Acute Kidney Injury after Lung Transplantation: A Systematic Review and Meta-Analysis


 , , , , and
, , , , and 
Abstract
:1. Introduction
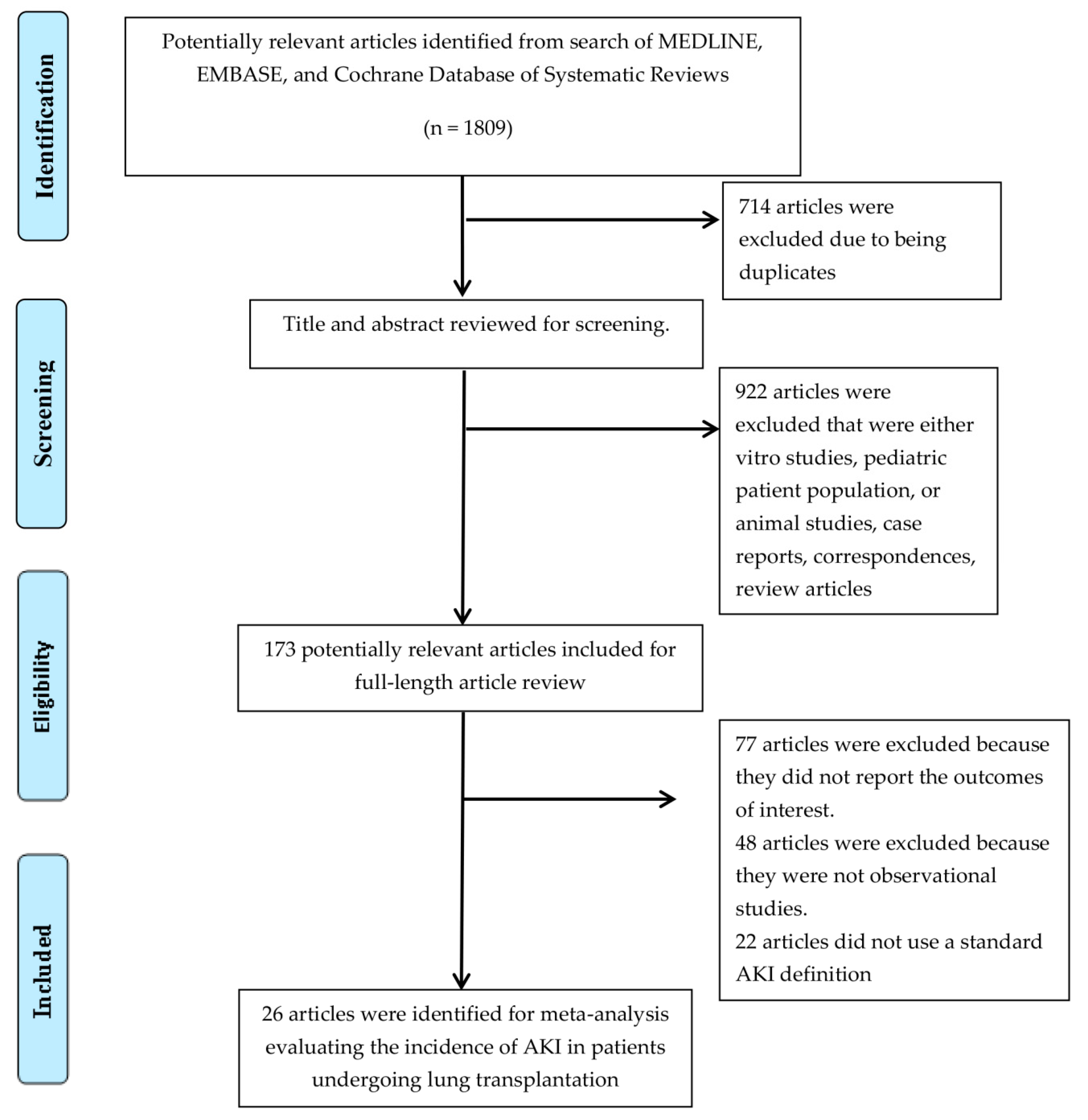
2. Methods
2.1. Information Sources and Search Strategy
2.2. Study Selection
2.3. Data Collection Process
2.4. Statistical Analysis
3. Results
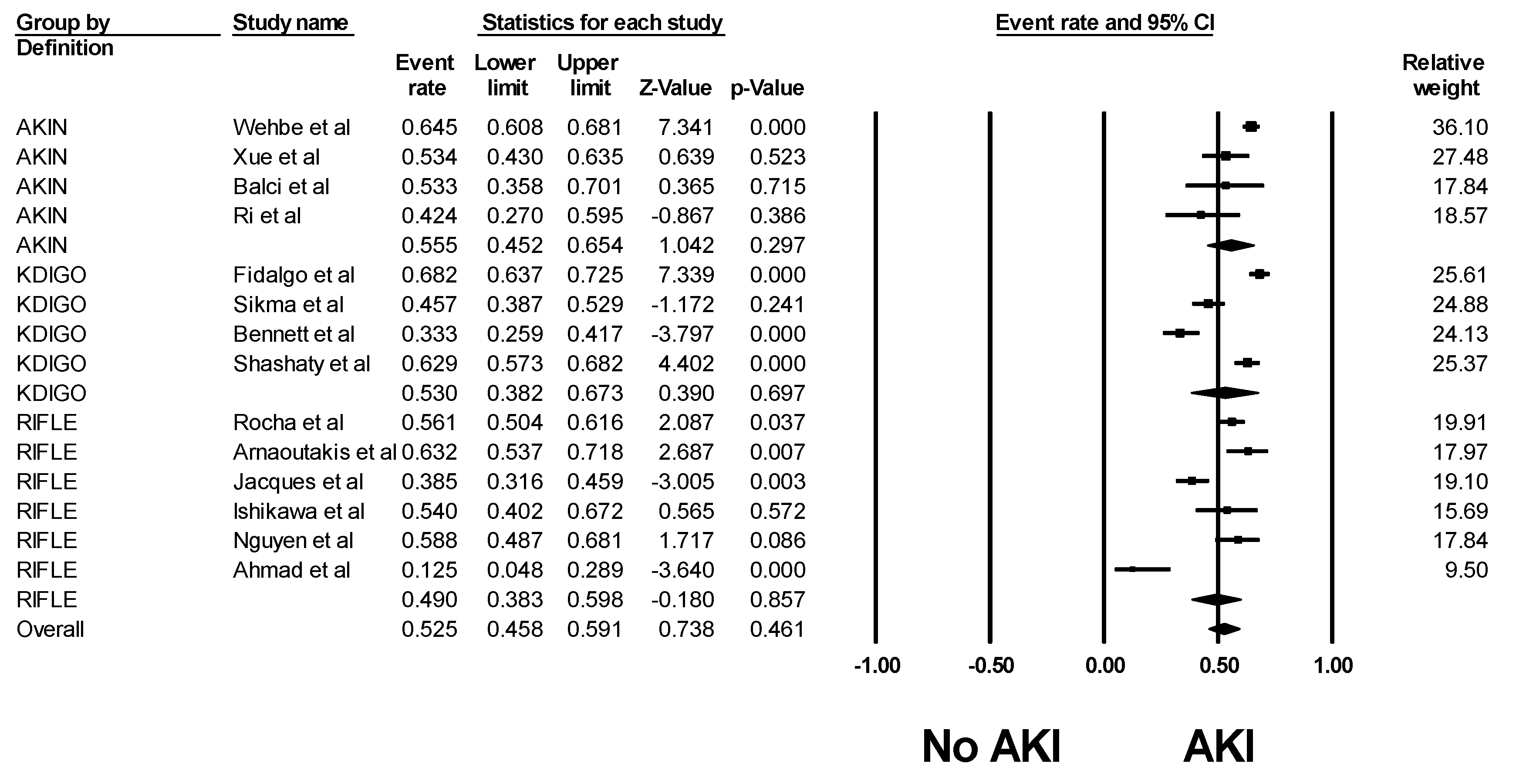
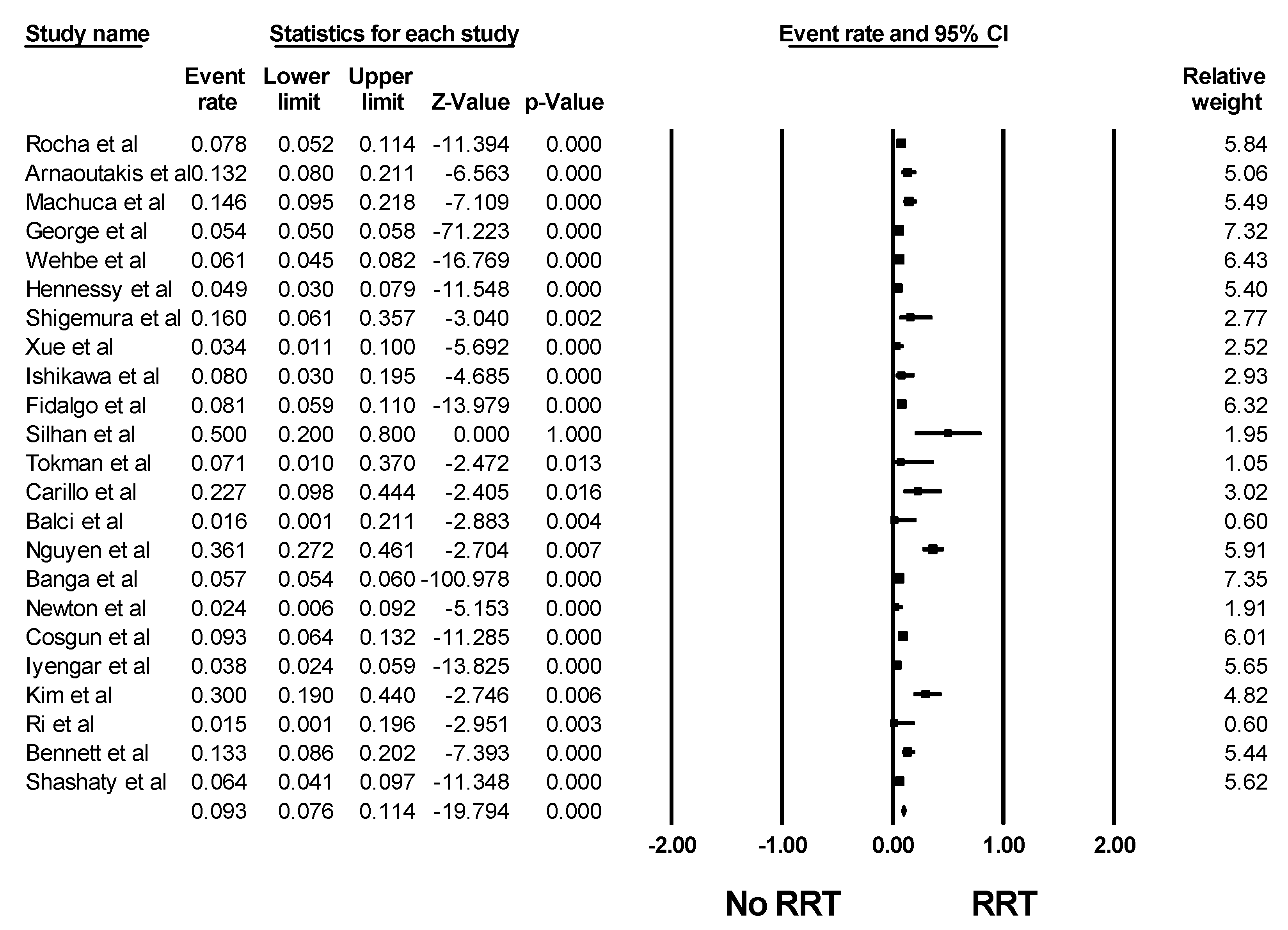
3.1. Incidence of Acute Kidney Injury among Patients after Lung Transplantation
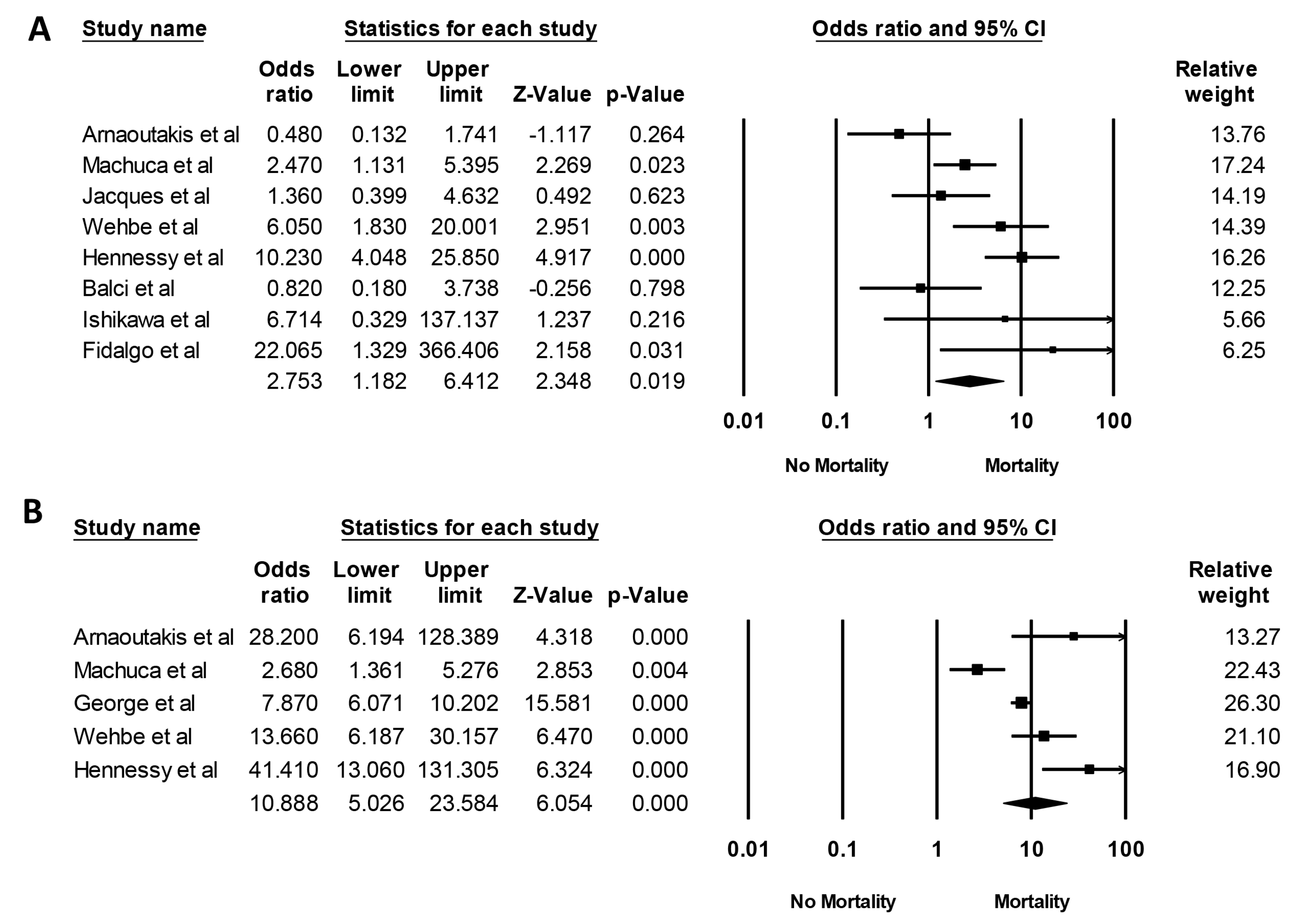
3.2. Mortality Risk of Acute Kidney Injury in Patients after Lung Transplantation
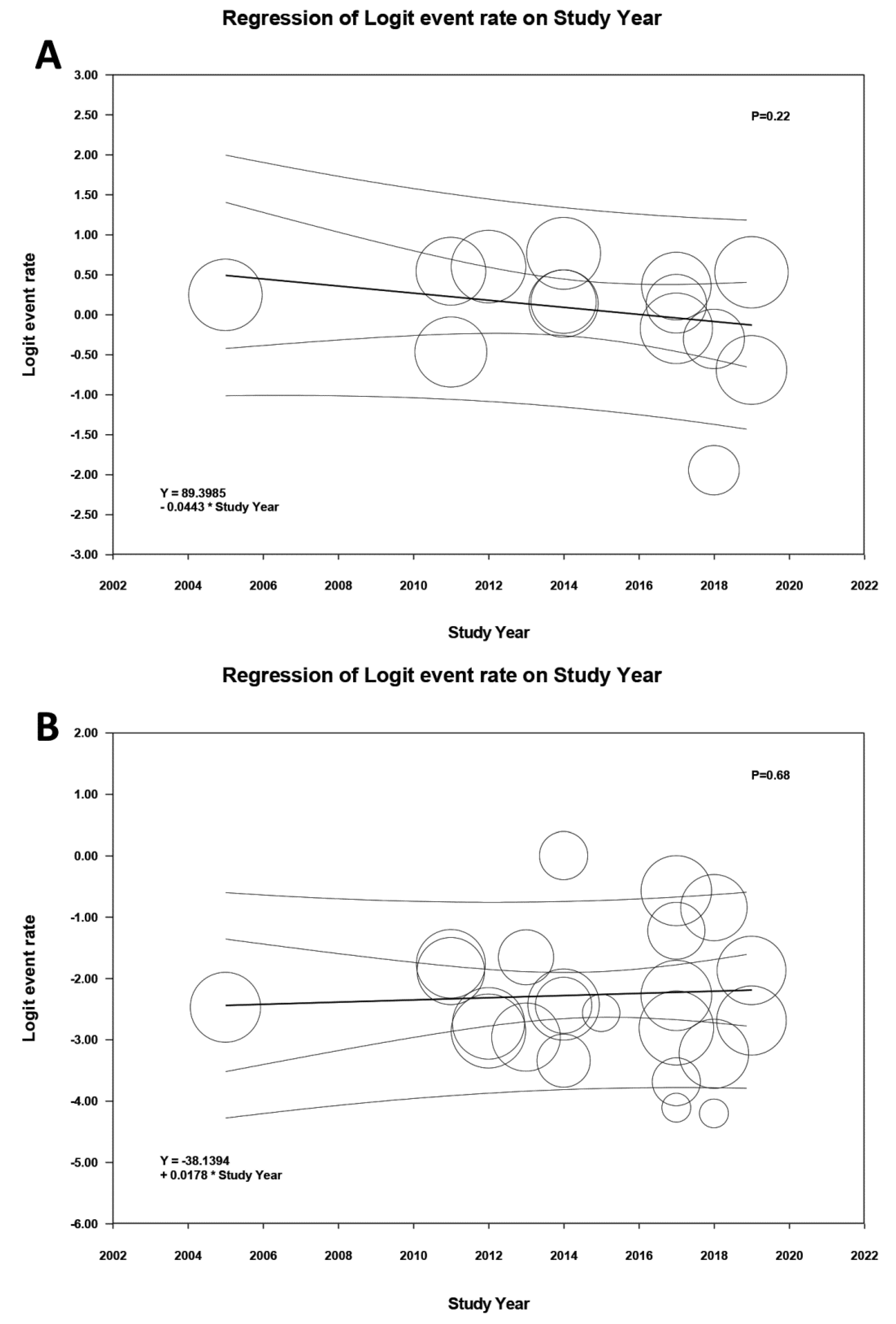
3.3. Evaluation for Publication Bias
4. Discussion and Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Gameiro, J.; Agapito Fonseca, J.; Jorge, S.; Lopes, J.A. Acute Kidney Injury Definition and Diagnosis: A Narrative Review. J. Clin. Med. 2018, 7, 307. [Google Scholar] [CrossRef] [PubMed]
- Thongprayoon, C.; Cheungpasitporn, W.; Mao, M.A.; Harrison, A.M.; Erickson, S.B. Elevated admission serum calcium phosphate product as an independent risk factor for acute kidney injury in hospitalized patients. Hosp Pract (1995) 2019, 47, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Thongprayoon, C.; Cheungpasitporn, W.; Mao, M.A.; Sakhuja, A.; Kashani, K. U-shape association of serum albumin level and acute kidney injury risk in hospitalized patients. PLoS ONE 2018, 13, e0199153. [Google Scholar] [CrossRef]
- Kashani, K.; Cheungpasitporn, W.; Ronco, C. Biomarkers of acute kidney injury: The pathway from discovery to clinical adoption. Clin. Chem. Lab. Med. 2017, 55, 1074–1089. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Fang, Y.; Teng, J.; Ding, X. Acute Kidney Injury Epidemiology: From Recognition to Intervention. Contrib. Nephrol. 2016, 187, 1–8. [Google Scholar] [PubMed]
- Negi, S.; Koreeda, D.; Kobayashi, S.; Yano, T.; Tatsuta, K.; Mima, T.; Shigematsu, T.; Ohya, M. Acute kidney injury: Epidemiology, outcomes, complications, and therapeutic strategies. Semin. Dial. 2018, 31, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Hoste, E.A.J.; Bagshaw, S.M.; Bellomo, R.; Cely, C.M.; Colman, R.; Cruz, D.N.; Edipidis, K.; Forni, L.G.; Gomersall, C.D.; Govil, D.; et al. Epidemiology of acute kidney injury in critically ill patients: The multinational AKI-EPI study. Intensiv. Care Med. 2015, 41, 1411–1423. [Google Scholar] [CrossRef]
- Cheungpasitporn, W.; Kashani, K. Electronic Data Systems and Acute Kidney Injury. Contrib. Nephrol. 2016, 187, 73–83. [Google Scholar]
- Sawhney, S.; Marks, A.; Fluck, N.; Levin, A.; McLernon, D.; Prescott, G.; Black, C. Post-discharge kidney function is associated with subsequent ten-year renal progression risk among survivors of acute kidney injury. Kidney Int. 2017, 92, 440–452. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, A.P.; Gabriel, R.A.; Golts, E.; Kistler, E.B.; Schmidt, U. Severity of Acute Kidney Injury in the Post-Lung Transplant Patient Is Associated with Higher Healthcare Resources and Cost. J. Cardiothorac. Vasc. Anesth. 2017, 31, 1361–1369. [Google Scholar] [CrossRef]
- Arnaoutakis, G.J.; George, T.J.; Robinson, C.W.; Gibbs, K.W.; Orens, J.B.; Merlo, C.A.; Shah, A.S. Severe acute kidney injury according to the RIFLE (risk, injury, failure, loss, end stage) criteria affects mortality in lung transplantation. J. Heart Lung Transplant. 2011, 30, 1161–1168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puttarajappa, C.M.; Bernardo, J.F.; Kellum, J.A. Renal Complications Following Lung Transplantation and Heart Transplantation. Crit. Care Clin. 2019, 35, 61–73. [Google Scholar] [CrossRef] [PubMed]
- Rocha, P.N.; Rocha, A.T.; Palmer, S.M.; Davis, R.D.; Smith, S.R. Acute renal failure after lung transplantation: Incidence, predictors and impact on perioperative morbidity and mortality. Am. J. Transplant. 2005, 5, 1469–1476. [Google Scholar] [CrossRef] [PubMed]
