SET Overexpression is Associated with Worse Recurrence-Free Survival in Patients with Primary Breast Cancer Receiving Adjuvant Tamoxifen Treatment

Abstract
:1. Introduction
2. Experimental Section
2.1. Patients
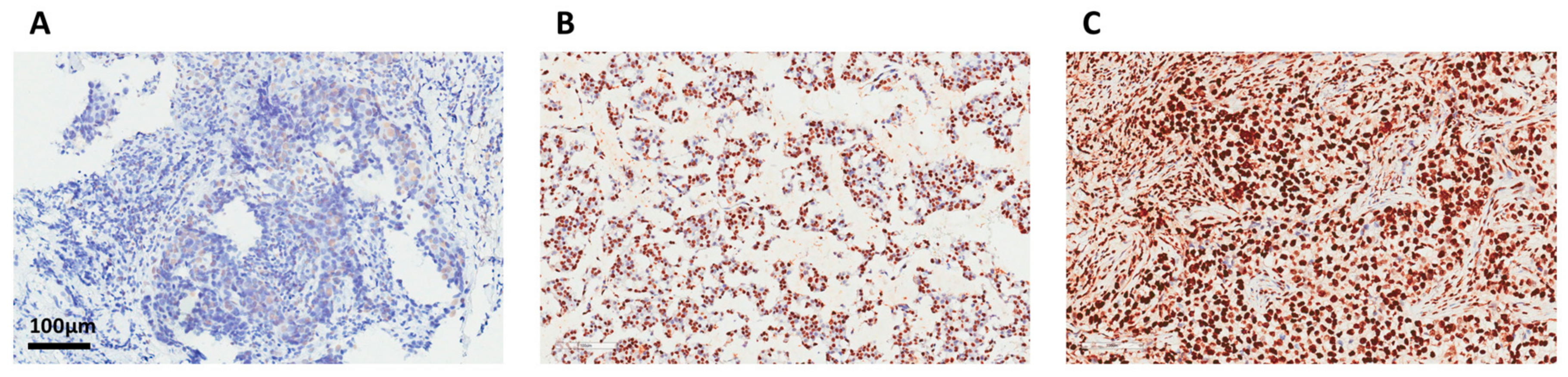
2.2. Immunohistochemistry
2.3. Determination of Histology Score (H-Score)
2.4. In Silico Survival Analysis with Public Open Database
2.5. Reagents and Antibodies
2.6. Cell Culture and Western Blot Analysis
2.7. Transient Transfection
2.8. Cell Viability Assay
2.9. Dual Luciferase Assay
2.10. Statistical Analysis
3. Results
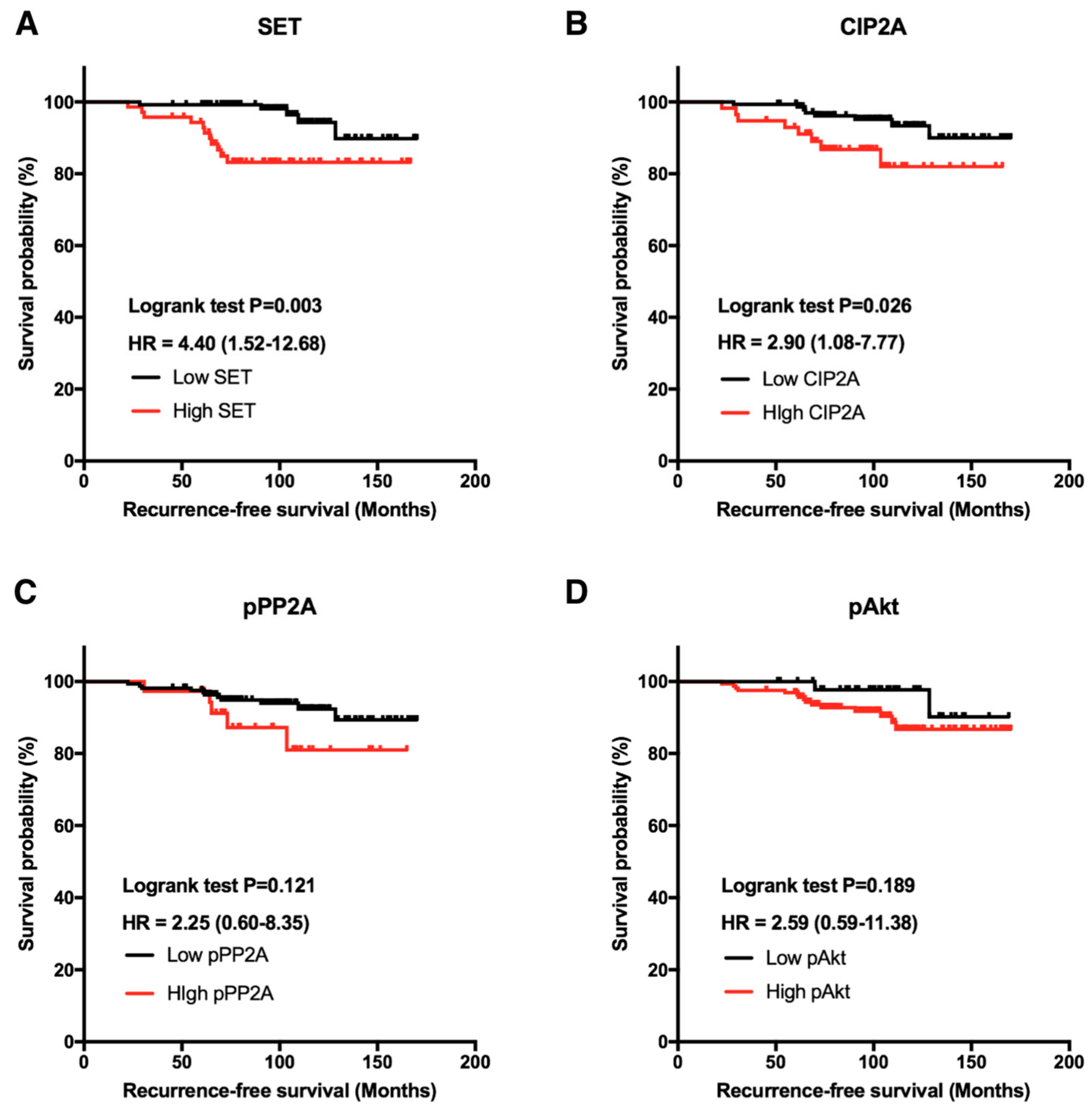
3.1. Clinical Significance of Biomarkers SET and CIP2A in Patients with Breast Cancer
3.2. Biomarker SET is an Independent Prognostic Predictor in ER-Positive Breast Cancer Receiving Adjuvant Tamoxifen Treatment
3.3. In Silico Analysis of Correlation of SET Gene Expression with Outcome in Public Data
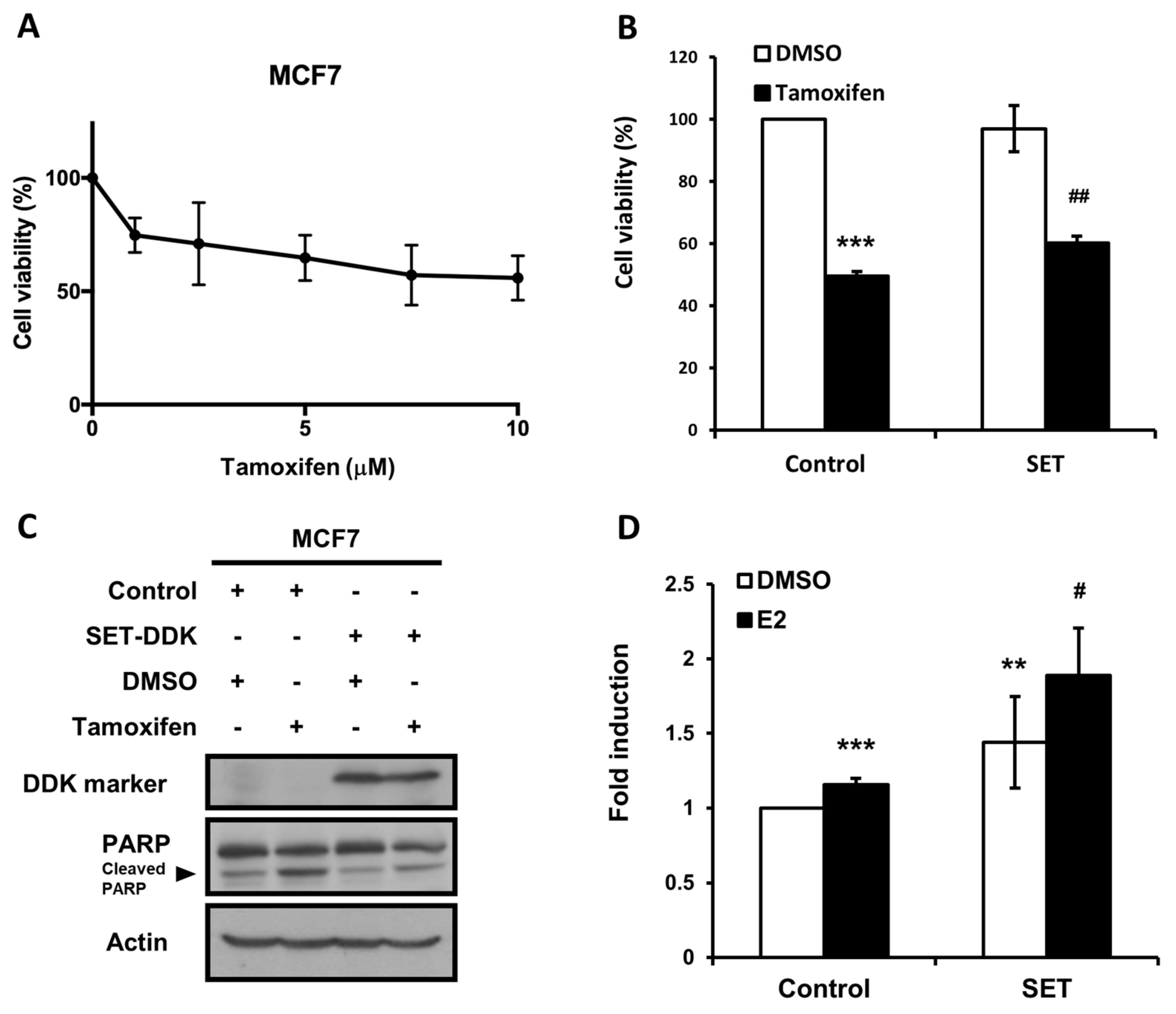
3.4. Overexpression of SET Suppressed the Anti-Cancer Effects of Tamoxifen on MCF7 Cells
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cheng, L.; Swartz, M.D.; Zhao, H.; Kapadia, A.S.; Lai, D.; Rowan, P.J.; Buchholz, T.A.; Giordano, S.H. Hazard of recurrence among women after primary breast cancer treatment-a 10-year follow-up using data from seer-medicare. Cancer Epidemiol. Biomark. Prev. 2012, 21, 800–809. [Google Scholar] [CrossRef] [PubMed]
- Ribelles, N.; Perez-Villa, L.; Jerez, J.M.; Pajares, B.; Vicioso, L.; Jimenez, B.; de Luque, V.; Franco, L.; Gallego, E.; Marquez, A.; et al. Pattern of recurrence of early breast cancer is different according to intrinsic subtype and proliferation index. Breast Cancer Res. 2013, 15, R98. [Google Scholar] [CrossRef] [PubMed]
- Metzger-Filho, O.; Sun, Z.; Viale, G.; Price, K.N.; Crivellari, D.; Snyder, R.D.; Gelber, R.D.; Castiglione-Gertsch, M.; Coates, A.S.; Goldhirsch, A.; et al. Patterns of recurrence and outcome according to breast cancer subtypes in lymph node-negative disease: Results from international breast cancer study group trials viii and ix. J. Clin. Oncol. 2013, 31, 3083–3090. [Google Scholar] [CrossRef] [PubMed]
