Polymorphisms in ERCC5 rs17655 and ERCC1 rs735482 Genes Associated with the Survival of Male Patients with Postoperative Oral Squamous Cell Carcinoma Treated with Adjuvant Concurrent Chemoradiotherapy

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Population
2.2. Sample Preparation and DNA Extraction
2.3. SNP Selection and Genotyping
2.4. Patient Treatment and Follow-Up
2.5. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics of Study Participants
3.2. Survival Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Chiang, C.-J.; Lo, W.-C.; Yang, Y.-W.; You, S.-L.; Chen, C.-J.; Lai, M.-S. Incidence and survival of adult cancer patients in Taiwan, 2002–2012. J. Formos. Med. Assoc. 2016, 115, 1076–1088. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amit, M.; Yen, T.C.; Liao, C.T.; Chaturvedi, P.; Agarwal, J.P.; Kowalski, L.P.; Ebrahimi, A.; Clark, J.R.; Kreppel, M.; Zoller, J.; et al. Improvement in survival of patients with oral cavity squamous cell carcinoma: An international collaborative study. Cancer 2013, 119, 4242–4248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leemans, C.R.; Tiwari, R.; Nauta, J.J.; van der Waal, I.; Snow, G.B. Recurrence at the primary site in head and neck cancer and the significance of neck lymph node metastases as a prognostic factor. Cancer 1994, 73, 187–190. [Google Scholar] [CrossRef] [Green Version]
- Markopoulos, A.K. Current Aspects on Oral Squamous Cell Carcinoma. Open Dent. J. 2012, 6, 126–130. [Google Scholar] [CrossRef] [PubMed]
- Adelstein, D.; Gillison, M.L.; Pfister, D.G.; Spencer, S.; Adkins, D.; Brizel, D.M.; Burtness, B.; Busse, P.M.; Caudell, J.J.; Cmelak, A.J.; et al. NCCN Guidelines Insights: Head and Neck Cancers, Version 2.2017. J. Natl. Compr. Cancer Netw. 2017, 15, 761–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Otsuru, M.; Ota, Y.; Aoki, T.; Sasaki, M.; Suzuki, T.; Denda, Y.; Takahashi, M.; Akiba, T.; Kaneko, A. A Study of Adjuvant Chemoradiotherapy with Tri-weekly Cisplatin for Postoperative High-risk Oral Squamous Cell Carcinoma. Tokai J. Exp. Clin. Med. 2017, 42, 19–24. [Google Scholar] [PubMed]
- Ferris, R.L.; Geiger, J.L.; Trivedi, S.; Schmitt, N.C.; Heron, D.E.; Johnson, J.T.; Kim, S.; Duvvuri, U.; Clump, D.A.; Bauman, J.E.; et al. Phase II trial of post-operative radiotherapy with concurrent cisplatin plus panitumumab in patients with high-risk, resected head and neck cancer. Ann. Oncol. 2016, 27, 2257–2262. [Google Scholar] [CrossRef] [Green Version]
- Bernier, J.; Domenge, C.; Ozsahin, M.; Matuszewska, K.; Lefebvre, J.L.; Greiner, R.H.; Giralt, J.; Maingon, P.; Rolland, F.; Bolla, M.; et al. Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N. Engl. J. Med. 2004, 350, 1945–1952. [Google Scholar] [CrossRef]
- Tanvetyanon, T.; Padhya, T.; McCaffrey, J.; Kish, J.A.; Deconti, R.C.; Trotti, A.; Rao, N.G. Postoperative concurrent chemotherapy and radiotherapy for high-risk cutaneous squamous cell carcinoma of the head and neck. Head Neck 2015, 37, 840–845. [Google Scholar] [CrossRef]
