Preoperative and Postoperative Assessment of Ultrasonographic Measurement of Inferior Vena Cava: A Prospective, Observational Study


Abstract
:1. Introduction
2. Material and Methods
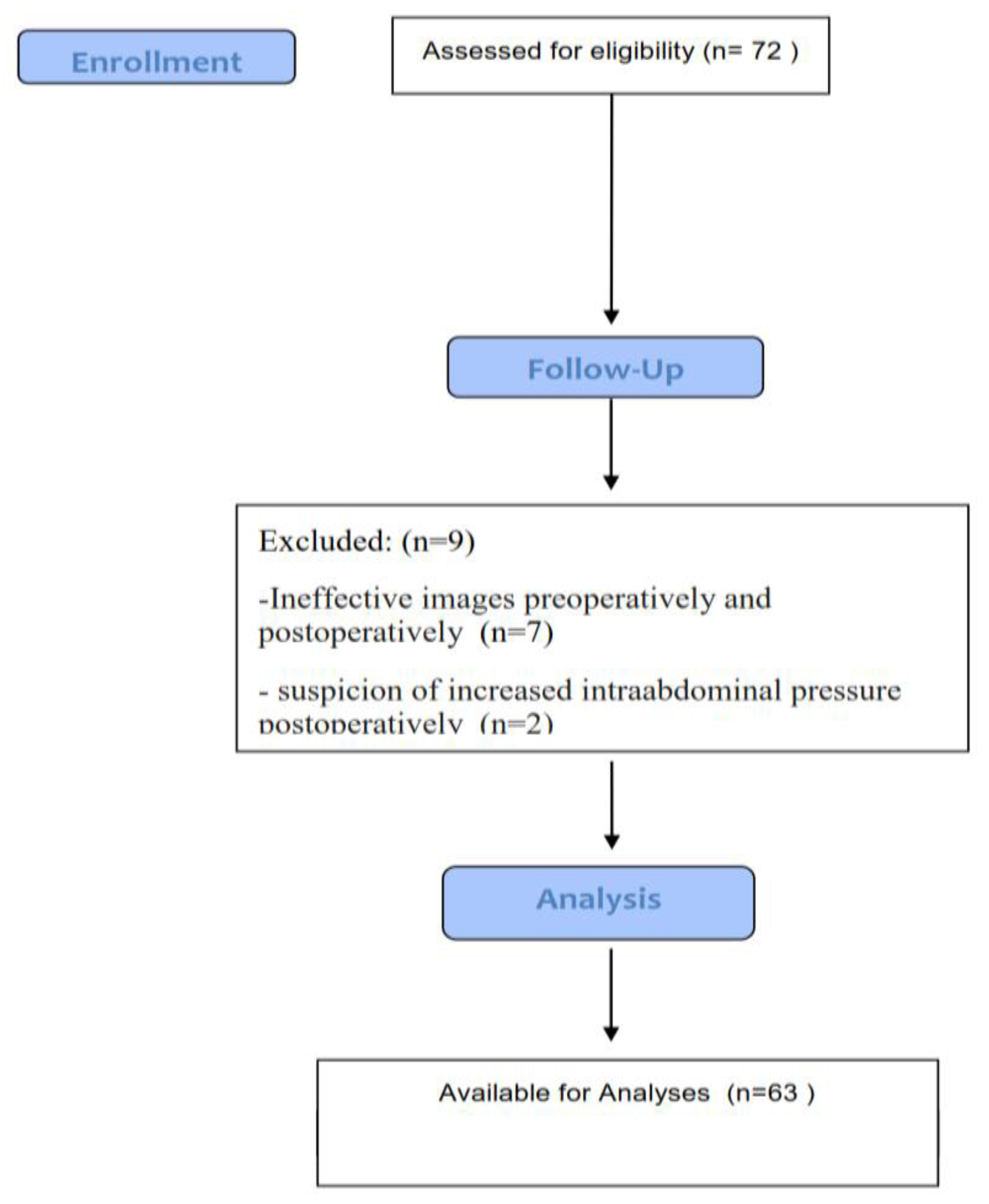
2.1. Patients
2.2. Preoperative Procedure
2.3. Anesthesia Management
2.4. Intraoperative Fluid Management
2.5. Postperative Procedure
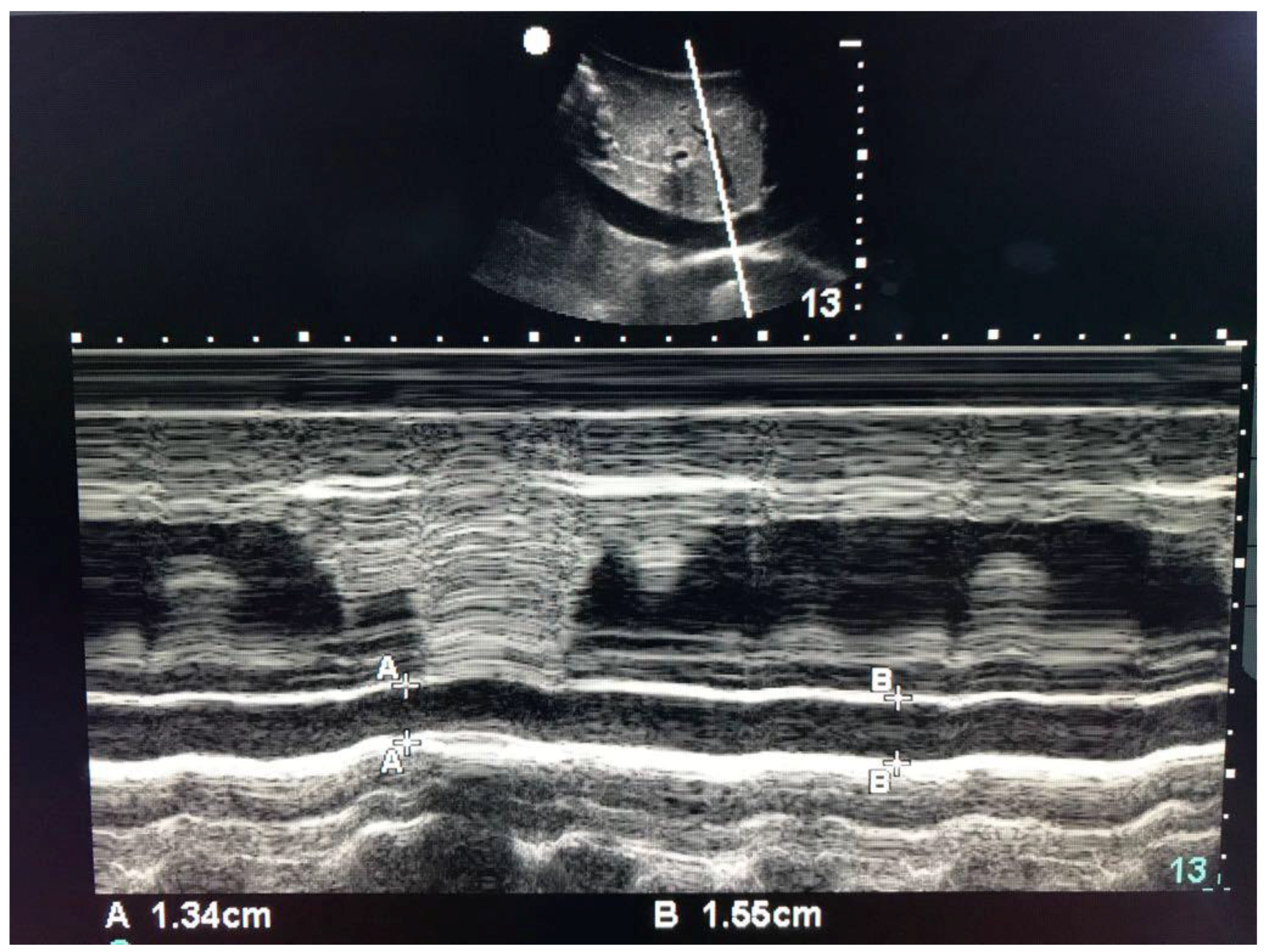
2.6. Data Collection
2.7. Statistical Analyses
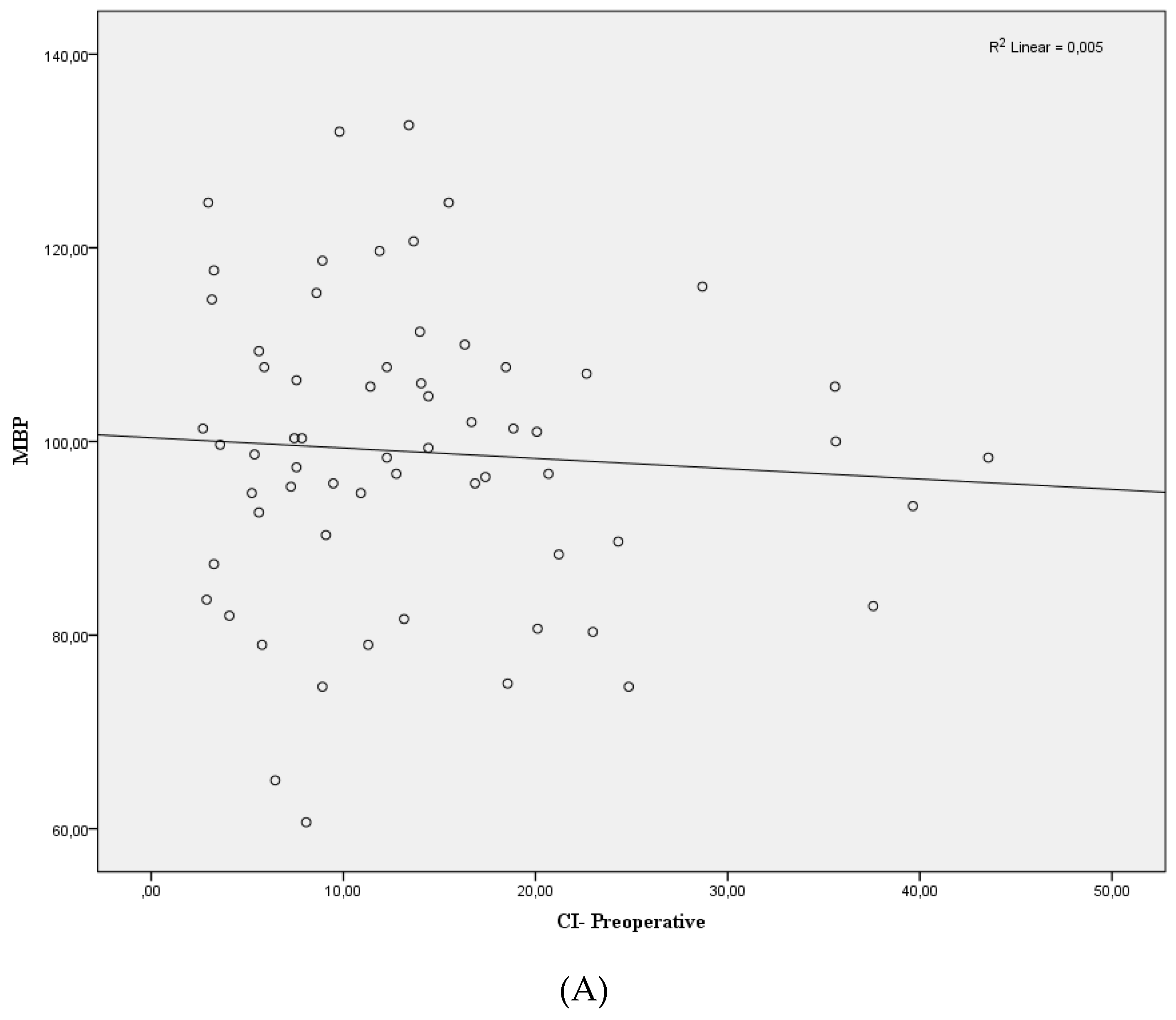
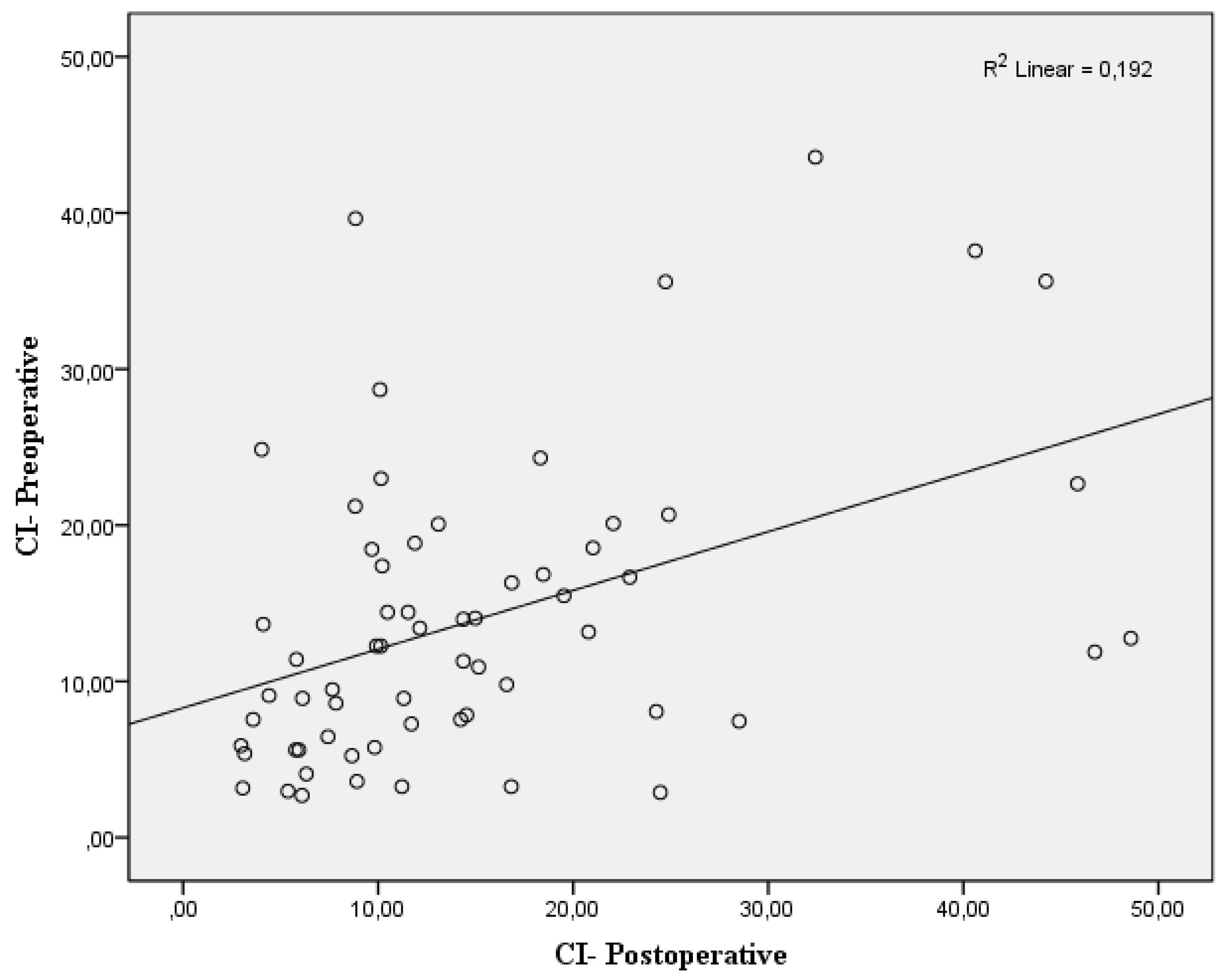
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Michard, F.; Biais, M. Rational fluid management: Dissecting facts from fiction. Br. J. Anaesth. 2012, 108, 369–371. [Google Scholar] [CrossRef] [PubMed]
- Chappell, D.; Jacob, M.; Hofmann-Kiefer, K.; Conzen, P.; Rehm, M. A rational approach to perioperative fluid management. Anesthesiology 2008, 109, 723–740. [Google Scholar] [CrossRef] [PubMed]
- Osman, D.; Ridel, C.; Ray, P.; Monnet, X.; Anguel, N.; Richard, C.; Teboul, J.L. Cardiac filling pressures are not appropriate to predict hemodynamic response to volume challenge. Crit. Care Med. 2007, 35, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Berger, M.M.; Gradwohl-Matis, I.; Brunauer, A.; Ulmer, H.; Dünser, M.W. Targets of perioperative fluid therapy and their effects on postoperative outcome: A systematic review and meta-analysis. Minerva Anestesiol. 2015, 81, 794–808. [Google Scholar] [PubMed]
