Effectiveness of Combined Smartwatch and Social Media Intervention on Breast Cancer Survivor Health Outcomes: A 10-Week Pilot Randomized Trial




Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Recruitment and Inclusion/Exclusion Criteria
2.3. Measures
2.3.1. Primary Outcome
2.3.2. Secondary Outcomes
2.4. Procedures
2.5. Statistical Analysis
3. Results
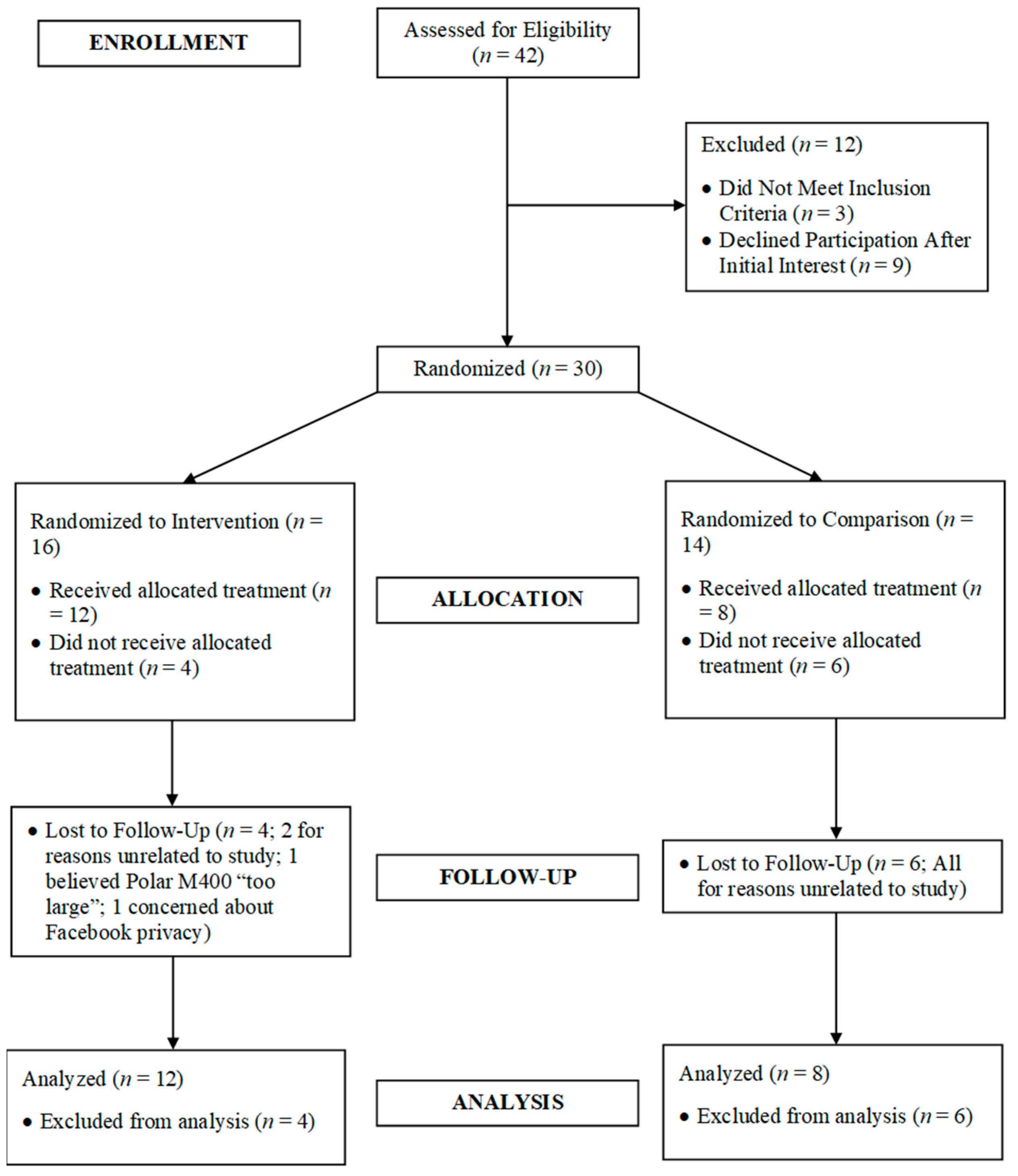
3.1. Baseline Comparisons and Participant Flow
3.2. Intervention Use/Acceptability
3.2.1. Primary Outcomes
3.2.2. Secondary Outcomes
3.3. Physiological Changes over Time
3.4. Psychosocial Construct Changes over Time
3.5. Quality of Life Changes over Time
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Amercian Cancer Society. How Common Is Breast Cancer? Available online: https://www.cancer.org/cancer/breast-cancer/about/how-common-is-breast-cancer.html (accessed on 16 May 2018).
