Transscleral Fixation of Black Diaphragm Intraocular Lens in Complete Aniridia and Aphakia Due to Posttraumatic Eye Rupture: A Pilot Study



 and
and 
Abstract
:1. Introduction
2. Material and Methods
2.1. Black Diaphragm Intraocular Lens
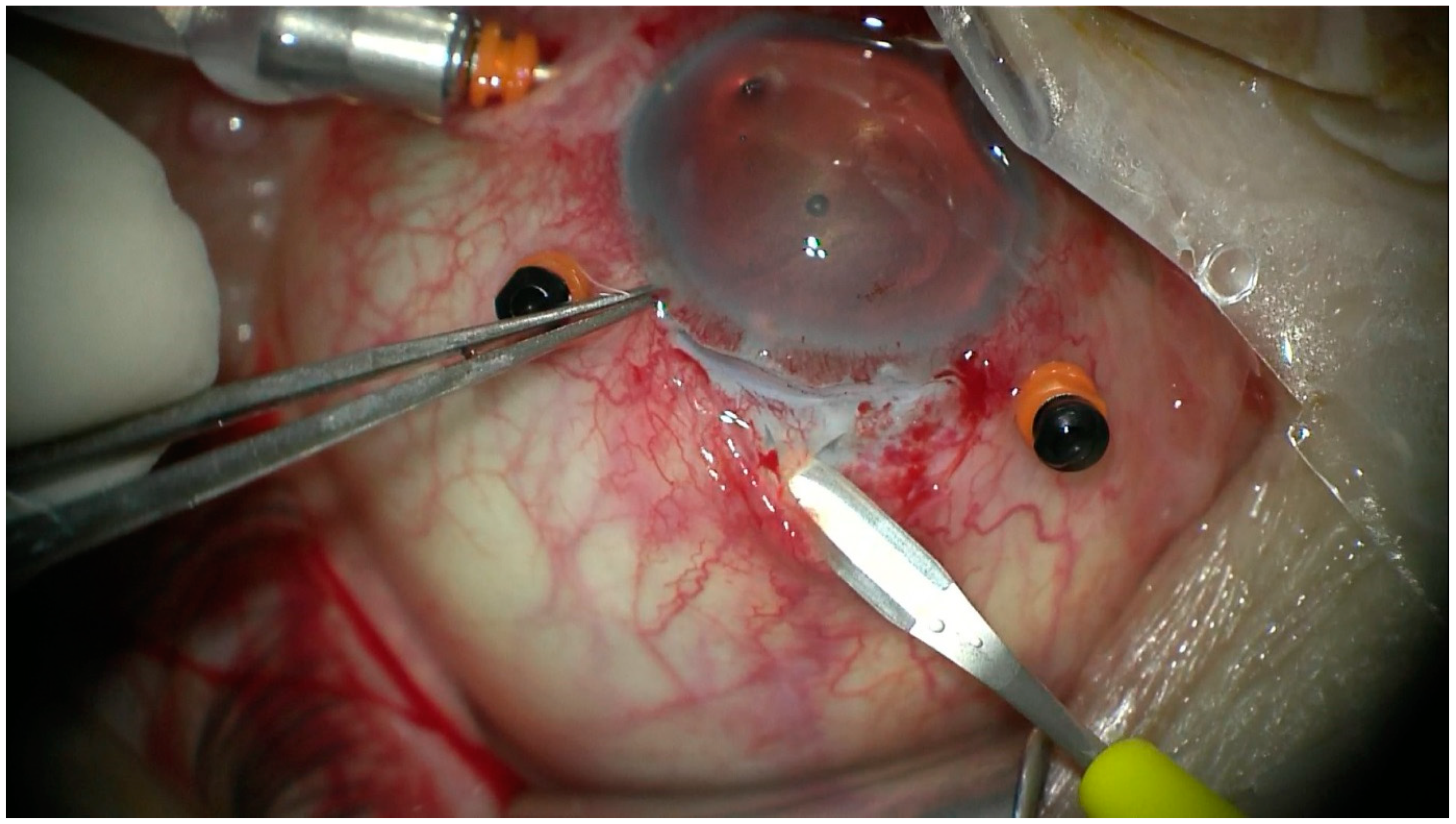
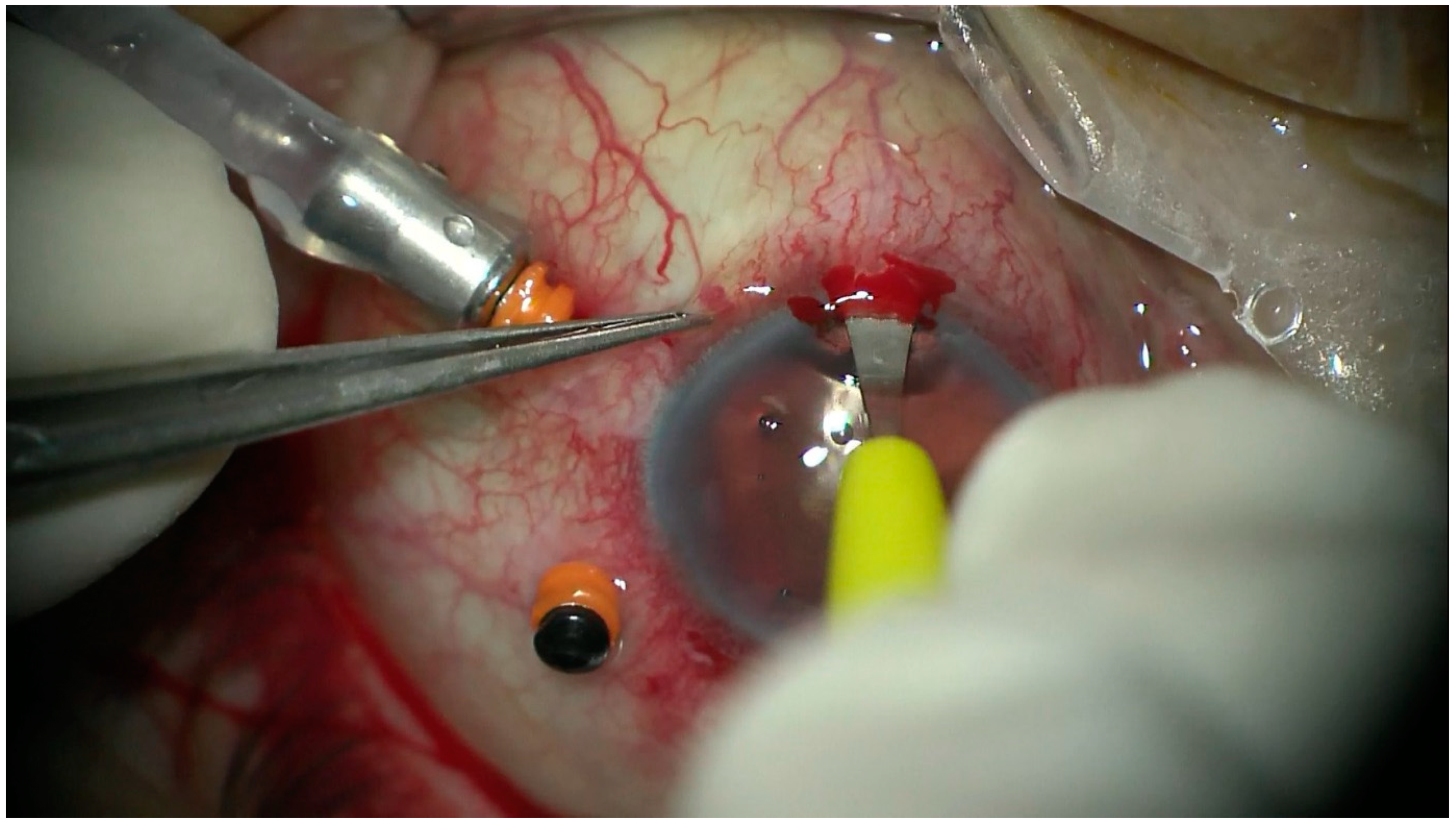
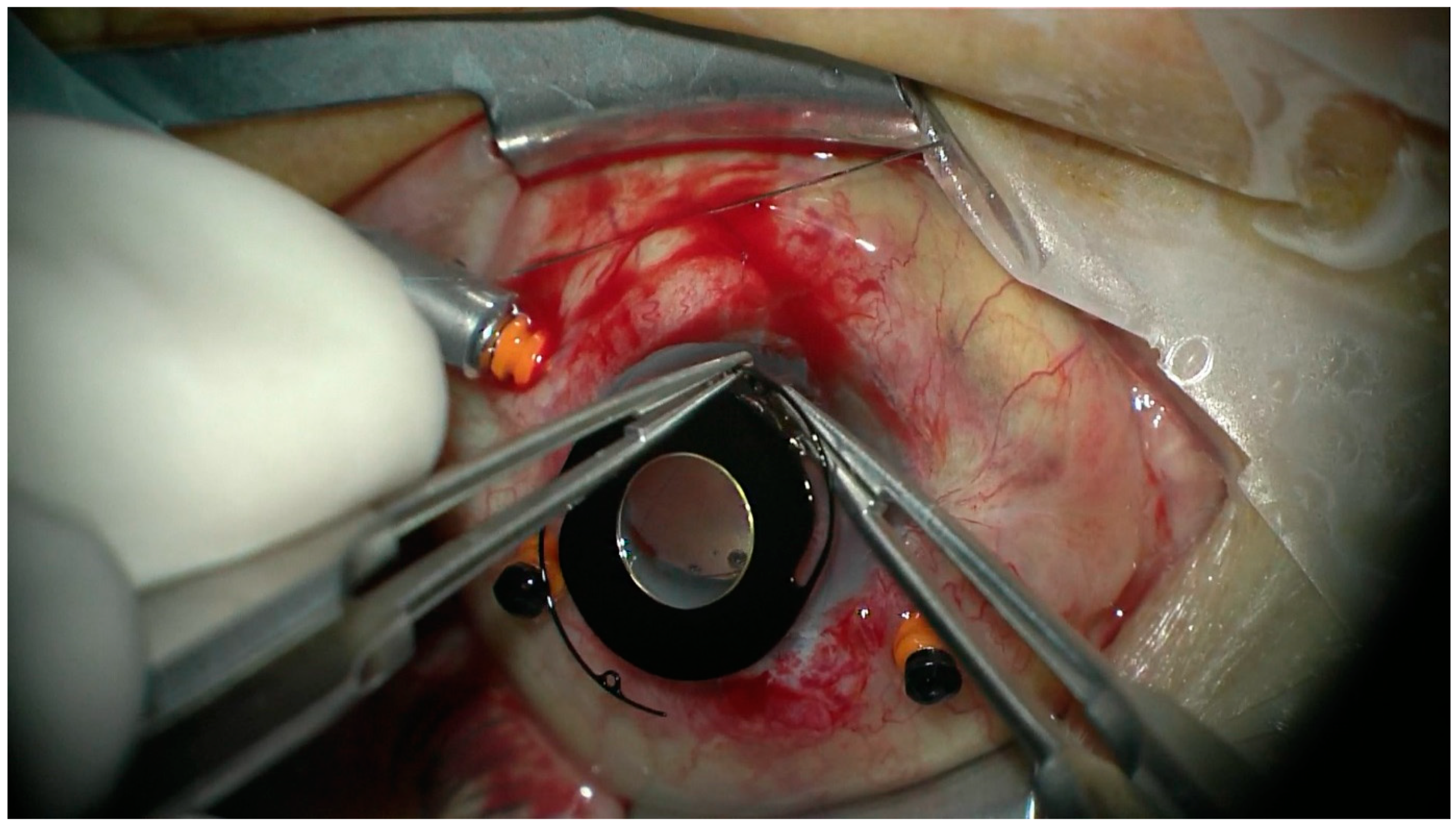
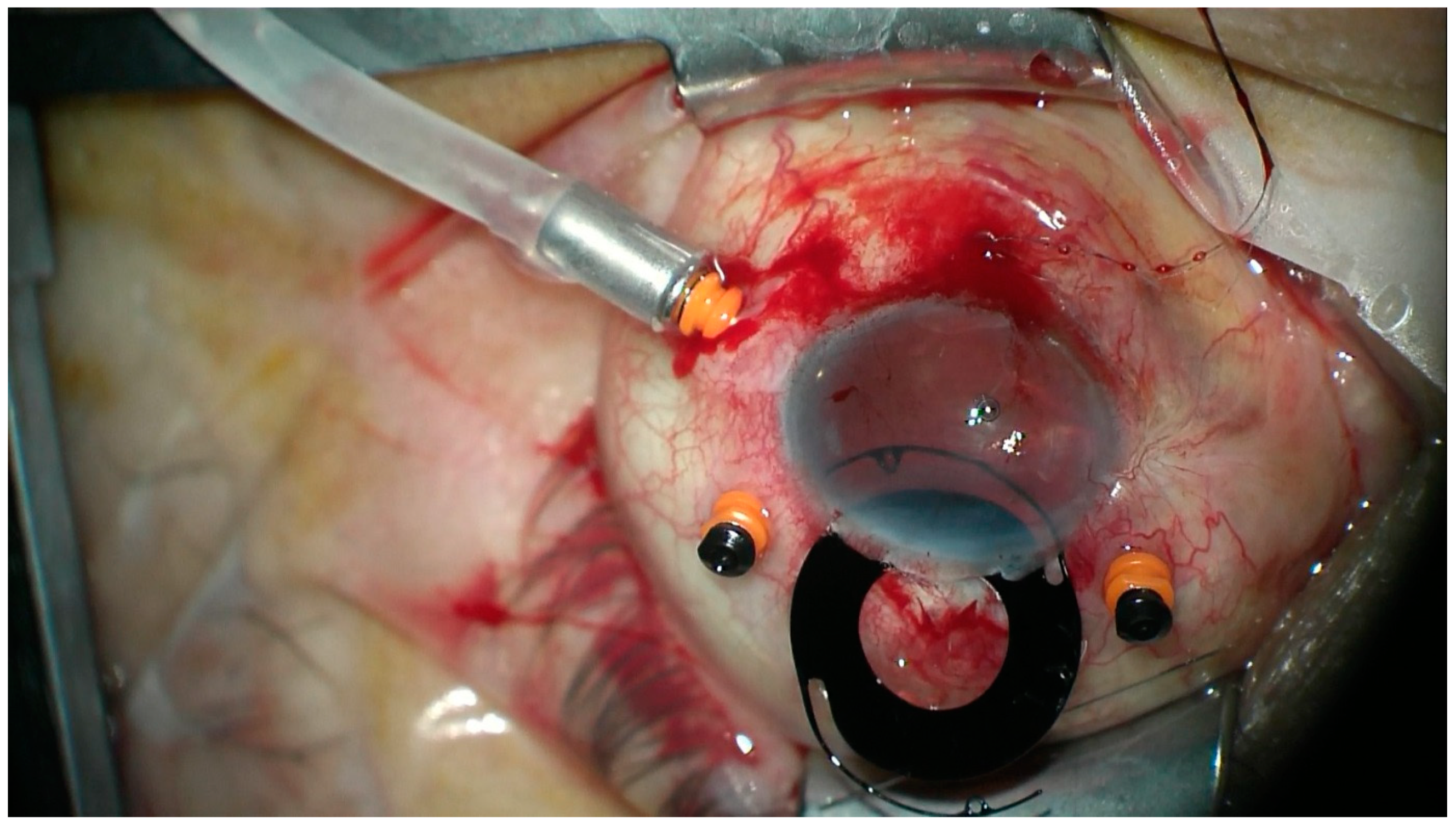
2.2. Surgical Technique
2.3. Patient and Public Involvement
3. Results
4. Discussion
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Kuhn, F.; Morris, R.; Witherspoon, C.D.; Heimann, K.; Jeffers, J.B.; Treister, G. A standardized classification of ocular trauma. Ophthalmology 1996, 103, 240–243. [Google Scholar] [CrossRef]
- Viestenz, A.; Küchle, M. Retrospective analysis of 417 cases of contusion and rupture of the globe with frequent avoidable causes of trauma: The Erlangen Ocular Contusion-Registry (EOCR) 1985–1995. Klin. Monbl. Augenheilkd. 2001, 218, 662–669. [Google Scholar] [CrossRef] [PubMed]
- Weissbart, S.B.; Ayres, B.D. Managment of aniridia and iris defects; an update of iris protesis options. Curr. Opin. Opththalmol. 2016, 27, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Narang, P.; Agraval, A. Single-pass four-throw technique for pupilloplasty. Eur. J. Ophthalmol. 2017, 27, 506–508. [Google Scholar] [CrossRef] [PubMed]
- Sundmacher, R.; Reinhard, T.; Althaus, C. Black-diaphragm intraocular lens for correction of aniridia. Ophthalmic Surg. 1994, 25, 180–185. [Google Scholar] [PubMed]
