Pregnancy in Chronic Kidney Disease: Need for Higher Awareness. A Pragmatic Review Focused on What Could Be Improved in the Different CKD Stages and Phases

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Chronic Kidney Disease
2.1. State of the Art: What We Know on the CKD-Pregnancy Relationship: CKD Stages
2.2. A Particular Case: Systemic Immunologic Diseases
2.3. What is Missing, and What We Still Need to Know
3. Dialysis
3.1. The State of the Art
3.2. What Is Missing and Could Be Done in the Clinical Practice
4. Kidney Transplantation
What Is Missing and Could Be Done in the Clinical Practice
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Drug | Main Features | FDA |
|---|---|---|
| Usually considered as relatively safe, when absolutely needed | ||
| Azathioprine (AZA) | It is teratogenic in animal models, at high doses, but not in humans, possibly because the foetal liver is not able to activate the drug. KDIGO and European Best Practice Guidelines suggest switch from Mycophenolate to AZA before pregnancy. | D |
| Cyclosporine A (CyA) | Hypertension, hyperglycaemia and nephrotoxicity may be relevant in pregnancy. CyA has not been associated with teratogenicity; SGA babies and preterm delivery have been reported, with an unclear link with maternal disease; levels vary in pregnancy and need strict monitoring. | C |
| Tacrolimus | The drug has similar effects and side effects as CyA; the experience is more limited than with CyA. | C |
| Steroids | The most frequently used short-acting corticosteroids are prednisone, methylprednisolone and prednisolone; among long-acting betamethasone and desamethasone. No major malformation reported, increase of labio-palatoschisis is debated. A risk of premature rupture of membranes has been reported, along with increased risk of infection and gestational diabetes. | C prednisone |
| Hydroxychloroquine | This synthetic antimalaric agent crosses the placenta but was not associated with foetal toxicity. | B |
| IV Immunoglobulin (IV Ig) | IV Ig is indicated in SLE pregnant patients with recurrent spontaneous abortion. Safety has not been fully established. | C |
| Rituximab | Animal studies have shown adverse effects on the fetus; no adequate studies in humans. Benefit may warrant use in highly selected cases. | C |
| Belimumab | In exceptional cases. No adequate studies in humans. Benefit may warrant use despite potential risks, in highly selected cases. | C |
| To be avoided | ||
| Cyclophosphamide | Reports suggest that pregnancy termination is common in case of inadvertent use. A few positive reports, mainly in SLE are available. | D |
| Methotrexate | Also employed for extrauterine pregnancy termination. Discontinuation for one–three menstrual cycles pre-conception is usually indicated. | X |
| Mycophenolate | Severe foetal malformations are reported, mainly cardiovascular and cranial. Discontinuation for at lest 6 months, also for stabilizing the kidney function, is usually indicted after kidney transplantation. | D |
| m-Tor inhibitors | Very few studies regard their use in pregnancy. They are teratogenic in animals; discontinuation in humans is matter of debate; KDIGO guidelines suggest discontinuation in prevision of pregnancy. | C |
| Thymoglobulin | Animal studies are not available. There are no controlled data in human pregnancy. | NA |
| Basiliximab | Animal studies failed to reveal embryotoxicity, or teratogenicity. IgG are cross the placental barrier and the IL-2 receptor plays an important role in development of the immune system. There are no controlled data in human pregnancy. | B |
| Alemtuzumab | In animal studies no teratogenic effects are observed. However, there was an increase in embryolethality in pregnant animals. There are no controlled data in human pregnancy, but potential benefits may warrant use of the drug in selected pregnant women despite potential risks. | C |
| Drug | Main Features | FDA |
|---|---|---|
| Usually considered as first choice | ||
| Alpha-methyldopa | Widely used in pregnancy, with no reported negative effects. May not be sufficient to correct severe hypertension in CKD. | B |
| Niphedipine | The long acting form is commonly used. In CKD the side effect of increasing peripheral oedema may be relevant. | C |
| Labetalol | Usually well tolerated, should be avoided in asthma. In a RCT it was comparable to alpha-methyldopa. | C |
| Usually considered as second choices | ||
| Beta-blockers | The main negative effect in older studies was foetal growth restriction, possibly as an effect of overzealous correction of BP. Beta1 selective beta-blockers (atenolol) are more often in cause. May be more effective than alpha-methyldopa, alone or in combined therapy. At delivery they may induce hypoglycaemia, hypotension and bradycardia (usually mild and transient). | D atenolol B pindolol C metoprol |
| Clonidine | The effect is similar to alpha-methyldopa; side effects may be more common and hypertensive rebounds at discontinuation are common; slowing fetal growth is occasionally reported. | C |
| Diuretics | They are usually avoided in pregnancy except for cardiological indications. Thiazides may be continued in patients previously on treatment. In Gitelman syndrome, аmiloride may be needed. | B hydrocloro-thiazide |
| To be avoided | ||
| Niphedipine short acting | Contraindicated by FDA, RCOG and AIPE for the risk of severe sudden hypotension with detrimental effect on placental flows. | X |
| ACE-i/ARBs and related drugs | Both are contraindicated in all phases of pregnancy; different malformations, involging cardiovascular, central nervous system, renal and bone are reported. Recent studies suggest that the risk is limited to the second and third trimester. | X |
| Drug | Main Features | FDA |
|---|---|---|
| Usually considered as first or second choices | ||
| Ampi-amoxycillin | Ampicillin and Amoxicillin are the first-choice antibiotics. | B |
| Clavulanic acid | Indicated when therapy with the previous ones is not effective, or according to antibiogramme. | B |
| Cephalosporins | Available data do not indicate an increase of malformations; risk for kernicterus is increased (mainly ceftriaxone). | B |
| Carbapenems | Meropenem is the first choice in severe infection; no demonstrated risks in humans; increased risk of malformations with imipenem-cilastatin in animals. | B |
| Aztreonam | Alternative in case of allergy to beta-lactams (parenteral only). | B |
| Macrolides | Eritromicine is a good alternative in case of contraindication to beta-lactamics. Claritromicine and azitromicine are a second choice. | B |
| Phosphomycin | Indicated in uncomplicated urinary tract-infections. | B |
| Nitrofurantoin | Contraindicated in G6PDH-deficiency. Contraindicated at the end of the pregnancy for risk of haemolytic anaemia in the new-born. | B |
| To be avoided (except when lifesaving) | ||
| Aminoglycosides | Associated with ototoxicity in the foetus and newborn. | D |
| Fluoroquinolones | Associated with abnormalities in the development of cartilages in animal studies | C |
| Tetracycline | Cause of various bone abnormalities. | D |
| Sulphonamides | Sulfamethoxazole/trimethoprim is a folic acid antagonist that increases the risk of kernicterus. | D |
| Drug | Main Features | FDA |
|---|---|---|
| Usually considered as relatively safe, when absolutely needed | ||
| Acetylsalicylate | At low doses may protect against pre-eclampsia; discontinuation before delivery is recommended. | A |
| Low molecular weight heparin | Do not cross the placenta. Safe for prophylaxis and treatment of thromboembolic complications in pregnancy and post-partum. | B |
| ESAs | Do not cross the placenta and are considered safe; there may a need to increase doses in pregnancy. | Not assigned |
| Allopurinol | Crosses the placenta. Animal reproduction studies have shown potential adverse effects on the fetus. No adequate studies in humans. Potential benefits may warrant use of in pregnant women despite potential risks. | C |
| Vitamin D | No advantage when given regardless of blood levels Vitamin D3 is recommended to correct deficiency. Cholecalciferol crosses the placenta but the transfer to the fetus is low; no evidence of adverse effects. Calcitriol, paricalcitol are teratogenic in animal studies. Animal studies have shown adverse effects of Ergocalciferol on the fetus. No adequate study in humans. | Not assigned Cholecalciferol C Ergocalciferol |
