Effects of Volatile versus Total Intravenous Anesthesia on Occurrence of Myocardial Injury after Non-Cardiac Surgery



Abstract
1. Introduction
2. Methods
2.1. Study Population and Data Collection
2.2. Study Outcomes and Definitions
2.3. Statistical Analysis
3. Results
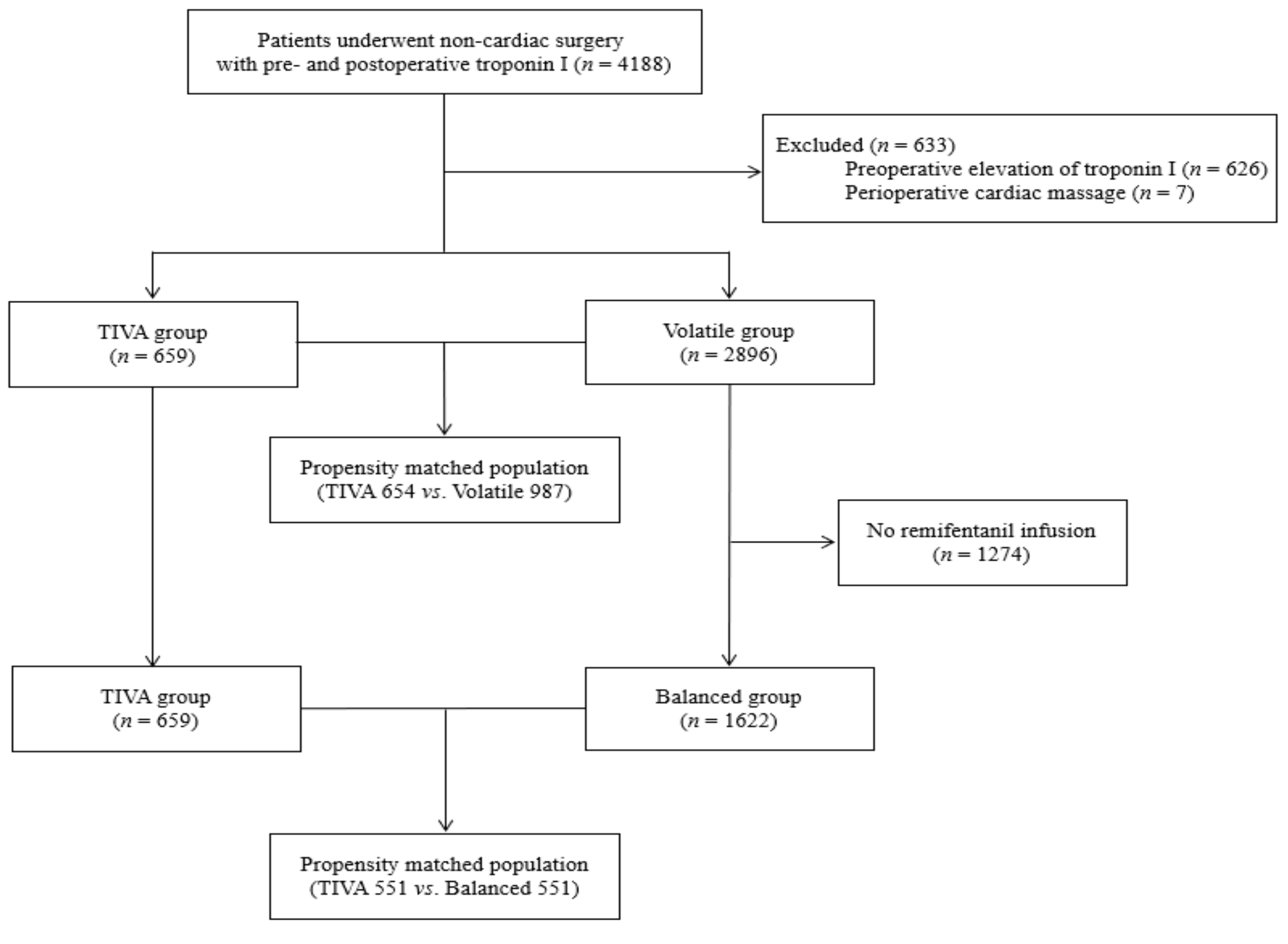
3.1. Patient Characteristics
3.2. Anesthetic Techniques and MINS after Matching
3.3. Anesthetic Techniques and Other Secondary Outcomes after Matching
3.4. Subanalysis of the Volatile Group: Volatile Only Group versus Balanced Group
3.5. Predictors of MINS
4. Discussion
4.1. Summary of Results
4.2. Current Evidence for Volatile Anesthetics vs. TIVA in Non-Cardiac Surgery
4.3. Possible Implications of Our Findings
4.4. Postoperative AKI
4.5. Other Things to Consider for Drug Selection in Non-Cardiac Surgery
4.6. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- Devereaux, P.J.; Szczeklik, W. Myocardial injury after non-cardiac surgery: Diagnosis and management. Eur. Heart J. 2019. [Google Scholar] [CrossRef] [PubMed]
- Writing Committee for the Vision Study Investigators; Devereaux, P.J.; Biccard, B.M.; Sigamani, A.; Xavier, D.; Chan, M.T.V.; Srinathan, S.K.; Walsh, M.; Abraham, V.; Pearse, R.; et al. Association of Postoperative High-Sensitivity Troponin Levels With Myocardial Injury and 30-Day Mortality Among Patients Undergoing Noncardiac Surgery. JAMA 2017, 317, 1642–1651. [Google Scholar] [PubMed]
- Botto, F.; Alonso-Coello, P.; Chan, M.T.; Villar, J.C.; Xavier, D.; Srinathan, S.; Guyatt, G.; Cruz, P.; Graham, M.; Wang, C.Y.; et al. Myocardial injury after noncardiac surgery: A large, international, prospective cohort study establishing diagnostic criteria, characteristics, predictors, and 30-day outcomes. Anesthesiology 2014, 120, 564–578. [Google Scholar] [CrossRef] [PubMed]
- Puelacher, C.; Lurati Buse, G.; Seeberger, D.; Sazgary, L.; Marbot, S.; Lampart, A.; Espinola, J.; Kindler, C.; Hammerer, A.; Seeberger, E.; et al. Perioperative Myocardial Injury After Noncardiac Surgery: Incidence, Mortality, and Characterization. Circulation 2018, 137, 1221–1232. [Google Scholar] [CrossRef]
- Khan, J.; Alonso-Coello, P.; Devereaux, P.J. Myocardial injury after noncardiac surgery. Curr. Opin. Cardiol. 2014, 29, 307–311. [Google Scholar] [CrossRef]
- Devereaux, P.J.; Sessler, D.I. Cardiac Complications in Patients Undergoing Major Noncardiac Surgery. N. Engl. J. Med. 2015, 373, 2258–2269. [Google Scholar] [CrossRef]
- Lotz, C.; Kehl, F. Volatile anesthetic-induced cardiac protection: Molecular mechanisms, clinical aspects, and interactions with nonvolatile agents. J. Cardiothorac. Vasc. Anesth. 2015, 29, 749–760. [Google Scholar] [CrossRef]
- Uhlig, C.; Bluth, T.; Schwarz, K.; Deckert, S.; Heinrich, L.; De Hert, S.; Landoni, G.; Serpa Neto, A.; Schultz, M.J.; Pelosi, P.; et al. Effects of Volatile Anesthetics on Mortality and Postoperative Pulmonary and Other Complications in Patients Undergoing Surgery: A Systematic Review and Meta-analysis. Anesthesiology 2016, 124, 1230–1245. [Google Scholar] [CrossRef]
