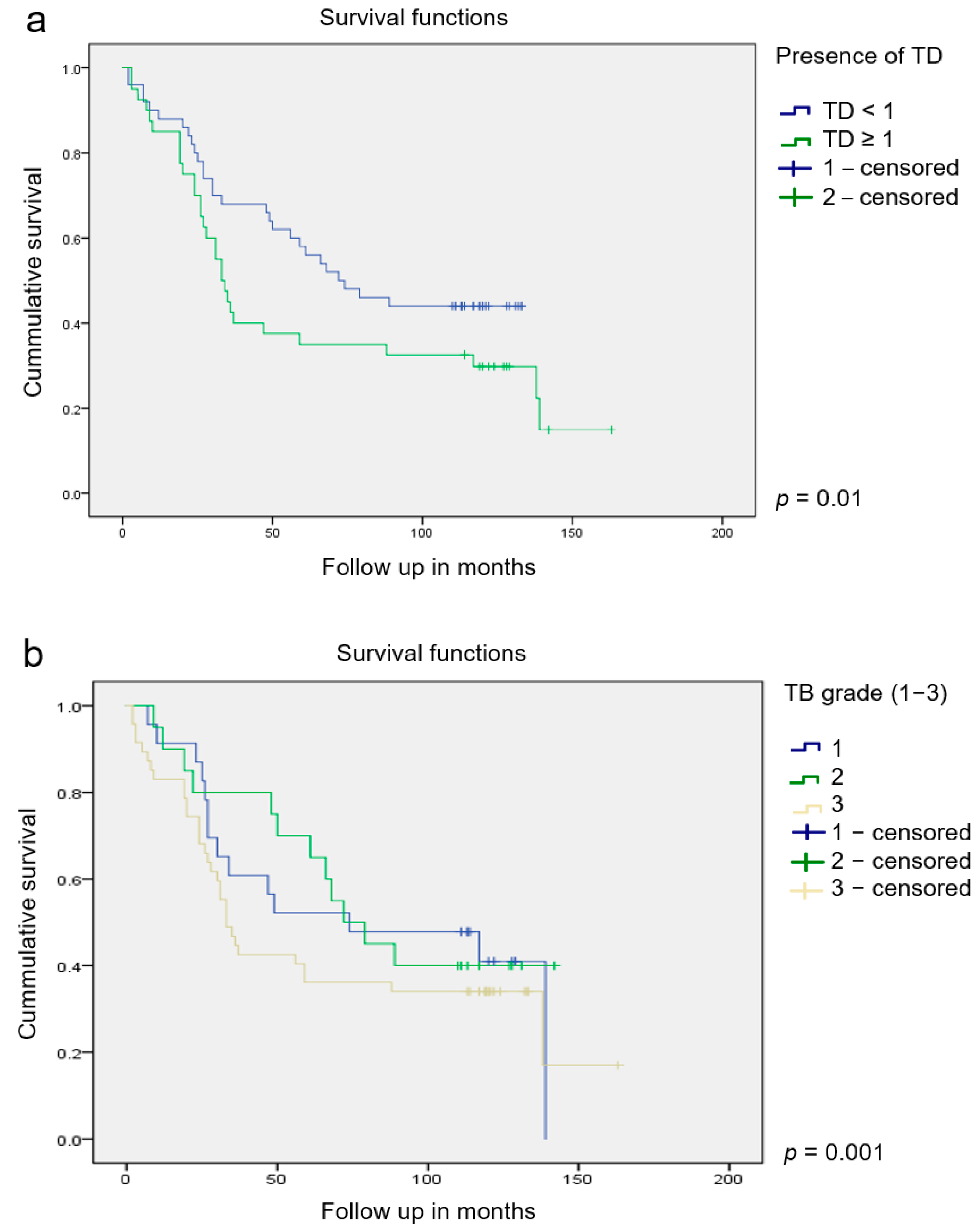
| TD− vs. TD+ | 2.1 | 1.9–2.92 | 0.010 |
| Number of TB, <30 vs. ≥30 | 1.9 | 1.36–3.74 | 0.002 |
| TB grade, Bd1 vs. Bd2, Bd3 | 2.28 | 1.93–4.76 | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bilić, Z.; Zovak, M.; Glavčić, G.; Mužina, D.; Ibukić, A.; Košec, A.; Tomas, D.; Demirović, A. The Relationship between Tumor Budding and Tumor Deposits in Patients with Stage III Colorectal Carcinoma. J. Clin. Med. 2024, 13, 2583. https://doi.org/10.3390/jcm13092583
Bilić Z, Zovak M, Glavčić G, Mužina D, Ibukić A, Košec A, Tomas D, Demirović A. The Relationship between Tumor Budding and Tumor Deposits in Patients with Stage III Colorectal Carcinoma. Journal of Clinical Medicine. 2024; 13(9):2583. https://doi.org/10.3390/jcm13092583
Chicago/Turabian StyleBilić, Zdenko, Mario Zovak, Goran Glavčić, Dubravka Mužina, Amir Ibukić, Andro Košec, Davor Tomas, and Alma Demirović. 2024. "The Relationship between Tumor Budding and Tumor Deposits in Patients with Stage III Colorectal Carcinoma" Journal of Clinical Medicine 13, no. 9: 2583. https://doi.org/10.3390/jcm13092583