Effects of Corticosteroid Treatment and Antigen Avoidance in a Large Hypersensitivity Pneumonitis Cohort: A Single-Centre Cohort Study

 , ,
, ,
Abstract
:1. Introduction
2. Experimental Section
2.1. Patient Selection and Data Collection
- Combination of compatible symptoms (dyspnoea and/or cough and/or symptoms with onset shortly after exposure (max 4–6 h) and/or recurrent viral symptoms), suggestive CT findings (extensive ground glass opacities (GGO) and/or centrilobular noduli and/or peribronchovascular fibrosis and/or upper lobe predominant fibrosis and/or airtrapping) and—if biopsy was performed—suggestive pathology data (presence of granuloma’s and/or giant cells and/or a bronchocentric inflammatory infiltrate and/or bronchocentric fibrosis and/or fibrosis with a mixed bronchocentric/usual interstitial pneumonia (UIP)-like pattern)
- Combination of compatible symptoms (cf supra) and suggestive CT findings (cf supra) and compatible pathology findings (any fibrosis and no other disease more probable according to the pathology report)
- Combination of compatible symptoms (cf supra) and compatible CT findings (fibrosis with a UIP-like or non-specific interstitial pneumonia (NSIP)-like pattern) and suggestive pathology findings (cf supra).
2.2. Outcome
2.3. Statistical Analysis
3. Results
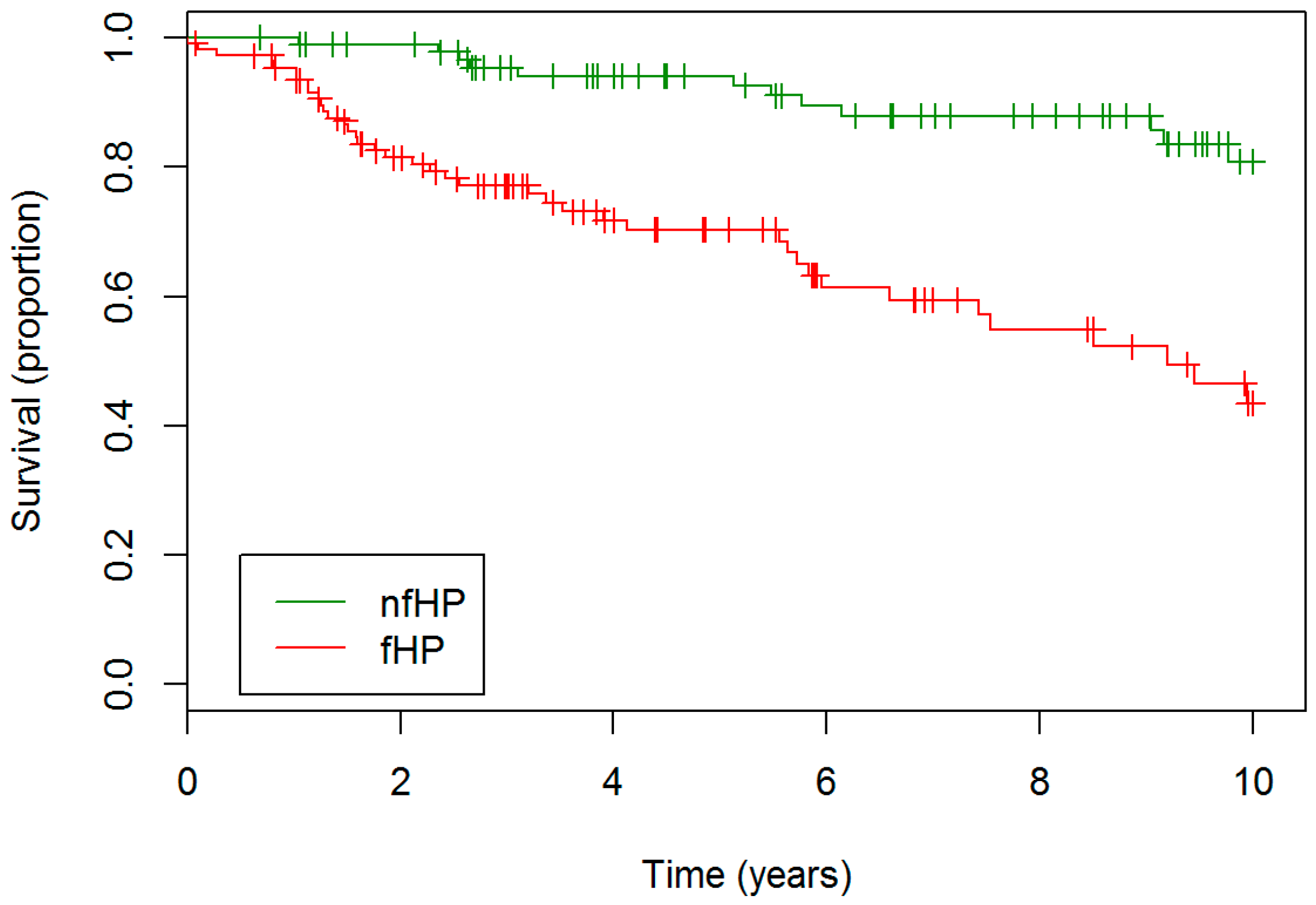
3.1. Diagnostic Categories and Considerations
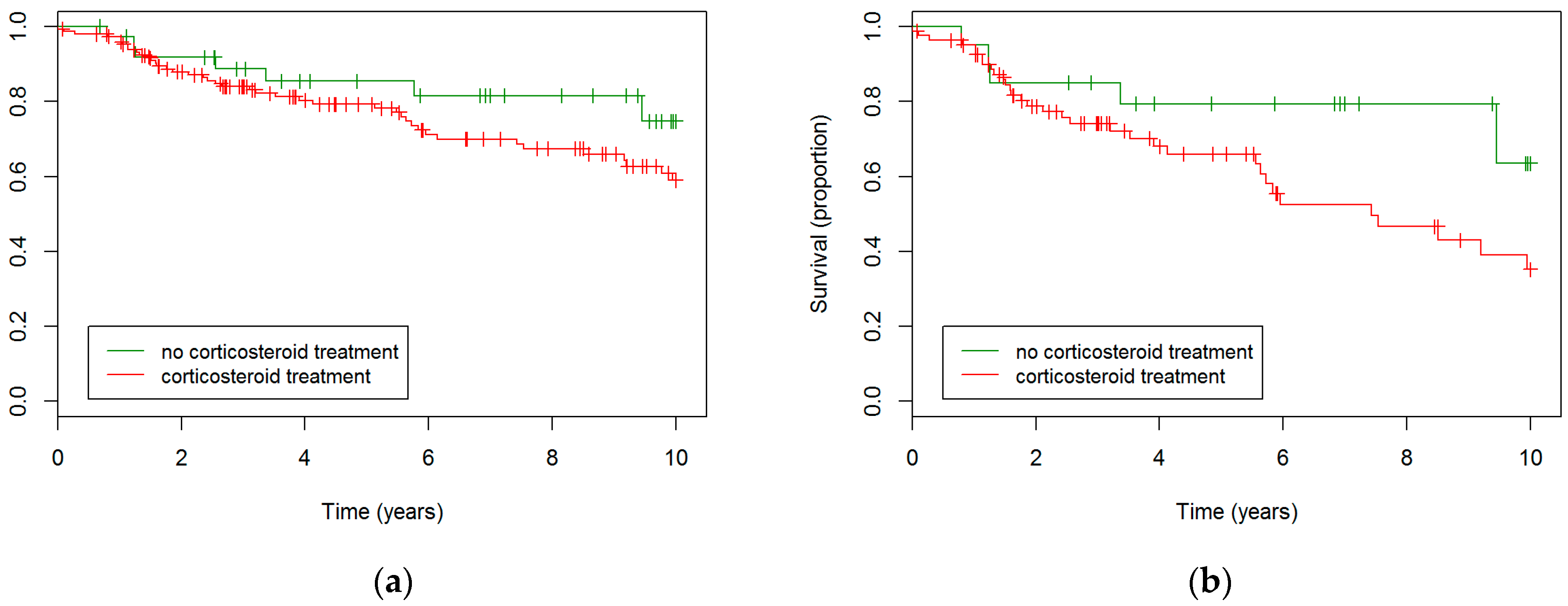
3.2. Corticosteroid Treatment
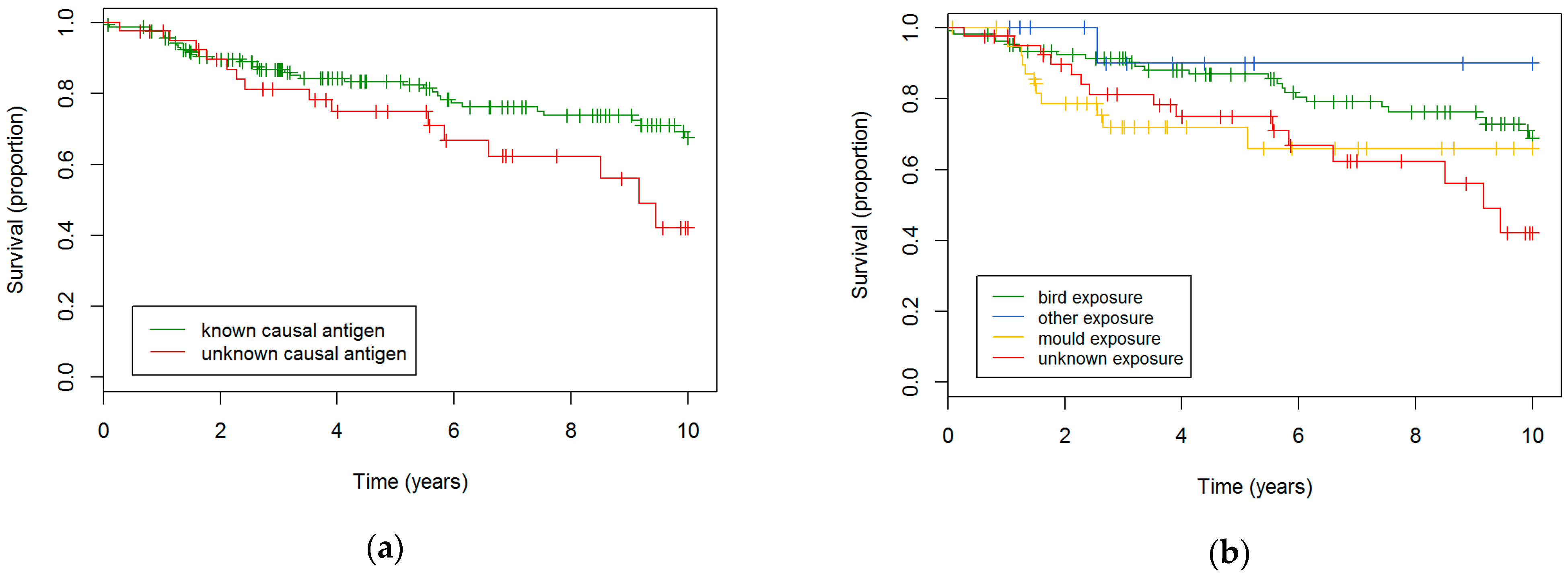
3.3. Exposure Type