- Leeman, J.E.; Li, J.G.; Pei, X.; Venigalla, P.; Zumsteg, Z.S.; Katsoulakis, E.; Lupovitch, E.; McBride, S.M.; Tsai, C.J.; Boyle, J.O.; et al. Patterns of Treatment Failure and Postrecurrence Outcomes Among Patients With Locally Advanced Head and Neck Squamous Cell Carcinoma After Chemoradiotherapy Using Modern Radiation Techniques. JAMA Oncol. 2017, 3, 1487–1494. [Google Scholar] [CrossRef]
- Jin, H.; Xie, X.; Wang, H.; Hu, J.; Liu, F.; Liu, Z.; Zhou, J.; Zhang, Y.; Xi, X.; Hu, B.; et al. ERCC1 Cys8092Ala and XRCC1 Arg399Gln polymorphisms predict progression-free survival after curative radiotherapy for nasopharyngeal carcinoma. PLoS ONE 2014, 9, e101256. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Qi, B.; Guo, X.; Tang, L.Q.; Chen, Q.Y.; Zhang, L.; Guo, L.; Luo, D.H.; Huang, P.Y.; Mo, H.Y.; et al. Genetic variations in radiation and chemotherapy drug action pathways and survival in locoregionally advanced nasopharyngeal carcinoma treated with chemoradiotherapy. PLoS ONE 2013, 8, e82750. [Google Scholar] [CrossRef] [PubMed]
- Lopes-Aguiar, L.; Costa, E.F.D.; Nogueira, G.A.S.; Lima, T.R.P.; Visacri, M.B.; Pincinato, E.C.; Calonga, L.; Mariano, F.V.; de Almeida Milani Altemani, A.M.; Altemani, J.M.C.; et al. XPD c.934G>A polymorphism of nucleotide excision repair pathway in outcome of head and neck squamous cell carcinoma patients treated with cisplatin chemoradiation. Oncotarget 2016, 8, 16190–16201. [Google Scholar] [CrossRef] [PubMed]
- Nanda, S.S.; Gandhi, A.K.; Rastogi, M.; Khurana, R.; Hadi, R.; Sahni, K.; Mishra, S.P.; Srivastava, A.K.; Bhatt, M.L.B.; Parmar, D. Evaluation of XRCC1 Gene Polymorphism as a Biomarker in Head and Neck Cancer Patients Undergoing Chemoradiation Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 593–601. [Google Scholar] [CrossRef]
- Rouillon, C.; White, M.F. The evolution and mechanisms of nucleotide excision repair proteins. Res. Microbiol. 2011, 162, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Gao, C.; Wang, J.; Li, C.; Zhang, W.; Liu, G. A Functional Polymorphism (rs10817938) in the XPA Promoter Region Is Associated with Poor Prognosis of Oral Squamous Cell Carcinoma in a Chinese Han Population. PLoS ONE 2016, 11, e0160801. [Google Scholar] [CrossRef] [PubMed]
- Tan, L.M.; Qiu, C.F.; Zhu, T.; Jin, Y.X.; Li, X.; Yin, J.Y.; Zhang, W.; Zhou, H.H.; Liu, Z.Q. Genetic Polymorphisms and Platinum-based Chemotherapy Treatment Outcomes in Patients with Non-Small Cell Lung Cancer: A Genetic Epidemiology Study Based Meta-analysis. Sci. Rep. 2017, 7, 5593. [Google Scholar] [CrossRef]
- Wang, C.; Nie, H.; Li, Y.; Liu, G.; Wang, X.; Xing, S.; Zhang, L.; Chen, X.; Chen, Y.; Li, Y. The study of the relation of DNA repair pathway genes SNPs and the sensitivity to radiotherapy and chemotherapy of NSCLC. Sci. Rep. 2016, 6, 26526. [Google Scholar] [CrossRef] [Green Version]
- Zhang, R.; Zhou, F.; Cheng, L.; Yu, A.; Zhu, M.; Wang, M.; Zhang, Z.; Xiang, J.; Wei, Q. Genetic variants in nucleotide excision repair pathway predict survival of esophageal squamous cell cancer patients receiving platinum-based chemotherapy. Mol. Carcinog. 2018, 57, 1553–1565. [Google Scholar] [CrossRef]