- Sundmacher, T.; Reinhard, T.; Althaus, C. Black diaphragm intraocular lens in congenital aniridia. Ger. J. Ophthalmol. 1994, 3, 197–201. [Google Scholar] [PubMed]
- Reinhard, T.; Sundmacher, R.; Althaus, C. Irisblenden-IOL bei Traumatischer Aniridie. Klein. Monbl. Augenheilkd. 1994, 205, 196–200. [Google Scholar] [CrossRef] [PubMed]
- Beltrame, G.; Salvetat, M.L.; Chizzolini, M.; Driussi, G.B.; Busatto, P.; di Giorgio, G.; Barosco, F.; Scuderi, B. Implantation of a black diaphragm intraocular lens in ten cases of post-traumatic aniridia. Eur. J. Ophthalmol. 2003, 13, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Dong, X.; Xu, H.; Yu, B.; Ying, L.; Xie, L. Long-term outcome of black diaphragm intraocular lens implantation in traumatic aniridia. Br. J. Ophthalmol. 2010, 94, 456–459. [Google Scholar] [CrossRef] [PubMed]
- Omulecki, W.; Synder, A. Parsplana vitrectomy and transscleral fixation of black diaphragm intraocular lens for the management of traumatic aniridia. Ophthalmic Surg. Lasers 2002, 33, 357–361. [Google Scholar] [PubMed]
- Lanzagorta-Aresti, A.; Menezo-Rozalen, J.L.; Martinez-Costa, R.; Cisneros-Lanuza, A. Ahmed valve for elevated intraocular pressure associated with black diaphragm lenses for aniridia. Eur. J. Ophthalmol. 2007, 17, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Qiu, X.; Ji, Y.; Zheng, T.; Lu, Y. Long-term efficacy and complications of black diaphragm intraocular lens implantation in patients with traumatic aniridia. Br. J. Ophthalmol. 2015, 99, 659–664. [Google Scholar] [CrossRef] [PubMed]