- Early Breast Cancer Trialists’ Collaborative Group. Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: An overview of the randomised trials. Lancet 2005, 365, 1687–1717. [Google Scholar]
- Cossetti, R.J.; Tyldesley, S.K.; Speers, C.H.; Zheng, Y.; Gelmon, K.A. Comparison of breast cancer recurrence and outcome patterns between patients treated from 1986 to 1992 and from 2004 to 2008. J. Clin. Oncol. 2015, 33, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Early Breast Cancer Trialists’ Collaborative Group; Davies, C.; Godwin, J.; Gray, R.; Clarke, M.; Cutter, D.; Darby, S.; McGale, P.; Pan, H.C.; Taylor, C.; et al. Relevance of breast cancer hormone receptors and other factors to the efficacy of adjuvant tamoxifen: Patient-level meta-analysis of randomised trials. Lancet 2011, 378, 771–784. [Google Scholar]
- Dowsett, M.; Cuzick, J.; Ingle, J.; Coates, A.; Forbes, J.; Bliss, J.; Buyse, M.; Baum, M.; Buzdar, A.; Colleoni, M.; et al. Meta-analysis of breast cancer outcomes in adjuvant trials of aromatase inhibitors versus tamoxifen. J. Clin. Oncol. 2010, 28, 509–518. [Google Scholar] [CrossRef] [PubMed]
- Schiavon, G.; Smith, I.E. Status of adjuvant endocrine therapy for breast cancer. Breast Cancer Res. 2014, 16, 206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisher, B.; Jeong, J.H.; Bryant, J.; Anderson, S.; Dignam, J.; Fisher, E.R.; Wolmark, N. Treatment of lymph-node-negative, oestrogen-receptor-positive breast cancer: Long-term findings from national surgical adjuvant breast and bowel project randomised clinical trials. Lancet 2004, 364, 858–868. [Google Scholar] [CrossRef]
- Rea, D.; Handley, K.; Bowden, S.J.; Perry, P.; Earl, H.M.; Poole, C.J.; Bates, T.; Chetiyawardana, S.; Dewar, J.A.; Fernando, I.N.; et al. Attom: Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years in 6953 women with early breast cancer. J. Clin. Oncol. 2013, 31, 5. [Google Scholar]
- Davies, C.; Pan, H.; Godwin, J.; Gray, R.; Arriagada, R.; Raina, V.; Abraham, M.; Medeiros Alencar, V.H.; Badran, A.; Bonfill, X.; et al. Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor-positive breast cancer: Atlas, a randomised trial. Lancet 2013, 381, 805–816. [Google Scholar] [CrossRef]