- Fidalgo, P.; Ahmed, M.; Meyer, S.R.; Lien, D.; Weinkauf, J.; Cardoso, F.S.; Jackson, K.; Bagshaw, S.M. Incidence and outcomes of acute kidney injury following orthotopic lung transplantation: A population-based cohort study. Nephrol. Dial. Transplant. 2014, 29, 1702–1709. [Google Scholar] [CrossRef]
- Fidalgo, P.; Ahmed, M.; Meyer, S.R.; Lien, D.; Weinkauf, J.; Kapasi, A.; Cardoso, F.S.; Jackson, K.; Bagshaw, S.M. Association between transient acute kidney injury and morbidity and mortality after lung transplantation: A retrospective cohort study. J. Crit. Care 2014, 29, 1028–1034. [Google Scholar] [CrossRef]
- Wehbe, E.; Duncan, A.E.; Dar, G.; Budev, M.; Stephany, B. Recovery from AKI and short- and long-term outcomes after lung transplantation. Clin. J. Am. Soc. Nephrol. 2013, 8, 19–25. [Google Scholar] [CrossRef]
- Chambers, D.C.; Yusen, R.D.; Cherikh, W.S.; Goldfarb, S.B.; Kucheryavaya, A.Y.; Khusch, K.; Levvey, B.J.; Lund, L.H.; Meiser, B.; Rossano, J.W.; et al. The Registry of the International Society for Heart and Lung Transplantation: Thirty-fourth Adult Lung and Heart-Lung Transplantation Report—2017; Focus Theme: Allograft ischemic time. J. Heart Lung Transplant. 2017, 36, 1047–1059. [Google Scholar] [CrossRef]
- Bloom, R.; Doyle, A. Kidney Disease after Heart and Lung Transplantation. Arab. Archaeol. Epigr. 2006, 6, 671–679. [Google Scholar] [CrossRef]
- George, T.J.; Arnaoutakis, G.J.; Beaty, C.A.; Pipeling, M.R.; Merlo, C.A.; Conte, J.V.; Shah, A.S. Acute kidney injury increases mortality after lung transplantation. Ann. Thorac. Surg. 2012, 94, 185–192. [Google Scholar] [CrossRef]
- Lafrance, J.P.; Miller, D.R. Acute kidney injury associates with increased long-term mortality. J. Am. Soc. Nephrol. JASN 2010, 21, 345–352. [Google Scholar] [CrossRef]
- Jacques, F.; El-Hamamsy, I.; Fortier, A.; Maltais, S.; Perrault, L.P.; Liberman, M.; Noiseux, N.; Ferraro, P. Acute renal failure following lung transplantation: Risk factors, mortality, and long-term consequences. Eur. J. Cardiothorac. Surg. 2012, 41, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Jardel, S.; Reynaud, Q.; Durieu, I. Long-term extrapulmonary comorbidities after lung transplantation in cystic fibrosis: Update of specificities. Clin. Transplant. 2018, 32, e13269. [Google Scholar] [CrossRef] [PubMed]
- Yusen, R.D.; Edwards, L.B.; Kucheryavaya, A.Y.; Benden, C.; Dipchand, A.I.; Goldfarb, S.B.; Levvey, B.J.; Lund, L.H.; Meiser, B.; Rossano, J.W.; et al. The Registry of the International Society for Heart and Lung Transplantation: Thirty-second Official Adult Lung and Heart-Lung Transplantation Report—2015; Focus Theme: Early Graft Failure. J. Heart Lung Transplant. 2015, 34, 1264–1277. [Google Scholar] [CrossRef] [PubMed]
- Balci, M.; Vayvada, M.; Salturk, C.; Kutlu, C.; Ari, E. Incidence of Early Acute Kidney Injury in Lung Transplant Patients: A Single-Center Experience. Transplant. Proc. 2017, 49, 593–598. [Google Scholar] [CrossRef]
- De La Morena, M.P.; Bravos, M.D.L.T.; Prado, R.F.; Roel, M.D.; Salcedo, J.G.; Costa, E.F.; Rivas, D.G.; Maté, J.B. Chronic Kidney Disease After Lung Transplantation: Incidence, Risk Factors, and Treatment. Transplant. Proc. 2010, 42, 3217–3219. [Google Scholar] [CrossRef]
- Hornum, M.; Iversen, M.; Steffensen, I.; Hovind, P.; Carlsen, J.; Andersen, L.W.; Steinbrüchel, D.A.; Feldt-Rasmussen, B.; Feldt-Rasmussen, B.; Feldt-Rasmussen, B. Rapid Decline in51Cr-EDTA Measured Renal Function During the First Weeks Following Lung Transplantation. Arab. Archaeol. Epigr. 2009, 9, 1420–1426. [Google Scholar] [CrossRef]
- Castro, A.G.; Llorca, J.; Cañas, B.S.; Fernández-Miret, B.; Zurbano, F.; Miñambres, E. Acute renal failure in lung transplantation: Incidence, correlation with subsequent kidney disease, and prognostic value. Arch. Bronconeumol. 2008, 44, 353–359. [Google Scholar] [CrossRef]
