Relative Dose Intensity of Induction-Phase Pazopanib Treatment of Soft Tissue Sarcoma: Its Relationship with Prognoses of Pazopanib Responders

 , and
, and
Abstract
:1. Introduction
2. Material and Methods
2.1. Patients and Treatments
2.2. Analyses
3. Results
3.1. Enrolled Patients in the Analyses
3.2. Relative Dose Intensity (RDI) of Pazopanib
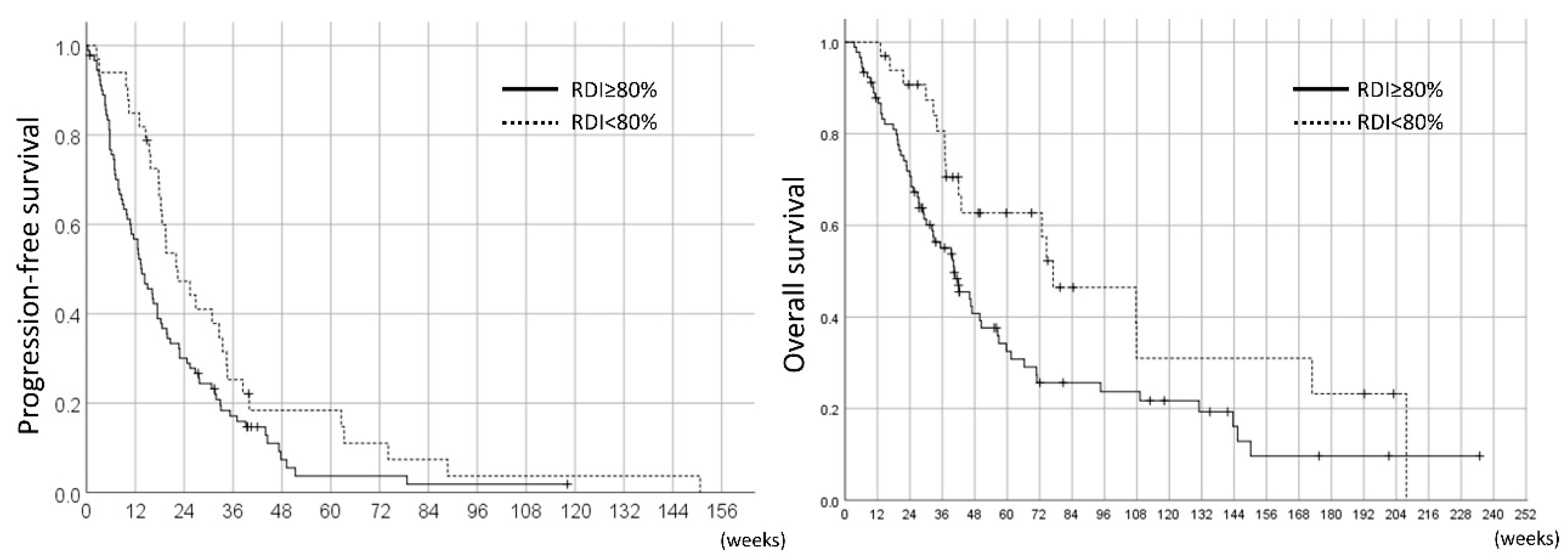
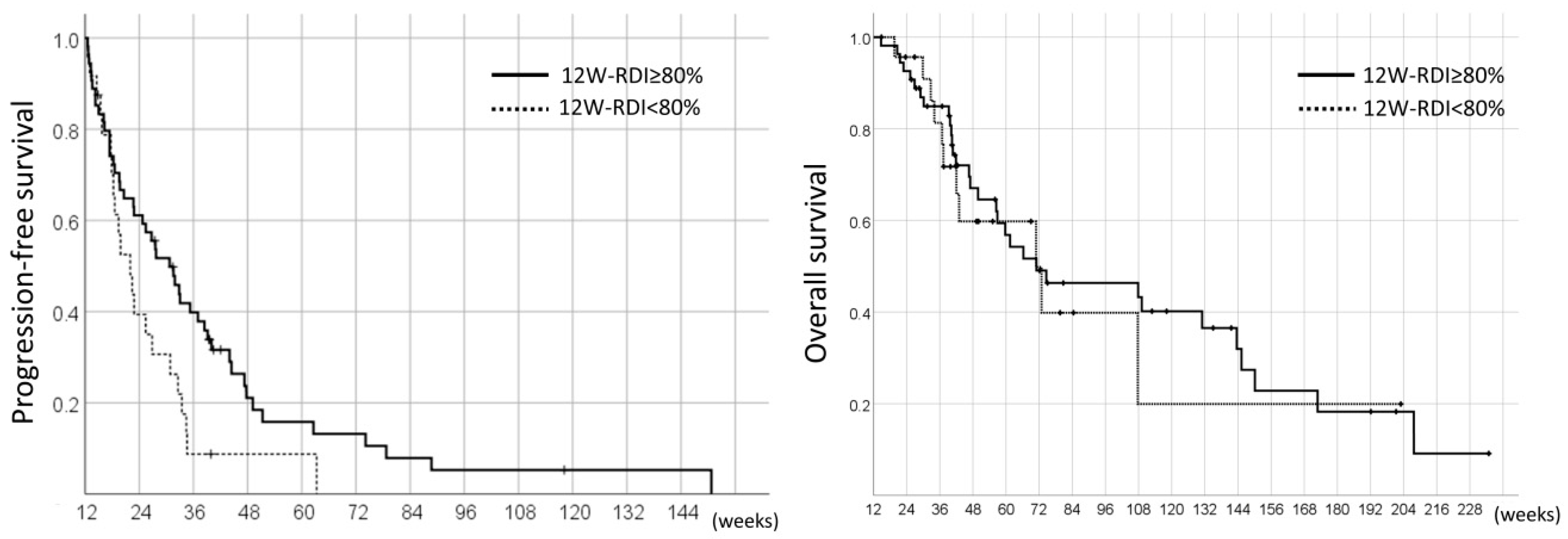
3.3. The Prognoses of the Pazopanib Responders
3.4. Adverse Events Observed in Pazopanib Responders
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hamberg, P.; Verweij, J.; Sleijfer, S. (Pre-)clinical pharmacology and activity of pazopanib, a novel multikinase angiogenesis inhibitor. Oncologist 2010, 15, 539–547. [Google Scholar] [CrossRef] [PubMed]
- Van der Graaf, W.T.; Blay, J.Y.; Chawla, S.P.; Kim, D.W.; Bui-Nguyen, B.; Casali, P.G.; Schöffski, P.; Aglietta, M.; Staddon, A.P.; Beppu, Y.; et al. Pazopanib for metastatic soft-tissue sarcoma (PALETTE): A randomised, double-blind, placebo-controlled phase 3 trial. Lancet 2012, 379, 1879–1886. [Google Scholar] [CrossRef]
- Hurwitz, H.I.; Dowlati, A.; Saini, S.; Savage, S.; Suttle, A.B.; Gibson, D.M.; Hodge, J.P.; Merkle, E.M.; Pandite, L. Phase I trial of pazopanib in patients with advanced cancer. Clin. Cancer Res. 2009, 15, 4220–4227. [Google Scholar] [CrossRef] [PubMed]
- Kasper, B.; Sleijfer, S.; Litière, S.; Marreaud, S.; Verweij, J.; Hodge, R.A.; Bauer, S.; Kerst, J.M.; van der Graaf, W.T. Long-term responders and survivors on pazopanib for advanced soft tissue sarcomas: Subanalysis of two European Organisation for Research and Treatment of Cancer (EORTC) clinical trials 62043 and 62072. Ann. Oncol. 2014, 25, 719–724. [Google Scholar] [CrossRef]
- Abe, K.; Yamamoto, N.; Hayashi, K.; Takeuchi, A.; Miwa, S.; Inatani, H.; Higuchi, T.; Taniguchi, Y.; Tsuchiya, H. Balancing prolonged survival with QoL using low-dose pazopanib maintenance: A comparison with the PALETTE Study. Anticancer Res. 2016, 36, 2893–2897. [Google Scholar] [PubMed]
- Sternberg, C.N.; Davis, I.D.; Mardiak, J.; Szczylik, C.; Lee, E.; Wagstaff, J.; Barrios, C.H.; Salman, P.; Gladkov, O.A.; Kavina, A.; et al. Pazopanib in locally advanced or metastatic renal cell carcinoma: Results of a randomized phase III trial. J. Clin. Oncol. 2010, 28, 1061–1068. [Google Scholar] [CrossRef]
