Impact of Exergaming on Children’s Motor Skill Competence and Health-Related Fitness: A Quasi-Experimental Study


1
Department of Sports Rehabilitation, College of Physical Education, Longyan University, Longyan 364012, China
2
Chronic Disease Research Institute, School of Public Health, School of Medicine, Zhejiang University, Hangzhou 310058, China
3
Department of Applied Human Sciences, University of Minnesota, Duluth, MN 55812, USA
4
Department of Physical Education, University of South Carolina, Columbia, SC 29208, USA
5
School of Kinesiology, University of Minnesota, Minneapolis, MN 55455, USA
*
Authors to whom correspondence should be addressed.
J. Clin. Med. 2018, 7(9), 261; https://doi.org/10.3390/jcm7090261
Submission received: 23 July 2018
/
Revised: 16 August 2018
/
Accepted: 4 September 2018
/
Published: 7 September 2018
(This article belongs to the Special Issue Emerging Technology Applications to Promote Physical Activity and Health)
Abstract
:This study was designed to examine the effectiveness of a combined exergaming and physical education (PE) program on children’s motor skill competence (MSC) and health-related fitness (HRF) as compared to traditional PE. A total of 261 second- and third-grade children (127 boys; 8.25 ± 0.66 years for male; 8.29 ± 0.74 years for female; 73.6% non-Hispanic white) participated in the nine-month study from 2012 to 2013. Children were assigned to one of the two groups: (a) intervention group (125 min of alternating PE and exergaming weekly); and (b) comparison group (125-min weekly PE). MSC was assessed via product scores in two locomotor and two object control skills. HRF included the cardiorespiratory fitness, musculoskeletal fitness, and body mass index (BMI). A multivariate analysis of variance (MANOVA) was performed to analyze the effect of the combined exergaming–PE program on children’s MSC and HRF. There were significant group by time interaction effects for BMI, p < 0.01, η2 = 0.20; musculoskeletal fitness, p < 0.01, η2 = 0.13; and object control skills (the comparison group demonstrating greater improvement), p = 0.01, η2 = 0.03. The findings suggest that the combined exergaming program can have a positive effect on children’s BMI and musculoskeletal fitness, indicating that exergaming can be an alternative school-based program to supplement traditional PE.
1. Introduction
Secular declines in children’s health-related fitness (HRF) is a growing concern globally [1,2,3] and places children at risk for many health issues, including cardiovascular diseases or metabolic syndrome [4], obesity [5], and lower health-related quality of life [6,7,8]. Similarly, inadequate levels of motor skill competence (MSC) are a concern among health professionals and physical educators [9,10] as the development of MSC is positively linked to children’s HRF [11,12] and physical activity (PA) [12,13]. Specifically, competence in fundamental locomotor (e.g., jumping and hopping) and object control (e.g., throwing and kicking) skills is a prerequisite to the development of transitional movement skills [10]. MSC can be enhanced at an early age through targeted intervention, which also is beneficial for overall HRF [14].
Although a body of literature has shown traditional school-based PA programs or physical education (PE) courses can be effective in improving children’s HRF [15] and MSC [16,17] in the short term, interventions with long-term sustainability are still needed [15]. To sustain development in children’s MSC and HRF, it is critical to design an integrated and fun PA intervention that appeals to children [18]. Exergaming (a.k.a., active video games), a type of video games that requires bodily movement to play the video game, has been shown to increase children’s light-to-moderate PA by capitalizing on their interests in games and maintaining PA enjoyment [9,19,20,21]. Exergaming is one of the innovative and fun ways to motivate children to be active and develop their motor skills [20,21,22]. For example, exergaming allows children of all skill levels to engage in sport games that they would not be able to unless they have the appropriate skill levels in traditional PE classes. This is also possible because in exergaming, children can still play without needing appropriate equipment for specific sports. A few studies have indicated that integrating exergaming into PE classes contributes to higher levels of children’s PA and energy expenditure in both the short- and long-term, possibly due to its fun components [23,24,25,26]. While exergaming is an effective means to promote children’s PA, evidence on school-based exergaming interventions to promote MSC is lacking [23,27].
Recent studies demonstrated that exergaming has an inconsistent impact on children’s MSC in the short term [28,29]. Zeng and Gao, in 2016, concluded in a systematic review that studies that prove exergaming can offer sufficient stimulus for MSC changes were still limited [30]. Moreover, most of these studies examined balance skills or postural stability, with very few addressing the two important categories of MSC in young children [30,31,32]. Furthermore, no studies have explored the combined effects of exergaming and PE on young children’s MSC and HRF across a nine-month school-based intervention. Therefore, this quasi-experimental study was designed to examine the effectiveness of school-based exergaming integration with traditional PE on children’s MSC and HRF compared to traditional PE.
2. Materials and Methods
2.1. Participants and Research Setting
A total of 261 second- and third-grade children (8.27 ± 0.70 years; 134 girls; 73.6% non-Hispanic white) from two public elementary schools in southern USA participated in this study across the school year. Due to administrative and logistical reasons, randomization of individual children into either the intervention group or the comparison group was not feasible. Hence, one school served as the intervention school with the other serving as the comparison group. Both public schools were Title I schools (i.e., more than 50% children receive free or reduced-price school meals) in the same school district and were similar in their demographics. The majority of children were from low-income families. Other detailed information about the participants and research setting can be found in a recently published paper [23]. The inclusion criteria for this study were children who were (1) enrolled in a public Title I elementary school; (2) aged 7–9 years; (3) without a diagnosed physical or mental disability according to school records; and (4) able to provide parental consent and child assent. The eligibility of inclusion was verified through demographic information and student records in the schools.