- Xue, J.; Wang, L.; Chen, C.-M.; Chen, J.-Y.; Sun, Z.-X. Acute kidney injury influences mortality in lung transplantation. Ren. Fail. 2014, 36, 541–545. [Google Scholar] [CrossRef] [Green Version]
- Ishikawa, S.; Griesdale, D.E.; Lohser, J. Acute Kidney Injury within 72 Hours After Lung Transplantation: Incidence and Perioperative Risk Factors. J. Cardiothorac. Vasc. Anesth. 2014, 28, 931–935. [Google Scholar] [CrossRef]
- Bagshaw, S.M.; George, C.; Bellomo, R. A comparison of the RIFLE and AKIN criteria for acute kidney injury in critically ill patients. Nephrol. Dial. Transplant. 2008, 23, 1569–1574. [Google Scholar] [CrossRef] [Green Version]
- Uchino, S.; Bellomo, R.; Goldsmith, D.; Bates, S.; Ronco, C. An assessment of the RIFLE criteria for acute renal failure in hospitalized patients. Crit. Care Med. 2006, 34, 1913–1917. [Google Scholar] [CrossRef] [PubMed]
- Palevsky, P.M.; Liu, K.D.; Brophy, P.D.; Chawla, L.S.; Parikh, C.R.; Thakar, C.V.; Tolwani, A.J.; Waikar, S.S.; Weisbord, S.D. KDOQI US Commentary on the 2012 KDIGO Clinical Practice Guideline for Acute Kidney Injury. Am. J. Kidney Dis. 2013, 61, 649–672. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Easterbrook, P.; Gopalan, R.; Berlin, J.; Matthews, D. Publication bias in clinical research. Lancet 1991, 337, 867–872. [Google Scholar] [CrossRef]
- Machuca, T.N.; Schio, S.M.; Camargo, S.M.; Lobato, V.; Costa, C.D.O.; Felicetti, J.C.; Moreira, J.S.; Camargo, J.J. Prognostic Factors in Lung Transplantation: The Santa Casa de Porto Alegre Experience. Transplantation 2011, 91, 1297–1303. [Google Scholar] [CrossRef]
- Wehbe, E.; Brock, R.; Budev, M.; Xu, M.; Demirjian, S.; Schreiber, M.J.; Stephany, B. Short-term and long-term outcomes of acute kidney injury after lung transplantation. J. Heart Lung Transplant. 2012, 31, 244–251. [Google Scholar] [CrossRef]
- Hennessy, S.A.; Gillen, J.R.; Hranjec, T.; Kozower, B.D.; Jones, D.R.; Kron, I.L.; Lau, C.L. Influence of hemodialysis on clinical outcomes after lung transplantation. J. Surg. Res. 2013, 183, 916–921. [Google Scholar] [CrossRef] [Green Version]
- Shigemura, N.; D’Cunha, J.; Bhama, J.K.; Shiose, A.; El Ela, A.A.; Hackmann, A.; Zaldonis, D.; Toyoda, Y.; Pilewski, J.M.; Luketich, J.D.; et al. Lobar Lung Transplantation: A Relevant Surgical Option in the Current Era of Lung Allocation Score. Ann. Thorac. Surg. 2013, 96, 451–456. [Google Scholar] [CrossRef]
- Silhan, L.L.; Shah, P.D.; Chambers, D.C.; Snyder, L.D.; Riise, G.C.; Wagner, C.L.; Hellström-Lindberg, E.; Orens, J.B.; Mewton, J.F.; Danoff, S.K.; et al. Lung transplantation in telomerase mutation carriers with pulmonary fibrosis. Eur. Respir. J. 2014, 44, 178–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tokman, S.; Singer, J.P.; Devine, M.S.; Westall, G.P.; Aubert, J.-D.; Tamm, M.; Snell, G.I.; Lee, J.S.; Goldberg, H.J.; Kukreja, J.; et al. Clinical outcomes of lung transplant recipients with telomerase mutations. J. Heart Lung Transplant. 2015, 34, 1318–1324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carillo, C.; Pecoraro, Y.; Anile, M.; Mantovani, S.; Oliva, A.; D’Abramo, A.; Amore, D.; Pagini, A.; De Giacomo, T.; Pugliese, F.; et al. Evaluation of Renal Function in Patients Undergoing Lung Transplantation. Transplant. Proc. 2017, 49, 699–701. [Google Scholar] [CrossRef] [PubMed]
- Sikma, M.A.; Hunault, C.C.; Van De Graaf, E.A.; Verhaar, M.C.; Kesecioglu, J.; De Lange, D.W.; Meulenbelt, J. High tacrolimus blood concentrations early after lung transplantation and the risk of kidney injury. Eur. J. Clin. Pharmacol. 2017, 73, 573–580. [Google Scholar] [CrossRef]
- Newton, C.A.; Kozlitina, J.; Lines, J.R.; Kaza, V.; Torres, F.; Garcia, C.K. Telomere length in patients with pulmonary fibrosis associated with chronic lung allograft dysfunction and post-lung transplantation survival. J. Heart Lung Transplant. 2017, 36, 845–853. [Google Scholar] [CrossRef]
