Moderating Effect of Insulin Resistance on the Relationship between Gray Matter Volumes and Cognitive Function

 , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Participants
2.2. Measures
2.2.1. Insulin Resistance and Homeostasis Model Assessment of Insulin Resistance
2.2.2. Cognitive Assessment
2.3. Brain Imaging Analysis
2.4. Statistical Analyses
3. Results
3.1. Demographic and Clinical Characteristics of Participants
3.2. Structural Changes in the Brain Associated with Insulin Resistance Exposure
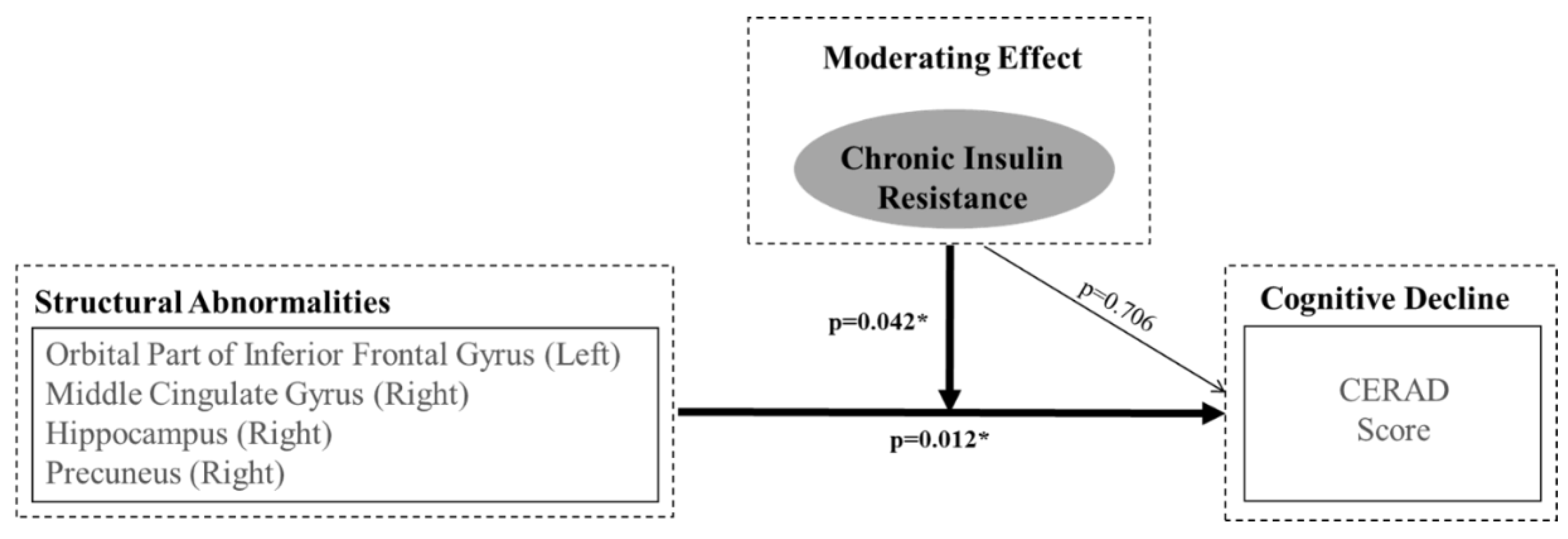
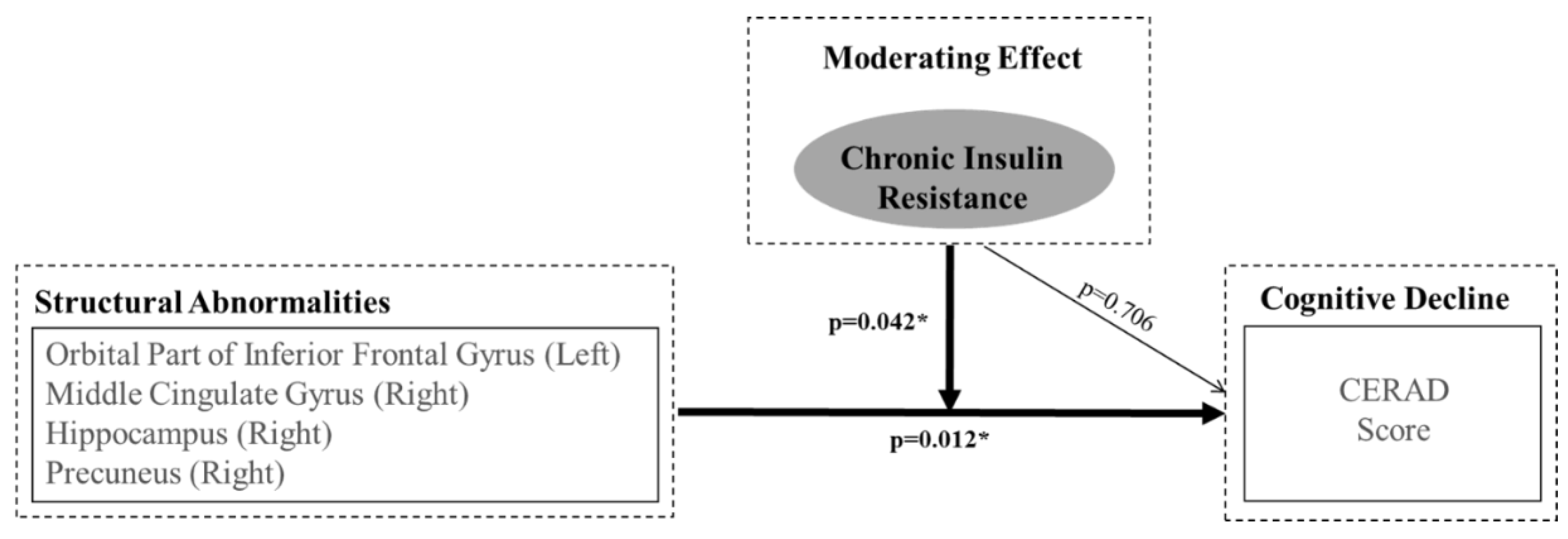
3.3. Moderating Effects of Insulin Resistance on the Relationship between Neuropathological Variations in Key Brain Regions Sensitive to Insulin and Cognitive Deterioration
4. Discussion
5. Conclusion
Author Contributions
Funding
Conflicts of interest
References
- Muntoni, S.; Muntoni, S. Insulin resistance: Pathophysiology and rationale for treatment. Ann. Nutr. Metab. 2011, 58, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Reaven, G.M. Role of insulin resistance in human disease. Diabetes 1988, 37, 1595–1607. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, G. Insulin and insulin resistance. Clin. Biochem. Rev. 2005, 26, 19–39. [Google Scholar] [PubMed]
- Arnold, S.E.; Arvanitakis, Z.; Macauley-Rambach, S.L.; Koenig, A.M.; Wang, H.-Y.; Ahima, R.S.; Craft, S.; Gandy, S.; Buettner, C.; Stoeckel, L.E.; et al. Brain insulin resistance in type 2 diabetes and alzheimer disease: Concepts and conundrums. Nat. Rev. Neurol. 2018, 14, 168–181. [Google Scholar] [CrossRef] [PubMed]
- Craft, S.; Watson, G.S. Insulin and neurodegenerative disease: Shared and specific mechanisms. Lancet Neurol. 2004, 3, 169–178. [Google Scholar] [CrossRef]
- Lester-Coll, N.; Rivera, E.J.; Soscia, S.J.; Doiron, K.; Wands, J.R.; de la Monte, S.M. Intracerebral streptozotocin model of type 3 diabetes: Relevance to sporadic alzheimer’s disease. J. Alzheimers Dis. 2006, 9, 13–33. [Google Scholar] [CrossRef] [PubMed]
- Rasgon, N.L.; Kenna, H.A.; Wroolie, T.E.; Kelley, R.; Silverman, D.; Brooks, J.; Williams, K.E.; Powers, B.N.; Hallmayer, J.; Reiss, A. Insulin resistance and hippocampal volume in women at risk for alzheimer’s disease. Neurobiol. Aging 2011, 32, 1942–1948. [Google Scholar] [CrossRef] [PubMed]
