Incremental Predictive Value of Longitudinal Axis Strain and Late Gadolinium Enhancement Using Standard CMR Imaging in Patients with Aortic Stenosis


Abstract
1. Introduction
2. Material and Methods
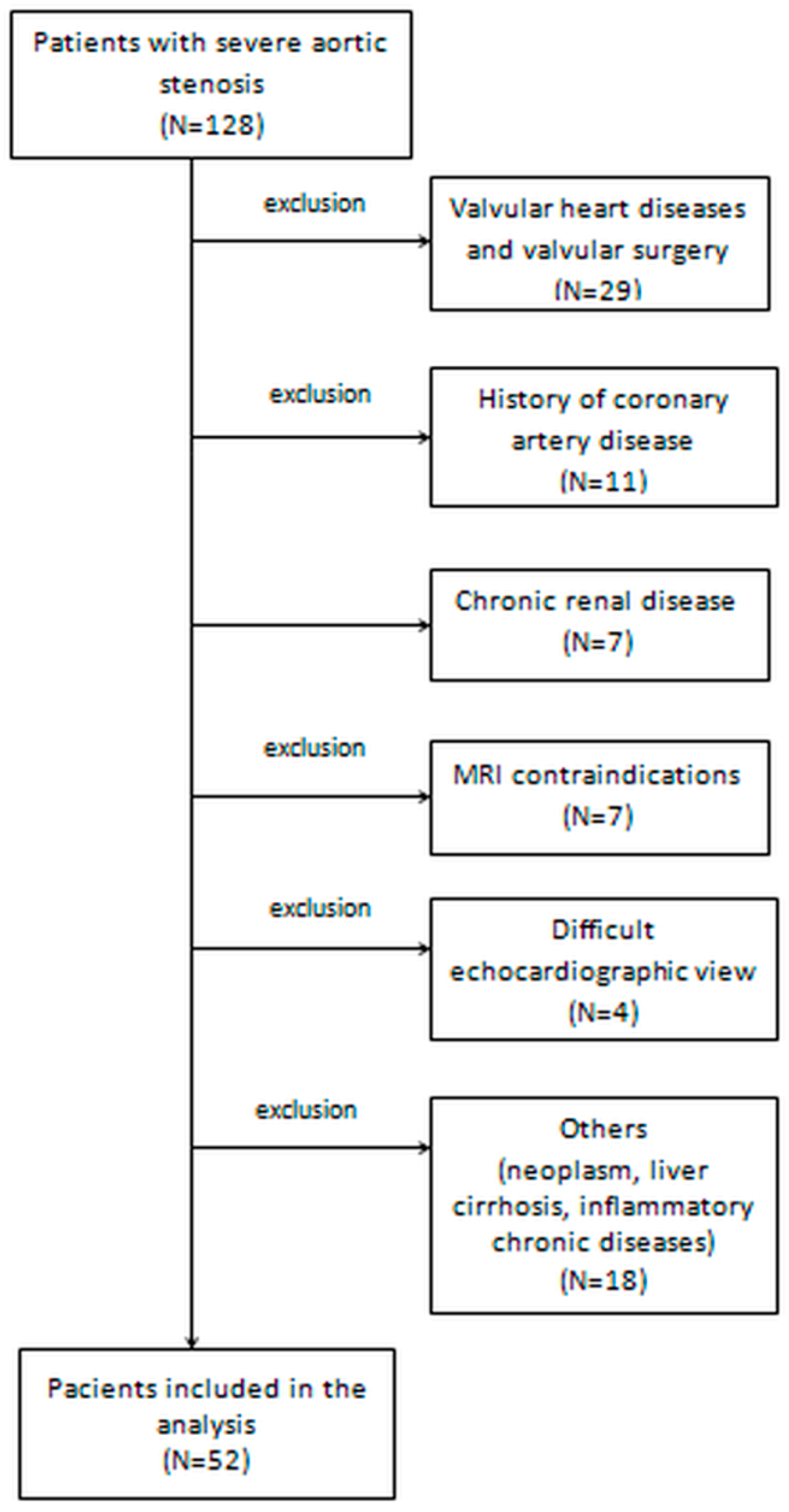
2.1. Study Patients
2.2. Medical History and Clinical Examination
2.3. Biochemical Analysis
2.4. Echocardiography
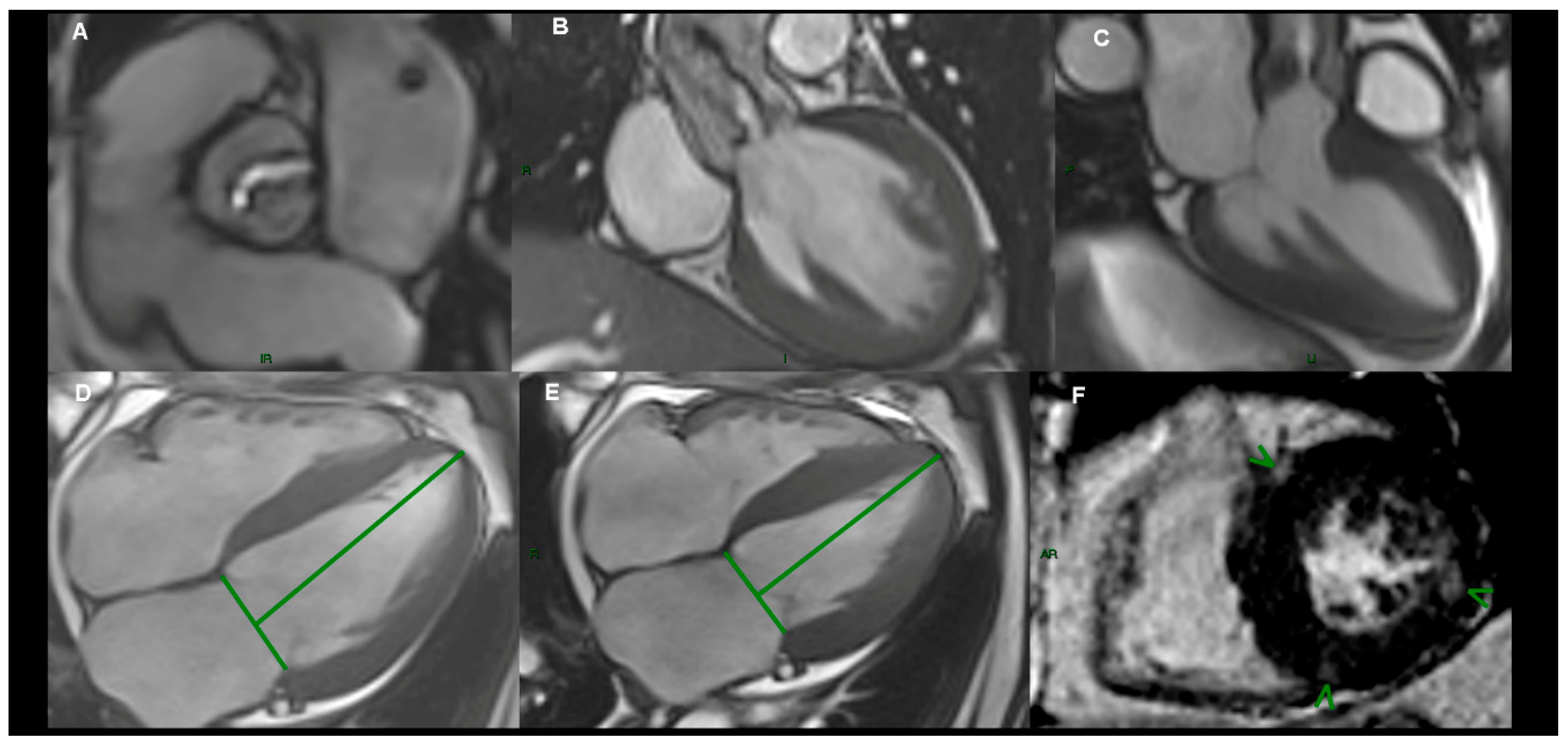
2.5. Cardiac Magnetic Resonance Imaging
2.6. Clinical Outcomes
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Reproducibility of CMR Measurements
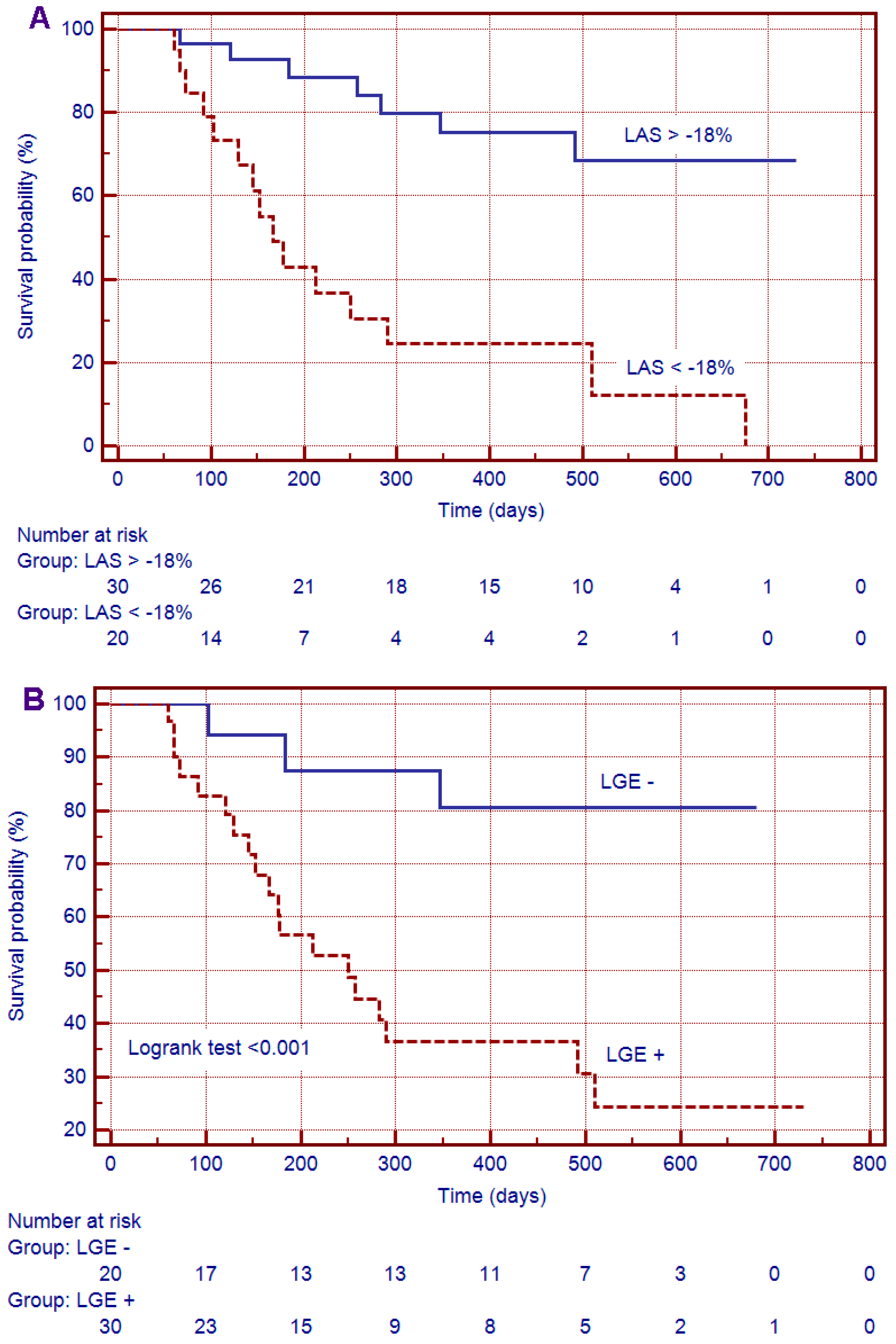
3.3. Survival Analysis
3.4. Uni- and Multivariate Analysis
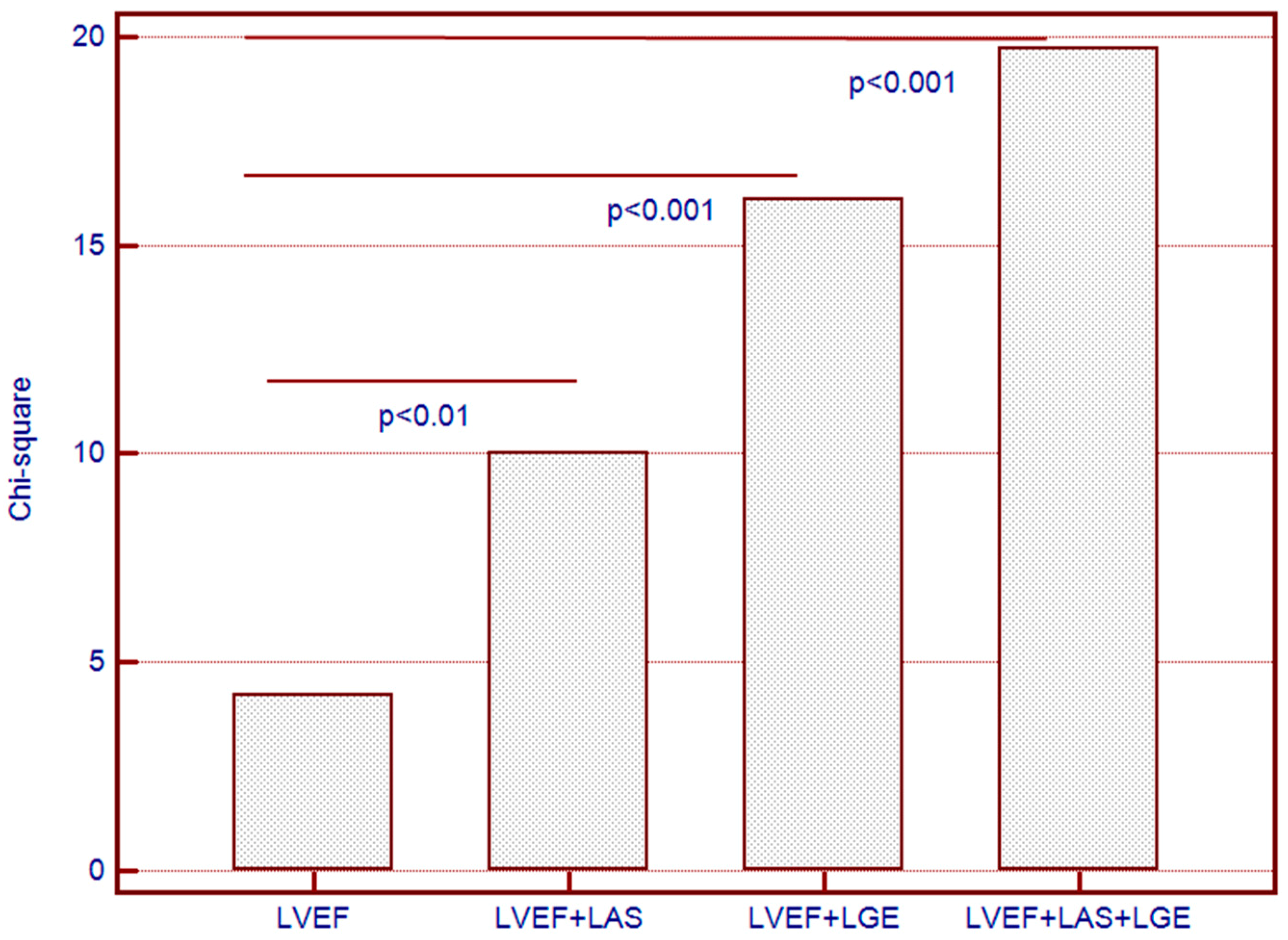
3.5. Incremental Predictive Value for the Combined End-Point
4. Discussion
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Thaden, J.J.; Nkomo, V.T.; Enriquez-Sarano, M. The global burden of aortic stenosis. Prog. Cardiovasc. Dis. 2014, 56, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Ng, A.C.; Delgado, V.; Bertini, M.; Antoni, M.L.; van Bommel, R.J.; van Rijnsoever, E.P.; van der Kley, F.; Ewe, S.H.; Witkowski, T.; Auger, D.; et al. Alterations in multidirectional myocardial functions in patients with aortic stenosis and preserved ejection fraction: A two-dimensional speckle tracking analysis. Eur. Heart J. 2011, 32, 1542–1550. [Google Scholar] [CrossRef] [PubMed]
- Nucifora, G.; Tantiongco, J.P.; Crouch, G.; Bennetts, J.; Sinhal, A.; Tully, P.J.; Bradbrook, C.; Baker, R.A.; Selvanayagam, J.B. Changes of left ventricular mechanics after trans-catheter aortic valve implantation and surgical aortic valve replacement for severe aortic stenosis: A tissue-tracking cardiac magnetic resonance study. Int. J. Cardiol. 2017, 228, 184–190. [Google Scholar] [CrossRef]
- Kupari, M.; Turto, H.; Lommi, J. Left ventricular hypertrophy in aortic valve stenosis: Preventive or promotive of systolic dysfunction and heart failure? Eur. Heart J. 2005, 26, 1790–1796. [Google Scholar] [CrossRef] [PubMed]
- Cioffi, G.; Faggiano, P.; Vizzardi, E.; Tarantini, L.; Cramariuc, D.; Gerdts, E.; de Simone, G. Prognostic effect of inappropriately high left ventricular mass in asymptomatic severe aortic stenosis. Heart 2011, 97, 301–307. [Google Scholar] [CrossRef]
