Safety Lapses Prior to Initiation of Hemodialysis for Acute Kidney Injury in Hospitalized Patients: A Patient Safety Initiative

 ,
,
Abstract
:1. Introduction
2. Experimental Section
2.1. Study Design and Setting
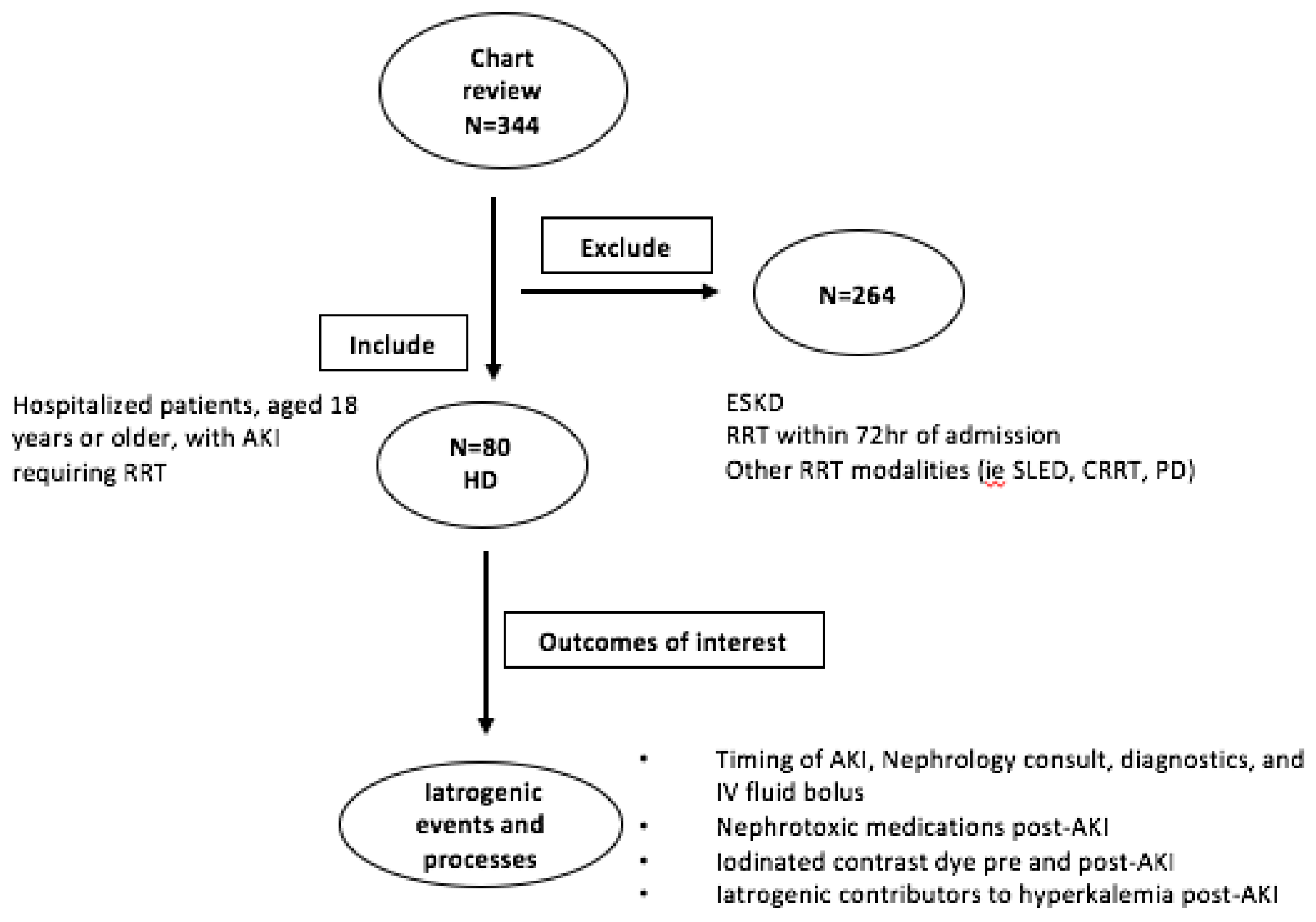
2.2. Patient Population, Inclusion and Exclusion Criteria
2.3. Data Sources and Data Collection
2.4. Outcomes and Analysis
3. Results
3.1. Patient Demographics and AKI Information
3.2. Nephrotoxins, Medications, Hyperkalemia and Indications for Dialysis
3.3. Summary of Representative Cases
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Wang, H.E.; Muntner, P.; Chertow, G.M.; Warnock, D.G. Acute Kidney Injury and Mortality in Hospitalized Patients. Am. J. Nephrol. 2012, 35, 349–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uchino, S.; Bellomo, R.; Goldsmith, D.; Bates, S.; Ronco, C. An assessment of the RIFLE criteria for acute renal failure in hospitalized patients. Crit. Care Med. 2006, 34, 1913–1917. [Google Scholar] [CrossRef] [PubMed]
- Metnitz, P.G.H.; Krenn, C.G.; Steltzer, H.; Lang, T.; Ploder, J.; Lenz, K.; Gall, J.-R.L.; Druml, W. Effect of acute renal failure requiring renal replacement therapy on outcome in critically ill patients. Crit. Care Med. 2002, 30, 2051–2058. [Google Scholar] [CrossRef] [PubMed]
- Coca, S.G.; Yusuf, B.; Shlipak, M.G.; Garg, A.X.; Parikh, C.R. Long-Term Risk of Mortality and Other Adverse Outcomes After Acute Kidney Injury: A Systematic Review and Meta-analysis. Am. J. Kidney Dis. 2009, 53, 961–973. [Google Scholar] [CrossRef] [PubMed]
- Coca, S.G.; Singanamala, S.; Parikh, C.R. Chronic kidney disease after acute kidney injury: A systematic review and meta-analysis. Kidney Int. 2012, 81, 442–448. [Google Scholar] [CrossRef] [PubMed]
- Chertow, G.M.; Burdick, E.; Honour, M.; Bonventre, J.V.; Bates, D.W. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J. Am. Soc. Nephrol. 2005, 16, 3365–3370. [Google Scholar] [CrossRef] [PubMed]
- Kerr, M.; Bedford, M.; Matthews, B.; O’Donoghue, D. The economic impact of acute kidney injury in England. Nephrol. Dial. Transplant. 2014, 29, 1362–1368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, E.G.; Bagshaw, S.M. Unnecessary Renal Replacement Therapy for Acute Kidney Injury is Harmful for Renal Recovery. Semin. Dial. 2015, 28, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Jo, S.K.; Rosner, M.H.; Okusa, M.D. Pharmacologic Treatment of Acute Kidney Injury: Why Drugs Haven’t Worked and What Is on the Horizon. Clin. J. Am. Soc. Nephrol. 2007, 2, 356–365. [Google Scholar] [CrossRef] [PubMed]