| Iron supplements | Multivitamin with iron is only recommended for use in pregnancy when benefit outweighs risk. Ferrous sulfate use is the most frequently used. Maternal anemia increases the risk of low birth-weight, premature delivery, and impaired cognitive development. Recent studies have linked high serum iron with an increased risk of gestational diabetes | A Multivitamin with iron Not assigned Ferrous sulfate |
| Sodium bicarbonate | No animal or human data availale. Sodium bicarbonate should only be given during pregnancy when benefit outweighs risk | C |
| Calcium carbonate | Malformation risk is unlikely in humans. In some patients, permanent hypercalcemia resulted in adverse effects on the fetus. No available data in humans. Low intake is associated with adverse pregnancy events. | Not assigned |
| To be avoided | ||
| Warfarin | Evidence of teratogenicity in animal studies. In humans, exposure during the first trimester caused congenital malformations in about 5% of the exposed. Mental retardation, blindness, schizencephaly, microcephaly, hydrocephalus, and other adverse pregnancy outcomes have been reported following exposure in the second and third trimesters. Fatal fetal hemorrhage and an increased risk of spontaneous abortion and fetal mortality are also reported. Case by case evaluation in the case of cardiac indications. | Not assigned |
| Novel anticoagulants | Animal studies show adverse effects for Rivaroxaban, Dabigatran and Edoxaban. No adequate study in humans, but potential benefits may warrant use in highly selected cases. | C |
| Calcimimetics | Animal studies show adverse effects, and there is no adequate study in humans; potential benefits may warrant use in highly selected cases. | C |
| Sevelamer | Animal studies show adverse effects, and there is no adequate study in humans; potential benefits may warrant use in highly selected cases | C |
References
- Davison, J.M.; Lindheimer, M.D. Pregnancy and chronic kidney disease. Semin. Nephrol. 2011, 31, 86–99. [Google Scholar] [CrossRef] [PubMed]
- Hall, M. Pregnancy in Women with CKD: A Success Story. Am. J. Kidney Dis. 2016, 68, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Cabiddu, G. Pregnancy and kidney disease: From medicine based on exceptions to exceptional medicine. J. Nephrol. 2017, 30, 303–305. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.J.; Ma, X.X.; Hao, L.; Liu, L.J.; Lv, J.C.; Zhang, H. A Systematic Review and Meta-Analysis of Outcomes of Pregnancy in CKD and CKD Outcomes in Pregnancy. Clin. J. Am. Soc. Nephrol. 2015, 10, 1964–1978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nevis, I.F.; Reitsma, A.; Dominic, A.; McDonald, S.; Thabane, L.; Akl, E.A.; Hladunewich, M.; Akbari, A.; Joseph, G.; Sia, W.; et al. Pregnancy outcomes in women with chronic kidney disease: A systematic review. Clin. J. Am. Soc. Nephrol. 2011, 6, 2587–2598. [Google Scholar] [CrossRef] [PubMed]
- Cabiddu, G.; Castellino, S.; Gernone, G.; Santoro, D.; Moroni, G.; Giannattasio, M.; Gregorini, G.; Giacchino, F.; Attini, R.; Loi, V.; et al. A best practice position statement on pregnancy in chronic kidney disease: The Italian Study Group on Kidney and Pregnancy. J. Nephrol. 2016, 29, 277–303. [Google Scholar] [CrossRef] [PubMed]
- Blom, K.; Odutayo, A.; Bramham, K.; Hladunewich, M.A. Pregnancy and Glomerular Disease: A Systematic Review of the Literature with Management Guidelines. Clin. J. Am. Soc. Nephrol. 2017, 12, 1862–1872. [Google Scholar] [CrossRef] [PubMed]
- August, P. Obstetric nephrology: Pregnancy and the kidney—Inextricably linked. Clin. J. Am. Soc. Nephrol. 2012, 7, 2071–2072. [Google Scholar] [CrossRef] [PubMed]
- Gianfreda, D.; Quaglini, S.; Frontini, G.; Raffiotta, F.; Messa, P.; Moroni, G. Does pregnancy have any impact on long term damage accrual and on the outcome of lupus nephritis? J. Autoimmun. 2017, 84, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Hladunewich, M.A.; Hou, S.; Odutayo, A.; Cornelis, T.; Pierratos, A.; Goldstein, M.; Tennankore, K.; Keunen, J.; Hui, D.; Chan, C.T. Intensive hemodialysis associates with improved pregnancy outcomes: A Canadian and United States cohort comparison. J. Am. Soc. Nephrol. 2014, 25, 1103–1109. [Google Scholar] [CrossRef] [PubMed]
- Webster, P.; Lightstone, L.; McKay, D.B.; Josephson, M.A. Pregnancy in chronic kidney disease and kidney transplantation. Kidney Int. 2017, 91, 1047–1056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kendrick, J.; Sharma, S.; Holmen, J.; Palit, S.; Nuccio, E.; Chonchol, M. Kidney disease and maternal and fetal outcomes in pregnancy. Am. J. Kidney Dis. 2015, 66, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Alrukhaimi, M.; Liu, Z.H.; Zakharova, E.; Levin, A.; World Kidney Day Steering Committee. What we do and do not know about women and kidney diseases; questions unanswered and answers unquestioned: Reflection on World Kidney Day and International Woman’s Day. BMC Nephrol. 2018, 19, 66. [Google Scholar] [CrossRef] [PubMed]
- Cornelis, T.; Odutayo, A.; Keunen, J.; Hladunewich, M. The kidney in normal pregnancy and preeclampsia. Semin. Nephrol. 2011, 31, 4–14. [Google Scholar] [CrossRef] [PubMed]
- Maynard, S.E.; Thadhani, R. Pregnancy and the kidney. J. Am. Soc. Nephrol. 2009, 20, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Bjornstad, P.; Cherney, D.Z.I. Kidney Function Can Predict Pregnancy Outcomes. Clin. J. Am. Soc. Nephrol. 2017, 12, 1029–1031. [Google Scholar] [CrossRef] [PubMed]
- Kattah, A.; Milic, N.; White, W.; Garovic, V. Spot urine protein measurements in normotensive pregnancies, pregnancies with isolated proteinuria and preeclampsia. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2017, 313, R418–R424. [Google Scholar] [CrossRef] [PubMed]
- August, P. Preeclampsia: A “nephrocentric” view. Adv. Chronic. Kidney Dis. 2013, 20, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Kallela, J.; Jääskeläinen, T.; Kortelainen, E.; Heinonen, S.; Kajantie, E.; Kere, J.; Kivinen, K.; Pouta, A.; Laivuori, H. The diagnosis of pre-eclampsia using two revised classifications in the Finnish Pre-eclampsia Consortium (FINNPEC) cohort. BMC Pregnancy Childbirth 2016, 16. [Google Scholar] [CrossRef] [PubMed]
- Jim, B.; Garovic, V.D. Acute Kidney Injury in Pregnancy. Semin. Nephrol. 2017, 37, 378–385. [Google Scholar] [CrossRef] [PubMed]
- Yamada, T.; Obata-Yasuoka, M.; Hamada, H.; Baba, Y.; Ohkuchi, A.; Yasuda, S.; Kawabata, K.; Minakawa, S.; Hirai, C.; Kusaka, H.; et al. Isolated gestational proteinuria preceding the diagnosis of preeclampsia—An observational study. Acta Obstet. Gynecol. Scand. 2016, 95, 1048–1054. [Google Scholar] [CrossRef] [PubMed]
- Shinar, S.; Asher-Landsberg, J.; Schwartz, A.; Ram-Weiner, M.; Kupferminc, M.J.; Many, A. Isolated proteinuria is a risk factor for pre-eclampsia: A retrospective analysis of the maternal and neonatal outcomes in women presenting with isolated gestational proteinuria. J. Perinatol. 2016, 36, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Morikawa, M.; Yamada, T.; Minakami, H. Outcome of pregnancy in patients with isolated proteinuria. Curr. Opin. Obstet. Gynecol. 2009, 21, 491–495. [Google Scholar] [CrossRef] [PubMed]
- Imbasciati, E.; Gregorini, G.; Cabiddu, G.; Gammaro, L.; Ambroso, G.; Del Giudice, A.; Ravani, P. Pregnancy in CKD stages 3 to 5: Fetal and maternal outcomes. Am. J. Kidney Dis. 2007, 49, 753–762. [Google Scholar] [CrossRef] [PubMed]