- Natarajan, D.; Prendergast, B. Aortic stenosis—Pathogenesis, prediction of progression, and percutaneous intervention. J. R. Coll. Physicians Edinb. 2017, 47, 172–175. [Google Scholar] [CrossRef]
- Gallego, I.; Beaumont, J.; López, B.; Ravassa, S.; Gómez-Doblas, J.J.; Moreno, M.U.; Valencia, F.; de Teresa, E.; Díez, J.; González, A. Potential role of microRNA-10b down-regulation in cardiomyocyte apoptosis in aortic stenosis patients. Clin. Sci. 2016, 130, 2139–2149. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Llamas, G.; Martín-Rojas, T.; de la Cuesta, F.; Calvo, E.; Gil-Dones, F.; Dardé, V.M.; Lopez-Almodovar, L.F.; Padial, L.R.; Lopez, J.A.; Vivanco, F.; et al. Modification of the secretion pattern of proteases, inflammatory mediators, and extracellular matrix proteins by human aortic valve is key in severe aortic stenosis. Mol. Cell. Proteom. 2013, 12, 2426–2439. [Google Scholar] [CrossRef]
- Kamimura, D.; Suzuki, T.; Fox, E.R.; Skelton, T.N.; Winniford, M.D.; Hall, M.E. Increased left ventricular diastolic stiffness is associated with heart failure symptoms in aortic stenosis patients with preserved ejection fraction. J. Card. Fail. 2017, 23, 81–88. [Google Scholar] [CrossRef]
- Dweck, M.R.; Joshi, S.; Murigu, T.; Alpendurada, F.; Jabbour, A.; Melina, G.; Banya, W.; Gulati, A.; Roussin, I.; Raza, S.; et al. Midwall fibrosis is an independent predictor of mortality in patients with aortic stenosis. J. Am. Coll. Cardiol. 2011, 58, 1271–1279. [Google Scholar] [CrossRef]
- Barone-Rochette, G.; Piérard, S.; De Meester de Ravenstein, C.; Seldrum, S.; Melchior, J.; Maes, F.; Pouleur, A.C.; Vancraeynest, D.; Pasquet, A.; Vanoverschelde, J.L.; et al. Prognostic significance of LGE by CMR in aortic stenosis patients undergoing valve replacement. J. Am. Coll. Cardiol. 2014, 64, 144–154. [Google Scholar] [CrossRef] [PubMed]
- Milano, A.D.; Faggian, G.; Dodonov, M.; Golia, G.; Tomezzoli, A.; Bortolotti, U.; Mazzucco, A. Prognostic value of myocardial fibrosis in patients with severe aortic valve stenosis. J. Thorac. Cardiovasc. Surg. 2012, 144, 830–837. [Google Scholar] [CrossRef] [PubMed]