- Convit, A.; Wolf, O.T.; Tarshish, C.; De Leon, M.J. Reduced glucose tolerance is associated with poor memory performance and hippocampal atrophy among normal elderly. Proc. Natl. Acad. Sci. USA 2003, 100, 2019–2022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willette, A.A.; Xu, G.; Johnson, S.C.; Birdsill, A.C.; Jonaitis, E.M.; Sager, M.A.; Hermann, B.P.; La Rue, A.; Asthana, S.; Bendlin, B.B. Insulin resistance, brain atrophy, and cognitive performance in late middle-aged adults. Diabetes Care 2013, 36, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Vanhanen, M.; Koivisto, K.; Moilanen, L.; Helkala, E.; Hänninen, T.; Soininen, H.; Kervinen, K.; Kesäniemi, Y.; Laakso, M.; Kuusisto, J. Association of metabolic syndrome with alzheimer disease: A population-based study. Neurology 2006, 67, 843–847. [Google Scholar] [CrossRef] [PubMed]
- García-Lara, J.M.A.; Aguilar-Navarro, S.; Gutiérrez-Robledo, L.M.; Ávila-Funes, J.A. The metabolic syndrome, diabetes, and alzheimer’s disease. Rev. Investig. Clin. 2010, 62, 343–349. [Google Scholar] [PubMed]
- Benedict, C.; Brooks, S.J.; Kullberg, J.; Burgos, J.; Kempton, M.J.; Nordenskjöld, R.; Nylander, R.; Kilander, L.; Craft, S.; Larsson, E.-M.; et al. Impaired insulin sensitivity as indexed by the homa score is associated with deficits in verbal fluency and temporal lobe gray matter volume in the elderly. Diabetes Care 2012, 35, 488–494. [Google Scholar] [CrossRef] [PubMed]
- Forti, P.; Pisacane, N.; Rietti, E.; Lucicesare, A.; Olivelli, V.; Mariani, E.; Mecocci, P.; Ravaglia, G. Metabolic syndrome and risk of dementia in older adults. J. Am. Geriatr. Soc. 2010, 58, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Ohara, T.; Doi, Y.; Ninomiya, T.; Hirakawa, Y.; Hata, J.; Iwaki, T.; Kanba, S.; Kiyohara, Y. Glucose tolerance status and risk of dementia in the community the hisayama study. Neurology 2011, 77, 1126–1134. [Google Scholar] [CrossRef] [PubMed]
- Katsuki, A.; Sumida, Y.; Gabazza, E.C.; Murashima, S.; Furuta, M.; Araki-Sasaki, R.; Hori, Y.; Yano, Y.; Adachi, Y. Homeostasis model assessment is a reliable indicator of insulin resistance during follow-up of patients with type 2 diabetes. Diabetes Care 2001, 24, 362–365. [Google Scholar] [CrossRef] [PubMed]
- Neergaard, J.S.; Dragsbæk, K.; Christiansen, C.; Nielsen, H.B.; Brix, S.; Karsdal, M.A.; Henriksen, K. Metabolic syndrome, insulin resistance and cognitive dysfunction: Does your metabolic profile affect your brain? Diabetes 2017, db161444. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.K.; Vidoni, E.D.; Honea, R.A.; Burns, J.M.; Initiative, A.s.D.N. Impaired glycemia increases disease progression in mild cognitive impairment. Neurobiol. Aging 2014, 35, 585–589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geijselaers, S.L.; Sep, S.J.; Schram, M.T.; van Boxtel, M.P.; Henry, R.M.; Verhey, F.R.; Kroon, A.A.; Schaper, N.C.; Dagnelie, P.C.; van der Kallen, C.J. Insulin resistance and cognitive performance in type 2 diabetes—The maastricht study. J. Diabetes Complicat. 2017, 31, 824–830. [Google Scholar] [CrossRef] [PubMed]