- Noblett, S.E.; Snowden, C.P.; Shenton, B.K.; Horgan, A.F. Randomized clinical trial assessing the effect of Doppler-optimized fluid management on outcome after elective colorectal resection. Br. J. Surg. 2006, 93, 1069–1076. [Google Scholar] [CrossRef] [PubMed]
- Sefidbakht, S.; Assadsangabi, R.; Abbasi, H.R.; Nabavizadeh, A. Sonographic measurement of the inferior vena cava as a predictor of shock in trauma patients. Emerg. Radiol. 2007, 14, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Arthur, M.E.; Landolfo, C.; Wade, M.; Castresana, M.R. Inferior Vena Cava Diameter (IVCD) Measured with Transesophageal Echocardiography (TEE) can be used to derive the Central Venous Pressure (CVP) in anesthetized mechanically ventilated patients. Echocardiography 2009, 26, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Brennan, J.M.; Ronan, A.; Goonewardena, S.; Blair, J.E.A.; Hammes, M.; Shah, D.; Vasaiwala, S.; Kirkpatrick, J.N.; Spencer, K.T. Handcarried ultrasound measurement of the inferior vena cava for assessment of intravascular volume status in the outpatient hemodialysis clinic. Clin. J. Am. Soc. Nephrol. 2006, 1, 749–753. [Google Scholar] [CrossRef] [PubMed]
- Dipti, A.; Soucy, Z.; Surana, A.; Chandra, S. Role of inferior vena cava diameter in assessment of volume status: A meta-analysis. Am. J. Emerg. Med. 2012, 30. [Google Scholar] [CrossRef] [PubMed]
- Sakurai, T.; Ando, Y.; Masunaga, Y.; Kusano, E.; Asano, Y. Diameter of the inferior vena cava as an index of dry weight in patients undergoing CAPD. Perit. Dial. Int. 1996, 16, 183–185. [Google Scholar] [PubMed]