- Garg, A.X.; Nevis, I.F.; McArthur, E.; Sontrop, J.M.; Koval, J.J.; Lam, N.N.; Hildebrand, A.M.; Reese, P.P.; Storsley, L.; Gill, J.S.; et al. Gestational hypertension and preeclampsia in living kidney donors. N. Engl. J. Med. 2015, 372, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Josephson, M.A. Transplantation: Pregnancy after kidney donation: More questions than answers. Nat. Rev. Nephrol. 2009, 5, 495–497. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Attini, R.; Vasario, E.; Conijn, A.; Biolcati, M.; D’Amico, F.; Consiglio, V.; Bontempo, S.; Todros, T. Pregnancy and chronic kidney disease: A challenge in all CKD stages. Clin. J. Am. Soc. Nephrol. 2010, 5, 844–855. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Cabiddu, G.; Attini, R.; Vigotti, F.N.; Maxia, S.; Lepori, N.; Tuveri, M.; Massidda, M.; Marchi, C.; Mura, S.; et al. Risk of Adverse Pregnancy Outcomes in Women with CKD. J. Am. Soc. Nephrol. 2015, 26, 2011–2022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seeger, H.; Salfeld, P.; Eisel, R.; Wagner, C.A.; Mohebbi, N. Complicated pregnancies in inherited distal renal tubular acidosis: Importance of acid-base balance. J. Nephrol. 2017, 30, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Yefet, E.; Tovbin, D.; Nachum, Z. Pregnancy outcomes in patients with Alport syndrome. Arch. Gynecol. Obstet. 2016, 293, 739–747. [Google Scholar] [CrossRef] [PubMed]
- Hladunewich, M.A.; Kim, S.J. Kidney Donation: What Might It Mean for Women Wishing to Become Pregnant. Am. J. Kidney Dis. 2015, 66, 386–388. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, H.N.; Akkina, S.K.; Leister, E.; Gillingham, K.; Cordner, G.; Guo, H.; Bailey, R.; Rogers, T.; Matas, A.J. Pregnancy outcomes after kidney donation. Am. J. Transplant. 2009, 9, 825–834. [Google Scholar] [CrossRef] [PubMed]
- Reisaeter, A.V.; Røislien, J.; Henriksen, T.; Irgens, L.M.; Hartmann, A. Pregnancy and birth after kidney donation: The Norwegian experience. Am J Transplant. 2009, 9, 820–824. [Google Scholar] [CrossRef] [PubMed]
- Klemetti, M.M.; Laivuori, H.; Tikkanen, M.; Nuutila, M.; Hiilesmaa, V.; Teramo, K. Obstetric and perinatal outcome in type 1 diabetes patients with diabetic nephropathy during 1988–2011. Diabetologia 2015, 58, 678–686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piccoli, G.B.; Clari, R.; Ghiotto, S.; Castelluccia, N.; Colombi, N.; Mauro, G.; Tavassoli, E.; Melluzza, C.; Cabiddu, G.; Gernone, G.; et al. Type 1 diabetes, diabetic nephropathy, and pregnancy: A systematic review and meta-study. Rev. Diabet. Stud. 2013, 10, 6–26. [Google Scholar] [CrossRef] [PubMed]
- Mathiesen, E.R.; Ringholm, L.; Feldt-Rasmussen, B.; Clausen, P.; Damm, P. Obstetric nephrology: Pregnancy in women with diabetic nephropathy—The role of antihypertensive treatment. Clin. J. Am. Soc. Nephrol. 2012, 7, 2081–2088. [Google Scholar] [CrossRef] [PubMed]
- Bramham, K. Diabetic Nephropathy and Pregnancy. Semin. Nephrol. 2017, 37, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Lightstone, L.; Hladunewich, M.A. Lupus Nephritis and Pregnancy: Concerns and Management. Semin. Nephrol. 2017, 37, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Buyon, J.P.; Kim, M.Y.; Guerra, M.M.; Laskin, C.A.; Petri, M.; Lockshin, M.D.; Sammaritano, L.; Branch, D.W.; Porter, T.F.; Sawitzke, A.; et al. Predictors of pregnancy outcomes in patients with lupus: A cohort study. Ann. Intern. Med. 2015, 163, 153–163. [Google Scholar] [CrossRef] [PubMed]
- Moroni, G.; Doria, A.; Giglio, E.; Imbasciati, E.; Tani, C.; Zen, M.; Strigini, F.; Zaina, B.; Tincani, A.; Gatto, M.; et al. Maternal outcome in pregnant women with lupus nephritis. A prospective multicenter study. J. Autoimmun. 2016, 74, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Bramham, K.; Seed, P.T.; Lightstone, L.; Nelson-Piercy, C.; Gill, C.; Webster, P.; Poston, L.; Chappell, L.C. Diagnostic and predictive biomarkers for pre-eclampsia in patients with established hypertension and chronic kidney disease. Kidney Int. 2016, 89, 874–885. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hussain, A.; Karovitch, A.; Carson, M.P. Blood pressure goals and treatment in pregnant patients with chronic kidney disease. Adv. Chronic. Kidney Dis. 2015, 22, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Cabiddu, G.; Attini, R.; Parisi, S.; Fassio, F.; Loi, V.; Gerbino, M.; Biolcati, M.; Pani, A.; Todros, T. Hypertension in CKD Pregnancy: A Question of Cause and Effect (Cause or Effect? This Is the Question). Curr. Hypertens. Rep. 2016, 18. [Google Scholar] [CrossRef] [PubMed]
- De Castro, I.; Easterling, T.R.; Bansal, N.; Jefferson, J.A. Nephrotic syndrome in pregnancy poses risks with both maternal and fetal complications. Kidney Int. 2017, 91, 1464–1472. [Google Scholar] [CrossRef] [PubMed]
- Su, X.; Lv, J.; Liu, Y.; Wang, J.; Ma, X.; Shi, S.; Liu, L.; Zhang, H. Pregnancy and Kidney Outcomes in Patients With IgA Nephropathy: A Cohort Study. Am. J. Kidney Dis. 2017, 70, 262–269. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Ma, X.; Zheng, J.; Liu, X.; Yan, T. A Systematic Review and Meta-Analysis of Kidney and Pregnancy Outcomes in IgA Nephropathy. Am. J. Nephrol. 2016, 44, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Attini, R.; Cabiddu, G.; Kooij, I.; Fassio, F.; Gerbino, M.; Maxia, S.; Biolcati, M.; Versino, E.; Todros, T. Maternal-foetal outcomes in pregnant women with glomerulonephritides. Are all glomerulonephritides alike in pregnancy? J. Autoimmun. 2017, 79, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Kooij, I.A.; Attini, R.; Montersino, B.; Fassio, F.; Gerbino, M.; Biolcati, M.; Cabiddu, G.; Versino, E.; Todros, T. A Systematic Review on Materno-Foetal Outcomes in Pregnant Women with IgA Nephropathy: A Case of “Late-Maternal” Preeclampsia? J. Clin. Med. 2018, 7. [Google Scholar] [CrossRef] [PubMed]
- Hollowell, J.G. Outcome of pregnancy in women with a history of vesico-ureteric reflux. BJU Int. 2008, 102, 780–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Attini, R.; Kooij, I.; Montersino, B.; Fassio, F.; Gerbino, M.; Biolcati, M.; Versino, E.; Todros, T.; Piccoli, G.B. Reflux nephropathy and the risk of preeclampsia and of other adverse pregnancy-related outcomes: A systematic review and meta-analysis of case series and reports in the new millennium. J. Nephrol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Wang, D.; Zand, L.; Harris, P.C.; White, W.M.; Garovic, V.D.; Kermott, C.A. Pregnancy outcomes in autosomal dominant polycystic kidney disease: A case-control study. J. Matern. Fetal Neonatal Med. 2016, 29, 807–812. [Google Scholar] [CrossRef] [PubMed]
- Tong, A.; Jesudason, S.; Craig, J.C.; Winkelmayer, W.C. Perspectives on pregnancy in women with chronic kidney disease: Systematic review of qualitative studies. Nephrol. Dial. Transplant. 2015, 30, 652–661. [Google Scholar] [CrossRef] [PubMed]
- Tong, A.; Brown, M.A.; Winkelmayer, W.C.; Craig, J.C.; Jesudason, S. Perspectives on Pregnancy in Women with CKD: A Semistructured Interview Study. Am. J. Kidney Dis. 2015, 66, 951–961. [Google Scholar] [CrossRef] [PubMed]
- Smyth, A.; Oliveira, G.H.; Lahr, B.D.; Bailey, K.R.; Norby, S.M.; Garovic, V.D. A systematic review and meta-analysis of pregnancy outcomes in patients with systemic lupus erythematosus and lupus nephritis. Clin. J. Am. Soc. Nephrol. 2010, 5, 2060–2068. [Google Scholar] [CrossRef] [PubMed]
- Carvalheiras, G.; Vita, P.; Marta, S.; Trovão, R.; Farinha, F.; Braga, J.; Rocha, G.; Almeida, I.; Marinho, A.; Mendonça, T.; et al. Pregnancy and systemic lupus erythematosus: Review of clinical features and outcome of 51 pregnancies at a single institution. Clin. Rev. Allergy Immunol. 2010, 38, 302–306. [Google Scholar] [CrossRef] [PubMed]
- Tower, C.; Mathen, S.; Crocker, I.; Bruce, I.N. Regulatory T cells in systemic lupus erythematosus and pregnancy. Am. J. Reprod. Immunol. 2013, 69, 588–595. [Google Scholar] [CrossRef] [PubMed]
- Niewold, T.B.; Hua, J.; Lehman, T.J.; Harley, J.B.; Crow, M.K. High serum IFN-alpha activity is a heritable risk factor for systemic lupus erythematosus. Genes Immun. 2007, 8, 492–502. [Google Scholar] [CrossRef] [PubMed]
- Buyon, J.P.; Kim, M.Y.; Guerra, M.M.; Lu, S.; Reeves, E.; Petri, M.; Laskin, C.A.; Lockshin, M.D.; Sammaritano, L.R.; Branch, D.W.; et al. Kidney Outcomes and Risk Factors for Nephritis (Flare/De Novo) in a Multiethnic Cohort of Pregnant Patients with Lupus. Clin. J. Am. Soc. Nephrol. 2017, 12, 940–946. [Google Scholar] [CrossRef] [PubMed]
- Buyon, J.P.; Kim, M.Y.; Salmon, J.E. Predictors of Pregnancy Outcomes in Patients with Lupus. Ann. Intern. Med. 2016, 164, 131. [Google Scholar] [CrossRef] [PubMed]
- Hughes, G.R. The antiphospholipid syndrome: Ten years on. Lancet 1993, 342, 341–344. [Google Scholar] [CrossRef]