- Tiehuis, A.; Mali, W.T.M.; Van Raamt, A.; Visseren, F.; Biessels, G.; van Zandvoort, M.; Kappelle, L.; van der Graaf, Y.; Group, S.S. Cognitive dysfunction and its clinical and radiological determinants in patients with symptomatic arterial disease and diabetes. J. Neurol. Sci. 2009, 283, 170–174. [Google Scholar] [CrossRef] [PubMed]
- Imamine, R.; Kawamura, T.; Umemura, T.; Umegaki, H.; Kawano, N.; Hotta, M.; Kouchi, Y.; Hatsuda, S.; Watarai, A.; Kanai, A. Does cerebral small vessel disease predict future decline of cognitive function in elderly people with type 2 diabetes? Diabetes Res. Clin. Pract. 2011, 94, 91–99. [Google Scholar] [CrossRef] [PubMed]
- McKhann, G.; Drachman, D.; Folstein, M.; Katzman, R.; Price, D.; Stadlan, E.M. Clinical diagnosis of alzheimer’s disease report of the nincds-adrda work group* under the auspices of department of health and human services task force on alzheimer’s disease. Neurology 1984, 34, 939. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.; Hosker, J.; Rudenski, A.; Naylor, B.; Treacher, D.; Turner, R. Homeostasis model assessment: Insulin resistance and β-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Lillioja, S.; Mott, D.M.; Howard, B.V.; Bennett, P.H.; Yki-Järvinen, H.; Freymond, D.; Nyomba, B.L.; Zurlo, F.; Swinburn, B.; Bogardus, C. Impaired glucose tolerance as a disorder of insulin action. N. Engl. J. Med. 1988, 318, 1217–1225. [Google Scholar] [CrossRef] [PubMed]
- Warram, J.H.; Martin, B.C.; Krolewski, A.S.; Soeldner, J.S.; Kahn, C.R. Slow glucose removal rate and hyperinsulinemia precede the development of type ii diabetes in the offspring of diabetic parents. Ann. Intern. Med. 1990, 113, 909–915. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Lee, K.U.; Lee, D.Y.; Kim, K.W.; Jhoo, J.H.; Kim, J.H.; Lee, K.H.; Kim, S.Y.; Han, S.H.; Woo, J.I. Development of the Korean version of the consortium to establish a registry for alzheimer’s disease assessment packet (CERAD-K): Clinical and neuropsychological assessment batteries. J. Gerontol. B Psychol. Sci. Soc. Sci. 2002, 57, P47–53. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.Y.; Lee, K.U.; Lee, J.H.; Kim, K.W.; Jhoo, J.H.; Youn, J.C.; Kim, S.Y.; Woo, S.I.; Woo, J.I. A normative study of the mini-mental state examination in the Korean elderly. J. Neuropsychiatr. Assoc. 2002, 41, 508–525. [Google Scholar]