- Landoni, G.; Greco, T.; Biondi-Zoccai, G.; Nigro Neto, C.; Febres, D.; Pintaudi, M.; Pasin, L.; Cabrini, L.; Finco, G.; Zangrillo, A. Anaesthetic drugs and survival: A Bayesian network meta-analysis of randomized trials in cardiac surgery. Br. J. Anaesth. 2013, 111, 886–896. [Google Scholar] [CrossRef]
- Lindholm, E.E.; Aune, E.; Noren, C.B.; Seljeflot, I.; Hayes, T.; Otterstad, J.E.; Kirkeboen, K.A. The anesthesia in abdominal aortic surgery (ABSENT) study: A prospective, randomized, controlled trial comparing troponin T release with fentanyl-sevoflurane and propofol-remifentanil anesthesia in major vascular surgery. Anesthesiology 2013, 119, 802–812. [Google Scholar] [CrossRef]
- Landoni, G.; Lomivorotov, V.V.; Nigro Neto, C.; Monaco, F.; Pasyuga, V.V.; Bradic, N.; Lembo, R.; Gazivoda, G.; Likhvantsev, V.V.; Lei, C.; et al. Volatile Anesthetics versus Total Intravenous Anesthesia for Cardiac Surgery. N. Engl. J. Med. 2019, 380, 1214–1225. [Google Scholar] [CrossRef] [PubMed]
- Sheng, M.; Zhang, G.; Wang, J.; Yang, Q.; Zhao, H.; Cheng, X.; Xu, Z. Remifentanil Induces Cardio Protection Against Ischemia/Reperfusion Injury by Inhibiting Endoplasmic Reticulum Stress Through the Maintenance of Zinc Homeostasis. Anesth. Analg. 2018, 127, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, V.S.; Jarolim, P. How to interpret elevated cardiac troponin levels. Circulation 2011, 124, 2350–2354. [Google Scholar] [CrossRef] [PubMed]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D. Executive Group on behalf of the Joint European Society of Cardiology/American College of Cardiology /American Heart Association /World Heart Federation Task Force for the Universal Definition of Myocardial, I. Fourth Universal Definition of Myocardial Infarction (2018). J. Am. Coll. Cardiol. 2018, 72, 2231–2264. [Google Scholar] [PubMed]
- Machado, M.N.; Nakazone, M.A.; Maia, L.N. Acute kidney injury based on KDIGO (Kidney Disease Improving Global Outcomes) criteria in patients with elevated baseline serum creatinine undergoing cardiac surgery. Braz. J. Cardiovasc. Surg. 2014, 29, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, S.D.; Knuuti, J. New ESC/ESA Guidelines on non-cardiac surgery: Cardiovascular assessment and management. Cardiovasc. Assess. Manag. 2014, 35, 2344–2345. [Google Scholar] [CrossRef]
- Pagel, P.S.; Crystal, G.J. The Discovery of Myocardial Preconditioning Using Volatile Anesthetics: A History and Contemporary Clinical Perspective. J. Cardiothorac. Vasc. Anesth. 2018, 32, 1112–1134. [Google Scholar] [CrossRef]
- Jakobsen, C.J.; Berg, H.; Hindsholm, K.B.; Faddy, N.; Sloth, E. The influence of propofol versus sevoflurane anesthesia on outcome in 10,535 cardiac surgical procedures. J. Cardiothorac. Vasc. Anesth. 2007, 21, 664–671. [Google Scholar] [CrossRef]