- Lee, E.S.; Han, W.; Kim, M.K.; Kim, J.; Yoo, T.K.; Lee, M.H.; Lee, K.H.; Kim, T.Y.; Moon, H.G.; Im, S.A.; et al. Factors associated with late recurrence after completion of 5-year adjuvant tamoxifen in estrogen receptor positive breast cancer. BMC Cancer 2016, 16, 430. [Google Scholar] [CrossRef] [PubMed]
- Sestak, I.; Dowsett, M.; Zabaglo, L.; Lopez-Knowles, E.; Ferree, S.; Cowens, J.W.; Cuzick, J. Factors predicting late recurrence for estrogen receptor-positive breast cancer. J. Natl. Cancer Inst. 2013, 105, 1504–1511. [Google Scholar] [CrossRef] [PubMed]
- Colombo, P.E.; Milanezi, F.; Weigelt, B.; Reis-Filho, J.S. Microarrays in the 2010s: The contribution of microarray-based gene expression profiling to breast cancer classification, prognostication and prediction. Breast Cancer Res. 2011, 13, 212. [Google Scholar] [CrossRef] [PubMed]
- Paik, S.; Shak, S.; Tang, G.; Kim, C.; Baker, J.; Cronin, M.; Baehner, F.L.; Walker, M.G.; Watson, D.; Park, T.; et al. A multigene assay to predict recurrence of tamoxifen-treated, node-negative breast cancer. N. Engl. J. Med. 2004, 351, 2817–2826. [Google Scholar] [CrossRef] [PubMed]
- Paik, S.; Tang, G.; Shak, S.; Kim, C.; Baker, J.; Kim, W.; Cronin, M.; Baehner, F.L.; Watson, D.; Bryant, J.; et al. Gene expression and benefit of chemotherapy in women with node-negative, estrogen receptor-positive breast cancer. J. Clin. Oncol. 2006, 24, 3726–3734. [Google Scholar] [CrossRef] [PubMed]
- Seshacharyulu, P.; Pandey, P.; Datta, K.; Batra, S.K. Phosphatase: PP2A structural importance, regulation and its aberrant expression in cancer. Cancer Lett. 2013, 335, 9–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruvolo, P.P. The broken “off” switch in cancer signaling: PP2A as a regulator of tumorigenesis, drug resistance, and immune surveillance. BBA Clin. 2016, 6, 87–99. [Google Scholar] [CrossRef] [PubMed]