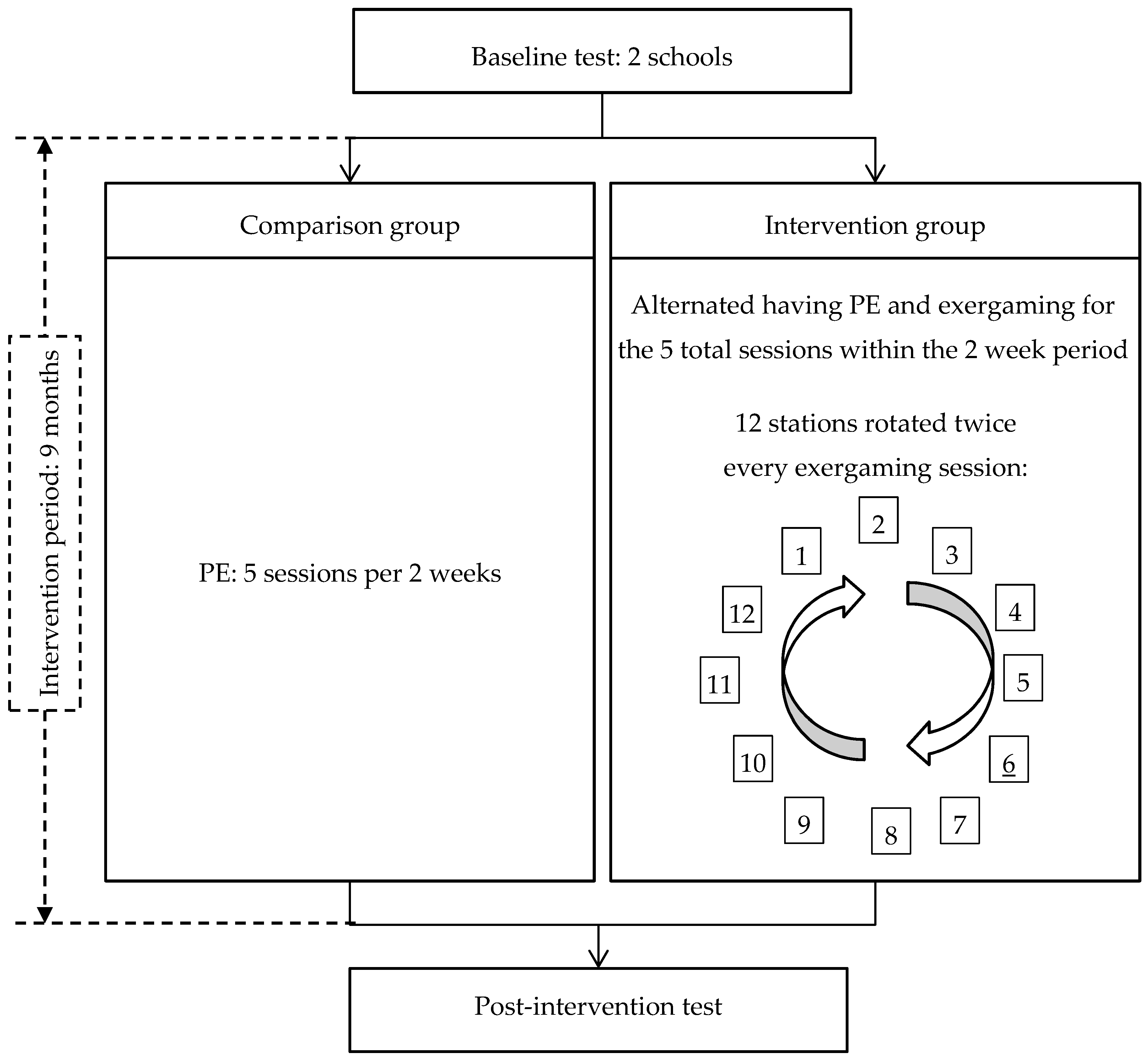
In the intervention school, the exergaming program was integrated into the school’s PE curriculum in such a way that exergaming and PE days alternated each week for a combined total of 125 min of biweekly PA; that is, out of 5 days of 25 min classes every two weeks, children’s schedules alternated having 3 PE classes in one week and 2 exergaming sessions the following week (Figure 1). A certified PE teacher taught PE and a full-time teacher, trained by the research team, coordinated and supervised children in the exergaming room (i.e., a modified classroom) at the school. In the comparison school, children had 125 min (25 min per class) of PE every two weeks taught by 2 certified teachers. Participants were recruited from 16 classes (average of ≈20 students per class) at the schools, with 8 classes from each school site. The study was approved by the University Institutional Review Board and parental consent and child assent were obtained.
2.2. Procedures
In the intervention school, 12 stations (costing approximately 600 US dollars per station), each equipped with 2 exergaming systems including Wii (Nintendo Co., Ltd., Kyoto, Japan) and Xbox Kinect (Microsoft Corp., Redmond, WA, USA) and a television, were installed in a classroom. Examples of the types of exergaming included were Kinect Ultimate Sports, Just Dance, Wii Sports, and Wii Fit. The variety of games allowed for autonomy in selection and promoted persistent motivation throughout the whole intervention period. A trained teacher supervised their participation of exergaming. Depending on the type of game, either all children participated in an exergaming session simultaneously (i.e., two children/station) or all children participated in one activity (e.g., Just Dance). Children rotated games twice during each session. During PE classes at both schools, a conventional multiactivity curriculum was promoted that mainly included sport- or game-based units and fitness activities [33].
2.3. Measures
Participants demographic information including age and gender was collected using an information sheet filled in by students, with assistance from research staff before intervention.
MSC assessments included performance on four skills (kicking, throwing, standing long jump, and hopping) based on our and other experts’ studies [34,35,36,37,38]. We used performance scores of skills to measure children’s MSC because the measures are sensitive in discriminating children’s competence levels across childhood and align with validated process-oriented assessments of motor skills [34,35,36,37]. The maximum speed for kicking (20-cm diameter playground balls) and throwing (using tennis balls) and maximum standing long jump distance were assessed from a total of five trials and used for analysis [38]. Throwing and kicking speed was measured using a radar gun (Stalker Radar, Plano, TX) [38]. For hopping, the average height of a minimum of three hops for each leg was used for analysis [35]. Both standing long jump and hopping performance were calculated based on children’s standing height [34,35]. The reliability of these tests (alpha coefficient method) were r = 0.70 (p < 0.01) according to a previous study [10].