- Rodriguez-Lopez, J.M.; Sanchez-Conde, P.; Lozano, F.S.; Nicolas, J.L.; Garcia-Criado, F.J.; Cascajo, C.; Muriel, C. Laboratory investigation: Effects of propofol on the systemic inflammatory response during aortic surgery. Can. J. Anaesth. 2006, 53, 701–710. [Google Scholar] [CrossRef]
- Sanchez-Conde, P.; Rodriguez-Lopez, J.M.; Nicolas, J.L.; Lozano, F.S.; Garcia-Criado, F.J.; Cascajo, C.; Gonzalez-Sarmiento, R.; Muriel, C. The comparative abilities of propofol and sevoflurane to modulate inflammation and oxidative stress in the kidney after aortic cross-clamping. Anesth. Analg. 2008, 106, 371–378, table of contents. [Google Scholar] [CrossRef]
- Fleisher, L.A.; Fleischmann, K.E.; Auerbach, A.D.; Barnason, S.A.; Beckman, J.A.; Bozkurt, B.; Davila-Roman, V.G.; Gerhard-Herman, M.D.; Holly, T.A.; Kane, G.C.; et al. 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014, 130, 2215–2245. [Google Scholar] [CrossRef] [PubMed]
- Landoni, G.; Fochi, O.; Bignami, E.; Calabro, M.G.; D’Arpa, M.C.; Moizo, E.; Mizzi, A.; Pappalardo, F.; Morelli, A.; Zangrillo, A. Cardiac protection by volatile anesthetics in non-cardiac surgery? A meta-analysis of randomized controlled studies on clinically relevant endpoints. HSR Proc. Intensive Care Cardiovasc. Anesth. 2009, 1, 34–43. [Google Scholar] [PubMed]
- Lurati Buse, G.A.; Schumacher, P.; Seeberger, E.; Studer, W.; Schuman, R.M.; Fassl, J.; Kasper, J.; Filipovic, M.; Bolliger, D.; Seeberger, M.D. Randomized comparison of sevoflurane versus propofol to reduce perioperative myocardial ischemia in patients undergoing noncardiac surgery. Circulation 2012, 126, 2696–2704. [Google Scholar] [CrossRef] [PubMed]
- Alsina, E.; Matute, E.; Ruiz-Huerta, A.D.; Gilsanz, F. The effects of sevoflurane or remifentanil on the stress response to surgical stimulus. Curr. Pharm. Des. 2014, 20, 5449–5468. [Google Scholar] [CrossRef]
- Wong, G.T.; Huang, Z.; Ji, S.; Irwin, M.G. Remifentanil reduces the release of biochemical markers of myocardial damage after coronary artery bypass surgery: A randomized trial. J. Cardiothorac. Vasc. Anesth. 2010, 24, 790–796. [Google Scholar] [CrossRef]
- Thompson, J.P.; Hall, A.P.; Russell, J.; Cagney, B.; Rowbotham, D.J. Effect of remifentanil on the haemodynamic response to orotracheal intubation. Br. J. Anaesth. 1998, 80, 467–469. [Google Scholar] [CrossRef]
- Zhang, Y.; Irwin, M.G.; Wong, T.M. Remifentanil preconditioning protects against ischemic injury in the intact rat heart. Anesthesiology 2004, 101, 918–923. [Google Scholar] [CrossRef]
- Motayagheni, N.; Phan, S.; Eshraghi, C.; Nozari, A.; Atala, A. A Review of Anesthetic Effects on Renal Function: Potential Organ Protection. Am. J. Nephrol. 2017, 46, 380–389. [Google Scholar] [CrossRef]
- Zheng, G.; Qu, H.; Li, F.; Ma, W.; Yang, H. Propofol attenuates sepsis-induced acute kidney injury by regulating miR-290-5p/CCL-2 signaling pathway. Braz. J. Med Biol. Res. 2018, 51, e7655. [Google Scholar] [CrossRef]
- Basu, S.; Meisert, I.; Eggensperger, E.; Krieger, E.; Krenn, C.G. Time course and attenuation of ischaemia-reperfusion induced oxidative injury by propofol in human renal transplantation. Redox Rep. Commun. Free Radic. Res. 2007, 12, 195–202. [Google Scholar] [CrossRef]