- Janghorban, M.; Farrell, A.S.; Allen-Petersen, B.L.; Pelz, C.; Daniel, C.J.; Oddo, J.; Langer, E.M.; Christensen, D.J.; Sears, R.C. Targeting c-MYC by antagonizing PP2A inhibitors in breast cancer. Proc. Natl. Acad. Sci. USA 2014, 111, 9157–9162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perrotti, D.; Neviani, P. Protein phosphatase 2A: A target for anticancer therapy. Lancet Oncol. 2013, 14, e229-238. [Google Scholar] [CrossRef]
- Liu, C.Y.; Hung, M.H.; Wang, D.S.; Chu, P.Y.; Su, J.C.; Teng, T.H.; Huang, C.T.; Chao, T.T.; Wang, C.Y.; Shiau, C.W.; et al. Tamoxifen induces apoptosis through cancerous inhibitor of protein phosphatase 2A-dependent phospho-akt inactivation in estrogen receptor-negative human breast cancer cells. Breast Cancer Res. 2014, 16, 431. [Google Scholar] [CrossRef] [PubMed]
- Junttila, M.R.; Puustinen, P.; Niemela, M.; Ahola, R.; Arnold, H.; Bottzauw, T.; Ala-aho, R.; Nielsen, C.; Ivaska, J.; Taya, Y.; et al. CIP2A inhibits PP2A in human malignancies. Cell 2007, 130, 51–62. [Google Scholar] [CrossRef] [PubMed]
- Khanna, A.; Pimanda, J.E.; Westermarck, J. Cancerous inhibitor of protein phosphatase 2A, an emerging human oncoprotein and a potential cancer therapy target. Cancer Res. 2013, 73, 6548–6553. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.M.; Chu, P.Y.; Tung, S.L.; Liu, C.Y.; Tsai, Y.F.; Lin, Y.S.; Wang, W.L.; Wang, Y.L.; Lien, P.J.; Chao, T.C.; et al. Overexpression of phosphoprotein phosphatase 2a predicts worse prognosis in patients with breast cancer: A 15-year follow-up. Hum. Pathol. 2017, 66, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Westermarck, J.; Hahn, W.C. Multiple pathways regulated by the tumor suppressor PP2A in transformation. Trends Mol. Med. 2008, 14, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Canela, N.; Rodriguez-Vilarrupla, A.; Estanyol, J.M.; Diaz, C.; Pujol, M.J.; Agell, N.; Bachs, O. The set protein regulates G2/M transition by modulating cyclin B-cyclin-dependent kinase 1 activity. J. Biol. Chem. 2003, 278, 1158–1164. [Google Scholar] [CrossRef] [PubMed]
- Katayose, Y.; Li, M.; Al-Murrani, S.W.; Shenolikar, S.; Damuni, Z. Protein phosphatase 2A inhibitors, I1 (PP2A) and I2 (PP2A), associate with and modify the substrate specificity of protein phosphatase 1. J. Biol. Chem. 2000, 275, 9209–9214. [Google Scholar] [CrossRef] [PubMed]