- Perazella, M.A. Renal vulnerability to drug toxicity. Clin. J. Am. Soc. Nephrol. 2009, 4, 1275–1283. [Google Scholar] [CrossRef] [PubMed]
- Ozkok, S.; Ozkok, A. Contrast-induced acute kidney injury: A review of practical points. World J. Nephrol. 2017, 6, 86–99. [Google Scholar] [CrossRef] [PubMed]
- Aycock, R.D.; Westafer, L.M.; Boxen, J.L.; Majlesi, N.; Schoenfeld, E.M.; Bannuru, R.R. Acute kidney injury after computed tomography: A meta-analysis. Ann. Emerg. Med. 2018, 71, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Stewart, J.; Findlay, G.; Smith, N.; Kelly, K.; Mason, M. Adding Insult to Injury: A Review of the Care of Patients Who Died in Hospital with a Primary Diagnosis of Acute Kidney Injury (Acute Renal Failure); National Confidential Enquiry into Patient Outcome and Death: London, UK, 2009. [Google Scholar]
- Handler, S.M.; Kane-Gill, S.L.; Kellum, J.A. Optimal and early detection of acute kidney injury requires effective clinical decision support systems. Nephrol. Dial. Transplant. 2014, 29, 1802–1803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirkendall, E.S.; Spires, W.L.; Mottes, T.A.; Schaffzin, J.K.; Barclay, C.; Goldstein, S.L. Development and perfmance of acute kidney injury triggers to identuify pediatric patients at risk for nephrotoxic medication-associated harm. Appl. Clin. Inform. 2014, 5, 313–333. [Google Scholar] [PubMed]
- Porter, C.J.; Jurrlink, I.; Bisset, L.H.; Bavakunji, R.; Mehta, R.L.; Devonald, M.A. A real-time electronic alert to improve detection of acute kidney injury in a large teaching hospital. Nephrol. Dial. Transplant. 2014, 29, 1888–1893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, F.P.; Shashaty, M.; Testani, J. Automated, electronic alerts for acute kidney injury: A single-blind, parallel-group, randomised controlled trial. Lancet 2015, 385, 1966–1974. [Google Scholar] [CrossRef]
- Lachance, P.; Villeneuve, P.-M.; Rewa, O.G.; Wilson, F.P.; Selby, N.M.; Featherstone, R.M.; Bagshaw, S.M. Association between e-alert implementation for detection of acute kidney injury and outcomes: A systematic review. Nephrol. Dial. Transplant. 2017, 32, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Laing, C. On the alert for outcome improvement in acute kidney injury. Lancet 2015, 385, 1924–1926. [Google Scholar] [CrossRef]
- About Our Hospital. Available online: http://www.ottawahospital.on.ca/en/about-us (accessed on 20 November 2017).
- Kidney Disease Improving Global Outcomes (KDIGO); Acute Kidney Injury Work Group. KDIGO Clinical Practice Guidelines for Acute Kidney Injury. Nephron Clin. Pract. 2012, 120, c179–c184. [Google Scholar]