- Yoo, Y.C.; Yoo, K.J.; Lim, B.J.; Jun, J.H.; Shim, J.K.; Kwak, Y.L. Propofol attenuates renal ischemia-reperfusion injury aggravated by hyperglycemia. J. Surg. Res. 2013, 183, 783–791. [Google Scholar] [CrossRef] [PubMed]
- Agewall, S.; Giannitsis, E.; Jernberg, T.; Katus, H. Troponin elevation in coronary vs. non-coronary disease. Eur. Heart J. 2011, 32, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Yap, A.; Lopez-Olivo, M.A.; Dubowitz, J.; Hiller, J.; Riedel, B.; The Global Onco-Anesthesia Research Collaboration Group. Anesthetic technique and cancer outcomes: A meta-analysis of total intravenous versus volatile anesthesia. Can. J. Anaesth. D’anesthésie 2019, 66, 546–561. [Google Scholar] [CrossRef] [PubMed]
- Wigmore, T.J.; Mohammed, K.; Jhanji, S. Long-term Survival for Patients Undergoing Volatile versus IV Anesthesia for Cancer Surgery: A Retrospective Analysis. Anesthesiology 2016, 124, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.F.; Lee, M.S.; Wong, C.S.; Lu, C.H.; Huang, Y.S.; Lin, K.T.; Lou, Y.S.; Lin, C.; Chang, Y.C.; Lai, H.C. Propofol-based Total Intravenous Anesthesia Is Associated with Better Survival Than Desflurane Anesthesia in Colon Cancer Surgery. Anesthesiology 2018, 129, 932–941. [Google Scholar] [CrossRef]


{kind=link}
| Before Matching | After Matching | |||||||
|---|---|---|---|---|---|---|---|---|
| TIVA (n = 659) | Volatile (n = 2896) | P | SMD | TIVA (n = 564) | Volatile (n = 978) | P | SMD | |
| Male sex | 299 (45.4) | 2014 (69.5) | <0.001 | 0.504 | 289 (51.2) | 542 (55.4) | 0.125 | 0.084 |
| Age, years | 63.02 (11.94) | 64.89 (± 12.71) | <0.001 | 0.152 | 63.50 (11.78) | 63.85 (13.21) | 0.595 | 0.028 |
| Smoking | 52 (7.9) | 413 (14.3) | <0.001 | 0.204 | 50 (8.9) | 99 (10.1) | 0.474 | 0.043 |
| BMI | 24.33 (3.76) | 23.68 (3.66) | <0.001 | −0.175 | 24.14 (3.69) | 24.03 (3.79) | 0.586 | 0.029 |
| Comorbidities | ||||||||
| Hypertension | 321 (48.7) | 1538 (53.1) | 0.046 | 0.088 | 278 (49.3) | 492 (50.3) | 0.740 | 0.020 |
| Diabetes | 147 (22.3) | 803 (27.7) | 0.005 | 0.125 | 138 (24.5) | 251 (25.7) | 0.645 | 0.028 |
| Old MI | 28 (4.2) | 151 (5.2) | 0.355 | 0.045 | 27 (4.8) | 56 (5.7) | 0.503 | 0.042 |
| Previous PCI | 48 (7.3) | 340 (11.7) | 0.001 | 0.152 | 47 (8.3) | 89 (9.1) | 0.676 | 0.027 |
| Previous CABG | 15 (2.3) | 147 (5.1) | 0.003 | 0.149 | 15 (2.7) | 39 (4.0) | 0.221 | 0.074 |
| PAOD | 15 (2.3) | 327 (11.3) | <0.001 | 0.364 | 15 (2.7) | 37 (3.8) | 0.303 | 0.064 |
| Carotid arterial disease | 56 (8.5) | 711 (24.6) | <0.001 | 0.237 | 97 (17.2) | 188 (19.2) | 0.358 | 0.052 |
| COPD | 69 (10.5) | 343 (11.8) | 0.354 | 0.044 | 62 (11.0) | 110 (11.2) | 0.945 | 0.008 |
| History of stroke | 78 (11.8) | 419 (14.5) | 0.090 | 0.078 | 73 (12.9) | 139 (14.2) | 0.535 | 0.037 |
| Chronic kidney disease | 29 (4.4) | 236 (8.1) | 0.001 | 0.155 | 28 (5.0) | 56 (5.7) | 0.604 | 0.034 |