- Miyakis, S.; Lockshin, M.D.; Atsumi, T.; Branch, D.W.; Brey, R.L.; Cervera, R.; Derksen, R.H.; DEGroot, P.G.; Koike, T.; Meroni, P.L.; et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J. Thromb. Haemost. 2006, 4, 295–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Simone, N.; Di Nicuolo, F.; D’Ippolito, S.; Castellani, R.; Tersigni, C.; Caruso, A.; Meroni, P.; Marana, R. Antiphospholipid antibodies affect human endometrial angiogenesis. Biol. Reprod. 2010, 83, 212–219. [Google Scholar] [CrossRef] [PubMed]
- Di Simone, N.; D’Ippolito, S.; Marana, R.; Di Nicuolo, F.; Castellani, R.; Pierangeli, S.S.; Chen, P.; Tersigni, C.; Scambia, G.; Meroni, P.L. Antiphospholipid antibodies affect human endometrial angiogenesis: Protective effect of a synthetic peptide (TIFI) mimicking the phospholipid binding site of β(2) glycoprotein I. Am. J. Reprod. Immunol. 2013, 70, 299–308. [Google Scholar] [CrossRef] [PubMed]
- D’Ippolito, S.; Marana, R.; Di Nicuolo, F.; Castellani, R.; Veglia, M.; Stinson, J.; Scambia, G.; Di Simone, N. Effect of Low Molecular Weight Heparins (LMWHs) on antiphospholipid Antibodies (aPL)-mediated inhibition of endometrial angiogenesis. PLoS ONE 2012, 7, e29660. [Google Scholar] [CrossRef] [PubMed]
- Asherson, R.A.; Khamashta, M.A.; Ordi-Ros, J.; Derksen, R.H.; Machin, S.J.; Barquinero, J.; Outt, H.H.; Harris, E.N.; Vilardell-Torres, M.; Hughes, G.R. The “primary” antiphospholipid syndrome: Major clinical and serological features. Medicine 1989, 8, 366–374. [Google Scholar] [CrossRef]
- Kochenour, N.K.; Branch, D.W.; Rote, N.S.; Scott, J.R. A new postpartum syndrome associated with antiphospholipid antibodies. Obstet. Gynecol. 1987, 69, 460–468. [Google Scholar] [PubMed]
- Ruffatti, A.; Calligaro, A.; Hoxha, A.; Trevisanuto, D.; Ruffatti, A.T.; Gervasi, M.T.; Cuffaro, S.; Pengo, V.; Punzi, L. Laboratory and clinical features of pregnant women with antiphospholipid syndrome and neonatal outcome. Arthritis Care Res. 2010, 62, 302–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pengo, V.; Banzato, A.; Bison, E.; Bracco, A.; Denas, G.; Ruffatti, A. What have we learned about antiphospholipid syndrome from patients and antiphospholipid carrier cohorts? Semin. Thromb. Hemost. 2012, 38, 322–327. [Google Scholar] [CrossRef] [PubMed]
- Hanouna, G.; Morel, N.; Le Thi Huong, D.; Josselin, L.; Vauthier-Brouzes, D.; Saadoun, D.; Kettaneh, A.; Levesque, K.; Le Guern, V.; Goffinet, F.; et al. Catastrophic antiphospholipid syndrome and pregnancy: An experience of 13 cases. Rheumatology 2013, 52, 1635–1641. [Google Scholar] [CrossRef] [PubMed]
- Smyth, A.; Garovich, V. Glomerular Disease in Pregnancy. In Core Concepts in Parenchymal Kidney Disease; Fervenza, F.C., Lin, J., Sethi, S., Singh, A.K., Eds.; Springer-Verlag: New York, NY, USA, 2014. [Google Scholar]
- Krause, M.L.; Makol, A. Management of rheumatoid arthritis during pregnancy: Challenges and solutions. Open Access Rheumatol. 2016, 8, 23–36. [Google Scholar] [PubMed]
- Brouwer, J.; Hazes, J.M.; Laven, J.S.; Dolhain, R.J. Fertility in women with rheumatoid arthritis: Influence of disease activity and medication. Ann. Rheum. Dis. 2015, 74, 1836–1841. [Google Scholar] [CrossRef] [PubMed]
- De Man, Y.A.; Dolhain, R.J.; van de Geijn, F.E.; Willemsen, S.P.; Hazes, J.M. Disease activity of rheumatoid arthritis during pregnancy: Results from a nationwide prospective study. Arthritis Rheum. 2008, 59, 1241–1248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrett, J.H.; Brennan, P.; Fiddler, M.; Silman, A.J. Does rheumatoid arthritis remit during pregnancy and relapse postpartum? Results from a nationwide study in the United Kingdom performed prospectively from late pregnancy. Arthritis Rheum. 1999, 42, 1219–1227. [Google Scholar] [CrossRef]
- Myasoedova, E.; Crowson, C.S.; Kremers, H.M.; Therneau, T.M.; Gabriel, S.E. Is the incidence of rheumatoid arthritis rising?: Results from Olmsted County, Minnesota, 1955-2007. Arthritis Rheum. 2010, 62, 1576–1582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Icardi, A.; Araghi, P.; Ciabattoni, M.; Romano, U.; Lazzarini, P.; Bianchi, G. Kidney involvement in rheumatoid arthritis. Reumatismo 2003, 55, 76–85. [Google Scholar] [CrossRef] [PubMed]
- Anders, H.J.; Vielhauer, V. Renal co-morbidity in patients with rheumatic diseases. Arthritis Res. Ther. 2011, 13, 222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiu, H.Y.; Huang HL2 Li, C.H.; Chen, H.A.; Yeh, C.L.; Chiu, S.H.; Lin, W.C.; Cheng, Y.P.; Tsai, T.F.; Ho, S. Increased Risk of Chronic Kidney Disease in Rheumatoid Arthritis Associated with Cardiovascular Complications—A National Population-Based Cohort Study. PLoS ONE 2015, 10, e0136508. [Google Scholar] [CrossRef] [PubMed]
- Rom, A.L.; Wu, C.S.; Olsen, J.; Kjaergaard, H.; Jawaheer, D.; Hetland, M.L.; Vestergaard, M.; Mørch, L.S. Fetal growth and preterm birth in children exposed to maternal or paternal rheumatoid arthritis: A nationwide cohort study. Arthritis Rheumatol. 2014, 66, 3265–3273. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.C.; Chen, S.F.; Lin, H.C.; Chen, Y.H. Increased risk of adverse pregnancy outcomes in women with rheumatoid arthritis: A nationwide population-based study. Ann. Rheum. Dis. 2010, 69, 715–717. [Google Scholar] [CrossRef] [PubMed]
- Sammaritano, L.R. Menopause in patients with autoimmune diseases. Autoimmun. Rev. 2012, 11, A430–A436. [Google Scholar] [CrossRef] [PubMed]
- Steen, V.D.; Syzd, A.; Johnson, J.P.; Greenberg, A.; Medsger, T.A., Jr. Kidney disease other than renal crisis in patients with diffuse scleroderma. J. Rheumatol. 2005, 32, 649–655. [Google Scholar] [PubMed]
- Sobanski, V.; Launay, D.; Depret, S.; Ducloy-Bouthors, A.S.; Hachulla, E. Special considerations in pregnant systemic sclerosis patients. Expert Rev. Clin. Immunol. 2016, 12, 1161–1173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chakravarty, E.F.; Khanna, D.; Chung, L. Pregnancy outcomes in systemic sclerosis, primary pulmonary hypertension, and sickle cell disease. Obstet. Gynecol. 2008, 111, 927–934. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.; Davison, J. Chronic kidney disease in pregnancy. BMJ 2008, 336, 211–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mol, B.W.J.; Roberts, C.T.; Thangaratinam, S.; Magee, L.A.; de Groot, C.J.M.; Hofmeyr, G.J. Pre-eclampsia. Lancet 2016, 387, 999–1011. [Google Scholar] [CrossRef]
- Luyckx, V.A.; Tonelli, M.; Stanifer, J.W. The global burden of kidney disease and the sustainable development goals. Bull. World Health Organ. 2018, 96, 414–422. [Google Scholar] [CrossRef] [PubMed]
- Stanifer, J.W.; Von Isenburg, M.; Chertow, G.M.; Anand, S. Chronic kidney disease care models in low- and middle-income countries: A systematic review. BMJ Glob. Health 2018, 3, e000728. [Google Scholar] [CrossRef] [PubMed]
- Koye, D.N.; Magliano, D.J.; Nelson, R.G.; Pavkov, M.E. The Global Epidemiology of Diabetes and Kidney Disease. Adv. Chronic. Kidney Dis. 2018, 25, 121–132. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Garcia, G.; Jha, V.; World Kidney Day Steering Committee. Chronic kidney disease in disadvantaged populations. Nephron Clin. Pract. 2014, 128, 292–296. [Google Scholar] [CrossRef] [PubMed]
- Perico, N.; Remuzzi, G. Prevention programs for chronic kidney disease in low-income countries. Intern. Emerg. Med. 2016, 11, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Ibarra-Hernández, M.; Orozco-Guillén, O.A.; de la Alcantar-Vallín, M.L.; Garrido-Roldan, R.; Jiménez-Alvarado, M.P.; Castro, K.B.; Villa-Villagrana, F.; Borbolla, M.; Gallardo-Gaona, J.M.; García-García, G.; et al. Acute kidney injury in pregnancy and the role of underlying CKD: A point of view from México. J. Nephrol. 2017, 30, 773–780. [Google Scholar] [CrossRef] [PubMed]
- Agampodi, S.B.; Wijerathne, B.T. Baseline renal function of pregnant women in a geographical region with an epidemic of chronic kidney disease of unknown aetiology in Sri Lanka. Nephrology 2016, 21, 794–795. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Fassio, F.; Attini, R.; Parisi, S.; Biolcati, M.; Ferraresi, M.; Pagano, A.; Daidola, G.; Deagostini, M.C.; Gaglioti, P.; et al. Pregnancy in CKD: Whom should we follow and why? Nephrol. Dial. Transplant. 2012, 27, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Antenatal care for uncomplicated pregnancies | Guidance and guidelines | NICE. Available online: https://www.nice.org.uk/Guidance/cg62 (accessed on 10 July 2018).