- Thavendiranathan, P.; Grant, A.D.; Negishi, T.; Plana, J.C.; Popović, Z.B.; Marwick, T.H. Reproducibility of echocardiographic techniques for sequential assessment of left ventricular ejection fraction and volumes: Application to patients undergoing cancer chemotherapy. J. Am. Coll. Cardiol. 2013, 61, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Thavendiranathan, P.; Popović, Z.B.; Flamm, S.D.; Dahiya, A.; Grimm, R.A.; Marwick, T.H. Improved interobserver variability and accuracy of echocardiographic visual left ventricular ejection fraction assessment through a self directed learning program using cardic magnetic resonance images. J. Am. Soc. Echocardiogr. 2013, 26, 1267–1273. [Google Scholar] [CrossRef] [PubMed]
- Delgado, V.; Tops, L.F.; van Bommel, R.J.; van der Kley, F.; Marsan, N.A.; Klautz, R.J.; Versteegh, M.I.; Holman, E.R.; Schalij, M.J.; Bax, J.J. Strain analysis in patients with severe aortic stenosis and preserved left ventricular ejection fraction undergoing surgical valve replacement. Eur. Heart J. 2009, 30, 3037–3047. [Google Scholar] [CrossRef] [PubMed]
- Naji, P.; Shah, S.; Svensson, L.G.; Gillinov, A.M.; Johnston, D.R.; Rodriguez, L.L.; Grimm, R.A.; Griffin, B.P.; Desai, M.Y. Incremental prognostic use of left ventricular global longitudinal strain in asymptomatic/minimally symptomatic patients with severe bioprosthetic aortic stenosis undergoing redo aortic valve replacement. Circ. Cardiovasc. Imaging 2017, 10, e005942. [Google Scholar] [CrossRef] [PubMed]
- Azevedo, C.F.; Nigri, M.; Higuchi, M.L.; Pomerantzeff, P.M.; Spina, G.S.; Sampaio, R.O.; Tarasoutchi, F.; Grinberg, M.; Rochitte, C.E. Prognostic significance of myocardial fibrosis quantification by histopathology and magnetic resonance imaging in patients with severe aortic valve disease. J. Am. Coll. Cardiol. 2010, 56, 278–287. [Google Scholar] [CrossRef]
- Arenja, N.; Riffel, J.H.; Fritz, T.; André, F.; Aus dem Siepen, F.; Mueller-Hennessen, M.; Giannitsis, E.; Katus, H.A.; Friedrich, M.G.; Buss, S.J. Diagnostic and prognostic value of long axis strain and myocardial contraction fraction using standard cardiovascular MR Imaging in patients with nonischemic dilated cardiomyopathies. Radiology 2017, 283, 681–691. [Google Scholar] [CrossRef]
- Nishimura, R.A.; Otto, C.M.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., III; Guyton, R.A.; O’Gara, P.T.; Ruiz, C.E.; Skubas, N.J.; Sorajja, P.; et al. 2014 AHA/ACC Guideline for the management of patients with valvular heart disease: Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014, 129, 2440–2492. [Google Scholar] [CrossRef]