| Dialysis | 9 (1.4) | 70 (2.4) | 0.132 | 0.077 | 9 (1.6) | 20 (2.0) | 0.667 | 0.034 |
| Cancer | 119 (18.1) | 672 (23.2) | 0.005 | 0.127 | 112 (19.9) | 212 (21.7) | 0.436 | 0.045 |
| Heart failure EF. | 9 (1.4) | 56 (1.9) | 0.412 | 0.045 | 9 (1.6) | 17 (1.7) | 0.997 | 0.011 |
| Arrythmia | 48 (7.3) | 264 (9.1) | 0.154 | 0.067 | 47 (8.3) | 81 (8.3) | 1.000 | −0.002 |
| Valve disease | 18 (2.7) | 83 (2.9) | 0.954 | 0.008 | 18 (3.2) | 28 (2.9) | 0.834 | −0.019 |
| Aortic disease | 8 (1.2) | 237 (8.2) | <0.001 | 0.334 | 8 (1.4) | 17 (1.7) | 0.787 | 0.026 |
| PTE DVT | 12 (1.8) | 52 (1.8) | 1.000 | −0.002 | 10 (1.8) | 17 (1.7) | 1.000 | −0.003 |
| Preop. CRP elevation | 160 (24.3) | 1262 (43.6) | <0.001 | 0.416 | 156 (27.7) | 297 (30.4) | 0.286 | 0.060 |
| Medication | ||||||||
| ACEi_ARB | 165 (25.0) | 825 (28.5) | 0.083 | 0.078 | 148 (26.2) | 255 (26.1) | 0.990 | −0.004 |
| Aspirin | 141 (21.4) | 831 (28.7) | <0.001 | 0.169 | 131 (23.2) | 241 (24.6) | 0.573 | 0.033 |
| BB | 82 (12.4) | 578 (20.0) | <0.001 | 0.205 | 76 (13.5) | 147 (15.0) | 0.446 | 0.045 |
| CCB | 165 (25.0) | 772 (26.7) | 0.422 | 0.037 | 145 (25.7) | 251 (25.7) | 1.000 | −0.001 |
| clopidogrel | 55 (8.3) | 402 (13.9) | <0.001 | 0.177 | 54 (9.6) | 104 (10.6) | 0.566 | 0.035 |
| Statin | 152 (23.1) | 806 (27.8) | 0.015 | 0.110 | 136 (24.1) | 245 (25.1) | 0.726 | 0.022 |
| Intraoperative parameter | ||||||||
| OP risk | <0.001 | 0.086 | ||||||
| Low | 38 (5.8) | 219 (7.6) | 0.072 | 38 (6.7) | 73 (7.5) | 0.028 | ||
| Intermediate | 611 (92.7) | 2039 (70.4) | −0.601 | 516 (91.5) | 869 (88.9) | −0.089 | ||
| High | 10 (1.5) | 638 (22.0) | 0.671 | 10 (1.8) | 36 (3.7) | 0.117 | ||
| Emergent operation | 87 (13.2) | 695 (24.0) | <0.001 | 0.280 | 84 (14.9) | 168 (17.2) | 0.273 | 0.062 |
| OP duration | 211.28 (124.81) | 208.92 (145.48) | 0.671 | −0.017 | 205.30 (118.04) | 195.11 (134.72) | 0.122 | 0.080 |
| inotropic requirement | 76 (11.5) | 940 (32.5) | <0.001 | 0.522 | 75 (13.3) | 161 (16.5) | 0.112 | 0.089 |
| RBC transfusion | 0.87 (0.59) | 0.75 (0.74) | <0.001 | −0.176 | 0.83 (0.59) | 0.79 (0.82) | 0.266 | 0.056 |
| Before Matching | After Matching | |||||||
|---|---|---|---|---|---|---|---|---|
| TIVA (n = 659) | Balanced (n = 1622) | P | SMD | TIVA (n = 551) | Balanced (n = 551) | P | SMD | |
| Male sex | 299 (45.4) | 1148 (70.8) | <0.001 | −0.533 | 288 (52.3) | 290 (52.6) | 0.952 | −0.007 |
| Age, years | 63.02 (11.94) | 65.61 (12.45) | <0.001 | 0.213 | 63.34 (11.61) | 64.20 (13.43) | 0.257 | −0.068 |
| Smoking | 52 (7.9) | 249 (15.4) | <0.001 | −0.234 | 51 (9.3) | 49 (8.9) | 0.916 | 0.013 |
| BMI | 24.33 (3.76) | 23.78 (3.61) | 0.001 | 0.149 | 24.16 (3.67) | 24.17 (3.76) | 0.958 | −0.003 |
| Comorbidities | ||||||||
| Hypertension | 321 (48.7) | 949 (58.5) | <0.001 | −0.197 | 277 (50.3) | 284 (51.5) | 0.718 | −0.025 |
| Diabetes | 147 (22.3) | 492 (30.3) | <0.001 | −0.183 | 135 (24.5) | 138 (25.0) | 0.889 | −0.013 |
| Old MI | 28 (4.2) | 92 (5.7) | 0.202 | −0.066 | 28 (5.1) | 30 (5.4) | 0.893 | −0.016 |