Cardiorespiratory fitness and musculoskeletal fitness components of children’s HRF was measured using the FITNESSGRAM®. Trained research staff implemented FITNESSGRAM® protocols for the Progressive Aerobic Cardiovascular Endurance Run (PACER), curl-ups, and push-ups [38]. Grip strength was also assessed using a children’s grip dynamometer (Lafayette Instrument, Lafayette IN) as an additional indicator of musculoskeletal fitness [39]. The best score of three trials for each hand was averaged and used for data analysis [23]. To assess body composition component of HRF, children’s body mass index (BMI) was calculated as the weight in kilograms divided by the height in meters squared. Children’s body height and weight were measured using a stadiometer (Seca GmbH, Hamburg, Germany) and digital weight scale (Detecto, Web City, MO, USA), respectively. The validity and reliability of all of these measures have been noted in previous studies [34,35,38,39,40]. Baseline MSC and HRF tests were measured in September of 2012 and post-tests were conducted in May of 2013.
2.4. Data Analysis
The demographic characteristics of participants were described through a descriptive analysis. Missing data of one or some indices of MSC and HRF were imputed by the expectation maximization (EM) method, although participants with missing data for all indices were excluded. All indices of MSC and HRF scores were normalized and then converted to standard T-scores (T-score = 50 + 10 * Z-score). Performance scores for the MSC tests were grouped according to locomotor and object control separately. The locomotor skill score was the mean T-scores for both standing long jump and hopping, while object control skill score was defined as the mean score of kicking and throwing T-scores. In regard to HRF, the musculoskeletal fitness score was calculated as the mean of the T-scores of grip strength, push-ups, and curl-ups.
T-tests and paired T-tests were conducted to observe any differences in all variables of interest between the comparison and intervention groups and between the pre- and post-intervention tests, respectively. Since there were significant between-group differences in baseline scores of PACER (higher in comparison group) and BMI (higher in intervention group), as well as curl-up (higher in comparison group), the difference in scores between pre- and post-tests for each variable were set as the outcome variable. In order to explore the effects of intervention on children’s MSC and HRF over time, a multivariate analysis of variance (MANOVA) was conducted. All descriptive and inferential statistical analyses were conducted using SPSS 20.0 (IBM Corp., Armonk, NY, USA) and the significance level was set at 0.05 for all statistical analyses.
3. Results
Eleven children were removed from the study from pre-test to post-test due to missing data for all indices of MSC and HRF (n = 10) or being an outlier (n = 1). Baseline demographic characteristics of participants are shown in Table 1. Children’s mean age was 8.27 years, and 75% of the sample was non-Hispanic white. The intervention effects on children’s MSC and HRF are described in Table 2. Significant group by time interaction effects were revealed for HRF and MSC variables including: musculoskeletal fitness, F (1, 250) = 38.33, p < 0.01, η2 = 0.13; BMI, F (1, 250) = 61.39, p < 0.01, η2 = 0.20; and object control skills, F (1, 250) = 6.77, p = 0.01, η2 = 0.03. While children in the comparison group displayed significantly higher cardiorespiratory fitness scores (PACER) than children in the intervention group at both baseline and post-tests (p < 0.01), the comparison and intervention groups both demonstrated increase over time in their cardiorespiratory fitness (p < 0.01). Likewise, the decline in intervention children’s BMI demonstrated a significant difference from the increased BMI in the comparison group. In addition, the between-group difference in the change scores of children’s musculoskeletal fitness was significant, favoring the intervention group.
In terms of children’s MSC, significant improvement effects over time were revealed in children’s object control skills in both the intervention and comparison groups (p < 0.01), with the comparison group demonstrating greater improvement, F (1, 250) = 6.77, p = 0.01, η2 = 0.03, compared to the intervention group. Slight improvement in the locomotor skills of children was observed in the intervention and comparison groups over time; however, these changes in score were not significant.
4. Discussion
As an innovative technology and potential tool for capturing and maintaining children’s interest and motivation to be physically active and fit [41], exergaming has been integrated into a traditional PE curriculum within the school day [24,25]. However, the impact of exergaming on children’s motor skills is not well understood. Our findings indicate that an integrated school-based exergaming/PE program demonstrated greater overall positive benefits on children’s muscle strength and BMI, compared to traditional PE only. This impact on fitness may be due to: (1) more light and moderate PA in exergaming compared to fitness activities offered in PE classes, which could lead to body weight improvement in children [42], and (2) specificity of fitness exergames (i.e., Wii Fit and Just Dance) offered in the intervention group, which can improve children’s some musculoskeletal fitness. Playing games from the Wii system may have improved children’s grip strength through use of the controllers [43]. Previous evidence has illustrated controversy on the notion that exergaming provides sufficient PA intensity to improve children’s HRF [19]. Specifically, some literature did not support the capability of exergaming to improve children’s physical fitness or to provide health benefits [19,27,44,45], while other literature suggests exergaming can promote health benefits associated with maintenance of weight status and increased cardiorespiratory fitness [46,47]. The inconsistent findings might be owed to the setting in which exergames were played (e.g., laboratory, home, or school), types of the games, duration/dose, and intervention fidelity [48,49,50]. Previous studies have shown that the following factors are important in enhancing children’s motivation, ultimately leading to appropriate improvement in their HRF: (a) presence of the supervision of specialist teachers; (b) appropriate organization behavior management; and (c) including a variety of PA programs [16,51,52]. Thus, we speculate that adequate supervision and consistent incorporation of different types of exergames offered to children led to greater increases in musculoskeletal fitness, as most of the previous relevant studies have intervened through only one type of exergame [20,49,53,54].