- Gravidanza Basso Rischio. Available online: http://www.aogoi.it/media/1058/gravidanza_basso_rischio.pdf (accessed on 10 July 2018).
- Haute Autorité de Santé—Suivi et Orientation des Femmes Enceintes en Fonction des Situations à Risque Identifiées. Available online: https://www.has-sante.fr/portail/jcms/c_547976/fr/suivi-et-orientation-des-femmes-enceintes-en-fonction-des-situations-a-risque-identifiees (accessed on 10 July 2018).
- Shahraki, A.D.; Bardeh, M.E.; Najarzadegan, M.R. Investigation of the relationship between idiopathic microscopic hematuria (in the first and second trimesters) and major adverse outcomes of pregnancy. Adv. Biomed. Res. 2016, 5, 186. [Google Scholar] [PubMed]
- Brown, M.A.; Holt, J.L.; Mangos, G.J.; Murray, N.; Curtis, J.; Homer, C. Microscopic hematuria in pregnancy: Relevance to pregnancy outcome. Am. J. Kidney Dis. 2005, 45, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Szeto, C.C.; To, K.F.; Lai, F.M.; Chow, K.M.; Tam, W.H.; Chung, K.Y.; Leung, C.B.; Lui, S.F.; Li, P.K.; Lau, T.K. Prevalence and implications of isolated microscopic hematuria in asymptomatic Chinese pregnant women. Nephron Clin. Pract. 2007, 105, c147–c152. [Google Scholar] [CrossRef] [PubMed]
- Rolfo, A.; Attini, R.; Tavassoli, E.; Neve, F.V.; Nigra, M.; Cicilano, M.; Nuzzo, A.M.; Giuffrida, D.; Biolcati, M.; Nichelatti, M.; et al. Is It Possible to Differentiate Chronic Kidney Disease and Preeclampsia by means of New and Old Biomarkers? A Prospective Study. Dis. Markers 2015, 2015, 127083. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Gaglioti, P.; Attini, R.; Parisi, S.; Bossotti, C.; Olearo, E.; Oberto, M.; Ferraresi, M.; Rolfo, A.; Versino, E.; et al. Pre-eclampsia or chronic kidney disease? The flow hypothesis. Nephrol. Dial. Transplant. 2013, 28, 1199–1206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rolfo, A.; Attini, R.; Nuzzo, A.M.; Piazzese, A.; Parisi, S.; Ferraresi, M.; Todros, T.; Piccoli, G.B. Chronic kidney disease may be differentially diagnosed from preeclampsia by serum biomarkers. Kidney Int. 2013, 83, 177–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alkhunaizi, A.; Melamed, N.; Hladunewich, M.A. Pregnancy in advanced chronic kidney disease and end-stage renal disease. Curr. Opin. Nephrol. Hypertens. 2015, 24, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Jesudason, S.; Grace, B.S.; McDonald, S.P. Pregnancy outcomes according to dialysis commencing before or after conception in women with ESRD. Clin. J. Am. Soc. Nephrol. 2014, 9, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Cabiddu, G.; Daidone, G.; Guzzo, G.; Maxia, S.; Ciniglio, I.; Postorino, V.; Loi, V.; Ghiotto, S.; Nichelatti, M.; et al. The children of dialysis: Live-born babies from on-dialysis mothers in Italy—An epidemiological perspective comparing dialysis, kidney transplantation and the overall population. Nephrol. Dial. Transplant. 2014, 29, 1578–1586. [Google Scholar] [CrossRef] [PubMed]
- Hladunewich, M.; Schatell, D. Intensive dialysis and pregnancy. Hemodial. Int. 2016, 20, 339–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hladunewich, M.; Hercz, A.E.; Keunen, J.; Chan, C.; Pierratos, A. Pregnancy in end stage renal disease. Semin. Dial. 2011, 24, 634–639. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Minelli, F.; Versino, E.; Cabiddu, G.; Attini, R.; Vigotti, F.N.; Rolfo, A.; Giuffrida, D.; Colombi, N.; Pani, A.; et al. Pregnancy in dialysis patients in the new millennium: A systematic review and meta-regression analysis correlating dialysis schedules and pregnancy outcomes. Nephrol. Dial. Transplant. 2016, 31, 1915–1934. [Google Scholar] [CrossRef] [PubMed]
- Sachdeva, M.; Barta, V.; Thakkar, J.; Sakhiya, V.; Miller, I. Pregnancy outcomes in women on hemodialysis: A national survey. Clin. Kidney J. 2017, 10, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Cabiddu, G.; Castellino, S.; Gernone, G.; Santoro, D.; Giacchino, F.; Credendino, O.; Daidone, G.; Gregorini, G.; Moroni, G.; Attini, R.; et al. Best practices on pregnancy on dialysis: The Italian Study Group on Kidney and Pregnancy. J. Nephrol. 2015, 28, 279–288. [Google Scholar] [CrossRef] [PubMed]
- Suarez, M.B.; Costa, M.L.; Parpinelli, M.Â.; Surita, F.G. Pregnancy in women undergoing hemodialysis: Case series in a Southeast Brazilian reference center. Rev. Bras. Ginecol. Obstet. 2015, 37, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Duffner, J.; Schulte-Kemna, L.; Reister, B.; Ludwig, U.; Keller, F.; van Erp, R.; Schröppel, B. Survey among nephrologists in Germany: Current practice and management of pregnant women on dialysis. Clin. Nephrol. 2017, 88, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Van Ek, G.F.; Krouwel, E.M.; Nicolai, M.P.J.; Den Oudsten, B.L.; Den Ouden, M.E.M.; Dieben, S.W.M.; Putter, H.; Pelger, R.C.M.; Elzevier, H.W. What is the role of nephrologists and nurses of the dialysis department in providing fertility care to CKD patients? A questionnaire study among care providers. Int. Urol. Nephrol. 2017, 49, 1273–1285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hildebrand, A.M.; Liu, K.; Shariff, S.Z.; Ray, J.G.; Sontrop, J.M.; Clark, W.F.; Hladunewich, M.A.; Garg, A.X. Characteristics and Outcomes of AKI Treated with Dialysis during Pregnancy and the Postpartum Period. J. Am. Soc. Nephrol. 2015, 26, 3085–3091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Ma, X.; Zheng, J.; Liu, X.; Yan, T. Pregnancy outcomes in patients with acute kidney injury during pregnancy: A systematic review and meta-analysis. BMC Pregnancy Childbirth 2017, 17, 235. [Google Scholar] [CrossRef] [PubMed]
- Prakash, J.; Ganiger, V.C.; Prakash, S.; Iqbal, M.; Kar, D.P.; Singh, U.; Verma, A. Acute kidney injury in pregnancy with special reference to pregnancy-specific disorders: A hospital based study (2014–2016). J. Nephrol. 2018, 31, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Nwoko, R.; Plecas, D.; Garovic, V.D. Acute kidney injury in the pregnant patient. Clin Nephrol 2012, 78, 478–486. [Google Scholar] [CrossRef] [PubMed]
- Leurs, P.; Machowska, A.; Lindholm, B. Timing of dialysis initiation: When to start? Which treatment? J. Ren. Nutr. 2015, 25, 238–241. [Google Scholar] [CrossRef] [PubMed]
- Rosansky, S.J.; Cancarini, G.; Clark, W.F.; Eggers, P.; Germaine, M.; Glassock, R.; Goldfarb, D.S.; Harris, D.; Hwang, S.J.; Imperial, E.B.; et al. Dialysis initiation: What’s the rush? Semin. Dial. 2013, 26, 650–657. [Google Scholar] [CrossRef] [PubMed]
- Rivara, M.B.; Mehrotra, R. Is early initiation of dialysis harmful? Semin. Dial. 2014, 27, 250–252. [Google Scholar] [CrossRef] [PubMed]