| Previous PCI | 48 (7.3) | 208 (12.8) | <0.001 | −0.185 | 48 (8.7) | 44 (8.0) | 0.744 | 0.026 |
| Previous CABG | 15 (2.3) | 101 (6.2) | <0.001 | −0.197 | 15 (2.7) | 16 (2.9) | 1.000 | −0.011 |
| PAOD | 15 (2.3) | 238 (14.7) | <0.001 | −0.457 | 15 (2.7) | 16 (2.9) | 1.000 | −0.011 |
| Carotid arterial disease | 56 (8.5) | 230 (14.2) | <0.001 | −0.18 | 56 (10.2) | 53 (9.6) | 0.840 | 0.018 |
| COPD | 69 (10.5) | 210 (12.9) | 0.117 | −0.077 | 65 (11.8) | 68 (12.3) | 0.853 | −0.017 |
| History of stroke | 78 (11.8) | 255 (15.7) | 0.021 | −0.113 | 70 (12.7) | 82 (14.9) | 0.337 | −0.063 |
| Chronic kidney disease | 29 (4.4) | 121 (7.5) | 0.010 | −0.13 | 27 (4.9) | 33 (6.0) | 0.507 | −0.048 |
| Dialysis | 9 (1.4) | 29 (1.8) | 0.594 | −0.034 | 9 (1.6) | 11 (2.0) | 0.821 | −0.027 |
| Cancer | 119 (18.1) | 303 (18.7) | 0.773 | −0.016 | 108 (19.6) | 115 (20.9) | 0.653 | −0.032 |
| Heart failure EF. | 9 (1.4) | 36 (2.2) | 0.245 | −0.064 | 9 (1.6) | 11 (2.0) | 0.821 | −0.027 |
| Arrythmia | 48 (7.3) | 154 (9.5) | 0.109 | −0.08 | 47 (8.5) | 58 (10.5) | 0.305 | −0.068 |
| Valve disease | 18 (2.7) | 51 (3.1) | 0.699 | −0.024 | 18 (3.3) | 19 (3.4) | 1.000 | −0.01 |
| Aortic disease | 8 (1.2) | 194 (12.0) | <0.001 | −0.444 | 8 (1.5) | 12 (2.2) | 0.498 | −0.054 |
| PTE DVT | 12 (1.8) | 29 (1.8) | 1.000 | −0.002 | 10 (1.8) | 13 (2.4) | 0.673 | −0.038 |
| Medication | ||||||||
| ACEi_ARB | 165 (25.0) | 514 (31.7) | 0.002 | −0.148 | 144 (26.1) | 136 (24.7) | 0.628 | 0.033 |
| Aspirin | 141 (21.4) | 535 (33.0) | <0.001 | −0.263 | 131 (23.8) | 125 (22.7) | 0.721 | 0.026 |
| BB | 82 (12.4) | 349 (21.5) | <0.001 | −0.243 | 80 (14.5) | 84 (15.2) | 0.800 | −0.02 |
| CCB | 165 (25.0) | 484 (29.8) | 0.024 | −0.108 | 148 (26.9) | 141 (25.6) | 0.681 | 0.029 |
| clopidogrel | 55 (8.3) | 260 (16.0) | <0.001 | −0.237 | 54 (9.8) | 51 (9.3) | 0.837 | 0.019 |
| Statin | 152 (23.1) | 533 (32.9) | <0.001 | −0.22 | 140 (25.4) | 140 (25.4) | 1.000 | 0 |
| Preop. CRP elevation | 160 (24.3) | 618 (38.1) | <0.001 | −0.302 | 155 (28.1) | 178 (32.3) | 0.149 | −0.091 |
| Intraoperative parameter | ||||||||
| OP risk | <0.001 | 0.659 | ||||||
| Low | 38 (5.8) | 90 (5.5) | 0.009 | 36 (6.5) | 39 (7.1) | −0.022 | ||
| Intermediate | 611 (92.7) | 1171 (72.2) | 0.56 | 505 (91.7) | 498 (90.4) | 0.044 | ||
| High | 10 (1.5) | 361 (22.3) | −0.676 | 10 (1.8) | 14 (2.5) | −0.05 | ||
| Emergent operation | 87 (13.2) | 276 (17.0) | 0.028 | −0.107 | 83 (15.1) | 89 (16.2) | 0.678 | −0.03 |
| OP duration | 211.28 (124.81) | 203.18 (117.68) | 0.143 | 0.067 | 205.19 (120.97) | 198.91 (125.69) | 0.398 | −0.051 |
| inotropic requirement | 76 (11.5) | 491 (30.3) | <0.001 | −0.474 | 75 (13.6) | 91 (16.5) | 0.206 | −0.081 |
| RBC transfusion | 0.87 (0.59) | 0.74 (0.61) | <0.001 | 0.214 | 0.81 (0.55) | 0.81 (0.62) | 0.959 | −0.003 |
| TIVA (n = 564) | Volatile (n = 97 ) | Univariable Analysis | Multivariable Analysis | |||
|---|---|---|---|---|---|---|
| Unadjusted OR (95% CI) | P-Value | Adjusted OR (95% CI) | P-Value | |||