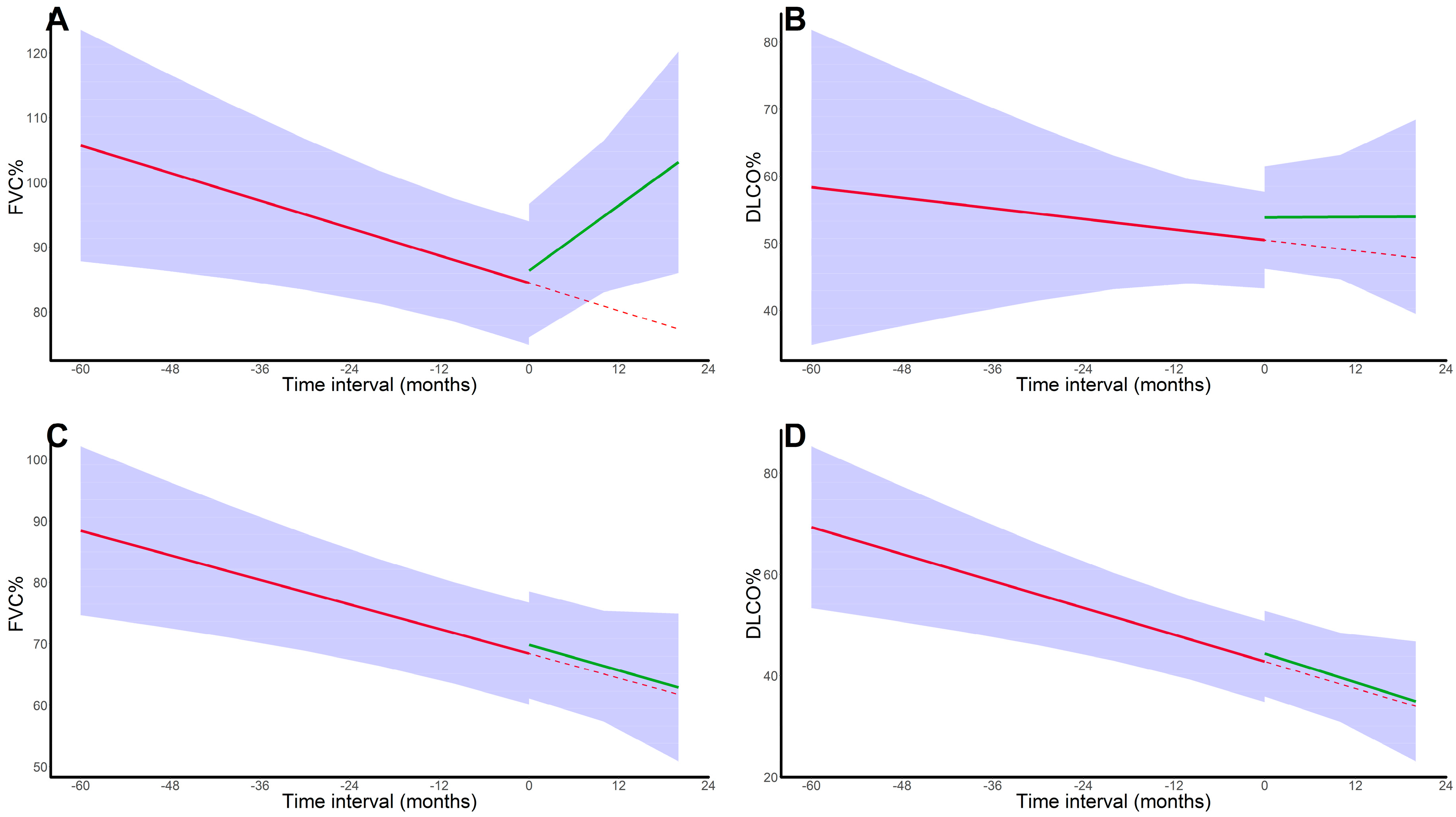
3.4. Exposure Avoidance
3.5. Clinical Behaviour Based on Symptoms Type and Chronicity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Solaymani-Dodaran, M.; West, J.; Smith, C.; Hubbard, R. Extrinsic allergic alveolitis: Incidence and mortality in the general population. QJM 2007, 100, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Costabel, U.; Bonella, F.; Guzman, J. Chronic Hypersensitivity Pneumonitis. Clin. Chest Med. 2012, 33, 151–163. [Google Scholar] [CrossRef] [PubMed]
- Lacasse, Y.; Girard, M.; Cormier, Y. Recent advances in hypersensitivity pneumonitis. Chest 2012, 142, 208–217. [Google Scholar] [CrossRef]
- Mönkäre, S. Influence of corticosteroid treatment on the course of farmer’s lung. Eur. J. Respir. Dis. 1983, 64, 283–293. [Google Scholar] [PubMed]
- Kokkarinen, J.I.; Tukiainen, H.O.; Terho, E.O. Effect of corticosteroid treatment on the recovery of pulmonary function in farmer’s lung. Am. Rev. Respir. Dis. 1992, 145, 3–5. [Google Scholar] [CrossRef] [PubMed]
- Morisset, J.; Johannson, K.A.; Vittinghoff, E.; Aravena, C.; Elicker, B.M.; Jones, K.D.; Fell, C.D.; Manganas, H.; Dubé, B.P.; Wolters, P.J.; et al. Use of Mycophenolate Mofetil or Azathioprine for the Management of Chronic Hypersensitivity Pneumonitis. Chest 2017, 151, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Adegunsoye, A.; Oldham, J.M.; Fernández Pérez, E.R.; Hamblin, M.; Patel, N.; Tener, M.; Bhanot, D.; Robinson, L.; Bullick, S.; Chen, L.; et al. Outcomes of immunosuppressive therapy in chronic hypersensitivity pneumonitis. ERJ Open Res. 2017, 3. [Google Scholar] [CrossRef]