- Zhou, F.; Zhu, M.; Wang, M.; Qiu, L.; Cheng, L.; Jia, M.; Xiang, J.; Wei, Q. Genetic variants of DNA repair genes predict the survival of patients with esophageal squamous cell cancer receiving platinum-based adjuvant chemotherapy. J. Transl. Med. 2016, 14, 154. [Google Scholar] [CrossRef]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA: A Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Stephens, M.; Smith, N.J.; Donnelly, P. A new statistical method for haplotype reconstruction from population data. Am. J. Hum. Genet. 2001, 68, 978–989. [Google Scholar] [CrossRef] [PubMed]
- Schärer, O.D. Nucleotide Excision Repair in Eukaryotes. Cold Spring Harb. Perspect. Biol. 2013, 5, a012609. [Google Scholar] [CrossRef] [PubMed]
- Friedberg, E.C. How nucleotide excision repair protects against cancer. Nat. Rev. Cancer 2001, 1, 22–33. [Google Scholar] [CrossRef] [PubMed]
- Naccarati, A.; Rosa, F.; Vymetalkova, V.; Barone, E.; Jiraskova, K.; Di Gaetano, C.; Novotny, J.; Levy, M.; Vodickova, L.; Gemignani, F.; et al. Double-strand break repair and colorectal cancer: Gene variants within 3′ UTRs and microRNAs binding as modulators of cancer risk and clinical outcome. Oncotarget 2016, 7, 23156–23169. [Google Scholar] [CrossRef]
- Mucha, B.; Pytel, D.; Markiewicz, L.; Cuchra, M.; Szymczak, I.; Przybylowska-Sygut, K.; Dziki, A.; Majsterek, I.; Dziki, L. Nucleotide Excision Repair Capacity and XPC and XPD Gene Polymorphism Modulate Colorectal Cancer Risk. Clin. Colorectal. Cancer 2018, 17, e435–e441. [Google Scholar] [CrossRef] [PubMed]
- Sugasawa, K.; Ng, J.M.; Masutani, C.; Iwai, S.; van der Spek, P.J.; Eker, A.P.; Hanaoka, F.; Bootsma, D.; Hoeijmakers, J.H. Xeroderma pigmentosum group C protein complex is the initiator of global genome nucleotide excision repair. Mol. Cell 1998, 2, 223–232. [Google Scholar] [CrossRef]
- Zheng, Y.; Deng, Z.; Yin, J.; Wang, S.; Lu, D.; Wen, X.; Li, X.; Xiao, D.; Hu, C.; Chen, X.; et al. The association of genetic variations in DNA repair pathways with severe toxicities in NSCLC patients undergoing platinum-based chemotherapy. Int. J. Cancer 2017, 141, 2336–2347. [Google Scholar] [CrossRef] [PubMed]
- Ravegnini, G.; Nannini, M.; Simeon, V.; Musti, M.; Sammarini, G.; Saponara, M.; Gatto, L.; Urbini, M.; Astolfi, A.; Biasco, G.; et al. Polymorphisms in DNA repair genes in gastrointestinal stromal tumours: Susceptibility and correlation with tumour characteristics and clinical outcome. Tumour Biol. 2016, 37, 13413–13423. [Google Scholar] [CrossRef]
- Li, Y.; Liu, Z.; Liu, H.; Wang, L.E.; Onodera, H.; Suzuki, A.; Suzuki, K.; Wadhwa, R.; Elimova, E.; Sudo, K.; et al. Potentially functional variants in the core nucleotide excision repair genes predict survival in Japanese gastric cancer patients. Carcinogenesis 2014, 35, 2031–2038. [Google Scholar] [CrossRef] [Green Version]