- Motzer, R.J.; Hutson, T.E.; Cella, D.; Reeves, J.; Hawkins, R.; Guo, J.; Nathan, P.; Staehler, M.; de Souza, P.; Merchan, J.R.; et al. Pazopanib versus sunitinib in metastatic renal-cell carcinoma. N. Engl. J. Med. 2013, 369, 722–731. [Google Scholar] [CrossRef]
- Suttle, A.B.; Ball, H.A.; Molimard, M.; Hutson, T.E.; Carpenter, C.; Rajagopalan, D.; Lin, Y.; Swann, S.; Amado, R.; Pandite, L. Relationships between pazopanib exposure and clinical safety and efficacy in patients with advanced renal cell carcinoma. Br. J. Cancer 2014, 111, 1909–1916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verheijen, R.B.; Swart, L.E.; Beijnen, J.H.; Schellens, J.H.M.; Huitema, A.D.R.; Steeghs, N. Exposure-survival analyses of pazopanib in renal cell carcinoma and soft tissue sarcoma patients: Opportunities for dose optimization. Cancer Chemother. Pharmacol. 2017, 80, 1171–1178. [Google Scholar] [CrossRef]
- Fletcher, C.D.M.; Bridge, J.A.; Hogendoorn, P.C.W.; Mertens, F. WHO Classification of Tumours of Soft Tissue and Bone, 4th ed.; International Agency Research on Cancer: Lyon, France, 2013; ISBN 978-92-832-2434-1. [Google Scholar]
- Sleijfer, S.; Ray-Coquard, I.; Papai, Z.; Le Cesne, A.; Scurr, M.; Schöffski, P.; Collin, F.; Pandite, L.; Marreaud, S.; De Brauwer, A.; et al. Pazopanib, a multikinase angiogenesis inhibitor, in patients with relapsed or refractory advanced soft tissue sarcoma: A phase II study from the European Organisation for Research and Treatment of Cancer-soft Tissue and Bone Sarcoma group (EORTC study 62043). J. Clin. Oncol. 2009, 27, 3126–3132. [Google Scholar] [CrossRef]
- Van Glabbeke, M.; Verweij, J.; Judson, I.; Nielsen, O.S.; EORTC Soft Tissue and Bone Sarcoma Group. Progression-free rate as the principal end-point for phase II trials in soft-tissue sarcomas. Eur. J. Cancer 2002, 38, 543–549. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef]
- Hughes, T.P.; Branford, S.; White, D.L.; Reynolds, J.; Koelmeyer, R.; Seymour, J.F.; Taylor, K.; Arthur, C.; Schwarer, A.; Morton, J.; et al. Impact of early dose intensity on cytogenetic and molecular responses in chronic-phase CML patients receiving 600 mg/day of imatinib as initial therapy. Blood 2008, 112, 3965–3973. [Google Scholar] [CrossRef] [PubMed]