- Vasakova, M.; Morell, F.; Walsh, S.; Leslie, K.; Raghu, G. Hypersensitivity pneumonitis: Perspectives in diagnosis and management. Am. J. Respir. Crit. Care Med. 2017, 196, 680–689. [Google Scholar] [CrossRef]
- Lacasse, Y.; Selman, M.; Costabel, U.; Dalphin, J.C.; Ando, M.; Morell, F.; Erkinjuntti-Pekkanen, R.; Müller, N.; Colby, T.V.; Schuyler, M.; et al. Clinical Diagnosis of Hypersensitivity Pneumonitis. Am. J. Respir. Crit. Care Med. 2003, 168, 952–958. [Google Scholar] [CrossRef] [Green Version]
- Lacasse, Y.; Selman, M.; Costabel, U.; Dalphin, J.C.; Morell, F.; Erkinjuntti-Pekkanen, R.; Mueller, N.L.; Colby, T.V.; Schuyler, M.; Jomphe, V.; et al. Classification of hypersensitivity pneumonitis: A hypothesis. Int. Arch. Allergy Immunol. 2009, 149, 161–166. [Google Scholar] [CrossRef]
- Pérez, E.R.F.; Swigris, J.J.; Forssén, A.V.; Tourin, O.; Solomon, J.J.; Huie, T.J.; Olson, A.L.; Brown, K.K.; Fernandez Perez, E.R.; Swigris, J.J.; et al. Identifying an inciting antigen is associated with improved survival in patients with chronic hypersensitivity pneumonitis. Chest 2013, 144, 1644–1651. [Google Scholar] [CrossRef]
- Salisbury, M.L.; Gu, T.; Murray, S.; Gross, B.H.; Chughtai, A.; Sayyouh, M.; Kazerooni, E.A.; Myers, J.L.; Lagstein, A.; Konopka, K.E.; et al. Hypersensitivity Pneumonitis: Radiologic Phenotypes are Associated with Distinct Survival Time and Pulmonary Function Trajectory. Chest 2018. [Google Scholar] [CrossRef] [PubMed]