- Banga, A.; Mohanka, M.; Mullins, J.; Bollineni, S.; Kaza, V.; Tanriover, B.; Torres, F. Characteristics and outcomes among patients with need for early dialysis after lung transplantation surgery. Clin. Transplant. 2017, 31, e13106. [Google Scholar] [CrossRef]
- Cosgun, T.; Tomaszek, S.; Opitz, I.; Wilhelm, M.; Schuurmans, M.M.; Weder, W.; Inci, I. Single-center experience with intraoperative extracorporeal membrane oxygenation use in lung transplantation. Int. J. Artif. Organs 2017. [Google Scholar] [CrossRef]
- Ahmad, O.; Shafii, A.E.; Mannino, D.M.; Choate, R.; Baz, M.A. Impact of donor lung pathogenic bacteria on patient outcomes in the immediate post-transplant period. Transpl. Infect. Dis. 2018, 20, e12986. [Google Scholar] [CrossRef]
- Iyengar, A.; Kwon, O.J.; Sanaiha, Y.; Eisenring, C.; Biniwale, R.; Ross, D.; Ardehali, A. Lung transplantation in the Lung Allocation Score era: Medium-term analysis from a single center. Clin. Transplant. 2018, 32, e13298. [Google Scholar] [CrossRef]
- Ri, H.S.; Son, H.J.; Oh, H.B.; Kim, S.Y.; Park, J.Y.; Kim, J.Y.; Choi, Y.J. Inhaled nitric oxide therapy was not associated with postoperative acute kidney injury in patients undergoing lung transplantation: A retrospective pilot study. Medicine 2018, 97, e10915. [Google Scholar] [CrossRef]
- Calabrese, D.R.; Florez, R.; Dewey, K.; Hui, C.; Torgerson, D.; Chong, T.; Faust, H.; Rajalingam, R.; Hays, S.R.; Golden, J.A.; et al. Genotypes associated with tacrolimus pharmacokinetics impact clinical outcomes in lung transplant recipients. Clin. Transplant. 2018, 32, e13332. [Google Scholar] [CrossRef] [PubMed]
- Bennett, D.; Fossi, A.; Marchetti, L.; Lanzarone, N.; Sisi, S.; Refini, R.M.; Sestini, P.; Luzzi, L.; Paladini, P.; Rottoli, P. Postoperative acute kidney injury in lung transplant recipients. Interact. Cardiovasc. Thorac. Surg. 2019, 28, 929–935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shashaty, M.G.S.; Forker, C.M.; Miano, T.A.; Wu, Q.; Yang, W.; Oyster, M.L.; Porteous, M.K.; Cantu, E.E., III; Diamond, J.M.; Christie, J.D. The association of post-lung transplant acute kidney injury with mortality is independent of primary graft dysfunction: A cohort study. Clin. Transplant. 2019, e13678. [Google Scholar] [CrossRef]
- Sharma, P.; Welch, K.; Eikstadt, R.; Marrero, J.A.; Fontana, R.J.; Lok, A.S. Renal outcomes after liver transplantation in the model for end-stage liver disease era. Liver Transplant. 2009, 15, 1142–1148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chatila, W.M.; Furukawa, S.; Gaughan, J.P.; Criner, G.J. Respiratory failure after lung transplantation. Chest 2003, 123, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Husain-Syed, F.; Slutsky, A.S.; Ronco, C. Lung–Kidney Cross-Talk in the Critically Ill Patient. Am. J. Respir. Crit. Care Med. 2016, 194, 402–414. [Google Scholar] [CrossRef] [PubMed]
- Sharkey, R.; Mulloy, E.; O’Neill, S. Acute effects of hypoxaemia, hyperoxaemia and hypercapnia on renal blood flow in normal and renal transplant subjects. Eur. Respir. J. 1998, 12, 653–657. [Google Scholar] [CrossRef]
- Hemlin, M.; Ljungman, S.; Carlson, J.; Maljukanovic, S.; Mobini, R.; Bech-Hanssen, O.; Skoogh, B.-E.; Skoogh, B. The effects of hypoxia and hypercapnia on renal and heart function, haemodynamics and plasma hormone levels in stable COPD patients. Clin. Respir. J. 2007, 1, 80–90. [Google Scholar] [CrossRef]
- Sharkey, R.A.; Mulloy, E.M.; O’Neill, S.J. The Acute Effects of Oxygen and Carbon Dioxide on Renal Vascular Resistance in Patients with an Acute Exacerbation of COPD. Chest 1999, 115, 1588–1592. [Google Scholar] [CrossRef]
- Anand, I.S.; Chandrashekhar, Y.; Ferrari, R.; Sarma, R.; Guleria, R.; Jindal, S.K.; Wahi, P.L.; Poole-Wilson, P.A.; Harris, P. Pathogenesis of congestive state in chronic obstructive pulmonary disease. Studies of body water and sodium, renal function, hemodynamics, and plasma hormones during edema and after recovery. Circulation 1992, 86, 12–21. [Google Scholar] [CrossRef]