Our findings in children’s MSC only partially supported the other portion of our hypothesis. When examining locomotor skills data, there was no significant difference in changes of score between the comparison and the intervention group, suggesting little impact of exergames on children’s hopping and standing long jump. While the comparison group demonstrated significantly greater improvement in object control skills as compared to the intervention group across the school year, the effect size was small (η2 = 0.03). The significant increase in object control skills in the traditional PE groups may be indicative of having more overall time spent in performing object control skills in a more ecologically valid setting (e.g., more time spent in PE). Specifically, no Wii or Xbox games provide opportunities for actual kicking and throwing activities. Games noted within exergaming games (e.g., Wii Sports and Kinect Ultimate Sports) do not necessarily demand that individuals demonstrate their highest level of throwing (e.g., primarily using elbow extension and wrist flexion in the Wii baseball game). Thus, the virtual games promoted in exergaming may not demand the same type of movement execution and effort to promote skill development to the same degree as traditional practice experiences.
In the present study, kicking skills of children in the intervention group increased over time; however, their standing long jump decreased at the end of the program. It appears that development of the standing long jump (locomotor skills) through semi-structured exergaming is more challenging than acquiring kicking skills (object control skills). Indeed, in two recent studies [31,55], similar findings were shown. The researchers tested the efficacy of six 50-min sessions of active video games (AVGs) on 6–10-year-olds’ actual and perceived objective motor skills. Not only did they not find any significant differences between the control and intervention groups on both outcomes, they also did not find any improvement in the skills between typically developing children and children with autism spectrum disorder. The authors suggested that the play nature of AVGs may not provide adequate practice of the correct movements that are required to perform the skills [31,55]. Similarly, Pedersen et al., in their study in which they examined the effects of 30-min Nintendo Wii tennis games in improving reaction time for contralateral arm movement in children aged 7–12 years, revealed that these short bouts of exergaming sessions did not enhance children’s motor processing speed (reaction time) [56]. Reaction time may not be directly related to the performance of object control skills measured in the current study; however, it is a good indicator of how children’s object control skills would be applied in more advanced sport skill settings.
On the contrary, other studies have shown that the use of exergaming could be a feasible and pleasant approach to improve elementary school or nontypically-developing children’s gross motor skills [32,57]. In one of these studies, an eight-week long exergaming intervention was found effective in improving children’s object control skills. In this case, however, the effectiveness of the intervention in enhancing the skills was due to the selection and implementation of exergames (i.e., Baseball mini games; NBA Baller Beats, Bowling, and Soccer mini games; Xbox Kinect) that were specifically geared toward developing the same six objective control skills, namely throwing, kicking, catching, dribbling, rolling, and striking. Based on these findings of previous literature, we speculate that the lack of games that would provide opportunities for children to practice throwing and kicking skills could have been one of the reasons why we did not observe improvement in object control skills in the current study.
Another important point to note may be the quality of play, to which Howie and her colleagues attributed the ineffectiveness of an exergaming (Xbox 360 with Kinect) intervention on children’s motor coordination (MABC-2) [58]. In this home-based exergaming intervention study for the clinical pediatric population, the authors mention motivation–outcome trade-off, which describes how self-selected games may increase children’s motivation to play longer, but not necessarily the quality of play that leads to motor skill improvement. The study suggests the importance of finding a challenging point for each individual and adhering to the game to experience motor skill improvement, instead of switching games that they favor. We speculate that this may be very much aligned to our findings in current study. Children in this present study could have played longer and at higher intensities to increase their HRF; however, not at high enough quality to contribute to improvement in object control skills.
In our previous study, in which we examined the effect of an exergaming program in increasing children’s PA, we did not see any significant increase in their PA levels [23]. However, significant exergaming effects on children’s HRF were observed in our current study. It is plausible that these inconsistent results between the two studies are due to several possible reasons. First, measurement of children’s PA was limited to school time, not whole days (24 h), which could not reflect actual total levels of daily PA. Second, increase in children’s HRF may not be due to total PA levels, but more due to other factors such as dietary intake, basic metabolic rate, and intensity of exercise. Third, it is possible that exergaming had a beneficial effect in current study because it was combined with PE. In this case, PE can provide opportunities that exergaming cannot offer and lead to greater effects of intervention than the effects that would be brought by PE or exergaming alone. However, further studies are warranted to explore the potential interactions.
This study was conducted in a real-world setting, examining the effects of a combination of exergaming and traditional PE, and including both HRF and MSC as outcome variables, which are the strengths of this study. However, the study is not without limitations. First, our study did not implement random recruitment or random assignment, which limits the generalizability. Second, it is also difficult to define the independent effect of exergaming on the outcomes as our intervention had both PE and exergaming sessions. Third, flexibility, which is one of the five HRF components, was not included in our HRF outcomes, and this study could improve by implementing a follow-up measurement to avoid potential seasonal effects on children’s HRF/MSC and to explore the durability of children’s interest in exergaming. Moreover, children in our study could have been exposed to a “Hawthorne Effect”, as teachers and research assistants were observing them at the time of testing. Children could have modified their behavior (e.g., making much more effort in physical activity) in response to their awareness of being observed or intervened. In addition, there might have been some motivational issues in children in the comparison group at the curl-ups testing, as the post-test score plummeted from the baseline. Examining our data, a good number of children who scored high in the baseline did not do as well in their post-test, which might have influenced the overall musculoskeletal fitness score in the comparison group. Lastly, the information about energy expenditure was not collected during the exergaming and PE sessions.
5. Conclusions
A well-implemented class combining exergaming and traditional PE can be beneficial in developing children’s musculoskeletal fitness and BMI compared to the sole traditional PE class. Considering the potential benefits of exergaming in stimulating children’s interest in PA and developing HRF [59], integration of an exergaming component into PE is partly recommended. However, when exergaming is implemented, several things should be taken into consideration. The structure of the exergaming may depend on the goal of the program, whether it be promotion of PA, enhancement of HRF, or/and improvement in MSC. If practitioners are in pursuit of children’s MSC, the traditional PE classes may be a better choice than exergaming. Future studies with randomization and long-term design are needed to confirm our results.