- Vourlekis, J.S.; Schwarz, M.I.; Cherniack, R.M.; Curran-Everett, D.; Cool, C.D.; Tuder, R.M.; King, T.E.; Brown, K.K. The effect of pulmonary fibrosis on survival in patients with hypersensitivity pneumonitis. Am. J. Med. 2004, 116, 662–668. [Google Scholar] [CrossRef] [PubMed]
- Sahin, H.; Brown, K.K.; Curran-Everett, D.; Hale, V.; Cool, C.D.; Vourlekis, J.S.; Lynch, D.A. Chronic hypersensitivity pneumonitis: CT features comparison with pathologic evidence of fibrosis and survival. Radiology 2007, 244, 591–598. [Google Scholar] [CrossRef]
- Hanak, V.; Golbin, J.M.; Hartman, T.E.; Ryu, J.H. High-resolution CT findings of parenchymal fibrosis correlate with prognosis in hypersensitivity pneumonitis. Chest 2008, 134, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Churg, A.; Sin, D.D.; Everett, D.; Brown, K.; Cool, C. Pathologic patterns and survival in chronic hypersensitivity pneumonitis. Am. J. Surg. Pathol. 2009, 33, 1765–1770. [Google Scholar] [CrossRef]
- Walsh, S.L.F.; Sverzellati, N.; Devaraj, A.; Wells, A.U.; Hansell, D.M. Chronic hypersensitivity pneumonitis: High resolution computed tomography patterns and pulmonary function indices as prognostic determinants. Eur. Radiol. 2012, 22, 1672–1679. [Google Scholar] [CrossRef]
- Wang, P.; Jones, K.D.; Urisman, A.; Elicker, B.M.; Urbania, T.; Johannson, K.A.; Assayag, D.; Lee, J.; Wolters, P.J.; Collard, H.R.; et al. Pathologic Findings and Prognosis in a Large Prospective Cohort of Chronic Hypersensitivity Pneumonitis. Chest 2017, 152, 502–509. [Google Scholar] [CrossRef]