- Howlader, N.; Noone, A.; Krapcho, M.; Miller, D.; Bishop, K.; Altekruse, S.; Kosary, C.; Yu, M.; Ruhl, J.; Tatalovich, Z.; et al. Seer Cancer Statistics Review; National Cancer Institute: Bethesda, MD, USA, 2016. [Google Scholar]
- Phillips, S.; McAuley, E. Physical activity, quality of life, and survivorship in breast cancer survivors: A brief review. CML Breast Cancer 2012, 24, 77–84. [Google Scholar]
- Jadoon, N.; Munir, W.; Shahzad, M.; Choudhry, Z. Assessment of depression and anxiety in adult cancer outpatients: A cross-sectional study. BMC Cancer 2010, 10, 594. [Google Scholar] [CrossRef] [PubMed]
- Phillips, S.; McAuley, E. Physical activity and fatigue in breast cancer survivors: A panel model examining the role of self-efficacy and depression. Cancer Epidemiol. Prev. Biomark. 2013, 22, 773–781. [Google Scholar] [CrossRef] [PubMed]
- Phillips, S.; McAuley, E. Physical activity and quality of life in breast cancer survivors: The role of self-efficacy and health status. Psychol. Oncol. 2014, 23, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Harrison, S.; Hayes, S.; Newman, B. Age-related differences in exercise and quality of life among breast cancer survivors. Med. Sci. Sports Exerc. 2010, 42, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Mack, D.; Meldrum, L.; Wilson, P.; Sabiston, C. Physical activity and psychological health in breast cancer survivors: An application of basic psychological needs theory. Appl. Psychol. Health Well Being 2013, 5, 369–388. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.; Alfano, C.; Reeve, B.; Irwin, M.; Bernstein, L.; Baumgartner, K.; Bowen, D.; McTiernan, A.; Ballard-Barbash, R. Race/ethnicity, physical activity, and quality of life in breast cancer survivors. Cancer Epidemiol. Prev. Biomark. 2009, 18, 656–663. [Google Scholar] [CrossRef] [PubMed]
- Taylor, D.; Nichols, J.; Pakiz, B.; Bardwell, W.; Flatt, S.; Rock, C. Relationships between cardiorespiratory fitness, physical activity, and psychosocial variables in overweight and obese breast cancer survivors. Int. J. Behav. Med. 2010, 17, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Lewis, B.; Napolitano, M.; Buman, M.; Williams, D.; Nigg, C. Future directions in physical activity intervention research: Expanding our focus to sedentary behaviors, technology, and dissemination. J. Behav. Med. 2017, 40, 112–126. [Google Scholar] [CrossRef] [PubMed]
- Brandt, C.; Clemensen, J.; Nielsen, J.; Sondergaard, J. Drivers of successful long-term lifestyle change, the role of e-health: A qualitative study. BMJ Open 2018, 8, e017466. [Google Scholar] [CrossRef] [PubMed]
- Statista. Consumer Wearables Revenues in the United States from 2014 to 2019 (in Billion U.S. Dollars). Available online: https://www.statista.com/statistics/503455/consumer-wearables-revenues-in-the-us (accessed on 16 May 2018).