Author Contributions
S.Y. and J.E.L. drafted the manuscript. Z.G. and D.F.S. designed and conducted the research and helped revise the manuscript. S.Y. analyzed data and had primary responsibility for the final content. All authors read and approved the final manuscript.
Funding
This study was funded by a grant from the National Institute of Child and Human Development (1R15HD071514-01A1) and China Postdoctoral Science Foundation (2017M621903).
Acknowledgments
The authors would like to thank the research assistants who helped with data collection and students and teachers who cooperated with data collection.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Roriz de Oliveira, M.S.; Seabra, A.; Garganta, R.; Ribeiro Maia, J.A. Decennial trend in passing rates of health-related physical fitness in children from Maia county, northern Portugal. Ann. Hum. Biol. 2012, 39, 453. [Google Scholar]
- Albon, H.M.; Hamlin, M.J.; Ross, J.J. Secular trends and distributional changes in health and fitness performance variables of 10–14-year-old children in New Zealand between 1991 and 2003. Br. J. Sport Med. 2010, 44, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; Yang, Y.; Kong, Z.X.; Zhang, Y.M.; Zhuang, J. Prevalence of physical fitness in Chinese school-aged children: Findings from the 2016 physical activity and fitness in China-the Youth Study. J. Sport Health Sci. 2017, 6, 395–403. [Google Scholar] [CrossRef]
- Smith, J.J.; Eather, N.; Morgan, P.J.; Plotnikoff, R.C.; Faigenbaum, A.D.; Lubans, D.R. The health benefits of muscular fitness for children and adolescents: A systematic review and meta-analysis. Sports Med. 2014, 44, 1209–1223. [Google Scholar] [CrossRef] [PubMed]
- Casonatto, J.; Fernandes, R.A.; Batista, M.B.; Cyrino, E.S.; Coelho-e-Silva, M.J.; de Arruda, M.; Ronque, E.R.V. Association between health-related physical fitness and body mass index status in children. J. Child Health Care 2016, 20, 294–303. [Google Scholar] [CrossRef] [PubMed]
- Gu, X.L.; Chang, M.; Solmon, M.A. Physical activity, physical fitness, and health-related quality of life in school-aged children. J. Teach. Phys. Educ. 2016, 35, 117–126. [Google Scholar] [CrossRef]
- Venckunas, T.; Emeljanovas, A.; Mieziene, B.; Volbekiene, V. Secular trends in physical fitness and body size in Lithuanian children and adolescents between 1992 and 2012. J. Epidemiol. Commun. Health 2017, 71, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, F.K.; Prista, A.; Gomes, T.N.Q.F.; Daca, T.; Madeira, A.; Katzmarzyk, P.T.; Maia, J.A.R. Secular trends in physical fitness of Mozambican school-aged children and adolescents. Am. J. Hum. Biol. 2015, 27, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Soltani, P.; Vilas-Boas, J.P. Sport Exergames for physical education. In Encyclopedia of Information Science and Technology, 4th ed.; IGI Global: Calgary, AB, Canada, 2018; pp. 7358–7367. [Google Scholar]
- Barnett, L.M.; Van Beurden, E.; Morgan, P.J.; Brooks, L.O.; Beard, J.R. Does childhood motor skill proficiency predict adolescent fitness? Med. Sci. Sport Exerc. 2008, 40, 2137–2144. [Google Scholar] [CrossRef] [PubMed]
- Re, A.H.N.; Cattuzzo, M.T.; Santos, F.M.C.; Monteiro, C.B.M. Anthropometric characteristics, field test scores and match-related technical performance in youth indoor soccer players with different playing status. Int. J. Perform. Anal. Sport 2014, 14, 482–492. [Google Scholar]
- Lima, R.A.; Pfeiffer, K.; Larsen, L.R.; Bugge, A.; Moller, N.C.; Anderson, L.B.; Stodden, D.F. Physical activity and motor competence present a positive reciprocal longitudinal relationship across childhood and early adolescence. J. Phys. Act. Health 2017, 14, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Haga, M.; Gisladottir, T.; Sigmundsson, H. The relationship between motor competence and physical fitness is weaker in the 15-16 yr. adolescent age group than in younger age groups (4–5 yr. and 11–12 yr.). Percept. Mot. Skill 2015, 121, 900–912. [Google Scholar] [CrossRef] [PubMed]
- Wick, K.; Leeger-Aschmann, C.S.; Monn, N.D.; Radtke, T.; Ott, L.V.; Rebholz, C.E.; Cruz, S.; Gerber, N.; Schmutz, E.A.; Puder, J.J.; et al. Interventions to promote fundamental movement skills in childcare and kindergarten: A systematic review and meta-analysis. Sports Med. 2017, 47, 2045–2068. [Google Scholar] [CrossRef] [PubMed]
- Lai, S.K.; Costigan, S.A.; Morgan, P.J.; Lubans, D.R.; Stodden, D.F.; Salmon, J.; Barnett, L.M. Do school-based interventions focusing on physical activity, fitness, or fundamental movement skill competency produce a sustained impact in these outcomes in children and adolescents? A systematic review of follow-up studies. Sports Med. 2014, 44, 67–79. [Google Scholar] [CrossRef] [PubMed]
- Tompsett, C.; Sanders, R.; Taylor, C.; Cobley, S. Pedagogical approaches to and effects of fundamental movement skill interventions on health outcomes: A systematic review. Sports Med. 2017, 47, 1795–1819. [Google Scholar] [CrossRef] [PubMed]