- Moghimi, S.; Riazi, E.M.; Maghsoudipour, M. Visual function after implantation of aniridia intraocular lens for traumatic aniridia in vitrectomized eye. Eur. J. Ophthalmol. 2007, 17, 660–665. [Google Scholar] [CrossRef] [PubMed]
- Aslam, S.A.; Wong, S.C.; Ficker, L.A.; MacLaren, R.E. Implantation of the black diaphragm intraocular lens in congenital and traumatic aniridia. Ophthalmology 2008, 115, 1705–1712. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Yuan, G.; Ying, L.; Yu, B.; Dong, X. Modified implantation of black diaphragm intraocular lens in traumatic aniridia. J. Cataract Refract. Surg. 2013, 39, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Qiu, X.; Ji, Y.; Zheng, T.; Lu, Y. The efficacy and complications of black diaphragm intra-ocular lens implantation in patients with congenital aniridia. Acta Ophthalmol. 2016, 94, 340–344. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | Gender | Age | Follow Up Period (Months) | Initial BCVA | Final BCVA | Final IOP (mmHg) | Ocular Comorbidities | Surgical Procedure | Type of BD IOL | Postoperative Complications | Secondary Interventions |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | male | 57 | 14 | light perception | counting fingers | 4 | retinal detachment, vitreous haemorrhage | BD IOL scleral fixation + PPV + silicone oil | 68 | silicone oil in the anterior chamber, hypotony | None |