- Lyon, M.; Blaivas, M.; Brannam, L. Sonographic measurement of the inferior vena cava as a marker of blood loss. Am. J. Emerg. Med. 2005, 23, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Barbier, C.; Loubières, Y.; Schmit, C.; Hayon, J.; Ricôme, J.L.; Jardin, F.; Vieillard-Baron, A. Respiratory changes in inferior vena cava diameter are helpful in predicting fluid responsiveness in ventilated septic patients. Intensive Care Med. 2004, 30, 1740–1746. [Google Scholar] [CrossRef] [PubMed]
- Feissel, M.; Michard, F.; Faller, J.P.; Teboul, J.L. The respiratory variation in inferior vena cava diameter as a guide to fluid therapy. Intensive Care Med. 2004, 30, 1834–1837. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Xu, X.; Ye, S.; Xu, L. Ultrasonographic measurement of the respiratory variation in the inferior vena cava diameter is predictive of fluid responsiveness in critically ill patients: Systematic review and meta-analysis. Ultrasound Med. Biol. 2014, 40, 845–853. [Google Scholar] [CrossRef] [PubMed]
- Brun, C.; Zieleskiewicz, L.; Textoris, J.; Muller, L.; Bellefleur, J.P.; Antonini, F.; Tourret, M.; Ortega, D.; Vellin, A.; Lefrant, J.Y.; et al. Prediction of fluid responsiveness in severe preeclamptic patients with oliguria. Intensive Care Med. 2013, 39, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z. Univariate description and bivariate statistical inference: The first step delving into data. Ann. Transl. Med. 2016, 4, 91. [Google Scholar] [CrossRef] [PubMed]