- Almalki, M.; Gray, K.; Sanchez, F. The use of self-quantification systems for personal health information: Big data management activities and prospects. Health Inf. Sci. Syst. 2015, 3, S1. [Google Scholar] [CrossRef] [PubMed]
- Lyons, E.; Lewis, Z.; Mayrsohn, B.; Rowland, J. Behavior change techniques implemented in electronic lifestyle activity monitors: A systematic content analysis. J. Med. Internet Res. 2014, 16, e192. [Google Scholar] [CrossRef] [PubMed]
- Pope, Z.; Lee, J.; Zeng, N.; Lee, H.; Gao, Z. Feasibility of smartphone application and social media intervention on breast cancer survivors’ health outcomes. Transl. Behav. Med. 2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, N.; Hadgraft, N.; Moore, M.; Rosenberg, D.; Lynch, C.; Reeves, M.; Lynch, B. A qualitative evaluation of breast cancer survivors’ acceptance of and preferences for consumer wearable technology activity trackers. Support. Care Cancer 2017, 25, 3375–3384. [Google Scholar] [CrossRef] [PubMed]
- Cadmus-Bertram, L.; Marcus, B.; Patterson, R.; Parker, B.; Morey, B. Randomized trial of a fitbit-based physical activity intervention for women. Am. J. Prev. Med. 2015, 49, 414–418. [Google Scholar] [CrossRef] [PubMed]
- Cadmus-Bertram, L.; Marcus, B.; Patterson, R.; Parker, B.; Morey, B. Use of the fitbit to measure adherence to a physical activity intervention among overweight or obese, postmenopausal women: Self-monitoring trajectory during 16 weeks. J. Med. Internet Res. 2015, 3, e96. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Cadmus-Bertram, L.; Natarajan, L.; White, M.; Madanat, H.; Nichols, J.; Ayala, G.; Pierce, J. Wearable sensor/device (fitbit one) and sms text-messaging prompts to increase physical activity in overweight and obese adults: A randomized controlled trial. Telemed. E-Health 2015, 21, 782–792. [Google Scholar] [CrossRef] [PubMed]
- Thompson, W.; Kuhle, C.; Koepp, G.; McCrady-Spitzer, S.; Levine, J. “Go4life” exercise counseling, accelerometer feedback, and activity levels in older people. Arch. Gerontol. Geriatr. 2014, 58, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Thorndike, A.; Mills, S.; Sonnenberg, L.; Palakshappa, D.; Gao, T.; Pau, C.; Regan, S. Activity monitor intervention to promote physical activity of physicians-in-training: Randomized controlled trial. PLoS ONE 2014, 9, e100251. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Lumpkin, A.; Lochbaum, M.; Stegemeier, S.; Kitten, K. Promoting physical activity using wearable activity tracker in college students: A cluster randomized trial. J. Sports Sci. 2018, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Rote, A. Physical activity intervention using fitbits in an introductory college health course. Health Educ. J. 2017, 76, 337–348. [Google Scholar] [CrossRef]
- Melton, B.; Buman, M.; Vogel, R.; Harris, B.; Bigham, L. Wearable devices to improve physical activity and sleep: A randomized controlled trial of college-aged african american women. J. Black Stud. 2016, 47, 610–625. [Google Scholar] [CrossRef]
- Nielsen-Bohlman, L.; Panzer, A.; Kindig, D. Health Literacy: A Prescription to End Confusion; The National Academies Press: Washington, DC, USA, 2004. [Google Scholar]
- Rikard, R.; Thompson, M.; McKinney, J.; Beauchamp, A. Examining health literacy disparities in the United States: A third look at the national assessment of adult literacy (NAAL). BMC Public Health 2016, 16, 975. [Google Scholar] [CrossRef] [PubMed]
- Patten, M. The role of theory in research. In Understanding Research Methods: An Overview of the Essentials, 9th ed.; Patten, M., Ed.; Pyrczak Publishing: Glendale, CA, USA, 2014; pp. 27–29. [Google Scholar]
- Statista. Distribution of Facebook Users in the United States as of January 2017, by Age Group and Gender. Available online: https://www.statista.com/statistics/187041/us-user-age-distribution-on-facebook/ (accessed on 16 May 2018).
