Cerebral White Matter Hyperintensity as a Healthcare Quotient

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Automated Measurement of WMH Volume
2.3. WMH-BHQ, a Novel Quotient Based on WMHV
2.4. Statistical Analysis
2.5. Standard Protocol Approvals, Registrations, and Participant Consents
2.6. Data Availability
3. Results
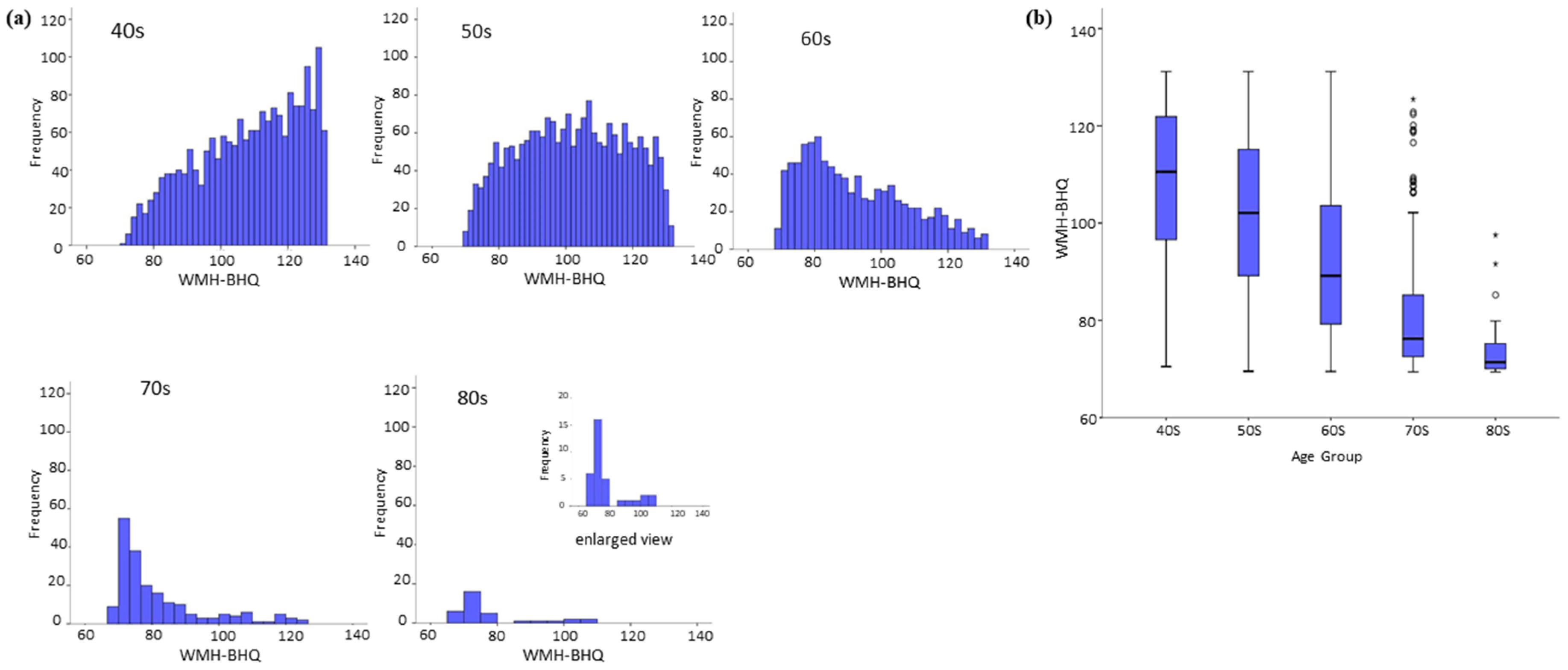
3.1. WMH-BHQ of Participants with no Medical History According to Age Decades
3.2. WMH-BHQ Histograms of Sex
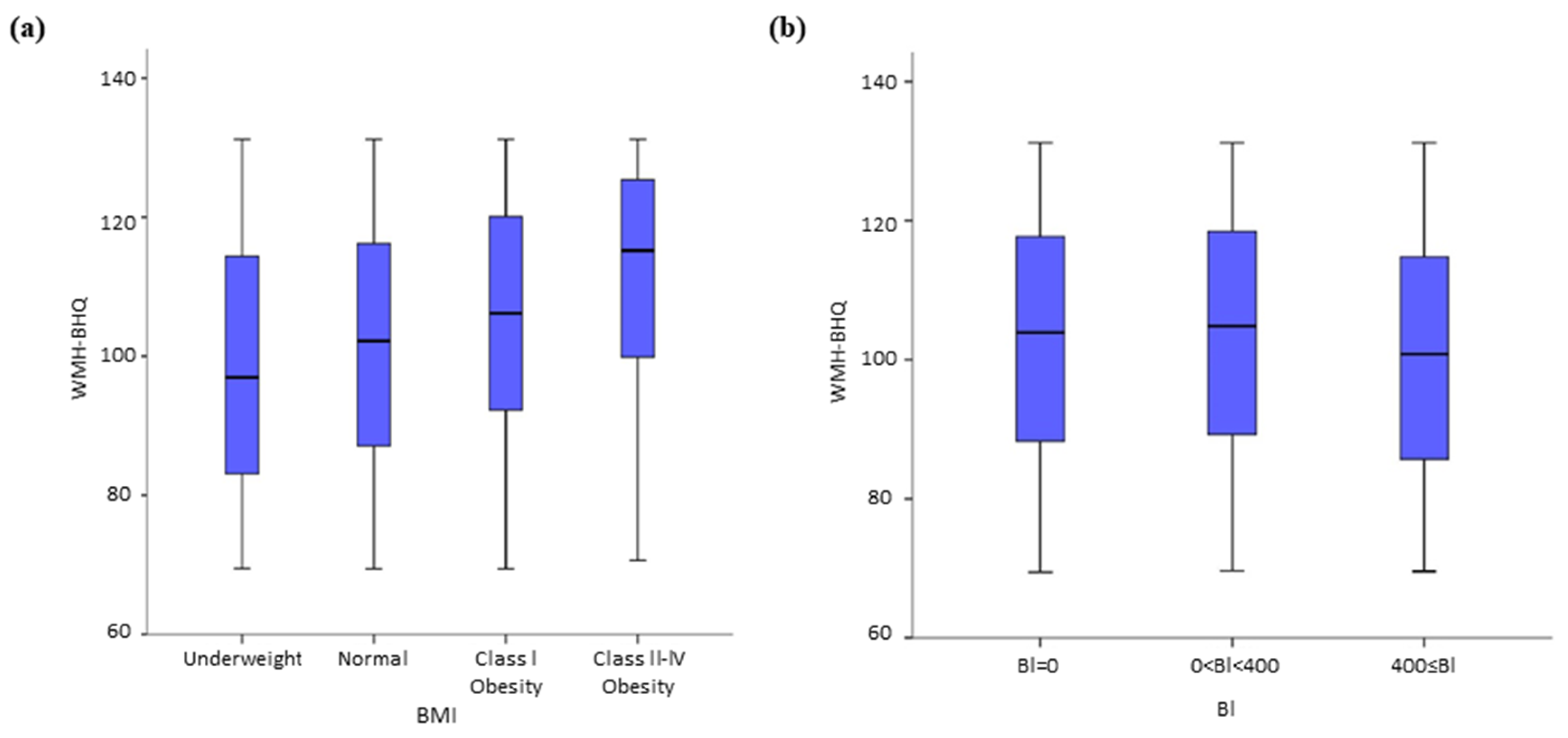
3.3. Analysis of WMH-BHQ Risk Factors: No VRCs
3.4. WMH-BHQ without VRCs: the Effect of Three Classifications and Two Criteria
3.5. WMH-BHQ with VRCs and Their Comorbidities
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pantoni, L. Cerebral small vessel disease: From pathogenesis and clinical characteristics to therapeutic challenges. Lancet Neurol. 2010, 9, 689–701. [Google Scholar] [CrossRef]
- Debette, S.; Markus, H.S. The clinical importance of white matter hyperintensities on brain magnetic resonance imaging: Systematic review and meta-analysis. BMJ 2010, 341, c3666. [Google Scholar] [CrossRef] [PubMed]
- Salat, D.H. Imaging small vessel-associated white matter changes in aging. Neuroscience 2014, 276, 174–186. [Google Scholar] [CrossRef] [PubMed]
- Zeestraten, E.A.; Lawrence, A.J.; Lambert, C.; Benjamin, P.; Brookes, R.L.; Mackinnon, A.D.; Morris, R.G.; Barrick, T.R.; Markus, H.S. Change in multimodal MRI markers predicts dementia risk in cerebral small vessel disease. Neurology 2017, 89, 1869–1876. [Google Scholar] [CrossRef] [Green Version]
- Ding, J.; Sigurðsson, S.; Jonson, P.V.; Eiriksdottir, G.; Charidimou, A.; Lopez, O.L.; van Buchem, M.A.; Guðnason, V.; Launer, L.J. Large perivascular spaces visible on magnetic resonance imaging, cerebral small vessel disease progression, and risk of dementia: The age, gene/environment susceptibility-reykjavik study. JAMA Neurol. 2017, 74, 1105–1112. [Google Scholar] [CrossRef]
- Baradaran, H.; Al-Dasuqi, K.; Knight-Greenfield, A.; Giambrone, A.; Delgado, D.; Ebani, E.J.; Kamel, H.; Gupta, A. Association between Carotid plaque features on CTA and cerebrovascular ischemia: A systematic review and meta-analysis. AJNR Am. J. Neuroradiol 2017, 38, 2321–2326. [Google Scholar] [CrossRef]