- Airapetian, N.; Maizel, J.; Alyamani, O.; Mahjoub, Y.; Lorne, E.; Levrard, M.; Ammenouche, N.; Seydi, A.; Tinturier, F.; Lobjoie, E.; et al. Does inferior vena cava respiratory variability predict fluid responsiveness in spontaneously breathing patients? Crit. Care 2015, 19, 400. [Google Scholar] [CrossRef] [PubMed]
- Muller, L.; Bobbia, X.; Toumi, M.; Louart, G.; Molinari, N.; Ragonnet, B.; Quintard, H.; Leone, M.; Zoric, L.; Lefrant, J.Y.; et al. Respiratory variations of inferior vena cava diameter to predict fluid responsiveness in spontaneously breathing patients with acute circulatory failure: Need for a cautious use. Crit. Care 2012, 16, R188. [Google Scholar] [CrossRef] [PubMed]
- Wallace, D.J.; Allison, M.; Stone, M.B. Inferior vena cava percentage collapse during respiration is affected by the sampling location: An ultrasound study in healthy volunteers. Acad. Emerg. Med. 2010, 17, 96–99. [Google Scholar] [CrossRef] [PubMed]
- Simonson, J.; Schiller, N. new method for noninvasive estimation of mean right atrial pressure based on two-dimensional echographic measurements of the inferior vena cava during measured. J. Am. Coll. Cardiol. 1988, 11, 557–564. [Google Scholar] [CrossRef]