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Muñoz, D.R.; et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease: The Task Force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2017, 38, 2739–2791. [Google Scholar] [CrossRef]
- Paparella, D.; Guida, P.; Di Eusanio, G.; Caparrotti, S.; Gregorini, R.; Cassese, M.; Fanelli, V.; Speziale, G.; Mazzei, V.; Zaccaria, S.; et al. Risk stratification for in-hospital mortality after cardiac surgery: External validation of EuroSCORE II in a prospective regional registry. Eur. J. Cardiothorac. Surg. 2014, 46, 840–888. [Google Scholar] [CrossRef] [PubMed]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., III; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39. [Google Scholar] [CrossRef]
- American Heart Association Writing Group on Myocardial Segmentation and Registration for Cardiac Imaging; Cerqueira, M.D.; Weissman, N.J.; Dilsizian, V.; Jacobs, A.K.; Kaul, S.; Laskey, W.K.; Pennell, D.J.; Rumberger, J.A.; Ryan, T.; et al. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. Circulation 2002, 105, 539–542. [Google Scholar] [PubMed]
- Motoki, H.; Borowski, A.G.; Shrestha, K.; Troughton, R.W.; Tang, W.H.; Thomas, J.D.; Klein, A.L. Incremental prognostic value of assessing left ventricular myocardial mechanics in patients with chronic systolic heart failure. J. Am. Coll. Cardiol. 2012, 60, 2074–2081. [Google Scholar] [CrossRef] [PubMed]
- Stanton, T.; Leano, R.; Marwick, T.H. Prediction of all-cause mortality from global longitudinal speckle strain: Comparison with ejection fraction and wall motion scoring. Circ. Cardiovasc. Imaging 2009, 2, 356–364. [Google Scholar] [CrossRef] [PubMed]
- Kalam, K.; Otahal, P.; Marwick, T.H. Prognostic implications of global LV dysfunction: A systematic review and meta-analysis of global longitudinal strain and ejection fraction. Heart 2014, 100, 1673–1680. [Google Scholar] [CrossRef]
- Obokata, M.; Nagata, Y.; Wu, V.C.; Kado, Y.; Kurabayashi, M.; Otsuji, Y.; Takeuchi, M. Direct comparison of cardiac magnetic resonance feature tracking and 2D/3D echocardiography speckle tracking for evaluation of global left ventricular strain. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 525–532. [Google Scholar] [CrossRef]