- Staals, J.; Makin, S.D.; Doubal, F.N.; Dennis, M.S.; Wardlaw, J.M. Stroke subtype, vascular risk factors, and total MRI brain small-vessel disease burden. Neurology 2014, 83, 1228–1234. [Google Scholar] [CrossRef]
- Pantoni, L.; Garcia, J.H. Pathogenesis of leukoaraiosis: A review. Stroke 1997, 28, 652–659. [Google Scholar] [CrossRef]
- Lin, J.; Wang, D.; Lan, L.; Fan, Y. Multiple factors involved in the pathogenesis of white matter lesions. Biomed. Res. Int. 2017, 2017, 1–9. [Google Scholar] [CrossRef]
- Habes, M.; Erus, G.; Toledo, J.B.; Zhang, T.; Bryan, N.; Launer, L.J.; Rosseel, Y.; Janowitz, D.; Doshi, J.; Van der Auwera, S.; et al. White matter hyperintensities and imaging patterns of brain ageing in the general population. Brain 2016, 139, 1164–1179. [Google Scholar] [CrossRef] [Green Version]
- Park, K.; Yasuda, N.; Toyonaga, S.; Yamada, S.M.; Nakabayashi, H.; Nakasato, M.; Nakagomi, T.; Tsubosaki, E.; Shimizu, K. Significant association between leukoaraiosis and metabolic syndrome in healthy subjects. Neurology 2007, 69, 974–978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bokura, H.; Yamaguchi, S.; Iijima, K.; Nagai, A.; Oguro, H. Metabolic syndrome is associated with silent ischemic brain lesions. Stroke 2008, 39, 1607–1609. [Google Scholar] [CrossRef] [PubMed]
- Assayag, E.B.; Eldor, R.; Korczyn, A.D.; Kliper, E.; Shenhar-Tsarfaty, S.; Tene, O.; Molad, J.; Shapira, I.; Berliner, S.; Volfson, V.; et al. Type 2 diabetes mellitus and impaired renal function are associated with brain alterations and poststroke cognitive decline. Stroke 2017, 48, 2368–2374. [Google Scholar] [CrossRef] [PubMed]
- Cole, J.H.; Ritchie, S.J.; Bastin, M.E.; Valdés Hernández, M.C.; Muñoz Maniega, S.; Royle, N.; Corley, J.; Pattie, A.; Harris, S.E.; Zhang, Q.; et al. Brain age predicts mortality. Mol. Psychiatry 2018, 23, 1385–1392. [Google Scholar] [CrossRef] [PubMed]
- Nemoto, K.; Oka, H.; Fukuda, H.; Yamakawa, Y. MRI-based brain healthcare quotients: A bridge between neural and behavioral analyses for keeping the brain healthy. PLoS ONE 2017, 12, e0187137. [Google Scholar] [CrossRef] [PubMed]
- Park, K.; Nakagawa, Y.; Kumagai, Y.; Nagahara, M. Leukoaraiosis, a common brain magnetic resonance imaging finding, as a predictor of traffic crashes. PLoS ONE 2013, 8, e57255. [Google Scholar] [CrossRef] [PubMed]
- Ashburner, J. SPM: A history. Neuroimage 2012, 62, 791–800. [Google Scholar] [CrossRef] [Green Version]