- Nagdev, A.D.; Merchant, R.C.; Tirado-Gonzalez, A.; Sisson, C.A.; Murphy, M.C. Emergency department bedside ultrasonographic measurement of the caval index for noninvasive determination of low central venous pressure. Ann. Emerg. Med. 2010, 55, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Muller, L.; Briere, M.; Bastide, S.; Roger, C.; Zoric, L.; Seni, G.; de La Coussaye, J.E.; Ripart, J.; Lefrant, J.Y. Preoperative fasting does not affect haemodynamic status: A prospective, non-inferiority, echocardiography study. Br. J. Anaesth. 2014, 112, 835–841. [Google Scholar] [CrossRef] [PubMed]
- Bundgaard-Nielsen, M.; Jørgensen, C.C.; Secher, N.H.; Kehlet, H. Functional intravascular volume deficit in patients before surgery. Acta Anaesthesiol. Scand. 2010, 54, 464–469. [Google Scholar] [CrossRef] [PubMed]
- Jacob, M.; Chappell, D.; Conzen, P.; Finsterer, U.; Rehm, M. Blood volume is normal after pre-operative overnight fasting. Acta Anaesthesiol. Scand. 2008, 52, 522–529. [Google Scholar] [CrossRef] [PubMed]
- Zengin, S.; Al, B.; Genc, S.; Yildirim, C.; Ercan, S.; Dogan, M.; Altunbas, G. Role of inferior vena cava and right ventricular diameter in assessment of volume status: A comparative study: Ultrasound and hypovolemia. Am. J. Emerg. Med. 2013, 31, 763–767. [Google Scholar] [CrossRef] [PubMed]
- Seif, D.; Mailhot, T.; Perera, P.; Mandavia, D. Caval sonography in shock a noninvasive method for evaluating intravascular volume in critically ILL patients. J. Ultrasound Med. 2012, 31, 1885–1890. [Google Scholar] [CrossRef] [PubMed]