- Onishi, T.; Saha, S.K.; Delgado-Montero, A.; Ludwig, D.R.; Onishi, T.; Schelbert, E.B.; Schwartzman, D.; Gorcsan, J., III. Global longitudinal strain and global circumferential strain by speckle-tracking echocardiography and feature-tracking cardiac magnetic resonance imaging: Comparison with left ventricular ejection fraction. J. Am. Soc. Echocardiogr. 2015, 28, 587–596. [Google Scholar] [CrossRef]
- Bourfiss, M.; Vigneault, D.M.; Aliyari Ghasebeh, M.; Murray, B.; James, C.A.; Tichnell, C.; Hoesein, F.A.; Zimmerman, S.L.; Kamel, I.R.; Calkins, H.; et al. Feature tracking CMR reveals abnormal strain in preclinical arrhythmogenic right ventricular dysplasia, cardiomyopathy: A multisoftware feasibility and clinical implementation study. J. Cardiovasc. Magn. Reson. 2017, 19, 66. [Google Scholar] [CrossRef]
- Li, R.; Yang, Z.G.; Xu, H.Y.; Shi, K.; Liu, X.; Diao, K.Y.; Guo, Y.K. Myocardial deformation in cardiac amyloid light-chain amyloidosis: Assessed with 3T cardiovascular magnetic resonance feature tracking. Sci. Rep. 2017, 7, 3794. [Google Scholar] [CrossRef] [PubMed]
- Al Musa, T.; Uddin, A.; Swoboda, P.P.; Garg, P.; Fairbairn, T.A.; Dobson, L.E.; Steadman, C.D.; Singh, A.; Erhayiem, B.; Plein, S.; et al. Myocardial strain and symptom severity in severe aortic stenosis: Insights from cardiovascular magnetic resonance. Quant. Imaging Med. Surg. 2017, 7, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Weidemann, F.; Herrmann, S.; Störk, S.; Niemann, M.; Frantz, S.; Lange, V.; Beer, M.; Gattenlöhner, S.; Voelker, W.; Ertl, G.; et al. Impact of myocardial fibrosis in patients with symptomatic severe aortic stenosis. Circulation 2009, 120, 577–584. [Google Scholar] [CrossRef] [PubMed]
- Kupari, M.; Laine, M.; Turto, H.; Lommi, J.; Werkkala, K. Circulating collagen metabolites, myocardial fibrosis and heart failure in aortic valve stenosis. J. Heart Valve Dis. 2013, 22, 166–176. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Test Group | Control Group | p-Value | |
|---|---|---|---|
| Clinical characteristics | n = 52 | n = 52 | |
| Age, years | 66 (7.5) | 66 (7.8) | NS |
| Male gender, n (%) | 29 (55.7) | 29 (55.7) | NS |
| Body surface area, m2 | 1.90 (0.24) | 1.97 (0.13) | NS |
| Body-mass index, kg/m2 | 28.5 (4.1) | 30.2 (4.9) | NS |
| Heart rate, bpm | 73 (11.6) | 72 (8.6) | NS |
| Systolic blood pressure, mmHg | 132 (18.1) | 133 (20.3) | NS |