- Hua, R.-X.; Zhuo, Z.-J.; Shen, G.-P.; Zhu, J.; Zhang, S.-D.; Xue, W.-Q.; Li, X.-Z.; Zhang, P.-F.; He, J.; Jia, W.-H. Polymorphisms in the XPC gene and gastric cancer susceptibility in a Southern Chinese population. Onco Targets Ther. 2016, 9, 5513–5519. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.L.; Yang, L.B.; Geng, X.L.; Zhou, Q.L.; Qin, H.; Yang, L.; Dong, Y.Z.; Zhong, J.J. The association of XPG and MMS19L polymorphisms response to chemotherapy in osteosarcoma. Pak. J. Med. Sci. 2013, 29, 1225–1229. [Google Scholar] [CrossRef] [PubMed]
- Song, X.; Sturgis, E.M.; Jin, L.; Wang, Z.; Wei, Q.; Li, G. Variants in nucleotide excision repair core genes and susceptibility to recurrence of squamous cell carcinoma of the oropharynx. Int. J. Cancer 2013, 133, 695–704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowden, N.A. Nucleotide excision repair: Why is it not used to predict response to platinum-based chemotherapy? Cancer Lett. 2014, 346, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Arriagada, R.; Bergman, B.; Dunant, A.; Le Chevalier, T.; Pignon, J.P.; Vansteenkiste, J. Cisplatin-based adjuvant chemotherapy in patients with completely resected non-small-cell lung cancer. N. Engl. J. Med. 2004, 350, 351–360. [Google Scholar] [CrossRef] [PubMed]
- Olaussen, K.A.; Dunant, A.; Fouret, P.; Brambilla, E.; Andre, F.; Haddad, V.; Taranchon, E.; Filipits, M.; Pirker, R.; Popper, H.H.; et al. DNA repair by ERCC1 in non-small-cell lung cancer and cisplatin-based adjuvant chemotherapy. N. Engl. J. Med. 2006, 355, 983–991. [Google Scholar] [CrossRef] [PubMed]
- Lafaurie, G.I.; Perdomo, S.J.; Buenahora, M.R.; Amaya, S.; Diaz-Baez, D. Human papilloma virus: An etiological and prognostic factor for oral cancer? J. Investig. Clin. Dent. 2018, 9, e12313. [Google Scholar] [CrossRef]
- Kwon, M.; Kim, J.W.; Roh, J.L.; Park, Y.; Cho, K.J.; Choi, S.H.; Nam, S.Y.; Kim, S.Y.; Lee, B.H. Recurrence and cancer-specific survival according to the expression of IL-4Ralpha and IL-13Ralpha1 in patients with oral cavity cancer. Eur. J. Cancer (Oxf. Engl.: 1990) 2015, 51, 177–185. [Google Scholar] [CrossRef]


{kind=link}
| Variable | n (%) |
|---|---|
| Total | 319 (100) |
| Mean age (SD), years | 49.72 (9.8) |
| Age, years | |
| <50 | 164 (51.41) |
| ≥50 | 155 (48.59) |
| Ethnicity of father | |
| Taiwanese | 230 (72.10) |
| Hakka | 72 (22.57) |
| Mainland Chinese | 17 (5.33) |
| Ethnicity of mother | |
| Taiwanese | 239 (74.92) |
| Hakka | 74 (23.20) |
| Mainland Chinese | 6 (1.88) |
| BMI, kg/m2 | |
| <18.5 | 22 (6.90) |
| 18.5–23.9 | 157 (49.22) |
| ≥24 | 140 (43.89) |
| Cigarette smoking | |
| Never | 47 (14.73) |
| Ever | 272 (85.27) |
| Alcohol drinking | |
| Never | 98 (30.72) |
| Ever | 221 (69.28) |
| Betel nut chewing | |
| Never | 44 (13.79) |
| Ever | 275 (86.21) |
| Tea drinking | |
| Never | 163 (51.10) |
| Ever | 156 (48.90) |
| Coffee drinking | |
| Never | 243 (76.18) |
| Ever | 76 (23.82) |
| Tumor differentiation | |
| Well differentiated | 51 (15.99) |
| Moderate | 210 (65.83) |
| Poor | 55 (17.24) |
| Unclear | 3 (0.94) |
| Primary tumor size | |
| T1–T2 | 122 (38.24) |
| T3–T4 | 197 (61.76) |
| Nodal involvement | |
| N0–N1 | 102 (31.97) |
| N2–N3 | 217 (67.92) |
| Perineural invasion | |
| No | 142 (44.51) |