- Salisbury, M.L.; Myers, J.L.; Belloli, E.A.; Kazerooni, E.A.; Martinez, F.J.; Flaherty, K.R. Diagnosis and treatment of fibrotic hypersensitivity pneumonia: Where we stand and where we need to go. Am. J. Respir. Crit. Care Med. 2017, 196, 690–699. [Google Scholar] [CrossRef] [PubMed]
- Morisset, J.; Johannson, K.A.; Jones, K.D.; Wolters, P.J.; Collard, H.R.; Walsh, S.L.F.; Ley, B. Identification of Diagnostic Criteria for Chronic Hypersensitivity Pneumonitis: An International Modified Delphi Survey. Am. J. Respir. Crit. Care Med. 2017, 197. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.; Egger, M.; Pocock, S.; Gøtzsche, P.; Vandenbroucke, J. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Gimenez, A.; Storrer, K.; Kuranishi, L.; Soares, M.R.; Ferreira, R.G.; Pereira, C.A.C. Change in FVC and survival in chronic fibrotic hypersensitivity pneumonitis. Thorax 2017. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| nfHP (N = 93) | fHP (N = 109) | p Value | |
|---|---|---|---|
| Age (year) | 55.12 ± 13.19 | 65.29 ± 11.72 | <0.001 |
| Gender (male) | 53 (57%) | 69 (63.3%) | 0.441 |
| Ever smoker | 36 (39.6%) | 49 (45.8%) | 0.46 |
| Active smoker | 1 (1.1%) | 3 (3%) | 0.624 |
| Exposure unknown | 10 (10.8%) | 31 (28.4%) | 0.003 |
| Positive SsIgGs | 53 (79.1%) | 55 (63.2%) | 0.06 |
| BAL lymphocytosis | 40.51 ± 25.57 | 19.64 ± 18.76 | <0.001 |
| FVC% baseline | 81.61 ± 22.91 | 72.26 ± 21.89 | 0.005 |
| DLCO% baseline | 57.2 ± 20.7 | 45.3 ± 17.5 | <0.001 |