| 2 | male | 49 | 13 | no light perception | light perception | 5 | retinal detachment | BD IOL scleral fixation + PPV + silicone oil | 67 L | silicone oil in the anterior chamber, hypotony | None |
| 3 | male | 31 | 13 | light perception | light perception | 22 | corneal scar | BD IOL scleral fixation + anterior vitrectomy | 67 G | corneal eodema, glaucoma | None |
| 4 | male | 30 | 24 | temporal light perception | counting fingers | 18 | retinal detachment, vitreous haemorrhage, corneal scar | BD IOL scleral fixation + PPV + silicone oil | 76 L | corneal scar, silicon oil in anterior chamber, BD IOL opacity | None |
| 5 | male | 43 | 24 | light perception | counting fingers | 15 | retinal detachment, vitreous haemorrhage, corneal scar, glaucoma | BD IOL scleral fixation + PPV + silicone oil | 67 L | corneal edema, glaucoma | PKP + PPV + silicone oil exchange; Ahmed valve implantation |
| 6 | male | 25 | 32 | hand movement | light perception without localization | 6 | retinal detachment, vitreous hemorrhage, corneal scar | BD IOL scleral fixation + PPV + silicone oil | 67 G | Hypotony | PPV + silicone oil exchange × 2 |
| 7 | female | 35 | 61 | counting fingers | light perception | 12 | corneal scar | PKP + PC IOL removal + BD IOL scleral fixation + PKP | 67 F | glaucoma, corneal opacity | None |
| 8 | male | 43 | 49 | hand movement | hand movement | 18 | corneal opacity, glaucoma | PKP + BD IOL scleral fixation + anterior vitrectomy + PKP | 67 G | graft disease, glaucoma | Ahmed valve implantation |