| Yes | 177 (55.49) |
| Vascular invasion | |
| No | 300 (94.04) |
| Yes | 19 (5.96) |
| Lymphatic invasion | |
| No | 279 (87.46) |
| Yes | 40 (12.54) |
| Extranodal extension | |
| No | 114 (35.74) |
| Yes | 205 (64.26) |
| Pathologic TNM stage | |
| III | 42 (13.17) |
| IV | 277 (86.83) |
| Variable | Overall Survival | Disease-Free Survival | ||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age | ||||
| <50 | 1.00 | 1.00 | ||
| ≥50 | 0.67 (0.44–1.03) | 0.068 | 0.81 (0.57–1.15) | 0.239 |
| Ethnicity of father | ||||
| Taiwanese | 1.00 | 1.00 | ||
| Hakka | 0.88 (0.51–1.50) | 0.633 | 0.66 (0.40–1.08) | 0.101 |
| Mainland Chinese | 1.27 (0.55–2.93) | 0.577 | 1.72 (0.94–3.14) | 0.079 |
| Ethnicity of mother | ||||
| Taiwanese | 1.00 | 1.00 | ||
| Hakka | 0.75 (0.43–1.29) | 0.295 | 0.67 (0.42–1.08) | 0.100 |
| Mainland Chinese | 1.80 (0.57–5.72) | 0.320 | 1.60 (0.59–4.37) | 0.355 |
| BMI, kg/m2 | ||||
| 18.5–23.9 | 1.00 | 1.00 | ||
| <18.5 | 0.85 (0.36–1.98) | 0.705 | 1.49 (0.79–2.84) | 0.223 |
| ≥24 | 0.66 (0.42–1.03) | 0.068 | 0.84 (0.58–1.23) | 0.372 |
| Cigarette smoking | ||||
| Never | 1.00 | 1.00 | ||
| Ever | 0.89 (0.51–1.57) | 0.675 | 1.02 (0.62–1.68) | 0.938 |
| Alcohol drinking | ||||
| Never | 1.00 | 1.00 | ||
| Ever | 0.99 (0.64–1.54) | 0.971 | 1.10 (0.75–1.61) | 0.636 |
| Betel nut chewing | ||||
| Never | 1.00 | 1.00 | ||
| Ever | 1.09 (0.58–2.05) | 0.794 | 1.40 (0.80–2.45) | 0.240 |
| Tea drinking | ||||
| Never | 1.00 | 1.00 | ||
| Ever | 0.93 (0.61–1.41) | 0.727 | 1.07 (0.75–1.53) | 0.701 |
| Coffee drinking | ||||
| Never | 1.00 | 1.00 | ||
| Ever | 0.65 (0.37–1.13) | 0.123 | 1.27 (0.85–1.89) | 0.251 |
| Tumor differentiation | ||||
| Well differentiated | 1.00 | 1.00 | ||
| Moderate | 0.94 (0.55–1.60) | 0.819 | 0.89 (0.56–1.44) | 0.645 |
| Poor | 0.84 (0.40–1.74) | 0.629 | 1.22 (0.68–2.18) | 0.500 |
| Unclear | 2.80 (0.37–1.19) | 0.319 | 1.66 (0.22–2.39) | 0.621 |
| Primary tumor size | ||||
| T1–T2 | 1.00 | 1.00 | ||
| T3–T4 | 1.29 (0.83–2.01) | 0.258 | 1.72 (1.17–2.53) | 0.006 * |
| Nodal involvement | ||||
| N0–N1 | 1.00 | 1.00 | ||
| N2–N3 | 2.41 (1.42–4.10) | 0.001 * | 1.63 (1.09–2.44) | 0.018 * |
| Perineural invasion | ||||
| No | 1.00 | 1.00 | ||
| Yes | 1.29 (0.85–1.98) | 0.238 | 1.27 (0.89–1.83) | 0.189 |
| Vascular invasion | ||||
| No | 1.00 | 1.00 | ||
| Yes | 1.43 (0.66–3.10) | 0.366 | 0.43 (0.43–2.00) | 0.856 |
| Lymphatic invasion | ||||
| No | 1.00 | 1.00 | ||
| Yes | 2.18 (1.30–3.67) | 0.003 * | 1.37 (0.82–2.28) | 0.233 |
| Extranodal extension | ||||
| No | 1.00 | 1.00 | ||
| Yes | 3.91 (2.13–7.19) | <0.001 * | 1.79 (1.20–2.69) | 0.005 * |
| Pathologic TNM stage | ||||
| III | 1.00 | 1.00 | ||
| IV | 1.64 (0.81–3.29) | 0.168 | 1.66 (0.93–2.96) | 0.087 |
| SNPs | Overall Survival | Disease-Free Survival | ||
|---|---|---|---|---|
| HR (95% CI) a | p Value | HR (95% CI) b | p Value | |
| ERCC5/XPG | ||||
| rs2094258 | ||||
| GG | 1.00 | 1.00 | ||
| GA | 1.14 (0.72–1.79) | 0.574 | 1.07 (0.73–1.57) | 0.726 |
| AA | 0.66 (0.30–1.44) | 0.294 | 1.02 (0.57–1.83) | 0.946 |