- Dunn, O.J. Multiple comparisons among means. J. Am. Stat. Assoc. 1961, 56, 52–64. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B. Stat. Methodol. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Darlington, R. Multiple regression in psychological research and practice. Psychol. Bull. 1968, 69, 161–182. [Google Scholar] [CrossRef]
- IBM Corp. IBM SPSS Statistics for Windows; Version 22.0; IBM Corp: Armonk, NY, USA, 2013. [Google Scholar]
- Schulz, U.G.; Rothwell, P.M. Differences in vascular risk factors between etiology subtypes of ischemic stroke: Importance of population-based studies. Stroke 2003, 34, 2050–2059. [Google Scholar] [CrossRef] [PubMed]
- Verhaaren, B.F.; Vernooij, M.W.; de Boer, R.; Hofman, A.; Niessen, W.J.; van der Lugt, A.; Ikram, M.A. High blood pressure and cerebral white matter lesion progression in the general population. Hypertension 2013, 61, 1354–1359. [Google Scholar] [CrossRef] [PubMed]
- Fatemi, F.; Kantarci, K.; Graff-Radford, J.; Preboske, G.M.; Weigand, S.D.; Przybelski, S.A.; Knopman, D.S.; Machulda, M.M.; Roberts, R.O.; Mielke, M.M. Sex differences in cerebrovascular pathologies on FLAIR in cognitively unimpaired elderly. Neurology 2018, 90, e466–e473. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Obesity and Overweight [Fact Sheet]; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Corvera, S.; Gealekman, O. Adipose tissue angiogenesis: Impact on obesity and type-2 diabetes. Biochim. Biophys. Acta 2014, 1842, 463–472. [Google Scholar] [CrossRef] [PubMed]
- La Paglia, L.; Listì, A.; Caruso, S.; Amodeo, V.; Passiglia, F.; Bazan, V.; Fanale, D. Potential role of ANGPTL4 in the cross talk between metabolism and cancer through PPAR signaling pathway. PPAR Res. 2017, 17, 8187–8235. [Google Scholar] [CrossRef] [PubMed]
- Kabboord, A.D.; van Eijk, M.; Fiocco, M.; van Balen, R.; Achterberg, W.P. Assessment of comorbidity burden and its association with functional rehabilitation outcome after stroke or hip fracture: A systematic review and meta-analysis. J. Am. Med. Dir. Assoc. 2016, 17, 1066.e13–1066.e21. [Google Scholar] [CrossRef]
- Hole, B.; Salem, J. How long do patients with chronic disease expect to live? A systematic review of the literature. BMJ Open 2016, 6, e012248. [Google Scholar] [CrossRef]
