
First Time Seizure in the Setting of a Congenital Heart Abnormality and MCA Mycotic Aneurysms

{kind=link}
{kind=link}
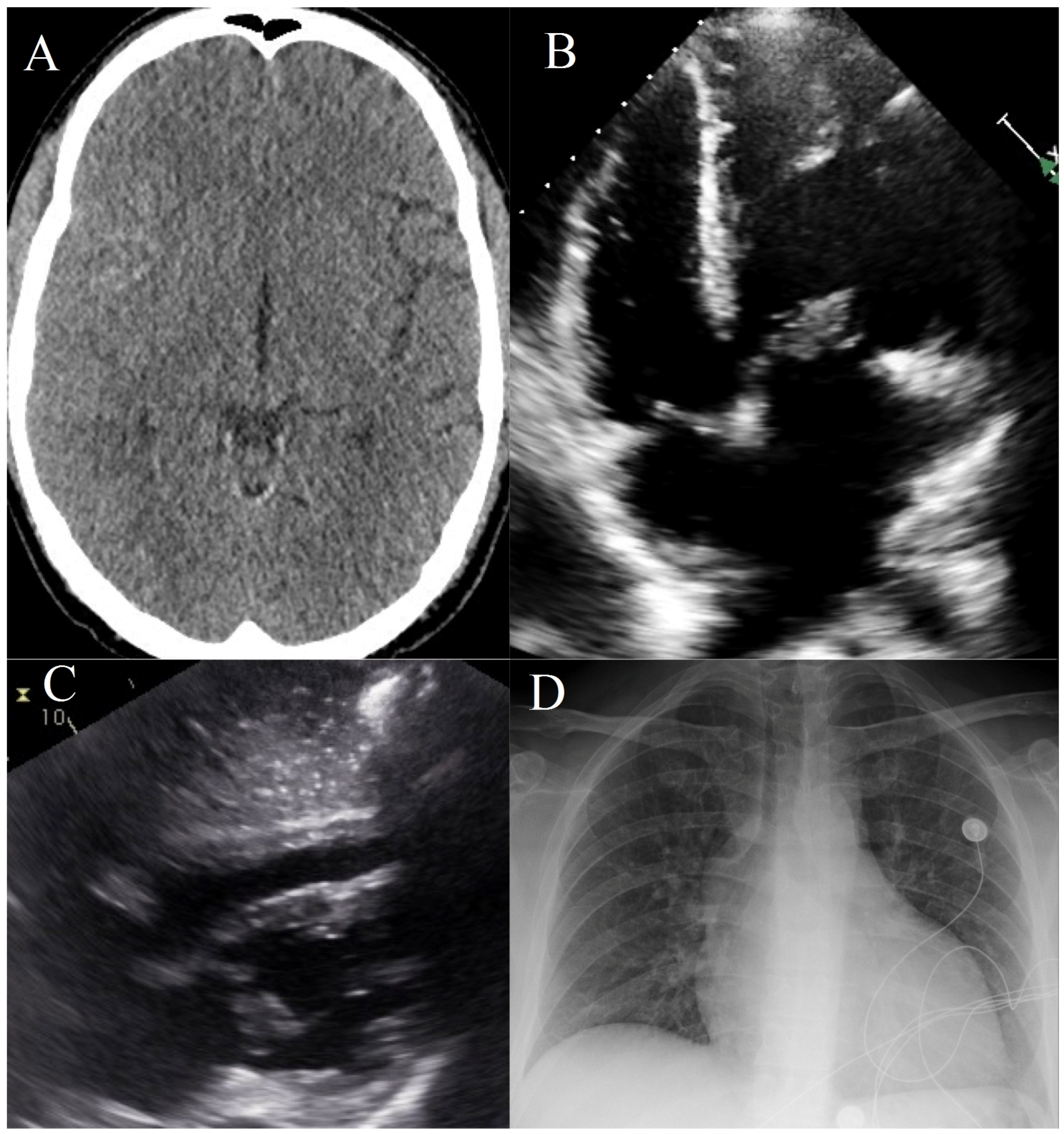
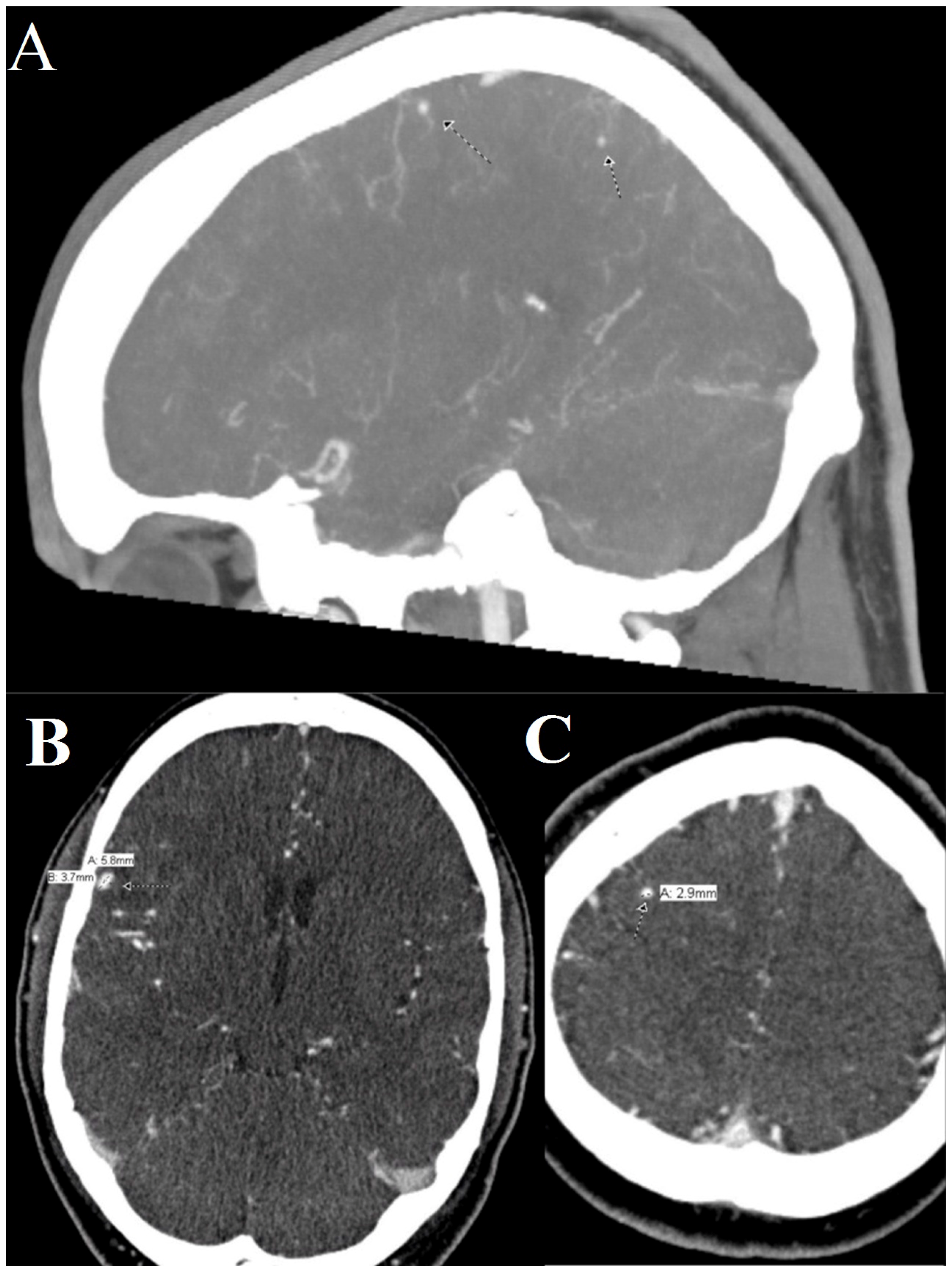
1. Clinical Presentation
2. Discussion
Conflicts of Interest
References
- Hoffman, J.I.E.; Kaplan, S. The Incidence of Congenital Heart Disease. J. Am. Coll. Cardiol. 2002, 39, 1890–1900. [Google Scholar] [CrossRef]
- Filippo, S.D.; Delahaye, F.; Semiond, B.; Celard, M.; Henaine, R.; Ninet, J.; Sassolas, F.; Bozio, A. Current Patterns of Infective Endocarditis in Congenital Heart Disease. Heart 2006, 92, 1490–1495. [Google Scholar] [CrossRef] [PubMed]
- Kong, K.H.; Chan, K.F. Ruptured Intracranial Mycotic Aneurysm: A Rare Cause of Intracranial Hemorrhage. Arch. Phys. Med. Rehabil. 1995, 76, 287–289. [Google Scholar] [CrossRef]
- Mayer, S.A.; Bernadini, G.L.; Solomon, R.A. Subarachnoid Hemorrhage. In Merritt’s Neurology, 13th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2016; Chapter 39. [Google Scholar]


© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minckler, M.R.; Curry, M.; Mosier, J.M. First Time Seizure in the Setting of a Congenital Heart Abnormality and MCA Mycotic Aneurysms. J. Clin. Med. 2016, 5, 46. https://doi.org/10.3390/jcm5040046
Minckler MR, Curry M, Mosier JM. First Time Seizure in the Setting of a Congenital Heart Abnormality and MCA Mycotic Aneurysms. Journal of Clinical Medicine. 2016; 5(4):46. https://doi.org/10.3390/jcm5040046
Chicago/Turabian StyleMinckler, Michael R., Merlin Curry, and Jarrod M. Mosier. 2016. "First Time Seizure in the Setting of a Congenital Heart Abnormality and MCA Mycotic Aneurysms" Journal of Clinical Medicine 5, no. 4: 46. https://doi.org/10.3390/jcm5040046