| Primary Outcome | ||||||
| MINS | 57 (10.1) | 147 (15.0) | 0.636 (0.459–0.880) | 0.006 | 0.642 (0.450–0.914) | 0.014 |
| Secondary Outcomes | ||||||
| 30-day mortality | 10 (1.77) | 32 (3.27) | 0.534 (0.260–1.094) | 0.086 | 0.617 (0.294–1.293) | 0.201 |
| AKI, all stage | 18 (3.19) | 86 (8.79) | 0.342 (0.203–0.575) | <0.001 | 0.346 (0.202–0.593) | 0.0001 |
| AKI 1 | 16 (2.83) | 67 (6.85) | 0.397 (0.228–0.692) | 0.001 | 0.395 (0.223–0.701) | 0.002 |
| AKI 2 | 1 (0.17) | 15 (1.53) | 0.114 (0.015–0.866) | 0.036 | 0.108 (0.013–0.928) | 0.043 |
| AKI 3 | 1 (0.17) | 4 (0.41) | 0.432 (0.048–3.879) | 0.454 | 0.301 (0.027–3.385) | 0.331 |
| In-hospital events | ||||||
| Mortality | 13 (2.31) | 32 (3.27) | 0.697 (0.363–1.340) | 0.281 | 0.955 (0.472–1.932) | 0.897 |
| Myocardial infarction | 3 (0.53) | 8 (0.81) | 0.648 (0.171–2.454) | 0.523 | 0.699 (0.182–2.686) | 0.602 |
| New arrythmia | 14 (2.48) | 30 (3.06) | 0.804 (0.423–1.530) | 0.507 | 0.783 (0.404–1.517) | 0.467 |
| New atrial fibrillation | 11 (1.95) | 31 (3.16) | 0.161 (0.303–1.218) | 0.608 | 0.581 (0.284–1.189) | 0.137 |
| TIVA (n = 551) | Balanced (n = 551) | Univariable Analysis | Multivariable Analysis | |||
|---|---|---|---|---|---|---|
| Unadjusted OR (95% CI) | P-Value | Adjusted OR (95% CI) | P-Value | |||
| Primary Outcome | ||||||
| MINS | 56 (10.2) | 71 (12.9) | 0.765 (0.527–1.110) | 0.158 | 0.832 (0.554–1.251) | 0.377 |
| Secondary Outcomes | ||||||
| 30-day mortality | 10 (0.22) | 16 (0.35) | 0.618 (0.278–1.374) | 0.238 | 0.597 (0.256–1.395) | 0.233 |
| AKI, all stage | 18 (3.99) | 41 (9.11) | 0.420 (0.238–0.741) | 0.003 | 0.362 (0.194–0.675) | 0.001 |
| AKI 1 | 15 (3.33) | 36 (7.98) | 0.400 (0.217–0.740) | 0.003 | 0.358 (0.184–0.698) | 0.003 |
| AKI 2 | 2 (0.43) | 4 (0.88) | 0.498 (0.091–2.731) | 0.422 | 0.238 (0.021–2.668) | 0.244 |
| AKI 3 | 1 (0.22) | 1 (0.22) | 1.000 (0.062–16.01) | 1.001 | 1.201 (0.048–29.98) | 0.911 |
| In-hospital events | ||||||
| Mortality | 14 (3.11) | 13 (2.88) | 1.079 (0.502–2.317) | 0.846 | 1.315 (0.577–2.995) | 0.515 |
| Myocardial infarction | 3 (0.66) | 3 (0.66) | 1.000 (0.201–4.976) | 1.001 | 1.105 (0.216–5.644) | 0.905 |
| New arrythmia | 11 (2.43) | 14 (3.11) | 0.781 (0.352–1.737) | 0.545 | 0.832 (0.371–1.864) | 0.655 |
| New atrial fibrillation | 8 (1.77) | 18 (3.99) | 0.436 (0.188–1.012) | 0.053 | 0.486 (0.202–1.168) | 0.107 |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| Unadjusted OR (95% CI) | P-Value | Adjusted OR (95% CI) | P-Value | |
| Anesthetic technique | 0.38 (0.29–0.50) | <0.001 | 0.62 (0.46–0.84) | 0.002 |
| Male sex | 1.15 (0.97–1.37) | 0.111 | 0.78 (0.64–0.95) | 0.015 |
| Age, years | 1.01 (1.00–1.01) | 0.05 | 1.02 (1.01–1.03) | <0.001 |
| Smoking | 0.91 (0.71–1.17) | 0.454 | ||
| BMI | 0.97 (0.95–0.99) | 0.013 | 0.97 (0.95–1.00) | 0.025 |
| Comorbidities | ||||
| Hypertension | 1.11 (0.94–1.31) | 0.209 | ||
| Diabetes | 1.21 (1.01–1.45) | 0.039 | 1.06 (0.85–1.31) | 0.609 |
| Old MI | 1.02 (0.71–1.49) | 0.879 | ||