- Saito, S.; Miyaji-Yamaguchi, M.; Shimoyama, T.; Nagata, K. Functional domains of template-activating factor-I as a protein phosphatase 2A inhibitor. Biochem. Biophys. Res. Commun. 1999, 259, 471–475. [Google Scholar] [CrossRef] [PubMed]
- Rincon, R.; Cristobal, I.; Zazo, S.; Arpi, O.; Menendez, S.; Manso, R.; Lluch, A.; Eroles, P.; Rovira, A.; Albanell, J.; et al. PP2A inhibition determines poor outcome and doxorubicin resistance in early breast cancer and its activation shows promising therapeutic effects. Oncotarget 2015, 6, 4299–4314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, S.W.; Xu, S.; Chen, H.; Liu, X.; Tang, Z.; Cui, Y.; Liu, J. Pathologic significance of SET/I2PP2A-mediated PP2A and non-PP2A pathways in polycystic ovary syndrome (PCOS). Clin. Chim. Acta 2017, 464, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Gu, Y.; Wang, H.; Yin, J.; Zheng, G.; Zhang, Z.; Lu, M.; Wang, C.; He, Z. Overexpression of PP2A inhibitor set oncoprotein is associated with tumor progression and poor prognosis in human non-small cell lung cancer. Oncotarget 2015, 6, 14913–14925. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.Y.; Tseng, L.M.; Su, J.C.; Chang, K.C.; Chu, P.Y.; Tai, W.T.; Shiau, C.W.; Chen, K.F. Novel sorafenib analogues induce apoptosis through SHP-1 dependent STAT3 inactivation in human breast cancer cells. Breast Cancer Res. 2013, 15, R63. [Google Scholar] [CrossRef] [PubMed]
- Gyorffy, B.; Lanczky, A.; Eklund, A.C.; Denkert, C.; Budczies, J.; Li, Q.; Szallasi, Z. An online survival analysis tool to rapidly assess the effect of 22,277 genes on breast cancer prognosis using microarray data of 1809 patients. Breast Cancer Res. Treat 2010, 123, 725–731. [Google Scholar] [CrossRef] [PubMed]
- Hung, M.H.; Wang, C.Y.; Chen, Y.L.; Chu, P.Y.; Hsiao, Y.J.; Tai, W.T.; Chao, T.T.; Yu, H.C.; Shiau, C.W.; Chen, K.F. Set antagonist enhances the chemosensitivity of non-small cell lung cancer cells by reactivating protein phosphatase 2A. Oncotarget 2016, 7, 638–655. [Google Scholar] [CrossRef] [PubMed]