- Santos, F.P.; Kantarjian, H.; Fava, C.; O’Brien, S.; Garcia-Manero, G.; Ravandi, F.; Wierda, W.; Thomas, D.; Shan, J.; Cortes, J. Clinical impact of dose reductions and interruptions of second-generation tyrosine kinase inhibitors in patients with chronic myeloid leukaemia. Br. J. Haematol. 2010, 150, 303–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porta, C.; Levy, A.; Hawkins, R.; Castellano, D.; Bellmunt, J.; Nathan, P.; McDermott, R.; Wagstaff, J.; Donnellan, P.; McCaffrey, J.; et al. Impact of adverse events, treatment modifications, and dose intensity on survival among patients with advanced renal cell carcinoma treated with first-line sunitinib: A medical chart review across ten centers in five European countries. Cancer Med. 2014, 3, 1517–1526. [Google Scholar] [CrossRef]
- Komatsu, Y.; Ohki, E.; Ueno, N.; Yoshida, A.; Toyoshima, Y.; Ueda, E.; Houzawa, H.; Togo, K.; Nishida, T. Safety, efficacy and prognostic analyses of sunitinib in the post-marketing surveillance study of Japanese patients with gastrointestinal stromal tumor. Jpn. J. Clin. Oncol. 2015, 45, 1016–1022. [Google Scholar] [CrossRef] [Green Version]
- Ishihara, H.; Takagi, T.; Kondo, T.; Iwamoto, K.; Tachibana, H.; Yoshida, K.; Omae, K.; Iizuka, J.; Kobayashi, H.; Tanabe, K. Decreased relative dose intensity during the early phase of treatment impacts the therapeutic efficacy of sunitinib in metastatic renal cell carcinoma. Jpn. J. Clin. Oncol. 2018, 48, 667–672. [Google Scholar] [CrossRef]
- Kawashima, A.; Takayama, H.; Arai, Y.; Tanigawa, G.; Nin, M.; Kajikawa, J.; Imazu, T.; Kinoshita, T.; Yasunaga, Y.; Inoue, H.; et al. One-month relative dose intensity of not less than 50% predicts favourable progression-free survival in sorafenib therapy for advanced renal cell carcinoma in Japanese patients. Eur. J. Cancer 2011, 47, 1521–1526. [Google Scholar] [CrossRef]
- Nakamura, T.; Matsumine, A.; Kawai, A.; Araki, N.; Goto, T.; Yonemoto, T.; Sugiura, H.; Nishida, Y.; Hiraga, H.; Honoki, K.; et al. The clinical outcome of pazopanib treatment in Japanese patients with relapsed soft tissue sarcoma: A Japanese Musculoskeletal Oncology Group (JMOG) study. Cancer 2016, 122, 1408–1416. [Google Scholar] [CrossRef] [Green Version]
- Gelderblom, H.; Judson, I.R.; Benson, C.; Merimsky, O.; Grignani, G.; Katz, D.; Freivogel, K.W.; Stein, D.; Jobanputra, M.; Mungul, A.; et al. Treatment patterns and clinical outcomes with pazopanib in patients with advanced soft tissue sarcomas in a compassionate use setting: Results of the SPIRE study. Acta Oncol. 2017, 56, 1769–1775. [Google Scholar] [CrossRef]