- Hamilton-Davies, C.; Mythen, M.G.; Salmon, J.B.; Jacobson, D.; Shukla, A.; Webb, A.R. Comparison of commonly used clinical indicators of hypovolaemia with gastrointestinal tonometry. Intensive Care Med. 1997, 23, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Marik, P.E.; Baram, M.; Vahid, B. Does central venous pressure predict fluid responsiveness? A systematic review of the literature and the tale of seven mares. Chest 2008, 134, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Holte, K. Pathophysiology and clinical implications of peroperative fluid management in elective surgery. Dan. Med. Bull. 2010, 57, B4156. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Value |
|---|---|
| Age (years) | 42.88 ± 17.38 (18–86) |
| Gender (M/F) | 32/31 |
| Height (cm) | 166.37 ± 9.18 (148–186) |
| Weight (kg) | 71.36 ± 11.76 (53–105) |
| BMI (kg/m2) | 25.73 ± 4.07 (17.72–37.78) |
| Operation duration (min) | 78.30 ± 45.45 (20–216) |
| Peroperatively infused fluid | 985.80 ± 484.27 (150–2500) |
| Preoperative hemodynamic parameters | |
| Preop Systolic BP | 136.40 ± 22.17 |
| Preop Diastolic BP | 80.14 ± 13.80 |
| Preop MBP | 98.88 ± 15.25 |
| ASA | |
| ASA I | 35 |
| ASA II | 22 |
| ASA III | 6 |
| Comorbidities | |
| Hypertension | 6 |
| Diabetes mellitus | 4 |
| Cardiovascular | 2 |
| Respiratory | 2 |
| Type of surgery | |
| General surgery | 33 |
| Orthopedia | 16 |
| Urology | 6 |
| Otolaryngology | 4 |
| Neurosurgery | 4 |
| Planned Anesthesia | |
| General | 39 |
| Spinal | 20 |
| Regional block | 4 |
| Surgery | |