| Additive model | 0.91 (0.66–1.25) | 0.559 | 1.03 (0.79–1.34) | 0.839 |
| Dominant model | 1.03 (0.66–1.59) | 0.910 | 1.06 (0.74–1.52) | 0.754 |
| Recessive model | 0.61 (0.29–1.28) | 0.193 | 0.99 (0.57–1.70) | 0.958 |
| rs1047768 | ||||
| TT | 1.00 | 1.00 | ||
| TC | 1.11 (0.72–1.72) | 0.635 | 0.93 (0.64–1.36) | 0.715 |
| CC | 0.63 (0.25–1.62) | 0.339 | 0.76 (0.39–1.51) | 0.438 |
| Additive model | 0.94 (0.67–1.31) | 0.699 | 0.90 (0.68–1.19) | 0.453 |
| Dominant model | 1.03 (0.67–1.58) | 0.891 | 0.90 (0.63–1.29) | 0.574 |
| Recessive model | 0.60 (0.24–1.49) | 0.272 | 0.79 (0.41–1.53) | 0.482 |
| rs17655 | ||||
| GG | 1.00 | 1.00 | ||
| GC | 0.95 (0.58–1.54) | 0.829 | 0.86 (0.56–1.31) | 0.482 |
| CC | 0.93 (0.51–1.69) | 0.811 | 1.38 (0.86–2.19) | 0.180 |
| Additive model | 0.96 (0.72–1.30) | 0.803 | 1.16 (0.91–1.49) | 0.238 |
| Dominant model | 0.94 (0.60–1.49) | 0.799 | 1.01 (0.69–1.49) | 0.954 |
| Recessive model | 0.96 (0.58–1.61) | 0.881 | 1.50 (1.01–2.24) | 0.045 * |
| rs873601 | ||||
| AA | 1.00 | 1.00 | ||
| AG | 0.77 (0.47–1.26) | 0.298 | 0.84 (0.55–1.31) | 0.448 |
| GG | 0.84 (0.47–1.51) | 0.556 | 1.29 (0.80–2.09) | 0.301 |
| Additive model | 0.91 (0.67–1.23) | 0.530 | 1.14 (0.88–1.48) | 0.311 |
| Dominant model | 0.79 (0.50–1.26) | 0.304 | 0.97 (0.65–1.46) | 0.900 |
| Recessive model | 1.00 (0.61–1.64) | 0.988 | 1.44 (0.97–2.14) | 0.070 |
| ERCC2/XPD | ||||
| rs13181 | ||||
| TT | 1.00 | 1.00 | ||
| TG | 1.03 (0.59–1.81) | 0.909 | 1.00 (0.61–1.64) | 0.997 |
| GG | - | 0.989 | - | 0.984 |
| Additive model | 1.03 (0.59–1.80) | 0.921 | 1.00 (0.61–1.63) | 0.993 |
| Dominant model | 1.03 (0.59–1.81) | 0.915 | 1.00 (0.61–1.64) | 0.998 |
| Recessive model | - | 0.989 | - | 0.984 |
| rs1799793 | ||||
| GG | 1.00 | 1.00 | ||
| GA | 1.10 (0.58–2.07) | 0.769 | 1.01 (0.58–1.73) | 0.983 |
| AA | - | 0.99 | - | - |
| Additive model | 1.10 (0.58–2.06) | 0.778 | 1.01 (0.58–1.73) | 0.983 |
| Dominant model | 1.10 (0.58–2.07) | 0.773 | 1.01 (0.58–1.73) | 0.983 |
| Recessive model | - | 0.99 | - | - |
| ERCC1 | ||||
| rs735482 | ||||
| AA | 1.00 | 1.00 | ||
| AC | 0.72 (0.46–1.14) | 0.163 | 0.86 (0.57–1.29) | 0.466 |
| CC | 0.83 (0.44–1.59) | 0.580 | 1.47 (0.89–2.44) | 0.134 |
| Additive model | 0.86 (0.62–1.19) | 0.352 | 1.16 (0.89–1.52) | 0.283 |
| Dominant model | 0.75 (0.48–1.15) | 0.183 | 0.98 (0.67–1.44) | 0.934 |
| Recessive model | 1.01 (0.56–1.83) | 0.975 | 1.61 (1.04–2.51) | 0.034 * |
| rs3212986 | ||||
| GG | 1.00 | 1.00 | ||
| GT | 1.20 (0.76–1.89) | 0.436 | 0.95 (0.66–1.39) | 0.806 |
| TT | 1.04 (0.48–2.28) | 0.922 | 0.96 (0.50–1.85) | 0.912 |
| Additive model | 1.08 (0.78–1.51) | 0.642 | 0.97 (0.73–1.29) | 0.833 |
| Recessive model | 1.17 (0.75–1.82) | 0.481 | 0.96 (0.67–1.37) | 0.805 |
| Dominant model | 0.94 (0.45–1.97) | 0.870 | 0.99 (0.53–1.85) | 0.967 |
| rs11615 | ||||
| CC | 1.00 | 1.00 | ||
| CT | 1.23 (0.79–1.91) | 0.351 | 0.85 (0.59–1.23) | 0.388 |
| TT | 0.90 (0.35–2.28) | 0.817 | 0.72 (0.33–1.59) | 0.416 |
| Additive model | 1.08 (0.77–1.51) | 0.661 | 0.85 (0.63–1.14) | 0.282 |
| Dominant model | 1.18 (0.77–1.81) | 0.438 | 0.83 (0.58–1.19) | 0.316 |