| 9 | female | 49 | 21 | hand movement | counting fingers | 5 | vitreous hemorrhage, corneal scar, post traumatic cataract, macular scar | BD IOL scleral fixation + anterior vitrectomy + | 67 G | corneal graft opacity, hypotony | PKP |
| 10 | male | 43 | 30 | 0.1 | 0.1 | 12 | corneal scar | BD IOL scleral fixation + anterior vitrectomy | 76 G | non | None |
| 11 | male | 50 | 12 | hand movement | hand movement | 14 | retinal detachment, strabismus | BD IOL scleral fixation + PPV + silicone oil | 67 G | none | None |
| 12 | male | 41 | 55 | 0.2 | 0.5 | 19 | corneal scar, post traumatic cataract | BD IOL scleral fixation + anterior vitrectomy | 67 G | BDI IOL subluxation, glaucoma | BD IOL repositioning |
| 13 | male | 26 | 42 | 0.02 | 0.02 | 18 | retinal detachment, corneal scar | BD IOL scleral fixation + PPV + C3F8 | 67 G | glaucoma, corneal opacity | Ahmed valve implantation |
| 14 | male | 79 | 120 | 0.2 | 0.2 | 18 | corneal scar | BD IOL scleral fixation + anterior vitrectomy | 67 G | none | None |
| Gender | Age | BCVA | BCVA Change (Patients) | Final IOP (mmHg) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | Min. | Mean | Max. | Initial | Final | Deterioration | No Change | Improvement | Min. | Mean | Max. | ||
| 12 | 2 | 25 | 43 | 79 | Min. | Max. | Min. | Max. | 2 | 6 | 6 | 4 | 13.3 | 22 |