| Hypertension, n (%) | 37 (71.1) | 28 (53.8) | NS |
| Diabetes mellitus, n (%) | 22 (42.3) | 14 (26.9) | <0.01 |
| Dyslipidemia, n (%) | 35 (67.3) | 24 (46.1) | NS |
| Smoking, n (%) | 19 (36.5) | 13 (25) | NS |
| 6MWD, m | 406 (138.1) | 592 (103.9) | <0.001 |
| Coronary artery disease, n (%) | 18 (32.6) | ||
| Chronic obstructive lung disease, n (%) | 7 (11.5) | ||
| Peripheral vascular disease, n (%) | 27 (51.9) | ||
| NYHA functional class ≥ III, n (%) | 15 (28.8) | ||
| Logistic EuroScore, % | 3.8 (1.3–5.9) | ||
| Medications | |||
| β-blockers, n (%) | 40 (76.9) | 14 (26.9) | <0.001 |
| ACEIs or ARBs, n (%) | 45 (86.5) | 10 (19.2) | <0.001 |
| Calcium channel blockers, n (%) | 6 (11.5) | 13 (25) | <0.01 |
| Statins, n (%) | 38 (73) | 15 (28.8) | <0.001 |
| ASA or other antiplatelet therapy, n (%) | 32 (61.5) | 13 (34.6) | <0.01 |
| Diuretics, n (%) | 37 (71.1) | 5 (9.6) | <0.001 |
| Echocardiography | |||
| Peak aortic velocity, m/s | 4.45 (0.47) | 1.31 (0.36) | <0.001 |
| Peak transaortic gradient, mmHg | 82.1 (17.9) | 7.2 (2.7) | <0.001 |
| Mean transaortic gradient, mmHg | 52.9 (14.7) | 3.6 (0.75) | <0.001 |
| AVA index, cm2/m2 | 0.52 (0.08) | 2.9 (0.08) | <0.001 |
| E/E’ ratio | 9.8 (3.2) | 6.5 (0.8) | <0.001 |
| DT, ms | 223 (52.2) | 185 (8.8) | <0.001 |
| sPAP, mmHg | 33.4 (7.3) | 26.2 (7.2) | NS |
| Cardiovascular magnetic resonance | |||
| LVEDV index, mL/m2 | 82.4 (21.6) | 61.8 (15.0) | <0.001 |
| LVESV index, mL/m2 | 35.7 (16.6) | 20.9 (5.8) | <0.001 |
| LVM index, g/m2 | 96.2 (24.3) | 62.1 (16.5) | <0.001 |
| LVEF, % | 58.4 (9.7) | 66.1 (4.7) | <0.001 |
| LVM/LVEDV, g/mL | 1.22 (0.35) | 1.04 (0.29) | <0.01 |
| LAV index, mL/m2 | 49.1 (11.6) | 25.5 (3.7) | <0.001 |
| LAS (%) | −17.7 (3.9) | −20.5 (1.5) | <0.001 |
| TAPSE, mm | 14.9 (2.5) | 19.8 (3.6) | <0.001 |
| LGE, n (%) | 30 (57.7) | ||
| Biomarker levels | |||
| PICP, ng/mL, IQR | 1.2 (0.37–7.3) | 0.42 (0.38–4.6) | <0.001 |
| PIIINP, ng/mL, IQR | 13.6 (2.5–68.3) | 9.7 (2.4–29.7) | <0.01 |
| hs-CRP, pg/mL, IQR | 1.1 (0.49–1.9) | 0.74 (0.16–1.1) | <0.001 |
| NT-proBNP, pg/mL, IQR | 1960 (170–9893) | 210 (60–390) | <0.001 |
| eGFR, ml/min/1.73 m2 | 88.1 (24.1) | 89.2 (19.6) | NS |
| Parameter | Coefficient Kappa | 95% Confidence Interval | Standard Error |
|---|---|---|---|
| Inter-reader | |||