- Hall, J.M.; McDonnell, D.P. The estrogen receptor beta-isoform (erbeta) of the human estrogen receptor modulates eralpha transcriptional activity and is a key regulator of the cellular response to estrogens and antiestrogens. Endocrinology 1999, 140, 5566–5578. [Google Scholar] [CrossRef] [PubMed]
- Edge, S.B.; Compton, C.C. The american joint committee on cancer: The 7th edition of the AJCC cancer staging manual and the future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef] [PubMed]
- Neviani, P.; Santhanam, R.; Trotta, R.; Notari, M.; Blaser, B.W.; Liu, S.; Mao, H.; Chang, J.S.; Galietta, A.; Uttam, A.; et al. The tumor suppressor PP2A is functionally inactivated in blast crisis CML through the inhibitory activity of the BCR/ABL-regulated set protein. Cancer Cell 2005, 8, 355–368. [Google Scholar] [CrossRef] [PubMed]
- Leopoldino, A.M.; Squarize, C.H.; Garcia, C.B.; Almeida, L.O.; Pestana, C.R.; Sobral, L.M.; Uyemura, S.A.; Tajara, E.H.; Silvio Gutkind, J.; Curti, C. Set protein accumulates in HNSCC and contributes to cell survival: Antioxidant defense, akt phosphorylation and avos acidification. Oral Oncol. 2012, 48, 1106–1113. [Google Scholar] [CrossRef] [PubMed]
- Cristobal, I.; Rincon, R.; Manso, R.; Carames, C.; Zazo, S.; Madoz-Gurpide, J.; Rojo, F.; Garcia-Foncillas, J. Deregulation of the PP2A inhibitor set shows promising therapeutic implications and determines poor clinical outcome in patients with metastatic colorectal cancer. Clin. Cancer Res. 2015, 21, 347–356. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Sidell, N. Anti-estrogenic effects of conjugated linoleic acid through modulation of estrogen receptor phosphorylation. Breast Cancer Res. Treat 2005, 94, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Cai, J.; Chen, S.; Zheng, X.; Hu, S.; Dong, W.; Lu, J.; Xing, J.; Dong, Y. Paclitaxel resistance in MCF-7/PTX cells is reversed by paeonol through suppression of the set/phosphatidylinositol 3-kinase/Akt pathway. Mol. Med. Rep. 2015, 12, 1506–1514. [Google Scholar] [CrossRef] [PubMed]