- Motzer, R.J.; Haas, N.B.; Donskov, F.; Gross-Goupil, M.; Varlamov, S.; Kopyltsov, E.; Lee, J.L.; Melichar, B.; Rini, B.I.; Choueiri, T.K.; et al. Randomized phase III trial of adjuvant pazopanib versus placebo after nephrectomy in patients with localized or locally advanced renal cell carcinoma. J. Clin. Oncol. 2017, 35, 3916–3923. [Google Scholar] [CrossRef] [PubMed]
- Grassi, P.; Verzoni, E.; Ratta, R.; Porcu, L.; Prisciandaro, M.; Mennitto, A.; Calareso, G.; de Braud, F.; Procopio, G. Does dose modification affect efficacy of first-line pazopanib in metastatic renal cell carcinoma? Drugs RD 2017, 17, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Sternberg, C.N.; Donskov, F.; Haas, N.B.; Doehn, C.; Russo, P.; Elmeliegy, M.; Baneyx, G.; Banerjee, H.; Aimone, P.; Motzer, R.J. Pazopanib exposure relationship with clinical efficacy and safety in the adjuvant treatment of advanced renal cell carcinoma. Clin. Cancer Res. 2018, 24, 3005–3013. [Google Scholar] [CrossRef] [PubMed]
- Koehler, K.; Liebner, D.; Chen, J.L. TP53 mutational status is predictive of pazopanib response in advanced sarcomas. Ann. Oncol. 2016, 27, 539–543. [Google Scholar] [CrossRef] [PubMed]
- Powles, T.; Bracarda, S.; Chen, M.; Norry, E.; Compton, N.; Heise, M.; Hutson, T.; Harter, P.; Carpenter, C.; Pandite, L.; et al. Characterisation of liver chemistry abnormalities associated with pazopanib monotherapy: A systematic review and meta-analysis of clinical trials in advanced cancer patients. Eur. J. Cancer 2015, 51, 1293–1302. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.F.; Reck, B.H.; Xue, Z.; Huang, L.; Baker, K.L.; Chen, M.; Chen, E.P.; Ellens, H.E.; Mooser, V.E.; Cardon, L.R.; et al. Pazopanib-induced hyperbilirubinemia is associated with Gilbert’s syndrome UGT1A1 polymorphism. Br. J. Cancer 2010, 102, 1371–1377. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Johnson, T.; Choueiri, T.K.; Deen, K.C.; Xue, Z.; Pandite, L.N.; Carpenter, C.; Xu, C.F. Hyperbilirubinemia in pazopanib- or sunitinib-treated patients in COMPARZ is associated with UGT1A1 polymorphisms. Ann. Oncol. 2013, 24, 2927–2928. [Google Scholar] [CrossRef]
- Evaluation of Genomic Applications in Practice and Prevention (EGAPP) Working Group. Recommendations from the EGAPP Working Group: Can UGT1A1 genotyping reduce morbidity and mortality in patients with metastatic colorectal cancer treated with irinotecan? Genet. Med. 2009, 11, 15–20. [Google Scholar] [CrossRef]
- Palomaki, G.E.; Bradley, L.A.; Douglas, M.P.; Kolor, K.; Dotson, W.D. Can UGT1A1 genotyping reduce morbidity and mortality in patients with metastatic colorectal cancer treated with irinotecan? An evidence-based review. Genet. Med. 2009, 11, 21–34. [Google Scholar] [CrossRef] [Green Version]