- Brug, J.; Oenema, A.; Ferreira, I. Theory, evidence, and intervention mapping to improve behavior, nutrition, and physical activity interventions. Int. J. Behav. Nutr. Phys. Act. 2005, 2, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, J.; Nelson, J.; Silverman, S. Developing the problem and using the literature. In Research Methods in Physical Activity, 6th ed.; Thomas, J., Nelson, J., Silverman, S., Eds.; Human Kinetics: Champaign, IL, USA, 2011; pp. 25–50. [Google Scholar]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Social Foundations of thought and Action: A Social Cognitive Theory; Prentice Hall: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Schulz, K.; Altman, D.; Moher, D.; Group, C. Consort 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMC Med. 2010, 8, 18. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects; World Medical Association: Washington, DC, USA, 2008; pp. 1–5. [Google Scholar]
- Canadian Society for Exercise Physiology. Par-Q Forms. Available online: http://www.csep.ca/view.asp?ccid=517 (accessed on 16 May 2018).
- Kaminsky, L.; Ozemek, C. A comparison of the actigraph gt1m and gt3x accelerometers under standardized and free-living conditions. Physiol. Meas. 2012, 33, 1869–1876. [Google Scholar] [CrossRef] [PubMed]
- Trost, S.; McIver, K.; Pate, R. Conducting accelerometer-based activity assessments in field-based research. Med. Sci. Sports Exerc. 2005, 37, S531–S543. [Google Scholar] [CrossRef] [PubMed]
- Troiano, R.; Berrigan, D.; Dodd, K.; Masse, L.; Tilert, T.; McDowell, M. Physical activity in the united states measured by accelerometer. Med. Sci. Sports Exerc. 2008, 40, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Aandstad, A.; Holtberget, K.; Hageberg, R.; Holme, I.; Anderssen, S. Validity and reliability of bioelectrical impedance analysis and skinfold thickness in predicting body fat in military personnel. Mil. Med. 2014, 179, 208–217. [Google Scholar] [CrossRef] [PubMed]
- Golding, L.; Meyers, C.; Sinning, W. Y’s Way to Physical Fitness: The Complete Guide to Fitness Testing and Instruction, 4th ed.; Human Kinetics: Champaign, IL, USA, 1998. [Google Scholar]
- Carlson, J.; Sallis, J.; Wagner, N.; Calfas, K.; Patrick, K.; Groesz, L.; Norman, G. Brief physical activity-related psychosocial measures: Reliability and construct validity. J. Phys. Act. Health 2012, 9, 1178–1186. [Google Scholar] [CrossRef] [PubMed]
- Sechrist, K.; Walker, S.; Pender, N. Development and psychometric evaluation of the exercise benefits/barriers scale. Res. Nurs. Health 1987, 10, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, W.; Wilson, P.; Hall, C.; Fraser, S.; Murray, T. Evidence for a multidimensional self-efficacy for exercise scale. Res. Q. Exerc. Sport 2008, 79, 222–234. [Google Scholar] [CrossRef] [PubMed]
- Harter, S. Effectance motivation reconsidered: Toward a developmental model. Hum. Dev. 1978, 21, 34–64. [Google Scholar] [CrossRef]
- Trost, S.; Pate, R.; Saunders, R.; Ward, D.; Dowda, M.; Felton, G. A prospective study of the determinants of physical activity in rural fifth-grade children. Prev. Med. 1997, 26, 257–263. [Google Scholar] [CrossRef] [PubMed]
- National Institutes of Health. Patient Reported Outcome Measurement Information System: Instrument Details. Available online: http://www.nihpromis.org/measures/instrumentdetails (accessed on 16 May 2018).