- Samanta, A.K.; Chakraborty, S.N.; Wang, Y.; Kantarjian, H.; Sun, X.; Hood, J.; Perrotti, D.; Arlinghaus, R.B. Jak2 inhibition deactivates Lyn kinase through the SET-PP2A-SHP1 pathway, causing apoptosis in drug-resistant cells from chronic myelogenous leukemia patients. Oncogene 2009, 28, 1669–1681. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | n = 218 | % |
|---|---|---|
| Age, years (Median, IQR) 1 | 50.6 (43.0 to 58.0) | |
| Adjuvant Tamoxifen treatment, months (Median, IQR) | 57.6 (31.3 to 67.8) | |
| Tumor stage (T) 2 | ||
| Tis | 6 | 2.8 |
| T1 | 96 | 44.0 |
| T2 | 112 | 51.4 |
| T3 | 3 | 1.4 |
| T4 | 1 | 0.5 |
| Nodal status (N) | ||
| N0 | 158 | 72.5 |
| N1 | 42 | 19.3 |
| N2 | 12 | 5.5 |
| N3 | 6 | 2.8 |
| AJCC tumor-node-metastasis (TNM) Stage | ||
| DCIS | 6 | 2.8 |
| I | 78 | 35.8 |
| II | 115 | 52.8 |
| III | 19 | 8.7 |
| Lymphovascular invasion | ||
| Absent | 189 | 86.3 |
| Present | 29 | 13.7 |
| Histologic grade | ||
| 1 | 36 | 16.5 |
| 2 | 146 | 67.0 |
| 3 | 36 | 16.5 |
| SET (Median, IQR) (n = 203) 3 | 80 (0 to 160) | |
| CIP2A (Median, IQR) (n = 202) 3 | 134 (80 to 200) | |
| pPP2A (Median, IQR) (n = 202) 3 | 133 (70 to 185) | |
| pAkt (Median, IQR) (n = 212) 3 | 142 (100 to 180) |
| Univariate RFS Analysis | Multivariate RFS Analysis | |||
|---|---|---|---|---|
| Hazard Ratio (95%CI) | p | Hazard Ratio (95%CI) | p | |
| SET H-score (>130 vs. ≤130) | 4.40 (1.52–12.68) | 0.003 | 3.72 (1.26–10.94) | 0.017 |
| CIP2A H-score (>195 vs. ≤195) | 2.90 (1.08–7.77) | 0.026 | 2.08 (0.72–6.00) | 0.173 |
| Lymphovascular invasion (present vs. absent) | 2.51 (0.87–7.27) | 0.088 | 2.85 (0.97–8.38) | 0.057 |
| Grade (3 vs. 2–1) | 2.05 (0.72–5.82) | 0.177 | 2.17 (0.73–6.45) | 0.162 |
| Stage (III vs. II–I-DCIS) | 2.33 (0.66–8.16) | 0.184 | 2.15 (0.46–10.08) | 0.330 |
| Characteristics | Number of Patients (n = 203) | SET Expression | p-value | |
|---|---|---|---|---|
| Low (n = 132) | High (n = 71) | |||
| Age | ||||
| ≤60 | 161 | 107 (81.1) | 54 (76.1) | 0.401 |
| >60 | 42 | 25 (18.9) | 17 (23.9) | |
| Tumor stage | ||||
| Tis | 6 | 5 (3.8) | 1 (1.4) | 0.818 |
| T1 | 92 | 60 (45.5) | 32 (45.1) | |
| T2 | 101 | 64 (48.5) | 37 (52.1) | |
| T3 | 3 | 2 (1.5) | 1 (1.4) | |
| T4 | 1 | 1 (0.8) | 0 (0) | |
| Nodal status | ||||
| N0 | 150 | 96 (72.7) | 54 (76.1) | 0.068 |