- Gallacher, K.I.; Batty, G.D.; McLean, G.; Mercer, S.W.; Guthrie, B.; May, C.R.; Langhorne, P.; Mair, F.S. Stroke, multimorbidity and polypharmacy in a nationally representative sample of 1,424,378 patients in Scotland: Implications for treatment burden. BMC Med. 2014, 12, 151. [Google Scholar] [CrossRef]
- Chróinín, D.N.; Asplund, K.; Åsberg, S.; Callaly, E.; Cuadrado-Godia, E.; Díez-Tejedor, E.; Di Napoli, M.; Engelter, S.T.; Furie, K.L.; Giannopoulos, S.; et al. Statin therapy and outcome after ischemic stroke: Systematic review and meta-analysis of observational studies and randomized trials. Stroke 2013, 44, 448–456. [Google Scholar] [CrossRef]
- Choi, J.Y.; Seo, W.K.; Kang, S.H.; Jung, J.M.; Cho, K.H.; Yu, S.; Oh, K. Statins improve survival in patients with cardioembolic stroke. Stroke 2014, 45, 1849–1852. [Google Scholar] [CrossRef]
- Garg, R.; Oh, E.; Naidech, A.; Kording, K.; Prabhakaran, S. Automating ischemic stroke subtype classification using machine learning and natural language processing. J. Stroke Cerebrovasc. Dis. 2019, 28, 2045–2051. [Google Scholar] [CrossRef] [PubMed]
- Schirmer, M.D.; Dalca, A.V.; Sridharan, R.; Giese, A.K.; Donahue, K.L.; Nardin, M.J.; Mocking, S.J.T.; McIntosh, E.C.; Frid, P.; Wasselius, J.; et al. White matter hyperintensity quantification in large scale clinical acute ischemic stroke cohort. The MRI-GENIE study. Neuroimage Clin. 2019, 23, 101884. [Google Scholar] [CrossRef] [PubMed]
- Ganau, L.; Prisco, L.; Ligarotti, G.K.I.; Ambu, R.; Ganau, M. Understanding the pathological basis of neurological diseases through diagnostic platforms based on innovations in biomedical engineering: New concepts and theranostic perspectives. Medicines (Basel) 2018, 5, 22. [Google Scholar] [CrossRef] [PubMed]
- Perri1, C.D.; Dwyer, M.G.; Wack, D.S.; Cox, J.L.; Hashmi, K.; Saluste, E.; Hussein, S.; Dalaker, T.O.; Schirda, C.; Bastianello, S. White Matter Hyperintensities on 1.5 and 3 Tesla Brain MRI in Healthy Individuals. J. Biomed. Gr. Comput. 2013. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Male | Female | Mean Age ± SD (Years) | Median Age (Years) | |
|---|---|---|---|---|---|
| No medical history | 5541 | 2760 | 2781 | 51.4 ± 9.8 | 51 |
| HT only | 1074 | 622 | 422 | 59.5 ± 9.3 | 59 |
| DM only | 150 | 114 | 36 | 59.3 ± 9.8 | 59 |
| DLP only | 299 | 124 | 175 | 56.9 ± 8.7 | 57 |
| HT + DLP | 220 | 124 | 96 | 60.0 ± 9.0 | 59 |
| HT + DM | 124 | 97 | 27 | 60.8 ± 9.0 | 60 |