- Morgan, P.J.; Barnett, L.M.; Cliff, D.P.; Okely, A.D.; Scott, H.A.; Cohen, K.E.; Lubans, D.R. Fundamental movement skill interventions in youth: A systematic review and meta-analysis. Pediatrics 2013, 132, E1361–E1383. [Google Scholar] [CrossRef] [PubMed]
- Butt, J.; Weinberg, R.S.; Breckon, J.D.; Claytor, R.P. Adolescent physical activity participation and motivational determinants across gender, age, and race. J. Phys. Act. Health 2011, 8, 1074–1083. [Google Scholar] [CrossRef] [PubMed]
- Kari, T. Promoting physical activity and fitness with exergames: Updated systematic review of systematic reviews. In Transforming Gaming and Computer Simulation Technologies across Industries; IGI Global: Calgary, AB, Canada, 2017; pp. 225–245. [Google Scholar]
- Chen, H.; Sun, H.C. Effects of active videogame and sports, play, and active recreation for kids physical education on children’s health-related fitness and enjoyment. Games Health J. 2017, 6, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Pasco, D.; Roure, C.; Kermarrec, G.; Pope, Z.; Gao, Z. The effects of a bike active video game on players’ physical activity and motivation. J. Sport Health Sci. 2017, 6, 25–32. [Google Scholar] [CrossRef]
- Barnett, L.M.; Bangay, S.; McKenzie, S.; Ridgers, N.D. Active gaming as a mechanism to promote physical activity and fundamental movement skill in children. Front. Public Health 2013, 1, 74. [Google Scholar] [CrossRef] [PubMed]
- Gao, Z.; Pope, Z.; Lee, J.E.; Stodden, D.; Roncesvalles, N.; Pasco, D.; Huang, C.C.; Feng, D. Impact of exergaming on young children’s school day energy expenditure and moderate-to-vigorous physical activity levels. J. Sport Health Sci. 2017, 6, 11–16. [Google Scholar] [CrossRef]
- Chukhlantseva, N. Integration of active videogames in physical training of school students. Sci. Educ. 2017, 4, 14–20. [Google Scholar] [CrossRef]
- Arajuo, J.G.E.; Batista, C.; Moura, D.L. Exergames in physical education: A systematic review. Movimento 2017, 23, 529–542. [Google Scholar]
- Staiano, A.E.; Beyl, R.A.; Hsia, D.S.; Katzmarzyk, P.T.; Newton, R.L. Twelve weeks of dance exergaming in overweight and obese adolescent girls: Transfer effects on physical activity, screen time, and self-efficacy. J. Sport Health Sci. 2017, 6, 4–10. [Google Scholar] [CrossRef] [PubMed]
- Norris, E.; Hamer, M.; Stamatakis, E. Active video games in schools and effects on physical activity and health: A systematic review. J. Pediatr. 2016, 172, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Barnett, L.M.; Ridgers, N.D.; Reynolds, J.; Hanna, L.; Salmon, J. Playing active video games may not develop movement skills: An intervention trial. Preve. Med. Rep. 2015, 2, 673–678. [Google Scholar] [CrossRef] [PubMed]
- Hulteen, R.M.; Johnson, T.M.; Ridgers, N.D.; Mellecker, R.R.; Barnett, L.M. Children’s movement skills when playing active video games. Percept. Mot. Skill 2015, 121, 767–790. [Google Scholar] [CrossRef] [PubMed]
- Zeng, N.; Gao, Z. Effects of exergaming on fundamental movement skills among children and young adults: A systematic review. In Gaming: Trends, Perspectives and Impact on Health; Nova Science Publishers: Hauppauge, NY, USA, 2016; pp. 41–58. [Google Scholar]
- Edwards, J.; Jeffrey, S.; May, T.; Rinehart, N.J.; Barnett, L.M. Does playing a sports active video game improve object control skills of children with autism spectrum disorder? J. Sport Health Sci. 2017, 6, 17–24. [Google Scholar] [CrossRef]
- Vernadakis, N.; Papastergiou, M.; Zetou, E.; Antoniou, P. The impact of an exergame-based intervention on children’s fundamental motor skills. Comput. Educ. 2015, 83, 90–102. [Google Scholar] [CrossRef]
- Metzler, M. Instructional Models for Physical Education; Holocomb Hathaway: Scottsdale, AZ, USA, 2005. [Google Scholar]
- Lane, A.P.; Molina, S.L.; Tolleson, D.A.; Langendorfer, S.J.; Goodway, J.D.; Stodden, D.F. Developmental sequences for the standing long jump landing: A pre-longitudinal screening. J. Mot. Learn. Dev. 2018, 6, 114–129. [Google Scholar] [CrossRef]
- Nesbitt, D.R.; Molina, S.; Sacko, R.; Robinson, L.; Brian, A.; Stodden, D.F. Examining the feasibility of supine-to-stand as a measure of functional motor competence. J. Mot. Learn. Dev. 2018, in press. [Google Scholar] [CrossRef]
- Stodden, D.F.; Langendorfer, S.J.; Fleisig, G.S.; Andrews, J.R. Kinematic constraints associated with the acquisition of overarm throwing part I: Step and trunk actions. Res. Q. Exerc. Sport 2006, 77, 417–427. [Google Scholar] [CrossRef] [PubMed]
- Stodden, D.F.; Langendorfer, S.J.; Fleisig, G.S.; Andrews, J.R. Kinematic constraints associated with the acquisition of overarm throwing part II: Upper extremity actions. Res. Q. Exerc. Sport 2006, 77, 428–436. [Google Scholar] [CrossRef] [PubMed]
- Stodden, D.F.; Gao, Z.; Goodway, J.D.; Langendorfer, S.J. Dynamic relationships between motor skill competence and health-related fitness in youth. Pediatr. Exerc. Sci. 2014, 26, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Pate, R.R.; Blimkie, C.; Castelli, D.; Corbin, C.B.; Daniels, S.R.; Kohl, H.W.; Malina, R.M.; Sacheck, J.; Stodden, D.F.; Whitt-Glover, M.; et al. Fitness measures and health outcomes in youth. In Institute of Medicine; Pillsbury, L., Oria, M., Pate, R., Eds.; National Academies Press: Washington, DC, USA, 2012. [Google Scholar]