- Ekblad, L.L.; Rinne, J.O.; Puukka, P.; Laine, H.; Ahtiluoto, S.; Sulkava, R.; Viitanen, M.; Jula, A. Insulin resistance predicts cognitive decline: An 11-year follow-up of a nationally representative adult population sample. Diabetes Care 2017, 40, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Markus, M.; Ittermann, T.; Wittfeld, K.; Schipf, S.; Siewert-Markus, U.; Bahls, M.; Bülow, R.; Werner, N.; Janowitz, D.; Baumeister, S. Prediabetes is associated with lower brain gray matter volume in the general population. The study of health in pomerania (ship). Nutr. Metab. Cardiovasc. Dis. 2017, 27, 1114–1122. [Google Scholar] [CrossRef] [PubMed]
- Baskin, D.G.; Figlewicz, D.P.; Woods, S.C.; Porte, D., Jr.; Dorsa, D.M. Insulin in the brain. Annu. Rev. Physiol. 1987, 49, 335–347. [Google Scholar] [CrossRef] [PubMed]
- Unger, J.W.; Livingston, J.N.; Moss, A.M. Insulin receptors in the central nervous system: Localization, signalling mechanisms and functional aspects. Prog. Neurobiol. 1991, 36, 343–362. [Google Scholar] [CrossRef]
- McDonald, C.; McEvoy, L.; Gharapetian, L.; Fennema-Notestine, C.; Hagler, D.; Holland, D.; Koyama, A.; Brewer, J.; Dale, A. Regional rates of neocortical atrophy from normal aging to early alzheimer disease. Neurology 2009, 73, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Burns, J.M.; Honea, R.A.; Vidoni, E.D.; Hutfles, L.J.; Brooks, W.M.; Swerdlow, R.H. Insulin is differentially related to cognitive decline and atrophy in alzheimer’s disease and aging. BBA-Mol. Basis Dis. 2012, 1822, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Risacher, S.L.; Huang, E.; Saykin, A.J.; Weiner, M.W.; Aisen, P.; Petersen, R.; Jack, C.R.; Jagust, W.; Trojanowki, J.Q. Type 2 diabetes mellitus is associated with brain atrophy and hypometabolism in the adni cohort. Neurology 2016. [Google Scholar] [CrossRef] [PubMed]
- Ishibashi, K.; Onishi, A.; Fujiwara, Y.; Ishiwata, K.; Ishii, K. Effects of glucose, insulin, and insulin resistance on cerebral 18f-fdg distribution in cognitively normal older subjects. PLoS ONE 2017, 12, e0181400. [Google Scholar] [CrossRef] [PubMed]
- Byun, M.S.; Kim, H.J.; Yi, D.; Choi, H.J.; Baek, H.; Lee, J.H.; Choe, Y.M.; Sohn, B.K.; Lee, J.-Y.; Lee, Y. Differential effects of blood insulin and hba1c on cerebral amyloid burden and neurodegeneration in nondiabetic cognitively normal older adults. Neurobiol. Aging 2017, 59, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Van der Heide, L.P.; Ramakers, G.M.; Smidt, M.P. Insulin signaling in the central nervous system: Learning to survive. Prog. Neurobiol. 2006, 79, 205–221. [Google Scholar] [CrossRef] [PubMed]