- Nesrallah, G.E.; Mustafa, R.A.; Clark, W.F.; Bass, A.; Barnieh, L.; Hemmelgarn, B.R.; Klarenbach, S.; Quinn, R.R.; Hiremath, S.; Ravani, P.; et al. Canadian Society of Nephrology 2014 clinical practice guideline for timing the initiation of chronic dialysis. CMAJ 2014, 186, 112–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, J.L.; De Oliveira, L.; Kirsztajn, G.M.; Sass, N. Chronic kidney disease in pregnancy requiring first-timedialysis. Int. J. Gynaecol. Obstet. 2010, 111, 45–48. [Google Scholar] [CrossRef] [PubMed]
- Cornelis, T.; Spaanderman, M.; Beerenhout, C.; Perschel, F.H.; Verlohren, S.; Schalkwijk, C.G.; van der Sande, F.M.; Kooman, J.P.; Hladunewich, M. Antiangiogenic factors and maternal hemodynamics during intensive hemodialysis in pregnancy. Hemodial. Int. 2013, 17, 639–643. [Google Scholar] [CrossRef] [PubMed]
- Attini, R.; Leone, F.; Parisi, S.; Fassio, F.; Capizzi, I.; Loi, V.; Colla, L.; Rossetti, M.; Gerbino, M.; Maxia, S.; et al. Vegan-vegetarian low-protein supplemented diets in pregnant CKD patients: Fifteen years of experience. BMC Nephrol. 2016, 17. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Clari, R.; Vigotti, F.N.; Leone, F.; Attini, R.; Cabiddu, G.; Mauro, G.; Castelluccia, N.; Colombi, N.; Capizzi, I.; et al. Vegan-vegetarian diets in pregnancy: Danger or panacea? A systematic narrative review. BJOG 2015, 122, 623–633. [Google Scholar] [CrossRef] [PubMed]
- Nava, J.; Moran, S.; Figueroa, V.; Salinas, A.; Lopez, M.; Urbina, R.; Gutierrez, A.; Lujan, J.L.; Orozco, A.; Montufar, R.; et al. Successful pregnancy in a CKD patient on a low-protein, supplemented diet: An opportunity to reflect on CKD and pregnancy in Mexico, an emerging country. J. Nephrol. 2017, 30, 877–882. [Google Scholar] [CrossRef] [PubMed]
- Leduc, V.; Ficheux, M.; Bechade, C.; Dreyfus, M.; Lobbedez, T.; Henri, P. Pregnancy on short-daily home hemodialysis using low dialysate flow rate: A new hope for the end-stage renal disease patients. Hemodial. Int. 2018, 22, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Brahmbhatt, Y.; Ikeme, A.; Bhogal, N.; Berghella, V. Successful Pregnancy Using the NxStage Home Hemodialysis System. Case Rep. Nephrol. 2016, 2016, 1358625. [Google Scholar] [CrossRef] [PubMed]
- Choi, C.Y.; Cho, N.J.; Park, S.; Gil, H.W.; Kim, Y.S.; Lee, E.Y. A case report of successful pregnancy and delivery after peritoneal dialysis in a patient misdiagnosed with primary infertility. Medicine 2018, 97, 11148. [Google Scholar] [CrossRef] [PubMed]
- Lim, T.S.; Shanmuganathan, M.; Wong, I.; Goh, B.L. Successful multigravid pregnancy in a 42-year-old patient on continuous ambulatory peritoneal dialysis and a review of the literature. BMC Nephrol. 2017, 18. [Google Scholar] [CrossRef] [PubMed]
- Ross, L.E.; Swift, P.A.; Newbold, S.M.; Bramham, K.; Hurley, A.; Gallagher, H. An Alternative Approach to Delivering Intensive Dialysis in Pregnancy. Perit. Dial. Int. 2016, 36, 575–577. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, N.A.; James, N.T.; Kucirka, L.M.; Boyarsky, B.J.; Garonzik-Wang, J.M.; Montgomery, R.A.; Segev, D.L. Pregnancy outcomes in kidney transplant recipients: A systematic review and meta-analysis. Am. J. Transplant. 2011, 11, 2388–2404. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, N.A.; Coscia, L.A.; Gomez-Lobo, V.; Moritz, M.J.; Armenti, V.T. Pregnancy after solid organ transplantation: A guide for obstetric management. Rev. Obstet. Gynecol. 2013, 6, 116–125. [Google Scholar] [PubMed]
- Bramham, K.; Nelson-Piercy, C.; Gao, H.; Pierce, M.; Bush, N.; Spark, P.; Brocklehurst, P.; Kurinczuk, J.J.; Knight, M. Pregnancy in renal transplant recipients: A UK national cohort study. Clin. J. Am. Soc. Nephrol. 2013, 8, 290–298. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, F.A.; Borg, M.; Gulyani, A.; McDonald, S.P.; Jesudason, S. Pregnancy outcomes and impact of pregnancy on graft function in women after kidney transplantation. Clin. Transplant. 2017, 31. [Google Scholar] [CrossRef] [PubMed]
- Saber, L.T.; Duarte, G.; Costa, J.A.; Cologna, A.J.; Garcia, T.M.; Ferraz, A.S. Pregnancy and kidney transplantation: Experience in a developing country. Am. J. Kidney Dis. 1995, 25, 465–470. [Google Scholar] [CrossRef]
- Kwek, J.L.; Tey, V.; Yang, L.; Kanagalingam, D.; Kee, T. Renal and obstetric outcomes in pregnancy after kidney transplantation: Twelve-year experience in a Singapore transplant center. J. Obstet. Gynaecol. Res. 2015, 41, 1337–1344. [Google Scholar] [CrossRef] [PubMed]
- Ghanem, M.E.; El-Baghdadi, L.A.; Badawy, A.M.; Bakr, M.A.; Sobhe, M.A.; Ghoneim, M.A. Pregnancy outcome after renal allograft transplantation: 15 Years experience. Eur. J. Obstet. Gynecol. Reprod. Biol. 2005, 121, 178–181. [Google Scholar] [CrossRef] [PubMed]
- Cabiddu, G.; Spotti, D.; Gernone, G.; Santoro, D.; Moroni, G.; Gregorini, G.; Giacchino, F.; Attini, R.; Limardo, M.; Gammaro, L.; et al. A best-practice position statement on pregnancy after kidney transplantation: Focusing on the unsolved questions. The Kidney and Pregnancy Study Group of the Italian Society of Nephrology. J. Nephrol. 2018, 31, 665–681. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Cabiddu, G.; Attini, R.; Gerbino, M.; Todeschini, P.; Perrino, M.L.; Manzione, A.M.; Piredda, G.B.; Gnappi, E.; Caputo, F.; et al. Outcomes of pregnancies after kidney transplantation: Lessons learned from CKD. A comparison of transplanted, nontransplanted chronic kidney disease patients and low-risk pregnancies: A multicenter nationwide analysis. Transplantation 2017, 101, 2536–2544. [Google Scholar] [CrossRef] [PubMed]
- Kukla, A.; Issa, N.; Ibrahim, H.N. Pregnancy in renal transplantation: Recipient and donor aspects in the Arab world. Arab. J. Urol. 2012, 10, 175–181. [Google Scholar] [CrossRef] [PubMed]
- EBPG Expert Group on Renal Transplantation. European best practice guidelines for renal transplantation. Section IV: Long-term management of the transplant recipient. IV.10. Pregnancy in renal transplant recipients. Nephrol. Dial. Transplant. 2002, 17, 50–55. [Google Scholar]
- Kidney Disease: Improving Global Outcomes (KDIGO) Transplant Work Group. KDIGO clinical practice guideline for the care of kidney transplant recipients. Am. J. Transplant. 2009, 9, S1–S155. [Google Scholar] [CrossRef] [PubMed]
- Josephson, M.A.; McKay, D.B. Women and transplantation: Fertility, sexuality, pregnancy, contraception. Adv. Chronic. Kidney Dis. 2013, 20, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Gizzo, S.; Noventa, M.; Saccardi, C.; Paccagnella, G.; Patrelli, T.S.; Cosmi, E.; D’Antona, D. Twin pregnancy after kidney transplantation: What’s on? A case report and review of literature. J. Matern. Fetal Neonatal Med. 2014, 27, 1816–1819. [Google Scholar] [CrossRef] [PubMed]
- Combs, J.; Kagan, A.; Boelkins, M.; Coscia, L.; Moritz, M.; Hofmann, R.M. Belatacept during pregnancy in renal transplant recipients: Two case reports. Am. J. Transplant. 2018, 18, 2079–2082. [Google Scholar] [CrossRef] [PubMed]