| DM + DLP | 35 | 19 | 16 | 57.0 ± 7.6 | 57 |
| HT + DM + DLP | 67 | 39 | 28 | 60.4 ± 7.6 | 59 |
| Classification and Criteria | |
|---|---|
| BMI | Underweight, BMI < 18.5; normal, 18.5 ≤ BMI < 25, overweight, 25 ≤ BMI< 30; and obese, BMI ≥ 30 |
| BI | BI = 0, 0 < BI < 400, and BI ≥ 400 |
| High BP | Systolic blood pressure (SBP) < 139, 140 ≤ SBP < 160, SBP ≥ 160 |
| IFG | A (fasting blood sugar (FBS) < 100 and HbA1c < 5.6%) B (100 ≤ FBS < 100 or 5.6% ≤ HbA1c < 6.0%) C (110 ≤ FBS < 126 or 6.0% ≤ HbA1c < 6.5%) D (FBS ≥ 126 or HbA1c ≥ 6.5%) |
| ALM | Triglycerides (TG); TG < 29, 30 ≤ TG< 140, 140 ≤ TG< 400, and TG ≥ 400 Ratios of LDL to HDL (LH ratio): LH ratio < 1, 1 ≤ LH ratio < 1.5, 1.5 ≤ LH ratio < 2, 2 ≤ LH ratio < 2.5, and LH ratio ≥ 2.5 |
| Mann-Whitney U (M-W U) Test | |||||||
|---|---|---|---|---|---|---|---|
| Male | Female | ||||||
| Age Decade | N | Mean Rank | N | Mean Rank | M-W U | Z | P |
| 30s | 351 | 276.7 | 239 | 323.1 | 35361 | −3.24 | 0.001 |
| 40s | 955 | 855.0 | 865 | 971.8 | 359991 | −4.74 | 0.001 |
| 50s | 920 | 971.9 | 1117 | 1057.8 | 470485.5 | −3.28 | 0.001 |
| 60s | 437 | 449.5 | 460 | 448.5 | 100299.5 | −0.05 | 0.957 |
| 70s | 89 | 88.0 | 82 | 83.9 | 3473 | −0.54 | 0.586 |
| 80s | 8 | 14.9 | 18 | 12.9 | 61 | −0.61 | 0.541 |
| Model | Unstandardized Coefficients | Standardized Coefficients | t | p | 95% Confidence Interval for B | ||
|---|---|---|---|---|---|---|---|
| B | Standard Error | Beta | Lower Bound | Upper Bound | |||
| (Constant) | 125.170 | 2.256 | 55.49 | <0.001 | 120.750 | 129.595 | |
| Age | −0.064 | 0.022 | −0.377 | −29.53 | <0.001 | −0.708 | −0.620 |
| Body mass index (BMI) | 0.693 | 0.070 | 0.135 | 9.86 | <0.001 | 0.556 | 0.831 |
| Systolic blood pressure (SBP) | −0.079 | 0.015 | −0.074 | −5.41 | <0.001 | −0.108 | −0.051 |
| Brinkman index (BI) | −0.003 | 0.001 | −0.049 | −3.88 | <0.001 | −0.004 | −0.001 |
| Fasting blood glucose (FBG) | 0.045 | 0.015 | 0.038 | 2.96 | 0.003 | 0.015 | 0.074 |
| Triglycerides (TG) | 0.008 | 0.003 | 0.036 | 2.75 | 0.006 | 0.002 | 0.013 |
| Pairwise Comparison by Dunn Test | ||||||
|---|---|---|---|---|---|---|
| Comparison 1 | Comparison 2 | Test Statistic | SD | Z | Unadjusted p-Value | Adjusted p-Value |
| No medical history | HT | 911.74 | 72.29 | 12.61 | <0.001 | <0.001 |
| DLP | 368.32 | 128.72 | 2.86 | 0.004 | 0.015 | |