- Lin, F.-J.; Pickard, A.; Krishnan, J.; Joo, M.; Au, D.; Carson, S.; Gillespie, S.; Henderson, A.; Lindenauer, P.; McBurnie, M.; et al. Measuring health-related quality of life in chronic obstructive pulmonary disease: Properties of the eq-5d-5l and promis-43 short form. BMC Med. Res. Methodol. 2014, 14, 78. [Google Scholar] [CrossRef] [PubMed]
- Yost, K.; Eton, D.; Garcia, S.; Cella, D. Minimally important differences were estimated for six promis-cancer scales in advanced-stage cancer patients. J. Clin. Epidemiol. 2011, 64, 507–516. [Google Scholar] [CrossRef] [PubMed]
- Polar. Polar M400 Gps Running Watch. Available online: https://www.polar.com/us-en/products/sport/M400 (accessed on 16 May 2018).
- Arnold, M.; Leitzmann, M.; Freisling, H.; Bray, F.; Romieu, I.; Renehan, A.; Soerjomataram, I. Obesity and cancer: An update of the global impact. Cancer Epidemiol. 2016, 41, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Belardi, V.; Gallagher, E.; Novosyadlyy, R.; LeRoith, D. Insulin and IGFs in obesity-related breast cancer. J. Mammary Gland Biol. Neoplasia 2013, 18, 277–289. [Google Scholar] [CrossRef] [PubMed]
- Dieli-Conwright, C.; Lee, K.; Kiwata, J. Reducing the risk of breast cancer recurrence: An evaluation of the effects and mechanisms of diet and exercise. Curr. Breast Cancer Rep. 2016, 8, 139–150. [Google Scholar] [CrossRef] [PubMed]
- Pew Research Center. Older Adults and Technology Use. Available online: http://www.pewinternet.org/2014/04/03/older-adults-and-technology-use/ (accessed on 16 May 2018).
- Van Volkom, M.; Stapley, J.; Amaturo, V. Revisiting the digital divide: Generational differences in technology use in everyday life. N. Am. J. Psychol. 2014, 16, 557–574. [Google Scholar]
- Faria, S.; Faria, O.; Cardeal, M.; Ito, M. Validation study of multi-frequency bioelectrical impedance with dual-energy X-ray absorptiometry among obese patients. Obes. Surg. 2014, 24, 1476–1480. [Google Scholar] [CrossRef] [PubMed]
- Loprinzi, P.; Cardinal, B.; Winters-Stone, K.; Smit, E.; Loprinzi, C. Physical activity and the risk of breast cancer recurrence: A literature review. Oncol. Nurs. Forum 2012, 39, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Fallowfield, L.; Jenkins, V. Psychosocial/survivorship issues in breast cancer: Are we doing better. JNCI J. Natl. Cancer Inst. 2015, 107. [Google Scholar] [CrossRef] [PubMed]
- Accortt, E.; Bower, J.; Stanton, A.; Ganz, P. Depression and vasomotor symptoms in young breast cancer survivors: The mediating role of sleep disturbance. Arch. Women Ment. Health 2015, 18, 565–568. [Google Scholar] [CrossRef] [PubMed]