- Coens, C.; van der Graaf, W.T.; Blay, J.Y.; Chawla, S.P.; Judson, I.; Sanfilippo, R.; Manson, S.C.; Hodge, R.A.; Marreaud, S.; Prins, J.B.; et al. Health-related quality-of-life results from PALETTE: A randomized, double-blind, phase 3 trial of pazopanib versus placebo in patients with soft tissue sarcoma whose disease has progressed during or after prior chemotherapy-a European Organization for research and treatment of cancer soft tissue and bone sarcoma group global network study (EORTC 62072). Cancer 2015, 121, 2933–2941. [Google Scholar] [CrossRef]
- De Wit, D.; van Erp, N.P.; den Hartigh, J.; Wolterbeek, R.; den Hollander-van Deursen, M.; Labots, M.; Guchelaar, H.J.; Verheul, H.M.; Gelderblom, H. Therapeutic drug monitoring to individualize the dosing of pazopanib: A pharmacokinetic feasibility study. Ther. Drug Monit. 2015, 37, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Verheijen, R.B.; Bins, S.; Mathijssen, R.H.; Lolkema, M.P.; van Doorn, L.; Schellens, J.H.; Beijnen, J.H.; Langenberg, M.H.; Huitema, A.D.; Steeghs, N.; et al. Individualized pazopanib dosing: A prospective feasibility study in cancer patients. Clin. Cancer Res. 2016, 22, 5738–5746. [Google Scholar] [CrossRef] [PubMed]
- Verheijen, R.B.; Beijnen, J.H.; Schellens, J.H.M.; Huitema, A.D.R.; Steeghs, N. Clinical pharmacokinetics and pharmacodynamics of pazopanib: Towards optimized dosing. Clin. Pharmacokinet. 2017, 56, 987–997. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | All STS Patients Treated with Pazopanib (n = 124) | Pazopanib Responders (n = 78) |
|---|---|---|
| Age, years; median (range) | 51 (19–85) | 56 (19–85) |
| Male | 57 (46%) | 34 (44%) |
| Female | 67 (54%) | 44 (56%) |
| ECOG PS: | ||
| 0 | 78 (63%) | 55 (71%) |
| 1 | 43 (35%) | 23 (29%) |
| 2 | 3 (2%) | 0 |
| Primary lesion: | ||
| Extremities | 43 (35%) | 30 (38%) |
| Non-extremities | 81 (65%) | 48 (62%) |
| Histology: | ||
| Leiomyosarcoma | 22 (18%) | 15 (19%) |
| Synovial sarcoma | 14 (11%) | 11 (14%) |
| Liposarcoma | 18 (15%) | 10 (13%) |
| Other sarcoma | 70 (56%) | 42 (54%) |
| Prior chemotherapy: | ||
| ≤1 regimen | 50 (40%) | 35 (45%) |
| ≥2 regimens | 74 (60%) | 43 (55%) |
| Adverse Events | 12W-RDI ≥ 80% (n = 54) | 12W-RDI < 80% (n = 24) | ||
|---|---|---|---|---|
| All-Grade | ≥ Grade 3 | All-Grade | ≥ Grade 3 | |