| Recessive model | 0.81 (0.33–2.01) | 0.652 | 0.78 (0.36–1.69) | 0.525 |
| XPC | ||||
| rs2228001 | ||||
| AA | 1.00 | 1.00 | ||
| AC | 1.07 (0.68–1.69) | 0.766 | 1.21 (0.83–1.78) | 0.329 |
| CC | 0.72 (0.30–1.73) | 0.457 | 0.75 (0.37–1.54) | 0.432 |
| Additive model | 0.94 (0.67–1.32) | 0.716 | 0.99 (0.75–1.31) | 0.941 |
| Dominant model | 1.01 (0.65–1.58) | 0.955 | 1.12 (0.77–1.63) | 0.539 |
| Recessive model | 0.69 (0.30–1.60) | 0.384 | 0.68 (0.34–1.34) | 0.260 |
| rs2228000 | ||||
| CC | 1.00 | 1.00 | ||
| TC | 1.06 (0.66–1.68) | 0.822 | 0.81 (0.55–1.18) | 0.267 |
| TT | 1.86 (0.97–3.56) | 0.062 | 1.11 (0.59–2.08) | 0.758 |
| Additive model | 1.28 (0.92–1.77) | 0.144 | 0.94 (0.70–1.25) | 0.652 |
| Dominant model | 1.18 (0.76–1.83) | 0.457 | 0.85 (0.59–1.22) | 0.373 |
| Recessive model | 1.81 (0.99–3.29) | 0.053 | 1.23 (0.67–2.26) | 0.501 |
| XPA | ||||
| rs1800975 | ||||
| AA | 1.00 | 1.00 | ||
| AG | 0.83 (0.50–1.36) | 0.461 | 0.83 (0.51–1.36) | 0.462 |
| GG | 0.65 (0.35–1.21) | 0.175 | 0.65 (0.35–1.21) | 0.174 |
| Additive model | 0.81 (0.60–1.10) | 0.174 | 0.90 (0.70–1.16) | 0.426 |
| Dominant model | 0.77 (0.48–1.24) | 0.282 | 0.77 (0.48–1.24) | 0.283 |
| Recessive model | 0.74 (0.44–1.25) | 0.260 | 0.73 (0.44–1.25) | 0.258 |
| rs10817938 | ||||
| TT | 1.00 | 1.00 | ||
| TC | 1.08 (0.68–1.72) | 0.731 | 1.28 (0.87–1.86) | 0.209 |
| CC | 1.68 (0.65–4.33) | 0.286 | 1.88 (0.75–4.74) | 0.180 |
| Additive model | 1.18 (0.82–1.69) | 0.386 | 1.31 (0.95–1.80) | 0.095 |
| Dominant model | 1.15 (0.74–1.77) | 0.543 | 1.32 (0.91–1.90) | 0.139 |
| Recessive model | 1.64 (0.64–4.17) | 0.304 | 1.73 (0.69–4.32) | 0.239 |
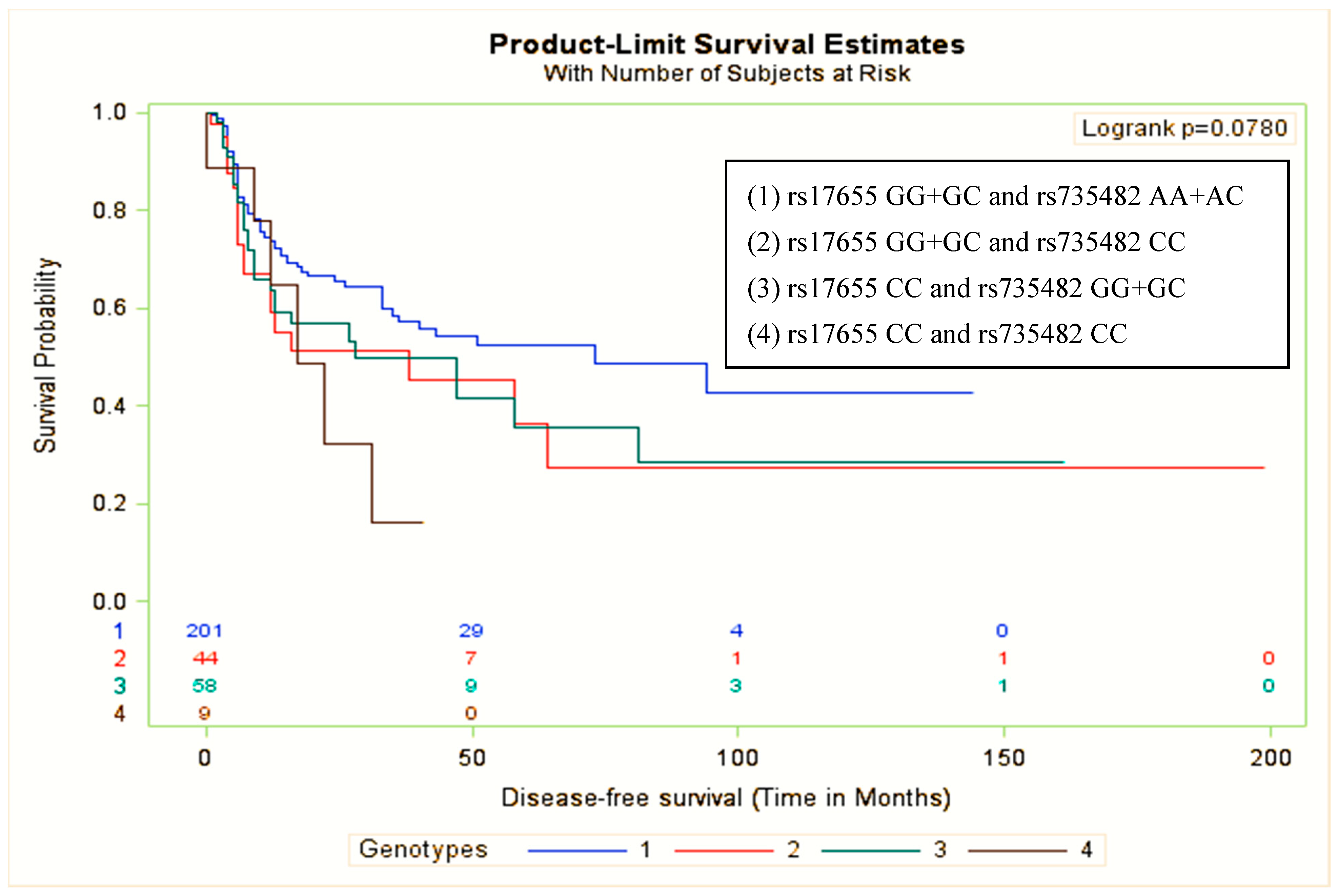
| ERCC5 rs17655 | ERCC1 rs735482 | No. | Event | HR (95% CI) a | p Value |
|---|---|---|---|---|---|
| GG+GC | AA+AC | 206 | 71 | 1.00 | |
| GG+GC | CC | 45 | 19 | 1.63 (0.98–2.72) | 0.060 |
| CC | GG+GC | 59 | 29 | 1.52 (0.98–2.37) | 0.062 |
| CC | CC | 9 | 6 | 2.60 (1.11–6.09) | 0.027 * |
| p for interaction | 0.929 | ||||
| ERCC5 rs17655 | ERCC1 rs735482 | |||||
|---|---|---|---|---|---|---|
| Variable | HR (95% CI) a | p Value | pInteraction | HR (95% CI) a | p Value | pInteraction |
| Age | 0.486 | 0.078 | ||||
| <50 | 1.74 (1.00–3.03) | 0.051 | 1.04 (0.53–2.06) | 0.911 | ||
| ≥50 | 1.24 (0.69–2.23) | 0.473 | 2.76 (1.47–5.19) | 0.002 * | ||
| BMI, kg/m2 | 0.160 | 0.597 | ||||
| 18.5–23.9 | 1.64 (0.95–2.82) | 0.075 | 1.89 (1.04–3.44) | 0.037 * | ||
| <18.5 | 3.06 (0.65–14.49) | 0.159 | 1.30 (0.05–31.65) | 0.871 | ||
| ≥24 | 0.81 (0.37–1.77) | 0.601 | 1.30 (0.62–2.72) | 0.495 | ||
| Cigarette smoking | 0.664 | 0.975 | ||||
| Never | 1.03 (0.35–2.98) | 0.962 | 1.99 (0.52–7.58) | 0.316 | ||
| Ever | 1.54 (0.99–2.41) | 0.056 | 1.61 (1.00–2.59) | 0.051 | ||
| Alcohol drinking | 0.993 | 0.676 | ||||
| Never | 1.59 (0.74–3.42) | 0.240 | 1.43 (0.64–3.22) | 0.387 | ||
| Ever | 1.52 (0.94–2.46) | 0.091 | 1.72 (1.00–2.96) | 0.050 | ||
| Betel nut chewing | 0.445 | 0.968 | ||||
| Never | 2.06 (0.53–8.11) | 0.299 | 1.64 (0.34–7.86) | 0.536 | ||