| Emergency | 16 |
| Elective | 47 |
| Total | 63 |
| Characteristic | preop | postop | p |
|---|---|---|---|
| IVC max diameter (cm ± SD) | 1.99 ± 0.31 | 2.05 ± 0.29 | 0.063 |
| IVC min diameter (cm ± SD) | 1.72 ± 0.33 | 1.74 ± 0.32 | 0.407 |
| CI index % | 14.0 ± 9.60 | 15.14 ± 11.18 | 0.416 |
| SBP | 136.39 ± 22.17 | 135.19 ± 24.19 | 0.710 |
| DBP | 80.14 ± 13.80 | 78.93 ± 17.26 | 0.605 |
| MBP | 98.89 ± 15.25 | 97.68 ± 18.24 | 0.621 |
| Total | 63 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaydu, A.; Gokcek, E. Preoperative and Postoperative Assessment of Ultrasonographic Measurement of Inferior Vena Cava: A Prospective, Observational Study. J. Clin. Med. 2018, 7, 145. https://doi.org/10.3390/jcm7060145
Kaydu A, Gokcek E. Preoperative and Postoperative Assessment of Ultrasonographic Measurement of Inferior Vena Cava: A Prospective, Observational Study. Journal of Clinical Medicine. 2018; 7(6):145. https://doi.org/10.3390/jcm7060145
Chicago/Turabian StyleKaydu, Ayhan, and Erhan Gokcek. 2018. "Preoperative and Postoperative Assessment of Ultrasonographic Measurement of Inferior Vena Cava: A Prospective, Observational Study" Journal of Clinical Medicine 7, no. 6: 145. https://doi.org/10.3390/jcm7060145
APA StyleKaydu, A., & Gokcek, E. (2018). Preoperative and Postoperative Assessment of Ultrasonographic Measurement of Inferior Vena Cava: A Prospective, Observational Study. Journal of Clinical Medicine, 7(6), 145. https://doi.org/10.3390/jcm7060145