- Kohl, H., III; Murray, T. (Eds.) Overweight and obesity. In Foundations of Physical Activity and Public Health; Human Kinetics: Champaign, IL, USA, 2012; pp. 95–117. [Google Scholar]
- Dethlefsen, C.; Pedersen, K.S.; Hojman, P. Every exercise bout matters: Linking systemic exercise responses to breast cancer control. Breast Cancer Res. Treat. 2017, 162, 399–408. [Google Scholar] [CrossRef] [PubMed]
- Kenney, W.; Wilmore, J.; Costill, D. (Eds.) Body composition and nutrition for sport. In Physiology of Sport and Exercise; Human Kinetics: Champaign, IL, USA, 2015; pp. 371–405. [Google Scholar]
- Alberto, F.; Nathanael, M.; Mathew, B.; Ainsworth, B.E. Wearable monitors criterion validity for energy expenditure in sedentary and light activities. J. Sport Health Sci. 2017, 6, 103–110. [Google Scholar] [CrossRef]
- Theodoropoulou, E.; Stavrou, N.; Karteroliotis, K. Neighborhood environment, physical activity, and quality of life in adults: Intermediary effects of personal and psychosocial factors. J. Sport Health Sci. 2017, 6, 96–102. [Google Scholar] [CrossRef]


{kind=link}
| Demographic Characteristics (n = 30) | |||||
|---|---|---|---|---|---|
| Experimental (n = 16) | Comparison (n = 14) | ||||
| Avg. (M ± SD) | Freq. (Counts) | Avg. (M ± SD) | Freq. (Counts) | p-Value | |
| Age (years) | 50.6 ± 7.4 | 54.9 ± 11.0 | 0.23 | ||
| Race/ethnicity | 0.28 | ||||
| ● Caucasian | 16 | 13 | |||
| ● Hispanic | 0 | 1 | |||
| Educational status | 0.98 | ||||
| ● Some college/technical school | 2 | 2 | |||
| ● College graduate | 5 | 4 | |||
| ● Graduate school | 9 | 8 | |||
| Health insurance | 0.12 | ||||
| ● Private | 16 | 12 | |||
| ● Medicaid | 0 | 2 | |||
| Employment status | 0.46 | ||||
| ● Full time | 9 | 7 | |||
| ● Part time | 5 | 4 | |||
| ● Retired | 0 | 2 | |||
| ● Housewife | 2 | 1 | |||
| Marital status | 0.60 | ||||
| ● Married | 14 | 10 | |||
| ● Separated/divorced | 1 | 2 | |||
| ● Widowed | 0 | 1 | |||
| ● Living with unmarried partner | 1 | 1 | |||
| Annual income (USD) | 0.65 | ||||
| ● $10,001–20,000 | 1 | 1 | |||
| ● $30,001–40,000 | 1 | 2 | |||
| ● $40,001–50,000 | 0 | 1 | |||
| ● $50,000–74,999 | 0 | 1 | |||
| ● $75,000–99,999 | 4 | 3 | |||
| ● ≥$100,000 | 10 | 6 | |||
| Clinical Characteristics (n = 30) | |||||
| Time in remission | 60.7 ± 39.7 | 48.7 ± 31.7 | 0.37 | ||
| Months since diagnosis | 0.12 | ||||
| ● ≤12 months | 0 | 1 | |||
| ● 13 to 24 months | 5 | 1 | |||
| ● 25 to 36 months | 2 | 3 | |||
| ● 49 to 60 months | 0 | 3 | |||
| ● ≥61 months | 9 | 6 | |||
| Diagnosed breast cancer stage | 0.68 | ||||
| ● Stage 0 | 3 | 1 | |||
| ● Stage 1 | 4 | 5 | |||
| ● Stage 2 | 7 | 5 | |||
| ● Stage 3 | 2 | 3 | |||
| Treatment type | 0.64 | ||||
| ● Surgery only | 2 | 4 | |||
| ● Surgery + radiation | 2 | 1 | |||