| N1 | 37 | 21 (15,9) | 16 (22.5) | |
| N2 | 11 | 10 (7.6) | 1 (1.4) | |
| N3 | 5 | 5 (3.8) | 0 (0) | |
| TNM Stage | ||||
| DCIS + I | 81 | 56 (42.4) | 25 (35.2) | 0.317 |
| II+III | 122 | 76 (57.6) | 46 (64.8) | |
| Grade | ||||
| 1 + 2 | 172 | 117 (88.6) | 55 (77.5) | 0.035 |
| 3 | 31 | 15 (11.4) | 16 (22.5) | |
| Lymphovascular invasion | ||||
| Absent | 172 | 115 (89.1) | 57 (83.8) | 0.286 |
| Present | 25 | 14 (10.9) | 11 (16.2) | |
| NA 1 | 6 | |||
| Tumor necrosis | ||||
| Absent | 168 | 112 (85.5) | 56 (78.9) | 0.230 |
| Present | 34 | 19 (14.5) | 15 (21.1) | |
| NA | 1 | |||
| CIP2A | ||||
| Low (<195) | 142 | 104 (80.6) | 39 (54.9) | <0.001 |
| High (>195) | 57 | 25 (19.4) | 32 (45.1) | |
| NA | 3 | |||
| pPP2A | ||||
| Low (<205) | 164 | 112 (86.2) | 52 (73.2) | 0.024 |
| High (>205) | 37 | 18 (13.8) | 19 (26.8) | |
| NA | 2 | |||
| pAkt | ||||
| Low (<195) | 45 | 29 (22.7) | 16 (22.9) | 0.974 |
| High (>195) | 153 | 99 (77.3) | 54 (77.1) | |
| NA | 5 | |||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Y.-H.; Chu, P.-Y.; Chen, J.-L.; Huang, C.-T.; Lee, C.-H.; Lau, K.-Y.; Wang, W.-L.; Wang, Y.-L.; Lien, P.-J.; Tseng, L.-M.; et al. SET Overexpression is Associated with Worse Recurrence-Free Survival in Patients with Primary Breast Cancer Receiving Adjuvant Tamoxifen Treatment. J. Clin. Med. 2018, 7, 245. https://doi.org/10.3390/jcm7090245
Huang Y-H, Chu P-Y, Chen J-L, Huang C-T, Lee C-H, Lau K-Y, Wang W-L, Wang Y-L, Lien P-J, Tseng L-M, et al. SET Overexpression is Associated with Worse Recurrence-Free Survival in Patients with Primary Breast Cancer Receiving Adjuvant Tamoxifen Treatment. Journal of Clinical Medicine. 2018; 7(9):245. https://doi.org/10.3390/jcm7090245
Chicago/Turabian StyleHuang, Yu-Hsiang, Pei-Yi Chu, Ji-Lin Chen, Chun-Teng Huang, Chia-Han Lee, Ka-Yi Lau, Wan-Lun Wang, Yu-Ling Wang, Pei-Ju Lien, Ling-Ming Tseng, and et al. 2018. "SET Overexpression is Associated with Worse Recurrence-Free Survival in Patients with Primary Breast Cancer Receiving Adjuvant Tamoxifen Treatment" Journal of Clinical Medicine 7, no. 9: 245. https://doi.org/10.3390/jcm7090245