- De la Monte, S.M. Insulin resistance and alzheimer’s disease. BMB Rep. 2009, 42, 475–481. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Categories | Mean (Standard Deviation or Number (%)) |
|---|---|
| Age (years) | 74.28 (6.74) |
| Sex (male/female) | 48/112 (28.9/67.5) |
| Education (years) | 7.87 (4.95) |
| Diabetes Mellitus | |
| DM (N, %) | 51 (30.7) |
| Prediabetes (N, %) | 80 (48.2) |
| Non-DM (N, %) | 29 (17.5) |
| HbA1c (%) | 6.24 (1.03) |
| Fasting Blood Sugar (mg/dL) | 112.18 (31.96) |
| Fasting Insulin (mIU/L) | 9.27 (5.79) |
| HOMA-IR | 2.63 (1.96) |
| Total cholesterol (mg/dL) | 181.9 (38.89) |
| HDL-cholesterol (mg/dL) | 50.41 (16.86) |
| Triglycerides | 122.69 (75.04) |
| Dementia | |
| Non-Dementia | 82 (50.25) |
| AD | 78 (48.75) |
| MMSE | 21.13 (5.51) |
| CERAD | 48.59 (17.24) |
| TIV (VBM) | 1.56 (0.13) |
| Dependent Variable | b | t | p |
|---|---|---|---|
| Brain Region | |||
| Left orbital part of inferior frontal gyrus | −0.012 | 1.979 | 0.052 |
| Right orbital part of inferior frontal gyrus | −0.018 | 2.256 | 0.027 |
| Left anterior cingulate gyrus | −0.006 | 0.907 | 0.367 |
| Right anterior cingulate gyrus | −0.012 | 1.714 | 0.091 |
| Left middle cingulate | −0.019 | 2.705 | 0.009 |
| Right middle cingulate | −0.013 | 2.035 | 0.046 |
| Left posterior cingulate gyrus | −0.015 | 1.770 | 0.081 |
| Right posterior cingulate gyrus | −0.014 | 2.286 | 0.025 |
| Left hippocampus | −0.010 | 1.831 | 0.071 |
| Right hippocampus | −0.014 | 2.393 | 0.019 |
| Left parahippocampal gyrus | 0.079 | 0.910 | 0.366 |
| Right parahippocampal gyrus | −0.017 | 2.139 | 0.036 |
| Left precuneus | −0.010 | 2.000 | 0.049 |
| Right precuneus | −0.009 | 1.928 | 0.058 |
| Coefficients | R2 | b | β | p |
|---|---|---|---|---|
| (constant) | 0.526 | 32.056 | 0.031 | |
| Age | −0.126 | −0.155 | 0.017 | |
| Gender | −0.184 | −0.015 | 0.961 | |
| Education | 0.614 | 0.553 | <0.001 | |
| Total intracranial volume | −3.540 | −0.084 | 0.774 | |
| Left orbital part of inferior frontal gyrus | 24.130 | 0.163 | 0.249 | |
| Right orbital part of inferior frontal gyrus | 28.515 | 0.176 | 0.043 | |
| Left anterior cingulate gyrus | −3.883 | −0.031 | 0.181 | |
| Right anterior cingulate gyrus | 20.603 | 0.163 | 0.017 | |
| Left middle cingulate | 97.188 | 0.608 | 0.017 | |