- Wind, A.E.; Takken, T.; Helders, P.J.M.; Engelbert, R.H.H. Is grip strength a predictor for total muscle strength in healthy children, adolescents, and young adults? Eur. J. Pediatr. 2010, 169, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Finco, M.D.; Reategui, E.; Zaro, M.A.; Sheehan, D.D.; Katz, L. Exergaming as an alternative for students unmotivated to participate in regular physical education classes. IJGBL 2015, 5, 1–10. [Google Scholar] [CrossRef]
- Sween, J.; Wallington, S.F.; Sheppard, V.; Taylor, T.; Llanos, A.A.; Adams-Campbell, L.L. The role of exergaming in improving physical activity: A review. J. Phys. Act. Health 2014, 11, 864–870. [Google Scholar] [CrossRef] [PubMed]
- Salem, Y.; Gropack, S.J.; Coffin, D.; Godwin, E.M. Effectiveness of a low-cost virtual reality system for children with developmental delay: A preliminary randomised single-blind controlled trial. Physiotherapy 2012, 98, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Gao, Z. Fight fire with fire? Promoting physical activity and health through active video games. J. Sport Health Sci. 2017, 6, 1–3. [Google Scholar] [CrossRef]
- Gao, Z.; Zhang, T.; Stodden, D. Children’s physical activity levels and psychological correlates in interactive dance versus aerobic dance. J. Sport Health Sci. 2013, 2, 146–151. [Google Scholar] [CrossRef]
- Maddison, R.; Mhurchu, C.N.; Jull, A.; Prapavessis, H.; Foley, L.S.; Jiang, Y.N. Active video games: The mediating effect of aerobic fitness on body composition. Int. J. Behav. Nutr. Phys. 2012, 9, 54. [Google Scholar] [CrossRef] [PubMed]
- Gao, Z.; Chen, S.; Pasco, D.; Pope, Z. A meta-analysis of active video games on health outcomes among children and adolescents. Obes. Rev. 2015, 16, 783–794. [Google Scholar] [CrossRef] [PubMed]
- Christison, A.L.; Evans, T.A.; Bleess, B.B.; Wang, H.P.; Aldag, J.C.; Binns, H.J. Exergaming for health: A randomized study of community-based exergaming curriculum in pediatric weight management. Games Health J. 2016, 5, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Naugle, K.E.; Naugle, K.M.; Wikstrom, E.A. Cardiovascular and affective outcomes of active gaming: Using the Nintendo Wii as a cardiovascular training tool. J. Strength Cond. Res. 2014, 28, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Foley, L.; Jiang, Y.N.; Mhurchu, C.N.; Jull, A.; Prapavessis, H.; Rodgers, A.; Maddison, R. The effect of active video games by ethnicity, sex and fitness: Subgroup analysis from a randomised controlled trial. Int. J. Behav. Nutr. Phys. 2014, 11, 46. [Google Scholar] [CrossRef] [PubMed]
- Hardy, L.L.; O’Hara, B.J.; Rogers, K.; St George, A.; Bauman, A. Contribution of organized and nonorganized activity to children’s motor skills and fitness. J. School Health 2014, 84, 690–696. [Google Scholar] [CrossRef] [PubMed]
- Laitakari, J.; Vuori, I.; Oja, P. Is long-term maintenance of health-related physical activity possible? An analysis of concepts and evidence. Health Educ. Res. 1996, 11, 463–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabel, M.; Sjolund, A.; Broeren, J.; Arvidsson, D.; Saury, J.M.; Gillenstrand, J.; Emanuelson, I.; Blomgren, K.; Lannering, B. Effects of physically active video gaming on cognition and activities of daily living in childhood brain tumor survivors: A randomized pilot study. Neuro-Oncol. Pract. 2017, 4, 98–110. [Google Scholar] [CrossRef]
- Gao, Z. Motivated but not active: The dilemmas of incorporating interactive dance into gym class. J. Phys. Act. Health 2012, 9, 794–800. [Google Scholar] [CrossRef] [PubMed]
- Johnson, T.M.; Ridgers, N.D.; Hulteen, R.M.; Mellecker, R.R.; Barnett, L.M. Does playing a sports active video game improve young children’s ball skill competence? J. Sci. Med. Sport 2016, 19, 432–436. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, S.J.; Cooley, P.D.; Cruickshank, V.J. Caution regarding exergames: A skill acquisition perspective. Phys. Educ. Sport Pedagog. 2017, 22, 246–256. [Google Scholar] [CrossRef]
- Page, Z.E.; Barrington, S.; Edwards, J.; Barnett, L.M. Do active video games benefit the motor skill development of non-typically developing children and adolescents: A systematic review. J. Sci. Med. Sport 2017, 20, 1087–1100. [Google Scholar] [CrossRef] [PubMed]
- Howie, E.K.; Campbell, A.C.; Abbott, R.A.; Straker, L.M. Understanding why an active video game intervention did not improve motor skill and physical activity in children with developmental coordination disorder: A quantity or quality issue? Res. Dev. Disabil. 2017, 60, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Baranowski, T. Exergaming: Hope for future physical activity? or blight on mankind? J. Sport Health Sci. 2017, 6, 44–46. [Google Scholar] [CrossRef]
Figure 1.
Study design and intervention flow.


{kind=link}
Table 1.