| LVEF | 0.95 | 0.907 to 0.974 | 0.023 |
| LAS | 0.93 | 0.912 to 0.962 | 0.027 |
| LGE | 0.89 | 0.795 to 0.940 | 0.078 |
| Intra-reader | |||
| LVEF | 0.99 | 0.989 to 0.998 | 0.002 |
| LAS | 0.96 | 0.953 to 0.985 | 0.014 |
| LGE | 0.91 | 0.905 to 0.942 | 0.033 |
| Variables | Sensibility | Specificity | PPV | NPV | ROC Threshold | AUC |
|---|---|---|---|---|---|---|
| LVEF | 0.67 | 0.90 | 0.87 | 0.73 | <50 | 0.759 |
| LGE | 0.75 | 0.68 | 0.66 | 0.76 | + | 0.717 |
| LAS | 0.77 | 0.90 | 0.85 | 0.84 | <−18 | 0.883 |
| PICP | 0.56 | 0.73 | 0.64 | 0.67 | >0.84 | 0.535 |
| PIIINP | 0.50 | 0.79 | 0.67 | 0.65 | >16.1 | 0.572 |
| No Events n = 30 | Events n = 22 | Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|---|---|
| Unadjusted HR (95% CI) | p Value | Adjusted HR (95% CI) | p Value | |||
| Age, years | 66 (10.1) | 68 (7.1) | 1.02 (0.95–1.09) | NS | ||
| Male gender, n, % | 14 (46.6) | 15 (68.1) | 0.40 (0.12–1.28) | NS | ||
| Body surface area, m2 | 1.91 (0.27) | 1.89 (0.20) | 0.76 (0.08–7.20) | NS | ||
| Systolic blood pressure | 131 (10.5) | 133 (15.2) | 1.00 (0.97–1.03) | NS | ||
| PICP, ng/mL, IQR | 1.2 (0.37–5.0) | 0.81 (0.38–7.3) | 1.06 (0.76–1.49) | NS | ||
| PIIINP, ng/mL, IQR | 10.5 (6.4–68.3) | 14.1 (2.5–56.8) | 1.01 (0.97–1.06) | NS | ||
| hs-CRP, pg/mL | 1.1 (0.49–1.9) | 0.94 (0.51–1.8) | 0.18 (0.03–0.95) | NS | ||
| NT-proBNP, pg/mL | 2206 (170–6735) | 2734 (234–9893) | 1.00 (0.99–1.01) | NS | ||
| eGFR, ml/min/1.73 m2 | 91.9 (25.4) | 88.5 (22.6) | 0.99 (0.97–1.01) | NS | ||
| 6MWD, m | 455 (129) | 340 (122) | 0.99 (0.98–1.00) | 0.001 | 0.99 (0.98–1.00) | NS |
| LVEDV index, mL/m2 | 75.3 (20.9) | 92.1 (18.8) | 1.02 (0.99–1.06) | <0.05 | ||
| LVESV index, mL/m2 | 29.9 (13.3) | 43.6 (17.8) | 1.04 (1.01–1.08) | <0.05 | ||
| LVM index, g/m2 | 93.2 (25.4) | 100.3 (22.5) | 1.01 (0.98–1.03) | NS | ||
| LVEF, % | 61.6 (7.9) | 54.1 (10.5) | 0.93 (0.87–0.99) | <0.01 | 0.97 (0.88–1.07) | NS |
| LAV index, mL/m2 | 49.8 (11.8) | 48.2 (11.6) | 0.98 (0.94–1.03) | NS | ||
| LVM/LVEDV, g/mL | 1.29 (0.36) | 1.12 (0.31) | 0.23 (0.04–1.27) | NS | ||
| LGE, n (%) | 12 (40) | 17 (77.2) | 5.55 (1.50–20.5) | <0.001 | 9.86 (1.77–54.0) | <0.01 |
| LAS (%) | −19.6 (3.1) | −15.1 (3.3) | 1.29 (1.07–1.55) | <0.001 | 1.32 (1.01–1.71) | <0.01 |
| TAPSE, mm | 19.3 (3.1) | 20.4 (4.3) | 1.08 (0.93–1.26) | NS | ||