| no light perception | 0.2 | light perception | 0.5 | |||||||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chorągiewicz, T.; Nowomiejska, K.; Haszcz, D.; Nowakowska, D.; Avitabile, T.; Reibaldi, M.; Jünemann, A.G.M.; Toro, M.D.; Rejdak, R. Transscleral Fixation of Black Diaphragm Intraocular Lens in Complete Aniridia and Aphakia Due to Posttraumatic Eye Rupture: A Pilot Study. J. Clin. Med. 2019, 8, 46. https://doi.org/10.3390/jcm8010046
Chorągiewicz T, Nowomiejska K, Haszcz D, Nowakowska D, Avitabile T, Reibaldi M, Jünemann AGM, Toro MD, Rejdak R. Transscleral Fixation of Black Diaphragm Intraocular Lens in Complete Aniridia and Aphakia Due to Posttraumatic Eye Rupture: A Pilot Study. Journal of Clinical Medicine. 2019; 8(1):46. https://doi.org/10.3390/jcm8010046
Chicago/Turabian StyleChorągiewicz, Tomasz, Katarzyna Nowomiejska, Dariusz Haszcz, Dominika Nowakowska, Teresio Avitabile, Michele Reibaldi, Anselm Gerhard Maria Jünemann, Mario Damiano Toro, and Robert Rejdak. 2019. "Transscleral Fixation of Black Diaphragm Intraocular Lens in Complete Aniridia and Aphakia Due to Posttraumatic Eye Rupture: A Pilot Study" Journal of Clinical Medicine 8, no. 1: 46. https://doi.org/10.3390/jcm8010046
APA StyleChorągiewicz, T., Nowomiejska, K., Haszcz, D., Nowakowska, D., Avitabile, T., Reibaldi, M., Jünemann, A. G. M., Toro, M. D., & Rejdak, R. (2019). Transscleral Fixation of Black Diaphragm Intraocular Lens in Complete Aniridia and Aphakia Due to Posttraumatic Eye Rupture: A Pilot Study. Journal of Clinical Medicine, 8(1), 46. https://doi.org/10.3390/jcm8010046