- Assalino, M.; Podetta, M.; Demuylder-Mischler, S.; Francini, K.; Pernin, N.; Randin, J.P.; Bosco, D.; Andres, A.; Berney, T. Successful pregnancy and delivery after simultaneous islet-kidney transplantation. Am. J. Transplant. 2018, 18, 2075–2078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahmoud, T.; Mujaibel, K.; Attia, H.; Zakaria, Z.; Yagan, J.; Gheith, O.; Halim, M.A.; Nair, P.; Al-Otaibi, T. Triplet Pregnancy in a Diabetic Mother With Kidney Transplant: Case Report and Review of the Literature. Exp. Clin. Transplant. 2017, 15, 139–146. [Google Scholar] [PubMed]
- Esposito, L.; Rostaing, L.; Kamar, N. Successful pregnancy after ABO-incompatible kidney transplantation. Transpl. Int. 2016, 29, 506–507. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, C.; Hussein, W.; Spencer, S.; Walshe, J.; Denton, M.; Conlon, P.J.; Magee, C. Reproductive health in Irish female renal transplant recipients. Ir. J. Med. Sci. 2012, 181, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Pietrzak, B.; Mazanowska, N.; Kociszewska-Najman, B.; Szymusik, I.; Grzechocińska, B.; Pazik, J.; Jabiry-Zieniewicz, Z.; Popow, A.; Wielgos, M. Successful Pregnancy Outcome after In Vitro Fertilization in a Kidney Graft Recipient: A Case Report and Literature Review. Ann. Transplant. 2015, 20, 338–341. [Google Scholar] [PubMed]
- Norrman, E.; Bergh, C.; Wennerholm, U.B. Pregnancy outcome and long-term follow-up after in vitro fertilization in women with renal transplantation. Hum. Reprod. 2015, 30, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Zheng, H.H.; Song, Y.; Wu, J.Y. Critical Ovarian Hyperstimulation Syndrome After In Vitro Fertilization Treatment in a Renal Transplant Recipient: A Case Report. Transplant. Proc. 2016, 48, 267–270. [Google Scholar] [CrossRef] [PubMed]
- El Houssni, S.; Sabri, S.; Benamar, L.; Ouzeddoun, N.; Bayahia, R.; Rhou, H. Pregnancy after renal transplantation: Effects on mother, child, and renal graft function. Saudi J. Kidney Dis. Transpl. 2016, 27, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.Y.; Kwon, O.J.; Kang, C.M. The effect of donor-recipient relationship on long-term outcomes of living related donor renal transplantation. Transplant. Proc. 2012, 44, 257–260. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Han, P.; Liu, Y.; Wang, H.; Yang, Y.; Qiu, F.; Peng, W.; Tang, L.; Fu, J.; Zhu, X.; et al. Study on the effect of kidney transplantation on the health of the patients’ offspring: A report on 252 Chinese children. Cell Biochem. Biophys. 2014, 68, 173–179. [Google Scholar] [CrossRef] [PubMed]

| Clinical Feature | Effect on Pregnancy | Effect on Maternal Health |
|---|---|---|
| CKD stage | Increase across stages (from stage 1 to stage 5) of preterm delivery, caesarean section, SGA | Increase in risk of kidney function impairment, development of hypertension, and proteinuria |
| Immunologic diseases | PE risk may be increased at least in some diseases (IgAGN, SLE); differential diagnosis with flares may be difficult | In CKD, maternal deaths are mainly described in SLE nephropathy (immunologic flares) |
| Diabetes and diabetic nephropathy | Increased risk in malformations, linked to diabetes, proportional to diabetes control | Same as CKD |
| Baseline hypertension | May be associated with a higher risk of preterm or SGA babies | Risk of kidney function impairment may be increased |
| Baseline proteinuria | May be associated with a higher risk of preterm or SGA babies | Risk of kidney function impairment and of persistent hypertension may be increased |
| Term | Definition | Main Issues in CKD |
|---|---|---|
| Maternal death | Death in pregnancy or within 1 week–1 month postpartum | Too rare to be quantified, at least in highly resourced settings, where cases are in the setting of severe flares of immunologic diseases (SLE in primis). |
| CKD progression | Decrease in GFR, rise in sCr, shift to a higher CKD stage | Differently assessed and estimated; may be linked to obstetric policy (anticipating delivery in the case of worsening of the kidney function); 20% and 80% in advanced CKD. Probably not increased in early CKD (stages 1–3a). |
| Immunologic flares and neonatal SLE | Flares of immunologic diseases in pregnancy | Risks are mainly but not exclusively limited to patients who start pregnancy with active disease or recent flare-up. Definition of a “safe” zone is not agreed; in quiescent, well-controlled diseases are probably equivalent to nonpregnant, carefully-matched controls. |
| Transplant rejection (kidney) | Acute rejection in pregnancy | Kidney rejection episodes are not increased with respect to matched controls; may be an issue in unplanned pregnancies. |
| Abortion | Foetal loss, before 21–24 gestational weeks | Scant data on advanced CKD. An issue in immunologic diseases (not exclusively linked to LLAC) and in diabetic nephropathy. |
| Stillbirth | Delivery of a nonviable infant, after 21–24 gestational weeks | Probably not increased in early CKD, too few data in late CKD stages; may be an issue in dialysis patients; when not linked to extreme prematurity, may be specifically linked to SLE, immunologic diseases, and diabetic nephropathy. |
| Perinatal death | Death within 1 week–1 month from delivery | Usually a result of extreme prematurity, which bears a risk of respiratory distress, neonatal sepsis, cerebral haemorrhage. |
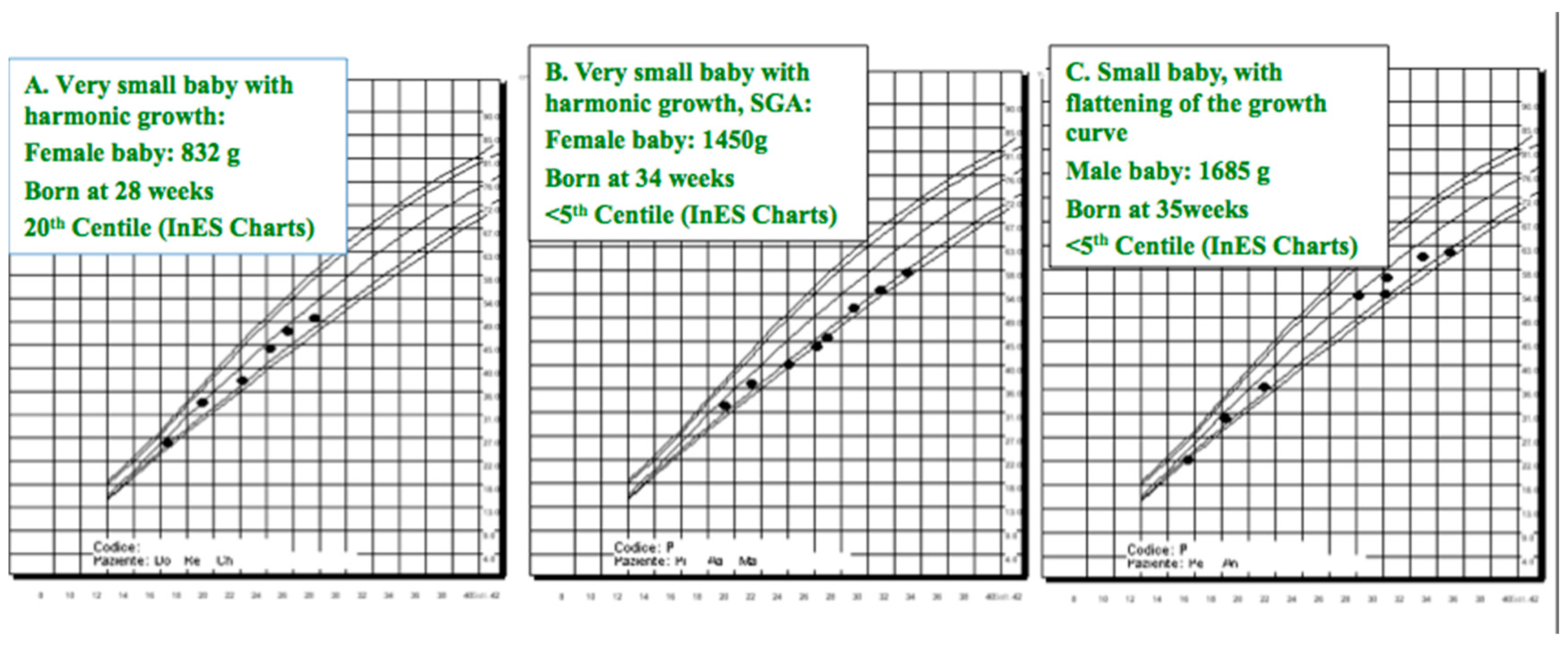
| Small, very small baby | A baby weighing <1500–2500 g at birth | Gestational age adjusted weight may be a better risk marker; however, very low birth weight may bear risks for future health, even without SGA. Different cut-points are used, the most common are 1500 for very small and 2500 for small baby. |
| Preterm, early extremely preterm | Delivery before 37, 32, or 34; 28 completed gestational weeks | Risk of preterm delivery increases across CKD stages. Definition of preterm and extremely preterm are agreed (<37 and <28 weeks, respectively); two cut-points are used for early preterm (<32 and <34 weeks) |
| Small for gestational age (SGA) | <5th or <10th centile for gestational age | SGA and IUGR may be associated, but IUGR is also a dynamic event, characterised by flattening of the growth curve. Both are better defined when several data in pregnancy are available. |
| Intrauterine growth restriction (IUGR) | <5th centile or flattening of the growth curve | Small, SGA, and IUGR babies are at higher risk of developing hypertension, metabolic syndrome, and CKD in adulthood. |
| Malformations | Any kind of malformations | Malformations are not increased in the absence of teratogen drugs; exception is diabetic nephropathy (increase in malformations attributed to diabetes); hereditary diseases may not be evident at birth. |