- Sharkey, R.A.; Mulloy, E.M.; Kilgallen, I.A.; O’Neill, S.J. Renal functional reserve in patients with severe chronic obstructive pulmonary disease. Thorax 1997, 52, 411–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacNee, W. Pathophysiology of cor pulmonale in chronic obstructive pulmonary disease. Part One. Am. J. Respir. Crit. Care Med. 1994, 150, 833–852. [Google Scholar] [CrossRef] [PubMed]
- Magouliotis, D.E.; Tasiopoulou, V.S.; Svokos, A.A.; Svokos, K.A.; Zacharoulis, D. Extracorporeal membrane oxygenation versus cardiopulmonary bypass during lung transplantation: A meta-analysis. Gen. Thorac. Cardiovasc. Surg. 2018, 66, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Cheungpasitporn, W.; Thongprayoon, C.; Kittanamongkolchai, W.; Srivali, N.; O′corragain, O.A.; Edmonds, P.J.; Ratanapo, S.; Spanuchart, I.; Erickson, S.B. Comparison of Renal Outcomes in Off-Pump Versus On-Pump Coronary Artery Bypass Grafting: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Nephrology 2015, 20, 727–735. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Cheungpasitporn, W.; Lertjitbanjong, P.; Aeddula, N.R.; Bathini, T.; Watthanasuntorn, K.; Srivali, N.; Mao, M.A.; Kashani, K. Incidence and Impact of Acute Kidney Injury in Patients Receiving Extracorporeal Membrane Oxygenation: A Meta-Analysis. J. Clin. Med. 2019, 8, 981. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Kaewput, W.; Thamcharoen, N.; Bathini, T.; Watthanasuntorn, K.; Lertjitbanjong, P.; Sharma, K.; Salim, S.A.; Ungprasert, P.; Wijarnpreecha, K.; et al. Incidence and Impact of Acute Kidney Injury after Liver Transplantation: A Meta-Analysis. J. Clin. Med. 2019, 8, 372. [Google Scholar] [CrossRef]
- Ojo, A.O.; Held, P.J.; Port, F.K.; Wolfe, R.A.; Leichtman, A.B.; Young, E.W.; Arndorfer, J.; Christensen, L.; Merion, R.M. Chronic Renal Failure after Transplantation of a Nonrenal Organ. N. Engl. J. Med. 2003, 349, 931–940. [Google Scholar] [CrossRef]
- Grimm, J.C.; Lui, C.; Kilic, A.; Valero, V., 3rd; Sciortino, C.M.; Whitman, G.J.; Shah, A.S. A risk score to predict acute renal failure in adult patients after lung transplantation. Ann. Thorac. Surg. 2015, 99, 251–257. [Google Scholar] [CrossRef]
- Imai, Y.; Parodo, J.; Kajikawa, O.; De Perrot, M.; Fischer, S.; Edwards, V.; Cutz, E.; Liu, M.; Keshavjee, S.; Martin, T.R.; et al. Injurious Mechanical Ventilation and End-Organ Epithelial Cell Apoptosis and Organ Dysfunction in an Experimental Model of Acute Respiratory Distress Syndrome. JAMA 2003, 289, 2104–2112. [Google Scholar] [CrossRef] [Green Version]
- Koyner, J.L.; Murray, P.T. Mechanical ventilation and the kidney. Blood Purif. 2010, 29, 52–68. [Google Scholar] [CrossRef]
- Brower, R.G.; Matthay, M.A.; Morris, A.; Schoenfeld, D.; Thompson, B.T.; Wheeler, A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N. Engl. J. Med. 2000, 342, 1301–1308. [Google Scholar] [CrossRef] [PubMed]
- Ojo, A.O. Renal Disease in Recipients of Nonrenal Solid Organ Transplantation. Semin. Nephrol. 2007, 27, 498–507. [Google Scholar] [CrossRef] [PubMed]
- Clajus, C.; Hanke, N.; Gottlieb, J.; Stadler, M.; Weismüller, T.J.; Strassburg, C.P.; Bröcker, V.; Bara, C.; Lehner, F.; Drube, J.; et al. Renal Comorbidity After Solid Organ and Stem Cell Transplantation. Arab. Archaeol. Epigr. 2012, 12, 1691–1699. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | Country | Patients | Number | AKI Definition | AKI Incidence |
|---|---|---|---|---|---|---|
| Rocha et al. [13] | 2005 | USA | Patents underwent lung transplantation | 296 | RIFLE criteria | AKI 166/296 (56.1%) RRT 23/296 (7.8%) |
| -Double 146/296 (49.3%) | ||||||
| -COPD 134/296 (45.3%) | ||||||
| -Cystic fibrosis 61/296 (20.6%) | ||||||
| -Idiopathic pulmonary fibrosis 31/296 (10.5%) | ||||||