| DM | 793.29 | 179.40 | 4.42 | <0.001 | <0.001 | |
| HT + DLP | 765.91 | 149.05 | 5.14 | <0.001 | <0.001 | |
| HT + DM | 1307.35 | 196.87 | 6.64 | <0.001 | <0.001 | |
| DLP + DM | 188.32 | 367.63 | 0.51 | 0.608 | 0.710 | |
| HT + DLP + DM | 928.24 | 266.47 | 3.48 | <0.001 | 0.002 | |
| HT | DLP | −543.42 | 141.77 | −3.83 | <0.001 | 0.001 |
| DM | −118.45 | 188.98 | −0.63 | 0.531 | 0.676 | |
| HT + DLP | −145.83 | 160.45 | −0.91 | 0.363 | 0.485 | |
| HT + DM | 395.61 | 205.63 | 1.92 | 0.054 | 0.098 | |
| DLP + DM | −723.42 | 372.40 | −1.94 | 0.052 | 0.098 | |
| HT + DLP + DM | 16.49 | 273.01 | 0.06 | 0.952 | 0.952 | |
| DLP | DM | 424.97 | 216.93 | 1.96 | 0.050 | 0.098 |
| HT + DLP | 397.59 | 192.58 | 2.07 | 0.039 | 0.098 | |
| HT + DM | 939.03 | 231.58 | 4.06 | <0.001 | <0.001 | |
| DLP + DM | −180.00 | 387.33 | −0.47 | 0.642 | 0.719 | |
| HT + DLP + DM | 559.91 | 293.05 | 1.91 | 0056 | 0.098 | |
| DM | HT + DLP | −27.38 | 229.57 | −0.12 | 0.905 | 0.939 |
| HT + DM | 514.06 | 263.15 | 1.95 | 0.051 | 0.098 | |
| DLP + DM | −604.97 | 406.99 | −1.49 | 0.137 | 0.211 | |
| HT + DLP + DM | 134.94 | 318.59 | 0.42 | 0.672 | 0.724 | |
| HT + DLP | HT + DM | 541.44 | 243.46 | 2.22 | 0.026 | 0.073 |
| DLP + DM | −577.59 | 394.55 | −1.46 | 0.143 | 0.211 | |
| HT + DLP + DM | 162.32 | 302.53 | 0.54 | 0.592 | 0.710 | |
| HT+DM | DLP + DM | −1119.08 | 414.99 | −2.70 | 0.007 | 0.022 |
| HT + DLP + DM | −379.12 | 328.74 | −1.15 | 0.249 | 0.348 | |
| DLP+DM | HT + DLP + DM | 739.91 | 452.18 | 1.64 | 0.102 | 0.168 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, K.; Nemoto, K.; Yamakawa, Y.; Yamashita, F.; Yoshida, K.; Tamura, M.; Kawaguchi, A.; Arai, T.; Sasaki, M. Cerebral White Matter Hyperintensity as a Healthcare Quotient. J. Clin. Med. 2019, 8, 1823. https://doi.org/10.3390/jcm8111823
Park K, Nemoto K, Yamakawa Y, Yamashita F, Yoshida K, Tamura M, Kawaguchi A, Arai T, Sasaki M. Cerebral White Matter Hyperintensity as a Healthcare Quotient. Journal of Clinical Medicine. 2019; 8(11):1823. https://doi.org/10.3390/jcm8111823
Chicago/Turabian StylePark, Kaechang, Kiyotaka Nemoto, Yoshinori Yamakawa, Fumio Yamashita, Keitaro Yoshida, Masashi Tamura, Atsushi Kawaguchi, Tetsuaki Arai, and Makoto Sasaki. 2019. "Cerebral White Matter Hyperintensity as a Healthcare Quotient" Journal of Clinical Medicine 8, no. 11: 1823. https://doi.org/10.3390/jcm8111823