| Traction bronchiectasis | 0 (0%) | 87 (79.8%) | <0.001 |
| Honeycombing | 0 (0%) | 40 (36.7%) | <0.001 |
| Discussed at MDD | 34 (39.1%) | 61 (58.1%) | 0.013 |
| Corticosteroid treatment | 67 (78.8%) | 82 (80.4%) | 0.934 |
| 2nd line immunosuppressive treatment * | 8 (10%) | 24 (24.5%) | 0.021 |
| Birds | Mould | Other/Unclear | Unknown | |
|---|---|---|---|---|
| nfHP | 61 (65.6%) | 16 (17.2%) | 6 (6.4%) | 10 (10.8%) |
| fHP | 45 (41.3%) | 24 (22.0%) | 9 (8.3%) | 31 (28.4%) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Sadeleer, L.J.; Hermans, F.; De Dycker, E.; Yserbyt, J.; Verschakelen, J.A.; Verbeken, E.K.; Verleden, G.M.; Wuyts, W.A. Effects of Corticosteroid Treatment and Antigen Avoidance in a Large Hypersensitivity Pneumonitis Cohort: A Single-Centre Cohort Study. J. Clin. Med. 2019, 8, 14. https://doi.org/10.3390/jcm8010014
De Sadeleer LJ, Hermans F, De Dycker E, Yserbyt J, Verschakelen JA, Verbeken EK, Verleden GM, Wuyts WA. Effects of Corticosteroid Treatment and Antigen Avoidance in a Large Hypersensitivity Pneumonitis Cohort: A Single-Centre Cohort Study. Journal of Clinical Medicine. 2019; 8(1):14. https://doi.org/10.3390/jcm8010014
Chicago/Turabian StyleDe Sadeleer, Laurens J., Frederik Hermans, Els De Dycker, Jonas Yserbyt, Johny A. Verschakelen, Eric K. Verbeken, Geert M. Verleden, and Wim A. Wuyts. 2019. "Effects of Corticosteroid Treatment and Antigen Avoidance in a Large Hypersensitivity Pneumonitis Cohort: A Single-Centre Cohort Study" Journal of Clinical Medicine 8, no. 1: 14. https://doi.org/10.3390/jcm8010014