| Arnaoutakis et al. [11] | 2011 | USA | Patients underwent lung transplantation | 106 | RIFLE criteria | AKI 67/106 (63.2%) RRT 14/106 (13.2%) |
| -Double 93/106 (87.7%) | ||||||
| -COPD 33/106 (31.1%) | ||||||
| -Idiopathic pulmonary fibrosis 22/106 (20.8%) | ||||||
| -Cystic fibrosis 21/106 (19.8%) | ||||||
| Machuca et al. [37] | 2011 | Brazil | Patients underwent lung transplantation | 130 | Doubling of baseline serum creatinine levels | AKI 41/130 (31.5%) RRT 19/130 (14.6%) |
| - Idiopathic pulmonary fibrosis 53/130 (40.8%) | ||||||
| -COPD 52/130 (40%) | ||||||
| -Lymphangioleiomyomatosis 8/130 (6.2%) | ||||||
| -Cystic fibrosis 4/130 (3%) | ||||||
| George et al. [19] | 2012 | USA | Patients underwent lung transplantation from UNOS database | 12,108 | RRT | RRT 655/12,108 (5.41%) |
| -Double 6876/12,108 (56.8%) | ||||||
| -COPD 4227/12,108 (34.9%) | ||||||
| -Idiopathic pulmonary fibrosis 3369/12,108 (27.8%) | ||||||
| Jacques et al. [21] | 2012 | Canada | Patients underwent lung transplantation | 174 | RIFLE criteria | AKI 67/174 (38.5%) |
| -Double 85/174 (58.9%) | ||||||
| -Emphysema 64/174 (36.8%) | ||||||
| -Cystic fibrosis 44 /174 (25.3%) | ||||||
| -Idiopathic pulmonary fibrosis 24/174 (13.8%) | ||||||
| Wehbe et al. [38] | 2012 | USA | Patients underwent lung transplantation | 657 | AKIN classification | AKI 424/657 (64.5%) RRT 40/657 (6.1%) |
| -Double 372/657 (56.6%) | ||||||
| -COPD 233/657 (35.5%) | ||||||
| -Idiopathic pulmonary fibrosis 212/657 (32.3%) | ||||||
| -Cystic fibrosis 90/657 (13.7%) | ||||||
| Hennessy et al. [39] | 2013 | USA | Patients underwent lung transplantation | 352 | SCr > 3 mg/dL within 5 days after surgery | AKI 33/325 (9.4%) RRT 16/325 (4.9%) |
| -Double 98/352 (27.8%) | ||||||
| -COPD 170/352 (48.2%) | ||||||
| -Cystic fibrosis28/352 (8%) | ||||||
| -Pulmonary fibrosis 53/352 (15%) | ||||||
| Shigemura et al. [40] | 2013 | USA | -Patients underwent lobar lung transplantation. | 25 | RRT | RRT 4/25 (16%) |
| -Double 13/25 (52%) | ||||||
| -Idiopathic pulmonary fibrosis 9/25 (36%) | ||||||
| -Sarcoidosis 4/25 (16%) | ||||||
| -Cystic fibrosis 2/25 (8%) | ||||||
| Xue et al. [28] | 2014 | China | Patients underwent lung transplantation | 88 | AKIN classification | AKI 47/88 (53.4%) RRT 3/88 (3.4%) |
| -Double 38/88 (43.2%) | ||||||
| -Idiopathic pulmonary fibrosis 46/88 (52.3%) | ||||||
| -COPD 19/88 (21.6%) | ||||||
| -Brochiectesis7/88 (8%) | ||||||
| Ishikawa et al. [29] | 2014 | Canada | Patients underwent lung transplantation | 50 | RIFLE criteria | AKI during first 72 hours after transplant 27/50 (54%) AKI during hospitalization 32/50 (64%) RRT 4/50 (8%) |
| -Double 15/50 (30%) | ||||||
| -Interstitial lung disease 18/50 (36%) | ||||||
| -COPD 14/50 (28%) | ||||||
| -Cystic fibrosis 10/50 (20%) | ||||||
| -Alpha 1 antitrypsin deficiency 5/50 (10%) | ||||||
| Fidalgo et al. [14] | 2014 | Canada | Patient underwent lung transplant | 445 | KDIGO criteria | Total AKI 306/445 (68.8%) AKI in lung transplant only 290/425 (68.2%) RRT 36/445 (8.1%) |
| -Double 354/445 (79.6%) | ||||||
| -Heart-lung transplant 20/445 (4.5%) | ||||||
| -COPD 149/445 (33.5%) | ||||||
| -Idiopathic pulmonary fibrosis 99/445 (22.2%) | ||||||
| -Cystic fibrosis 71/445 (16%) | ||||||
| Silhan et al. [41] | 2014 | USA | Pulmonary fibrosis patients with telomerase mutation carriers underwent lung transplant | 8 | RRT | RRT 4/8 (50%) |
| -Double 5/8 (62.5%) | ||||||
| Tokman et al. [42] | 2015 | USA | Pulmonary fibrosis patients underwent lung transplantation | 14 | Increase in serum creatinine of ≥ 1.5 times from baseline within seven days after transplant | AKI 8/14 (57.1%) RRT 1/14 (7.1%) |
| -Double 12/14 (85.7%) | ||||||
| Sikma et al. [44] | 2017 | Netherlands | Patient underwent lung transplantation | 186 | KDIGO criteria | AKI 85/186 (45.7%) |
| -Double 148/186 (79.6%) | ||||||
| -COPD/alpha 1 antitrypsin deficiency 80/186 (43%) | ||||||