| E/E’ ratio | 8.9 (1.9) | 11.1 (4.1) | 1.25 (1.02–1.53) | <0.01 | 1.36 (0.98–1.88) | NS |
| Peak aortic velocity, m/s | 4.35 (0.33) | 4.59 (0.59) | 3.18 (0.84–11.9) | NS | ||
| Peak aortic gradient, mmHg | 78.7 (12.9) | 86.9 (22.6) | 1.02 (0.99–1.06) | NS | ||
| Mean aortic gradient, mmHg | 51.5 (12.5) | 54.7 (17.4) | 1.01 (0.97–1.05) | NS | ||
| AVA index, cm2/m2 | 0.52 (0.08) | 0.51 (0.08) | 0.17 (0.08–0.98) | NS | ||
| Variables | Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 |
|---|---|---|---|---|---|---|
| HR 95% | HR 95% | HR 95% | HR 95% | HR 95% | HR 95% | |
| Age | 1.01 (0.95–1.08) | 0.96 (0.89–1.03) | 1.01 (0.95–1.08) | 1.00 (0.95–1.06) | 1.00 (0.95–1.06) | 1.01 (0.96–1.07) |
| 6MWD | 0.99 (0.98–1.00) | |||||
| E/E’ | 1.24 (1.01–1.54) ** | |||||
| LVEF | 0.94 (0.88–1.01) | |||||
| LAS | 1.33 (1.01–1.74) ** | |||||
| LGE | 11.3 (1.82–70.2) * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agoston-Coldea, L.; Bheecarry, K.; Cionca, C.; Petra, C.; Strimbu, L.; Ober, C.; Lupu, S.; Fodor, D.; Mocan, T. Incremental Predictive Value of Longitudinal Axis Strain and Late Gadolinium Enhancement Using Standard CMR Imaging in Patients with Aortic Stenosis. J. Clin. Med. 2019, 8, 165. https://doi.org/10.3390/jcm8020165
Agoston-Coldea L, Bheecarry K, Cionca C, Petra C, Strimbu L, Ober C, Lupu S, Fodor D, Mocan T. Incremental Predictive Value of Longitudinal Axis Strain and Late Gadolinium Enhancement Using Standard CMR Imaging in Patients with Aortic Stenosis. Journal of Clinical Medicine. 2019; 8(2):165. https://doi.org/10.3390/jcm8020165
Chicago/Turabian StyleAgoston-Coldea, Lucia, Kunal Bheecarry, Carmen Cionca, Cristian Petra, Lelia Strimbu, Camelia Ober, Silvia Lupu, Daniela Fodor, and Teodora Mocan. 2019. "Incremental Predictive Value of Longitudinal Axis Strain and Late Gadolinium Enhancement Using Standard CMR Imaging in Patients with Aortic Stenosis" Journal of Clinical Medicine 8, no. 2: 165. https://doi.org/10.3390/jcm8020165
APA StyleAgoston-Coldea, L., Bheecarry, K., Cionca, C., Petra, C., Strimbu, L., Ober, C., Lupu, S., Fodor, D., & Mocan, T. (2019). Incremental Predictive Value of Longitudinal Axis Strain and Late Gadolinium Enhancement Using Standard CMR Imaging in Patients with Aortic Stenosis. Journal of Clinical Medicine, 8(2), 165. https://doi.org/10.3390/jcm8020165