- Ricci, Z.; Cruz, D.N.; Ronco, C. Classification and staging of acute kidney injury: Beyond the RIFLE and AKIN criteria. Nat. Rev. Nephrol. 2011, 7, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Harel, Z.; Wald, R.; Liu, J.J.; Bell, C.M. Lapses in safety in end-stage renal disease patients admitted to surgical services. Hemodial. Int. 2012, 16, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Soares, D.M.; Pessanha, J.F.; Sharma, A.; Brocca, A.; Ronco, C. Delayed Nephrology Consultation and High Mortality on Acute Kidney Injury: A. Meta-Analysis. Blood Purif. 2017, 43, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Meier, P.; Bonfils, R.M.; Vogt, B.; Burnand, B.; Burnier, M. Referral Patterns and Outcomes in Noncritically Ill Patients with Hospital-Acquired Acute Kidney Injury. Clin. J. Am. Soc. Nephrol. 2011, 6, 2215–2225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- E Silva, V.T.C.; Liaño, F.; Muriel, A.; Díez, R.; de Castro, I.; Yu, L. Nephrology Referral and Outcomes in Critically Ill Acute KIdney Injury Patients. PLoS ONE 2013, 8, e70482. [Google Scholar]
- Ponce, D.; Zorzenon, C.D.P.F.; Santos, N.Y.D.; Balbi, A.L. Early nephrology consultation can have an impact on outcome of acute kidney injury patients. Nephrol. Dial. Transplant. 2011, 26, 3202–3206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balasubramanian, G.; Al-Aly, Z.; Moiz, A.; Rauchman, M.; Zhang, Z.; Gopalakrishnan, R.; Balasubramanian, S.; El-Achkar, T.M. Early nephrologist involvement in hospital-acquired acute kidney injury: A pilot study. Am. J. Kidney Dis. 2011, 57, 228–234. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Mean age in years (SD) | 65.5 (+/− 15.4) |
| Male sex, n (%) | 50 (62) |
| Mean baseline serum creatinine in mg/dL (SD) | 1.6 (+/− 0.9) |
| Co-morbidities, n (%) | |
| Hypertension | 54 (68) |
| Diabetes mellitus | 47 (59) |
| Chronic kidney disease | 43 (54) |
| Congestive heart failure | 33 (41) |
| Peripheral vascular disease | 13 (16) |
| Home medications, n (%) | |
| Thiazide diuretic or furosemide | (54) |
| ACEi or ARB | (50) |
| Metformin | (23) |
| Spironolactone | (15) |
| Admission diagnoses * | |
| Sepsis | 26 (33) |
| Congestive heart failure | 17 (21) |
| Acute coronary syndrome | 14 (18) |
| Acute kidney injury | 15 (19) |
| Malignancy | 8 (10) |
| Hospitalization and outcomes | |
| Admitted upon hospital transfer, n (%) | (23.7) |
| Median hospital length of stay, days (IQR) | 28.0 (16.3–53.5) |