| -Sarcoidosis/Interstitial lung disease/usual interstitial pneumonia 14/186 (7.5%) | ||||||
| Carillo et al. [43] | 2017 | Italy | Patients underwent lung transplantation | 22 | RRT | RRT 5/22 (22.7%) |
| -Double 6/22 (27.3%) | ||||||
| -Pulmonary fibrosis 13/22 (59%) | ||||||
| -Emphysema 7/22(31.8%) | ||||||
| Balci et al. [24] | 2017 | Turkey | Patients underwent lung transplantation | 30 | AKIN classification | AKI 16/30 (53.3%) RRT 0/30 (0%) |
| -Idiopathic pulmonary fibrosis 10/30 (33.3%) | ||||||
| -COPD 6/30 (20%) | ||||||
| -Cystic fibrosis/bronchiectasis 9/30 (30%) | ||||||
| Nguyen et al. [10] | 2017 | USA | Patients underwent lung transplantation | 97 | RIFLE criteria | AKI 57/97 (58.8%) RRT 35/97 (38.5%) |
| -Double 55/97 (56.7%) | ||||||
| -COPD 11/97 (11.3%) | ||||||
| -Idiopathic pulmonary fibrosis 50/97 (51.5%) | ||||||
| -Cystic fibrosis 20/97 (20.6%) | ||||||
| -Pulmonary hypertension 11/97 (11.3%) | ||||||
| Banga et al. [46] | 2017 | USA | Patients underwent lung transplantation. Data was from UNOS database from 1994–2014 | 24,110 | RRT | RRT 1369/24,110 (5.7%) |
| Newton et al. [45] | 2017 | USA | Pulmonary fibrosis patients underwent lung transplantation. | 82 | increase in serum creatinine to ≥ 1.5 times from baseline within 7 days after transplant | AKI 54/82 (65.9%) RRT 2/82 (2.4%) |
| -Double 70/82 (85.4%) | ||||||
| Cosgun et al. [47] | 2017 | USA | Patient underwent lung transplantation | 291 | RRT | RRT 27/291 (9.3%) |
| -Double 285/291 (97.9%) | ||||||
| -Requiring intraoperative ECMO 134/291 (46.0%) | ||||||
| -Cystic fibrosis 89/291 (30.6%) | ||||||
| -COPD 88/291 (30.2%) | ||||||
| -Idiopathic pulmonary fibrosis 63/291 (21.6%) | ||||||
| Ahmad et al. [48] | 2018 | USA | Patients underwent lung transplantation from brain death donors | 32 | RIFLE criteria | AKI at 24 hours post-transplant = 6/32 (18.8%) AKI at 72 hours post-transplant = 4/32 (12.5%) |
| -Double 20/32 (62.5%) | ||||||
| -Interstitial lung disease 24/32 (75%) | ||||||
| -COPD 8/32 (25%) | ||||||
| Iyengar et al. [49] | 2018 | USA | Patients underwent lung transplantation | 501 | RRT | RRT 19/501 (3.8%) |
| -Double 267/501 (53.3%) | ||||||
| Ri et al. [50] | 2018 | Korea | Patient underwent lung transplantation | 33 | AKIN criteria | AKI 14/33 (42.4%) RRT 0/33 (0%) |
| -Idiopathic pulmonary fibrosis 12/33 (36.4%) | ||||||
| -Interstitial lung disease 20/33 (60.6%) | ||||||
| -Primary pulmonary hypertension 1/14 (7.1%) | ||||||
| Calabrese et al. [51] | 2018 | USA | Patient underwent lung transplantation | 321 | KDIGO criteria | AKI KDIGO stage 2 and 3 61/321 (19.0%) |
| -Double 288/321 (89.7%) | ||||||
| -Heart-lung 6/321 (1.9%) | ||||||
| -Idiopathic pulmonary fibrosis 210/321 (65.4%) | ||||||
| -COPD 66/321 (20.6%) | ||||||
| -Cystic fibrosis 31/321 (9.7%) | ||||||
| Bennett et al. [52] | 2019 | Italy | Patients underwent lung transplantation | 135 | KDIGO criteria | AKI 45/135 (33.3%) RRT 18/135 (13.3%) |
| -Double 66/135 (48.9%) | ||||||
| -Pulmonary fibrosis 72/135 (53.33%) | ||||||
| -COPD 28/135 (20.74%) | ||||||
| -Cystic fibrosis 25/135 (18.52%) | ||||||
| Shashaty et al. [53] | 2019 | USA | Patients underwent lung transplantation | 299 | KDIGO criteria | AKI 188/299 (62.9%) RRT 19/299 (6.4%) |
| -Double 180/299 (60.2%) | ||||||
| -COPD 119/299 (39.8%) | ||||||
| -Interstitial lung disease 123/299 (41.1%) | ||||||
| -Cystic fibrosis 26/299 (8.70%) |
| Study | Year | Results | Confounder Adjustment |
|---|---|---|---|
| Rocha et al. [13] | 2005 | One-year mortality | None |
| AKI: 4.33 (2.08–8.99) | |||
| RRT: 23.70 (8.29–67.80) | |||
| Five-year mortality | |||
| AKI: 1.44 (0.90–2.30) | |||
| RRT: 9.73 (2.82–33.53) | |||
| Arnaoutakis et al. [11] | 2011 | In-hospital mortality | Lung allocation score, pre-transplant GFR, recipient age, donor cigarette use, postoperative tracheostomy |
| AKI: 0.48 (0.13–1.71) | |||
| RRT: 28.2 (6.18–128.1) | |||