Demographic characteristics of participants in baseline and post-intervention.
| Variables * | Baseline | Post-Intervention | ||||
|---|---|---|---|---|---|---|
| Comparison (n = 115) | Intervention (n = 135) | p Value ‡ | Comparison (n = 115) | Intervention (n = 135) | p Value ‡ | |
| Age (years) | 8.41 (0.71) | 8.14 (0.67) | 0.002 | / | / | / |
| Girls (counts) † | 59 (51.3) | 70 (51.9) | 0.931 | / | / | / |
| White American (counts) † | 69 (60.0) | 118 (87.4) | <0.001 | / | / | / |
| Height (cm) | 131.77 (7.59) | 129.46 (6.83) | 0.012 | 132.73 (7.24) | 132.80 (7.19) | 0.942 |
| Weight (kg) | 30.77 (9.12) | 31.69 (8.69) | 0.417 | 33.73 (9.65) | 32.95 (9.72) | 0.524 |
| Motor skill competence | ||||||
| Kicking (m/s) | 10.95 (1.79) | 11.06 (2.46) | 0.691 | 12.06 (1.87) | 11.84 (1.92) | 0.360 |
| Throwing (m/s) | 14.10 (3.82) | 14.55 (3.35) | 0.317 | 14.74 (3.87) | 14.48 (3.69) | 0.586 |
| Standing long jump (%) | 0.93 (0.15) | 0.93 (0.17) | 0.979 | 0.93 (0.15) | 0.91 (0.17) | 0.390 |
| Hops (%) | 0.64 (0.12) | 0.62 (0.14) | 0.190 | 0.67 (0.12) | 0.70 (0.14) | 0.124 |
| Health-related fitness | ||||||
| PACER (laps) | 22.92 (11.15) | 14.04 (7.08) | <0.001 | 26.87 (13.24) | 20.67 (9.30) | <0.001 |
| Grip strength (kg) | 13.90 (2.96) | 14.50 (3.48) | 0.143 | 12.86 (3.66) | 16.22 (4.01) | <0.001 |
| Push-ups (counts) | 7.47 (6.26) | 6.24 (6.07) | 0.116 | 9.32 (6.47) | 8.65 (6.23) | 0.409 |
| Curl-ups (counts) | 34.60 (26.57) | 23.49 (21.86) | <0.001 | 18.58 (18.93) | 21.33 (19.65) | 0.262 |
| BMI (kg/cm2) | 17.60 (3.78) | 18.72 (3.67) | 0.019 | 18.88 (3.89) | 18.42 (3.87) | 0.346 |
Note: * All values are the mean, with standard deviation in brackets; † Frequencies (percentage); ‡ Student’s T-test for continuous variables and chi-squared test for categorical variables; Standing long jump (%): standing long jump (cm) divided by body height (cm); Hops (%): hops (cm) divided by body height (cm); PACER: progressive aerobic cardiovascular endurance run; BMI: body mass index.
Table 2.
Baseline and post-intervention motor skill competence and health-related fitness descriptive and inferential statistics.
Table 2.
Baseline and post-intervention motor skill competence and health-related fitness descriptive and inferential statistics.
| Tests | Conditions | Baseline T-Scored Mean (SD) | Post-Test T-Scored Mean (SD) | Diff. Mean (SD) | F | p | η2 |
|---|---|---|---|---|---|---|---|
| MSC | |||||||
| Locomotor | Intervention (n = 135) | 49.34 (7.23) | 50.11 (7.21) | 0.77 (4.64) | 1.03 | 0.311 | 0.00 |
| Comparison (n = 115) | 49.77 (6.68) | 49.98 (6.68) | 0.20 (4.16) | ||||
| Object control | Intervention (n = 135) | 49.02 (9.21) | 50.87 ‡ (9.01) | 1.85 (5.51) | 6.77 | 0.010 | 0.03 |
| Comparison (n = 115) | 48.20 (8.45) | 51.73 ‡ (8.66) | 3.54 (4.59) | ||||
| HRF | |||||||
| PACER | Intervention (n = 135) | 44.23 † (6.33) | 49.00 ‡ (8.56) | 4.77 (6.40) | 1.77 | 0.184 | 0.01 |
| Comparison (n = 115) | 52.21 (9.95) | 55.69 ‡ (11.84) | 3.48 (8.93) | ||||
| Musculoskeletal fitness | Intervention (n = 135) | 49.37 (6.74) | 51.25 ‡ (7.08) | 1.88 (5.19) | 38.33 | <0.001 | 0.13 |
| Comparison (n = 115) | 50.83 (7.64) | 48.30 ‡ (6.08) | −2.53 (6.08) | ||||
| Body mass index | Intervention (n = 135) | 50.81 * (9.76) | 50.01 † (10.31) | −0.80 (4.33) | 61.39 | <0.001 | 0.20 |
| Comparison (n = 115) | 47.83 (10.06) | 51.24 ‡ (10.35) | 3.41 (4.12) |
Note: Musculoskeletal fitness: represents the compiled score for grip strength, curl-ups, and push-ups tests; SD: standard deviation; MSC: motor skill competence; Locomotor: combining standing long jump and hops; Object control: combining kicking and throwing; HRF: health-related fitness; PACER: progressive aerobic cardiovascular endurance run; Musculoskeletal fitness: combining grip strength, push-ups, and curl-ups; Diff.: difference between the baseline and post-test. T test was conducted to observe the difference between comparison and intervention groups at the baseline. * p < 0.05 compared with comparison group; † p < 0.01 compared with comparison group; ‡ p < 0.01 compared with baseline.
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Ye, S.; Lee, J.E.; Stodden, D.F.; Gao, Z. Impact of Exergaming on Children’s Motor Skill Competence and Health-Related Fitness: A Quasi-Experimental Study. J. Clin. Med. 2018, 7, 261. https://doi.org/10.3390/jcm7090261
AMA Style
Ye S, Lee JE, Stodden DF, Gao Z. Impact of Exergaming on Children’s Motor Skill Competence and Health-Related Fitness: A Quasi-Experimental Study. Journal of Clinical Medicine. 2018; 7(9):261. https://doi.org/10.3390/jcm7090261
Chicago/Turabian StyleYe, Sunyue, Jung Eun Lee, David F. Stodden, and Zan Gao. 2018. "Impact of Exergaming on Children’s Motor Skill Competence and Health-Related Fitness: A Quasi-Experimental Study" Journal of Clinical Medicine 7, no. 9: 261. https://doi.org/10.3390/jcm7090261
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.