| Hereditary kidney diseases | Any kind of CKD | Several forms of CKD have a hereditary pattern or predisposition, among them, ADPKD, Alport’s, vescico ureteral reflux and CAKUT, IgA, kidney tubular disorders, and mitochondrial diseases. |
| CKD-hypertension | Higher risk of hypertension and CKD in adulthood | Lower nephron number in preterm babies; the risks are probably higher in SGA–IUGR babies than in preterm babies adequate for gestational age. |
| Other long-term issues | Developmental disorders | Cerebral haemorrhage or neonatal sepsis, not specific of CKD, are a threat in all preterm babies. |
| Pre-Eclampsia/HELLP | Hemolytic Uremic Syndrome (HUS) | Thrombotic Thrombocytopenic Purpura (TTP) | |
|---|---|---|---|
| Usual time of onset | After 20 gestational weeks | postpartum | 2nd and 3rd trimester |
| Arterial hypertension | +++ | + | + |
| Renal failure | + (mainly in HELLP) | +++ | + |
| Renal prognosis | Recovery | 75% ESRD | Usually good |
| Neurological impairment | + | + | +++ |
| Hemolytic anemia | ++ (HELLP) | +++ | +++ |
| Low platelet count | +++ (HELLP) | +++ | +++ |
| Intravascular coagulation | + | Usually absent | ++ |
| Proteinuria | +++ | + | Rare |
| Abnormal liver function tests | +++ (HELLP) | Usually absent | Usually absent |
| Complement alternative pathway activation | + (HELLP) | +++ | Usually absent |
| Reduced ADAMTS13 | + | Usually absent | +++ |
| Treatment | Supportive treatment | Plasmapheresis; plasma infusion Anti-MAC antibodies | Plasmapheresis; plasma infusion Anti-CD20 antibodies |
| Sign or Symptom | Interference in Pregnancy | Potential Correction |
|---|---|---|
| Hypertension | Blood pressure is physiologically reduced, particularly in the 1st trimester; mild–moderate hypertension may be masked by the physiologic changes in early pregnancy. | Attention to “high normal” BP; strict monitoring in presence of risk factors (obesity, diabetes, family history, age, CKD); if associated with proteinuria, interference in PE diagnosis. |
| Kidney function reduction | Kidney function physiologically increased, in particular in 1st–2nd trimester; CKD stages 2–3 may be missed, in particular if reference eGFR of nonpregnant women is employed. | Lack of hyperfiltration is a potential sign of initial reduction of kidney function; “normal” values outside pregnancy should be interpreted with caution in pregnancy. |
| Hematuria | Presence of contaminant RBCs in the urine is common and microhematuria may be misinterpreted as of gynaecologic origin. Possible underestimation in polyuria. | Microscopic examination, search for urinary casts, and attention to correct sampling avoid missing this sign pointing to a glomerular origin (most frequent, IgA nephropathy). |
| Proteinuria | The physiologic limit is increased to 300 mg/day. Proteinuria may show day-to-day and circadian variations. If assessed on spot urine collection, mild proteinuria may be missed in patients with polyuria. | Repeated tests and 24 h urine assessment in cases with trace proteinuria may avoid missing low-grade (albeit clinically relevant) proteinuria. |
| Tubular derangements | The usual workout of physiologic pregnancy includes the major ions (Na, K, Calcium). Mild hypokalaemia and hyponatremia are common, due to physiologic hemodilution. | Tubular derangements may be elusive. Phosphate, Mg, bicarbonate should be controlled in severe hypokalaemia, severe hyponatremia, or unexplained polyuria. |
| Urinary infection | Urinary infections are common and usually asymptomatic. Several societies suggest at least one urinary culture per trimester. | Repeatedly positive urinary cultures suggest performing ultrasounds of the kidney and urinary tract. |
| Item | Indications | Open Issues |
|---|---|---|
| Number of sessions | Daily hemodialysis (DHD) is superior to thrice weekly dialysis | DHD is differently defined (5–7 sessions/week); no data on adjustment per body size or residual renal function (RRF): urea level should probably guide the choice. Unclear advantage of shorter/more frequent or of longer/less frequent sessions in presence of RRF. |
| Duration of session | The longest, the best, according to the Canadian experience | Scattered positive experience with short DHD; difficult to distinguish between effect of frequency and duration. Long-hours dialysis is more effective in removal of middle molecules and phosphate. |
| Weight loss | The lowest, the best; attention to avoid dehydration and oligoamnios | The evaluation of weight gain remains empiric. Unclear role for bioimpedance, BNP, BP. Unclear role of biomarkers (s-Flt1, PlGF) in diagnosis of PE. |
| Blood flow | Low blood flow (150–250 mL/min) may be reasonable in intensive HD | Lower blood flow has to be balanced with higher need for anticoagulation. Long-hours dialysis is associated with better removal of middle molecules and compartmentalised toxins: depuration markers alternative to urea are not identified. Hypophosphatemia is often found: subtle deficits of trace metals or vitamins may be relevant; the role of multivitamin supplementation is not clear. |
| Dialysate flow | Low dialysate flow advised in long-hours dialysis (300 mL/min) | |
| Dialysis efficiency | The most common target is “near normal” urea (10–15 umol/L) following the day break | |
| Dialysis membrane | Biocompatible membranes | No study addressed to different membranes; low-flux membranes limit nutrient loss; high-flux membranes increase middle molecules clearance, but increase also nutrient loss and may induce back-filtration. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piccoli, G.B.; Zakharova, E.; Attini, R.; Ibarra Hernandez, M.; Orozco Guillien, A.; Alrukhaimi, M.; Liu, Z.-H.; Ashuntantang, G.; Covella, B.; Cabiddu, G.; et al. Pregnancy in Chronic Kidney Disease: Need for Higher Awareness. A Pragmatic Review Focused on What Could Be Improved in the Different CKD Stages and Phases. J. Clin. Med. 2018, 7, 415. https://doi.org/10.3390/jcm7110415
Piccoli GB, Zakharova E, Attini R, Ibarra Hernandez M, Orozco Guillien A, Alrukhaimi M, Liu Z-H, Ashuntantang G, Covella B, Cabiddu G, et al. Pregnancy in Chronic Kidney Disease: Need for Higher Awareness. A Pragmatic Review Focused on What Could Be Improved in the Different CKD Stages and Phases. Journal of Clinical Medicine. 2018; 7(11):415. https://doi.org/10.3390/jcm7110415
Chicago/Turabian StylePiccoli, Giorgina B., Elena Zakharova, Rossella Attini, Margarita Ibarra Hernandez, Alejandra Orozco Guillien, Mona Alrukhaimi, Zhi-Hong Liu, Gloria Ashuntantang, Bianca Covella, Gianfranca Cabiddu, and et al. 2018. "Pregnancy in Chronic Kidney Disease: Need for Higher Awareness. A Pragmatic Review Focused on What Could Be Improved in the Different CKD Stages and Phases" Journal of Clinical Medicine 7, no. 11: 415. https://doi.org/10.3390/jcm7110415