| One-year mortality | |||
| AKI: 0.47 (0.20–1.14) | |||
| RRT: 4.97 (1.54–16.0) | |||
| Machuca et al. [37] | 2011 | Mortality | Mechanical ventilation duration, reintubation, acute rejection in the first month, coronary heart disease |
| AKI: 2.47 (1.13–5.39) | |||
| RRT: 2.68 (1.36–5.27) | |||
| George et al. [19] | 2012 | 30-day mortality | Recipient age, GFR, BMI, diagnosis, mean pulmonary artery pressure, ICU status, ECMO support, donor age, bilateral lung transplant, ischemic time, annual center volume |
| RRT: 7.87 (6.07–10.20) | |||
| One-year mortality | |||
| RRT: 7.89 (6.80–9.15) | |||
| Five-year mortality | |||
| RRT: 5.35 (4.72–6.07) | |||
| Jacques et al. [21] | 2012 | 30-day mortality | Age, sex, indication, ICU length of stay, coronary artery disease, aprotinin use, double lung transplantation |
| AKI:1.36 (0.40–4.64) | |||
| Long-term mortality | |||
| AKI: 1.54 (0.79–2.99) | |||
| Wehbe et al. [38] | 2012 | Hospital mortality | Age, sex, race, type on lung transplantation, COPD, pre-transplantation diabetes, baseline creatinine |
| AKI: 6.05 (1.83–20.00) | |||
| RRT: 13.66 (6.19–30.17) | |||
| One-year mortality | |||
| AKI: 2.92 (1.76–4.82) | |||
| Hennessy et al. [39] | 2013 | 30-day mortality | None |
| AKI: 10.23 (4.05–25.86) | |||
| RRT: 41.41 (13.06–131.31) | |||
| One-year mortality | |||
| AKI: 7.01 (3.29–14.92) | |||
| RRT: 43.04 (9.48–195.50) | |||
| Xue et al. [28] | 2014 | Five-year mortality | Age, sex, type, and cause of lung transplant, hypertension, and diabetes |
| AKI: 1.48 (1.04–2.11) | |||
| Ishikawa et al. [29] | 2014 | Mortality | None |
| AKI: 3/27 (11%) vs. 0/23 (0%) | |||
| Fidalgo et al. [14] | 2014 | Hospital mortality | Age, sex, COPD, eGFR, LAS score, diabetes mellitus, pulmonary artery pressure, previous sternotomy, type of lung transplant, ICU length of stay |
| AKI: 22/306 (7%) vs. 0/139 (0%) | |||
| One-year mortality | |||
| AKI: 2.81 (1.15–6.84) | |||
| Balci et al. [24] | 2017 | 30-day mortality | None |
| AKI: 0.82 (0.18–3.74) | |||
| Nguyen et al. [10] | 2017 | One-year mortality | None |
| AKI: 1.73 (0.42–7.13) | |||
| RRT: 1.20 (0.32–4.60) | |||
| Banga et al. [46] | 2017 | One-year mortality | Age, serum albumin, type of procedure, CMV mismatch, Length of hospital stay after transplantation, recipient hospitalized at the time of transplant, history of prior cardiac surgery, acute rejection |
| RRT: 7.23 (6.2–8.43) | |||
| Five-year mortality | |||
| RRT: 3.96 (3.43–4.56) | |||
| Bennett et al. [52] | 2019 | One-year mortality | None |
| AKI: 6.20 (2.74–14.05) | |||
| RRT: 21.60 (5.75–81.11) | |||
| Shashaty et al. [53] | 2019 | One-year mortality | Primary graft dysfunction, age, bilateral lung transplant |
| AKI: 3.64 (1.68–7.88) |
| Reported Risk Factors for AKI after Lung Transplantation |
|---|
|
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lertjitbanjong, P.; Thongprayoon, C.; Cheungpasitporn, W.; O’Corragain, O.A.; Srivali, N.; Bathini, T.; Watthanasuntorn, K.; Aeddula, N.R.; Salim, S.A.; Ungprasert, P.; et al. Acute Kidney Injury after Lung Transplantation: A Systematic Review and Meta-Analysis. J. Clin. Med. 2019, 8, 1713. https://doi.org/10.3390/jcm8101713
Lertjitbanjong P, Thongprayoon C, Cheungpasitporn W, O’Corragain OA, Srivali N, Bathini T, Watthanasuntorn K, Aeddula NR, Salim SA, Ungprasert P, et al. Acute Kidney Injury after Lung Transplantation: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2019; 8(10):1713. https://doi.org/10.3390/jcm8101713
Chicago/Turabian StyleLertjitbanjong, Ploypin, Charat Thongprayoon, Wisit Cheungpasitporn, Oisín A. O’Corragain, Narat Srivali, Tarun Bathini, Kanramon Watthanasuntorn, Narothama Reddy Aeddula, Sohail Abdul Salim, Patompong Ungprasert, and et al. 2019. "Acute Kidney Injury after Lung Transplantation: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 8, no. 10: 1713. https://doi.org/10.3390/jcm8101713