| Hematologic adverse events: | 45 (83%) | 12 (22%) | 20 (83%) | 7 (29%) |
| Leukocytopenia | 21 (39%) | 2 (4%) | 11 (46%) | 1 (4%) |
| Neutropenia | 25 (46%) | 4 (9%) | 11 (46%) | 3 (13%) |
| Lymphocytopenia | 19 (35%) | 8 (15%) | 12 (50%) | 3 (13%) |
| Anemia | 14 (26%) | 0 | 11 (46%) | 0 |
| Thrombocytopenia | 19 (35%) | 0 | 11 (46%) | 0 |
| Non-hematologic adverse events: | 54 (100%) | 12 (22%) | 24 (100%) | 11 (46%) |
| Diarrhea | 31 (57%) | 0 | 10 (42%) | 0 |
| Hypertension | 29 (54%) | 9 (17%) | 15 (63%) | 3 (13%) |
| Nausea/anorexia | 28 (52%) | 0 | 17 (31%) | 0 |
| Fatigue | 26 (48%) | 0 | 16 (67%) | 0 |
| Hand-foot-syndrome | 20 (37%) | 0 | 8 (33%) | 0 |
| Infection | 10 (19%) | 2 (4%) | 3 (13%) | 1 (4%) |
| Pneumothorax | 7 (13%) | 2 (4%) | 0 | 0 |
| Total bilirubin increase | 17 (31%) | 0 | 14 (58%) | 0 |
| AST/ALT increase | 40 (74%) | 1 (2%) | 21 (88%) | 8 (33%) |
| Serum creatinine increase | 9 (17%) | 0 | 7 (29%) | 1 (4%) |
| Electrolytes disorder 1 | 25 (46%) | 0 | 14 (58%) | 2 (8%) |
| Hypothyroidism | 30 (56%) | 0 | 10 (42%) | 0 |
| Other adverse events 2 | 37 (69%) | 4 (7%) | 15 (63%) | 1 (4%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakano, K.; Funauchi, Y.; Hayakawa, K.; Tanizawa, T.; Ae, K.; Matsumoto, S.; Takahashi, S. Relative Dose Intensity of Induction-Phase Pazopanib Treatment of Soft Tissue Sarcoma: Its Relationship with Prognoses of Pazopanib Responders. J. Clin. Med. 2019, 8, 60. https://doi.org/10.3390/jcm8010060
Nakano K, Funauchi Y, Hayakawa K, Tanizawa T, Ae K, Matsumoto S, Takahashi S. Relative Dose Intensity of Induction-Phase Pazopanib Treatment of Soft Tissue Sarcoma: Its Relationship with Prognoses of Pazopanib Responders. Journal of Clinical Medicine. 2019; 8(1):60. https://doi.org/10.3390/jcm8010060
Chicago/Turabian StyleNakano, Kenji, Yuki Funauchi, Keiko Hayakawa, Taisuke Tanizawa, Keisuke Ae, Seiichi Matsumoto, and Shunji Takahashi. 2019. "Relative Dose Intensity of Induction-Phase Pazopanib Treatment of Soft Tissue Sarcoma: Its Relationship with Prognoses of Pazopanib Responders" Journal of Clinical Medicine 8, no. 1: 60. https://doi.org/10.3390/jcm8010060
APA StyleNakano, K., Funauchi, Y., Hayakawa, K., Tanizawa, T., Ae, K., Matsumoto, S., & Takahashi, S. (2019). Relative Dose Intensity of Induction-Phase Pazopanib Treatment of Soft Tissue Sarcoma: Its Relationship with Prognoses of Pazopanib Responders. Journal of Clinical Medicine, 8(1), 60. https://doi.org/10.3390/jcm8010060