| Right middle cingulate | 81.576 | 0.532 | 0.020 | |
| Left posterior cingulate gyrus | 18.788 | 0.120 | 0.396 | |
| Right posterior cingulate gyrus | −24.494 | −0.145 | 0.797 | |
| Left hippocampus | 8.727 | 0.080 | 0.468 | |
| Right hippocampus | 77.891 | 0.669 | 0.039 | |
| Left parahippocampal gyrus | 7.829 | 0.074 | 0.272 | |
| Right parahippocampal gyrus | 60.357 | 0.554 | 0.014 | |
| Left precuneus | 15.296 | 0.088 | 0.087 | |
| Right precuneus | 27.050 | 0.166 | 0.221 | |
| HOMA-IR | 0.895 | 0.067 | 0.471 | |
| (Left orbital part of inferior frontal gyrus) × (HOMA-IR) | −160.049 | −0.445 | 0.014 | |
| (Right orbital part of inferior frontal gyrus) × (HOMA-IR) | −97.260 | −0.219 | 0.316 | |
| (Left anterior cingulate gyrus) × (HOMA-IR) | −7.900 | −0.031 | 0.489 | |
| (Right anterior cingulate gyrus) × (HOMA-IR) | −115.485 | −0.364 | 0.281 | |
| (Left middle cingulate) × (HOMA-IR) | −161.328 | −0.532 | 0.177 | |
| (Right middle cingulate)×(HOMA-IR) | −293.304 | −0.881 | 0.047 | |
| (Left posterior cingulate gyrus)×(HOMA-IR) | 0.849 | 0.002 | 0.489 | |
| (Right posterior cingulate gyrus)×(HOMA-IR) | 11.730 | 0.033 | 0.422 | |
| (Left hippocampus) × (HOMA-IR) | 125.596 | 0.413 | 0.414 | |
| (Right hippocampus) × (HOMA-IR) | −216.084 | −0.671 | 0.099 | |
| (Left parahippocampal gyrus) × (HOMA-IR) | −24.386 | −0.085 | 0.518 | |
| (Right parahippocampal gyrus) × (HOMA-IR) | −133.345 | −0.430 | 0.654 | |
| (Left precuneus) × (HOMA-IR) | −65.383 | −0.142 | 0.366 | |
| (Right precuneus) × (HOMA-IR) | −98.985 | −0.264 | 0.095 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.; Kim, J.; Shin, S.A.; Park, S.; Yoon, D.H.; Kim, H.; Kim, Y.K.; Moon, M.K.; Koo, B.K.; Lee, J.-Y. Moderating Effect of Insulin Resistance on the Relationship between Gray Matter Volumes and Cognitive Function. J. Clin. Med. 2018, 7, 413. https://doi.org/10.3390/jcm7110413
Lee J, Kim J, Shin SA, Park S, Yoon DH, Kim H, Kim YK, Moon MK, Koo BK, Lee J-Y. Moderating Effect of Insulin Resistance on the Relationship between Gray Matter Volumes and Cognitive Function. Journal of Clinical Medicine. 2018; 7(11):413. https://doi.org/10.3390/jcm7110413
Chicago/Turabian StyleLee, Jiyeon, Jihyeon Kim, Seong A Shin, Soowon Park, Dong Hyun Yoon, Hongrae Kim, Yu Kyeong Kim, Min Kyong Moon, Bo Kyung Koo, and Jun-Young Lee. 2018. "Moderating Effect of Insulin Resistance on the Relationship between Gray Matter Volumes and Cognitive Function" Journal of Clinical Medicine 7, no. 11: 413. https://doi.org/10.3390/jcm7110413