| In-hospital mortality, n (%) | (26.2) |
| AKI present at admission, n (%) | 40 (50.0) |
| Median time from admission to AKI, days (IQR) | 4.5 (2.0–11.2) |
| Median time from AKI to Nephrology consult, days (IQR) | 3.0 (1.0–5.7) |
| Median time from AKI to first hemodialysis, days (IQR) | 6.0 (4.0–11.0) |
| Tests and initial management, n (%) | |
| IV fluid administration within 24 h for pre-renal AKI, n = 35 | 29 (83) |
| Urinalysis and routine microscopy | 61 (76) |
| Renal ultrasound | 53 (66) |
| Urine electrolytes | 45 (56) |
| Medications, n (%) | |
| ACEi or ARB | 16 (20) |
| Spironolactone | 11 (14) |
| NSAIDs | 1 (1) |
| Aminoglycoside antibiotic | 1 (1) |
| Contrast exposure, n (%) | 24 (30) |
| Intravenous | 15 (19) |
| Intra-arterial | 9 (11) |
| Occurrence of hyperkalemia (n = 80), n (%) | |
| During admission, after AKI | 33 (41) |
| As an indication for dialysis | 28 (35) |
| Safety lapses in patients with hyperkalemia as a subsequent indication for hemodialysis (n = 28), n (%) | |
| Low potassium diet not ordered | 13 (46) |
| Oral potassium supplements given while serum potassium ≥ 5.0 mmol/L | 2 (7) |
| ACEi, ARB and/or spironolactone given while serum potassium ≥ 5.0 mmol/L | 6 (21) |
| Admission Diagnoses | Indication(s) for HD | Summary of Events after AKI and Prior to Initiation of HD |
|---|---|---|
| Lymphoma, AKI | Hyperkalemia, Volume overload |
|
| Sepsis, NSTEMI and AKI | Volume overload |
|
| NSTEMI, then AKI * | Volume overload Hyperkalemia |
|
| Anemia, AKI | Respiratory failure |
|
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Douvris, A.; Zeid, K.; Hiremath, S.; Brown, P.A.; Sood, M.M.; Abou Arkoub, R.; Malhi, G.; Clark, E.G. Safety Lapses Prior to Initiation of Hemodialysis for Acute Kidney Injury in Hospitalized Patients: A Patient Safety Initiative. J. Clin. Med. 2018, 7, 317. https://doi.org/10.3390/jcm7100317
Douvris A, Zeid K, Hiremath S, Brown PA, Sood MM, Abou Arkoub R, Malhi G, Clark EG. Safety Lapses Prior to Initiation of Hemodialysis for Acute Kidney Injury in Hospitalized Patients: A Patient Safety Initiative. Journal of Clinical Medicine. 2018; 7(10):317. https://doi.org/10.3390/jcm7100317
Chicago/Turabian StyleDouvris, Adrianna, Khalid Zeid, Swapnil Hiremath, Pierre Antoine Brown, Manish M. Sood, Rima Abou Arkoub, Gurpreet Malhi, and Edward G. Clark. 2018. "Safety Lapses Prior to Initiation of Hemodialysis for Acute Kidney Injury in Hospitalized Patients: A Patient Safety Initiative" Journal of Clinical Medicine 7, no. 10: 317. https://doi.org/10.3390/jcm7100317