| ● Surgery + chemo | 5 | 5 | |||
| ● Surgery + radiation + chemo | 7 | 4 | |||
| Tamoxifen use | 0.92 | ||||
| ● Yes | 10 | 9 | |||
| ● No | 6 | 5 | |||
| Follow-up care in past 12 months | 1.00 | ||||
| ● Yes | 16 | 14 | |||
| ● No | 0 | 0 | |||
| Clinical breast exam frequency | 0.57 | ||||
| ● Never | 1 | 0 | |||
| ● Every 3–6 months | 2 | 2 | |||
| ● Every 6–12 months | 5 | 5 | |||
| ● Once yearly | 6 | 7 | |||
| ● Other | 2 | 0 | |||
| Comorbidities | 0.23 | ||||
| ● None | 13 | 14 | |||
| ● 1 | 1 | 0 | |||
| ● ≥2 | 2 | 0 | |||
| Experimental (n = 16) | Comparison (n = 14) | p-Value | |
|---|---|---|---|
| Primary Outcomes | |||
| Daily MVPA | 26.7 ± 18.4 | 20.9 ± 17.6 | 0.40 |
| Daily LPA | 72.9 ± 44.1 | 77.3 ± 48.2 | 0.80 |
| Daily SB | 378.0 ± 192.5 | 361.7 ± 201.0 | 0.82 |
| Daily EE | 272.5 ± 166.6 | 303.1 ± 240.9 | 0.69 |
| Daily steps | 4099.8 ± 2651.6 | 3092.7 ± 2214.0 | 0.27 |
| Secondary Outcomes | |||
| Physiological variables | |||
| Weight (kg) | 76.0 ± 13.0 | 85.0 ± 24.9 | 0.24 |
| Body fat (%) | 39.4 ± 5.5 | 38.6 ± 9.8 | 0.81 |
| Cardiorespiratory fitness | 113.2 ± 20.7 | 106.1 ± 23.4 | 0.39 |
| Psychosocial variables | |||
| Self-efficacy # | 73.3 ± 22.1 | 80.3 ± 14.5 | 0.33 |
| Social support $ | 2.8 ± 1.1 | 2.1 ± 1.0 | 0.06 |
| Enjoyment $ | 3.2 ± 0.5 | 3.3 ± 0.5 | 0.55 |
| Barriers @ | 2.0 ± 0.5 | 1.9 ± 0.4 | 0.57 |
| Outcome expectancy $ | 3.9 ± 0.5 | 4.1 ± 0.5 | 0.55 |
| Quality of life variables | |||
| Physical functioning ** | 1.2 ± 0.4 | 1.3 ± 0.3 | 0.64 |
| Anxiety ** | 1.8 ± 0.8 | 1.5 ± 0.7 | 0.34 |
| Depression ** | 1.3 ± 0.3 | 1.1 ± 0.3 | 0.21 |
| Fatigue ** | 2.5 ± 1.1 | 2.3 ± 0.6 | 0.51 |
| Sleep quality ** | 3.1 ± 1.0 | 3.4 ± 0.9 | 0.39 |
| Sleep disturbances ** | 2.9 ± 0.6 | 2.6 ± 0.5 | 0.17 |
| Social roles/activities limitations ** | 2.2 ± 1.1 | 2.1 ± 0.8 | 0.76 |
| Pain limitations ** | 1.7 ± 0.8 | 1.5 ± 0.6 | 0.51 |
| Pain intensity & | 2.0 ± 1.3 | 2.2 ± 1.9 | 0.72 |
| Experimental (n = 12) | Comparison (n = 8) | p-Value b | |||
|---|---|---|---|---|---|
| Baseline | 10 Weeks | Baseline | 10 Weeks | ||
| Daily MVPA | 30.7 ± 13.2 | 34.2 ± 18.7 | 30.2 ± 16.2 | 37.8 ± 20.4 | 0.49 |
| Daily LPA | 91.4 ± 28.8 | 98.9 ± 29.5 | 100.4 ± 31.6 | 108.5 ± 47.9 | 0.76 |
| Daily SB | 464.4 ± 50.7 | 466.8 ± 34.7 | 449.2 ± 54.9 | 449.6 ± 53.2 | 0.82 |
| Daily EE | 333.1 ± 113.3 | 359.9 ± 147.4 | 395.5 ± 229.9 | 418.0 ± 188.9 | 0.44 |
| Daily steps | 4832.4 ± 1816.4 | 5175.1 ± 2308.2 | 4411.6 ± 1624.7 | 4746.0 ± 2044.9 | 0.76 |
| Experimental (n = 12) | Comparison (n = 8) | p-Value b | |||
|---|---|---|---|---|---|
| Baseline | 10 Weeks | Baseline | 10 Weeks | ||
| Physiological variables | |||||