| Previous PCI | 1.45 (1.14–1.85) | 0.003 | 1.44 (0.98–2.12) | 0.064 |
| Previous CABG | 2.11 (1.51–2.96) | <0.001 | 2.05 (1.32–3.29) | 0.001 |
| PAOD | 1.00 (0.76–1.32) | 0.981 | ||
| Carotid arterial disease | 1.03 (0.80–1.33) | 0.821 | 1.08 (0.78–1.50) | 0.636 |
| COPD | 1.08 (0.84–1.39) | 0.542 | ||
| History of stroke | 1.39 (1.12–1.74) | 0.003 | 1.40 (1.08–1.82) | 0.011 |
| Chronic kidney disease | 3.65 (2.82–4.73) | <0.001 | 3.55 (2.54–5.00) | <0.001 |
| Dialysis | 2.76 (1.75–4.37) | <0.001 | 0.77 (0.42–1.41) | 0.401 |
| Cancer | 1.02 (0.94–1.24) | 0.839 | ||
| Heart failure | 2.35 (1.41–3.92) | 0.001 | 1.79 (0.94–3.30) | 0.065 |
| Arrythmia | 1.35 (1.03–1.77) | 0.028 | 1.16 (0.84–1.59) | 0.375 |
| Valve disease | 2.05 (1.65–3.13) | 0.001 | 2.28 (1.43–3.64) | 0.001 |
| Aortic disease | 2.24 (1.70–2.96) | <0.001 | 0.98 (0.71–1.37) | 0.915 |
| PTE DVT | 0.56 (0.27–1.18) | 0.126 | 0.50 (0.22–1.15) | 0.103 |
| Preop. CRP elevation | 0.71 (0.60–0.84) | <0.001 | 1.14 (0.94–1.39) | 0.194 |
| Medication | ||||
| ACEi_ARB | 0.97 (0.81–1.17) | 0.764 | ||
| Aspirin | 1.19 (1.00–1.43) | 0.056 | 1.20 (0.95–1.52) | 0.131 |
| BB | 1.54 (1.27–1.88) | <0.001 | 1.10 (0.87–1.40) | 1.103 |
| CCB | 1.06 (0.88–1.27) | 0.538 | ||
| Clopidogrel | 1.31 (1.04–1.66) | 0.021 | 1.11 (0.82–1.51) | 0.497 |
| Statin | 1.05 (0.87–1.26) | 0.622 | ||
| Intraoperative parameter | ||||
| Operation risk | <0.001 | 0.021 | ||
| Low | ||||
| Intermediate | 0.91 (0.65–1.27) | 0.75 (0.52–1.09) | ||
| High | 2.16 (1.52–3.08) | 1.05 (0.68–1.60) | ||
| Emergent operation | 1.69 (1.41–2.04) | <0.001 | 2.11 (1.68–2.65) | <0.001 |
| Operation duration | 1.00 (1.00–1.00) | <0.002 | 1.00 (1.00–1.00) | <0.001 |
| Inotropic requirement | 5.08 (1.27–6.04) | <0.001 | 3.38 (2.78–4.12) | <0.001 |
| RBC transfusion | 1.82 (1.61–2.05) | <0.001 | 1.38 (1.21–1.58) | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, J.-H.; Park, J.; Lee, S.-H.; Oh, A.-r.; Lee, J.-H.; Min, J.J. Effects of Volatile versus Total Intravenous Anesthesia on Occurrence of Myocardial Injury after Non-Cardiac Surgery. J. Clin. Med. 2019, 8, 1999. https://doi.org/10.3390/jcm8111999
Kwon J-H, Park J, Lee S-H, Oh A-r, Lee J-H, Min JJ. Effects of Volatile versus Total Intravenous Anesthesia on Occurrence of Myocardial Injury after Non-Cardiac Surgery. Journal of Clinical Medicine. 2019; 8(11):1999. https://doi.org/10.3390/jcm8111999
Chicago/Turabian StyleKwon, Ji-Hye, Jungchan Park, Seung-Hwa Lee, Ah-ran Oh, Jong-Hwan Lee, and Jeong Jin Min. 2019. "Effects of Volatile versus Total Intravenous Anesthesia on Occurrence of Myocardial Injury after Non-Cardiac Surgery" Journal of Clinical Medicine 8, no. 11: 1999. https://doi.org/10.3390/jcm8111999
APA StyleKwon, J.-H., Park, J., Lee, S.-H., Oh, A.-r., Lee, J.-H., & Min, J. J. (2019). Effects of Volatile versus Total Intravenous Anesthesia on Occurrence of Myocardial Injury after Non-Cardiac Surgery. Journal of Clinical Medicine, 8(11), 1999. https://doi.org/10.3390/jcm8111999