| Ever | 1.41 (0.92–2.14) | 0.112 | 1.63 (1.02–2.62) | 0.043 * | ||
| Tea drinking | 0.331 | 0.986 | ||||
| Never | 1.88 (1.05–3.35) | 0.033 * | 1.60 (0.87–2.94) | 0.134 | ||
| Ever | 1.27 (0.73–2.24) | 0.400 | 1.57 (0.81–3.04) | 0.183 | ||
| Coffee drinking | 0.073 | 0.077 | ||||
| Never | 1.30 (0.82–2.08) | 0.066 | 2.09 (1.28–3.41) | 0.003 * | ||
| Ever | 2.83 (1.27–6.33) | 0.011 * | 0.72 (0.22–2.42) | 0.601 | ||
| Tumor differentiation | 0.492 | 0.949 | ||||
| Well differentiated | 1.08 (0.43–2.68) | 0.875 | 3.74 (1.26–11.09) | 0.018 * | ||
| Moderate | 1.43 (0.84–2.42) | 0.184 | 1.06 (0.57–1.98) | 0.858 | ||
| Poor | 2.15 (0.88–5.22) | 0.093 | 3.48 (1.23–9.88) | 0.019 * | ||
| Primary tumor size | 0.146 | 0.394 | ||||
| T1–T2 | 0.96 (0.45–2.03) | 0.905 | 1.12 (0.49–2.56) | 0.788 | ||
| T3–T4 | 1.83 (1.14–2.93) | 0.013 * | 1.76 (1.04–3.00) | 0.036 * | ||
| Nodal involvement | 0.328 | 0.125 | ||||
| N0–N1 | 2.25 (1.06–4.81) | 0.036 * | 3.16 (1.47–6.80) | 0.003 * | ||
| N2–N3 | 1.32 (0.82–2.13) | 0.252 | 1.23 (0.69–2.19) | 0.479 | ||
| Perineural invasion | 0.008 * | 0.416 | ||||
| No | 0.77 (0.40–1.49) | 0.429 | 2.07 (1.06–4.03) | 0.032 * | ||
| Yes | 2.46 (1.46–4.15) | <0.001 * | 1.32 (0.72–2.44) | 0.370 | ||
| Vascular invasion | 0.410 | <0.001 * | ||||
| No | 1.45 (0.96–2.19) | 0.078 | 1.51 (0.96–2.37) | 0.076 | ||
| Yes | 1.27 (0.16–10.34) | 0.826 | - | |||
| Lymphatic invasion | 0.553 | 0.449 | ||||
| No | 1.43 (0.92–2.23) | 0.111 | 1.71 (1.07–2.73) | 0.025 * | ||
| Yes | 1.84 (0.64–5.31) | 0.260 | 0.90 (0.20–4.16) | 0.892 | ||
| Extranodal extension | 0.253 | 0.720 | ||||
| No | 2.35 (1.12–4.94) | 0.024 * | 2.17 (0.87–5.40) | 0.097 | ||
| Yes | 1.31 (0.81–2.13) | 0.277 | 1.52 (0.90–2.57) | 0.118 | ||
| Pathologic TNM stage | 0.850 | 0.585 | ||||
| III | 1.70 (0.48–6.09) | 0.414 | 4.82 (0.98–23.58) | 0.053 | ||
| IV | 1.51 (0.99–2.31) | 0.055 | 1.54 (0.96–2.47) | 0.075 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Senghore, T.; Chien, H.-T.; Wang, W.-C.; Chen, Y.-X.; Young, C.-K.; Huang, S.-F.; Yeh, C.-C. Polymorphisms in ERCC5 rs17655 and ERCC1 rs735482 Genes Associated with the Survival of Male Patients with Postoperative Oral Squamous Cell Carcinoma Treated with Adjuvant Concurrent Chemoradiotherapy. J. Clin. Med. 2019, 8, 33. https://doi.org/10.3390/jcm8010033
Senghore T, Chien H-T, Wang W-C, Chen Y-X, Young C-K, Huang S-F, Yeh C-C. Polymorphisms in ERCC5 rs17655 and ERCC1 rs735482 Genes Associated with the Survival of Male Patients with Postoperative Oral Squamous Cell Carcinoma Treated with Adjuvant Concurrent Chemoradiotherapy. Journal of Clinical Medicine. 2019; 8(1):33. https://doi.org/10.3390/jcm8010033
Chicago/Turabian StyleSenghore, Thomas, Huei-Tzu Chien, Wen-Chang Wang, You-Xin Chen, Chi-Kuang Young, Shiang-Fu Huang, and Chih-Ching Yeh. 2019. "Polymorphisms in ERCC5 rs17655 and ERCC1 rs735482 Genes Associated with the Survival of Male Patients with Postoperative Oral Squamous Cell Carcinoma Treated with Adjuvant Concurrent Chemoradiotherapy" Journal of Clinical Medicine 8, no. 1: 33. https://doi.org/10.3390/jcm8010033