| Weight (kg) | 76.6 ± 13.3 | 76.9 ± 12.2 | 78.0 ± 22.6 | 78.0 ± 23.0 | 0.62 |
| Body fat (%) | 39.8 ± 6.0 | 40.2 ± 5.4 | 36.0 ± 10.6 | 35.0 ± 10.8 | 0.12 |
| Cardiorespiratory fitness | 110.4 ± 18.5 | 105.7 ± 21.7 | 104.8 ± 29.3 | 100.3 ± 21.6 | 0.97 |
| Psychosocial variables | |||||
| Self-efficacy # | 75.6 ± 25.1 | 67.9 ± 26.5 | 78.2 ± 12.1 | 71.8 ± 14.8 | 0.98 |
| Social support $ | 3.0 ± 1.1 | 2.7 ± 1.3 | 2.4 ± 1.1 | 3.0 ± 1.1 | 0.05 |
| Enjoyment $ | 3.3 ± 0.5 | 3.2 ± 0.5 | 3.2 ± 0.6 | 3.3 ± 0.6 | 0.53 |
| Barriers @ | 2.0 ± 0.5 | 2.0 ± 0.5 | 2.1 ± 0.2 | 1.8 ± 0.4 | 0.04 |
| Outcome expectancy $ | 4.1 ± 0.5 | 3.9 ± 0.5 | 4.0 ± 0.6 | 4.0 ± 0.6 | 0.34 |
| Experimental (n = 12) | Comparison (n = 8) | p-Value b | |||
|---|---|---|---|---|---|
| Baseline | 10 Weeks | Baseline | 10 Weeks | ||
| Physical functioning ** | 1.1 ± 0.2 | 1.1 ± 0.2 | 1.2 ± 0.2 | 1.1 ± 0.2 | 0.78 |
| Anxiety ** | 1.8 ± 0.8 | 2.0 ± 0.8 | 1.7 ± 0.7 | 1.5 ± 0.7 | 0.19 |
| Depression ** | 1.2 ± 0.3 | 1.4 ± 0.4 | 1.1 ± 0.3 | 1.1 ± 0.1 | 0.41 |
| Fatigue ** | 2.3 ± 1.0 | 2.3 ± 0.8 | 2.4 ± 0.6 | 2.2 ± 0.9 | 0.31 |
| Sleep quality ** | 3.1 ± 0.9 | 3.3 ± 0.6 | 3.6 ± 0.9 | 3.5 ± 0.9 | 0.62 |
| Sleep disturbances ** | 2.8 ± 0.6 | 2.5 ± 0.4 | 2.5 ± 0.5 | 2.5 ± 0.4 | 0.64 |
| Social roles/activities limitations ** | 2.0 ± 0.9 | 1.8 ± 0.7 | 1.9 ± 0.7 | 1.9 ± 0.5 | 0.64 |
| Pain limitations ** | 1.5 ± 0.5 | 1.5 ± 0.6 | 1.4 ± 0.5 | 1.4 ± 0.4 | 1.0 |
| Pain intensity & | 1.8 ± 1.0 | 1.8 ± 1.8 | 2.0 ± 1.9 | 1.8 ± 1.4 | 0.97 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pope, Z.C.; Zeng, N.; Zhang, R.; Lee, H.Y.; Gao, Z. Effectiveness of Combined Smartwatch and Social Media Intervention on Breast Cancer Survivor Health Outcomes: A 10-Week Pilot Randomized Trial. J. Clin. Med. 2018, 7, 140. https://doi.org/10.3390/jcm7060140
Pope ZC, Zeng N, Zhang R, Lee HY, Gao Z. Effectiveness of Combined Smartwatch and Social Media Intervention on Breast Cancer Survivor Health Outcomes: A 10-Week Pilot Randomized Trial. Journal of Clinical Medicine. 2018; 7(6):140. https://doi.org/10.3390/jcm7060140
Chicago/Turabian StylePope, Zachary C., Nan Zeng, Rui Zhang, Hee Yun Lee, and Zan Gao. 2018. "Effectiveness of Combined Smartwatch and Social Media Intervention on Breast Cancer Survivor Health Outcomes: A 10-Week Pilot Randomized Trial" Journal of Clinical Medicine 7, no. 6: 140. https://doi.org/10.3390/jcm7060140
APA StylePope, Z. C., Zeng, N., Zhang, R., Lee, H. Y., & Gao, Z. (2018). Effectiveness of Combined Smartwatch and Social Media Intervention on Breast Cancer Survivor Health Outcomes: A 10-Week Pilot Randomized Trial. Journal of Clinical Medicine, 7(6), 140. https://doi.org/10.3390/jcm7060140