Temporal Trends of Severe Hypoglycemia and Subsequent Mortality in Patients with Advanced Diabetic Kidney Diseases Transitioning to Dialysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Patient Selection and Definition of Dialysis Modality
2.3. Outcome Variables
2.4. Baseline Characteristics
2.5. Statistical Analysis
3. Results
3.1. Subject Characteristics
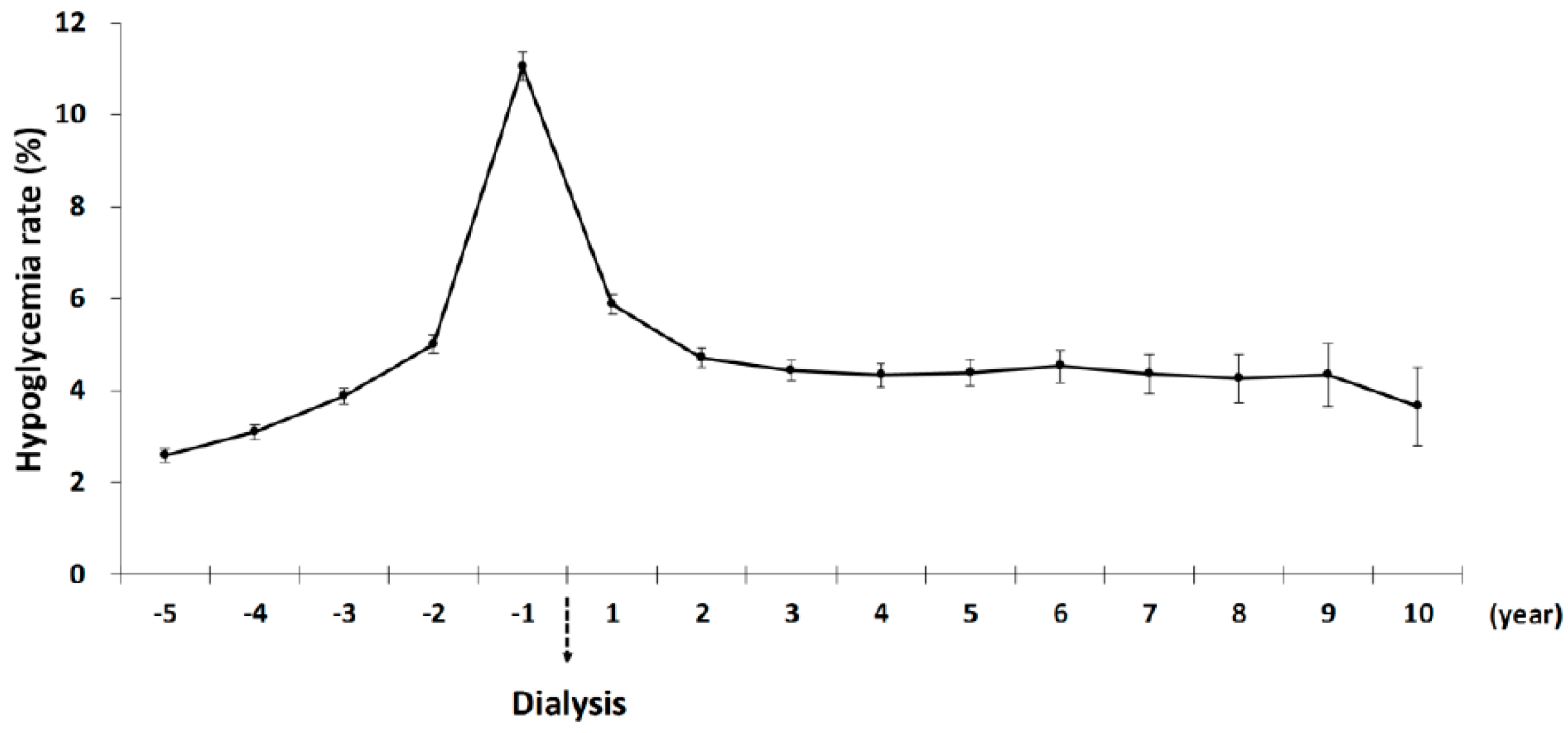
3.2. Temporal Trends of Hypoglycemia in Advanced DKD Patients Transitioning to Dialysis
3.3. Comparison of Hypoglycemic Rates between the HD and PD Cohorts
3.4. Risk Factors of One-Year Severe Hypoglycemia among Advanced DKD Patients after Transitioning to Dialysis
3.5. Risk Factors of One-Year Mortality among DKD Patients Transitioning to Dialysis
4. Discussion
4.1. Trajectory of Severe Hypoglycemia over the Dialysis Transition Period
4.2. One-Year Mortality after Dialysis
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Kdoqi. Clinical practice guidelines and clinical practice recommendations for diabetes and chronic kidney disease. Am. J. Kidney Dis. 2007, 49, S12–S154. [Google Scholar] [CrossRef]
- Zoungas, S.; Patel, A.; Chalmers, J.; de Galan, B.E.; Li, Q.; Billot, L.; Woodward, M.; Ninomiya, T.; Neal, B.; MacMahon, S.; et al. Severe hypoglycemia and risks of vascular events and death. N. Engl. J. Med. 2010, 363, 1410–1418. [Google Scholar] [CrossRef] [PubMed]
- Bonds, D.E.; Miller, M.E.; Bergenstal, R.M.; Buse, J.B.; Byington, R.P.; Cutler, J.A.; Dudl, R.J.; Ismail-Beigi, F.; Kimel, A.R.; Hoogwerf, B.; et al. The association between symptomatic, severe hypoglycaemia and mortality in type 2 diabetes: Retrospective epidemiological analysis of the ACCORD study. BMJ 2010, 340, b4909. [Google Scholar] [CrossRef] [PubMed]
- Abe, M.; Kalantar-Zadeh, K. Haemodialysis-induced hypoglycaemia and glycaemic disarrays. Nat. Rev. Nephrol. 2015, 11, 302. [Google Scholar] [CrossRef] [PubMed]
- Gosmanov, A.R.; Gosmanova, E.O.; Kovesdy, C.P. Evaluation and management of diabetic and non-diabetic hypoglycemia in end-stage renal disease. Nephrol. Dial. Transplant. 2015, 31, 8–15. [Google Scholar] [CrossRef] [Green Version]
- Moen, M.F.; Zhan, M.; Hsu, V.D.; Walker, L.D.; Einhorn, L.M.; Seliger, S.L.; Fink, J.C. Frequency of hypoglycemia and its significance in chronic kidney disease. Clin. J. Am. Soc. Nephrol. 2009, 4, 1121–1127. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Kopple, J.D.; Regidor, D.R.; Jing, J.; Shinaberger, C.S.; Aronovitz, J.; McAllister, C.J.; Whellan, D.; Sharma, K. A1C and survival in maintenance hemodialysis patients. Diabetes Care 2007, 30, 1049–1055. [Google Scholar] [CrossRef]
- Robinson, R.T.C.E.; Harris, N.D.; Ireland, R.H.; Lee, S.; Newman, C.; Heller, S.R. Mechanisms of abnormal cardiac repolarization during insulin-induced hypoglycemia. Diabetes 2003, 52, 1469–1474. [Google Scholar]
- Lukowsky, L.R.; Kheifets, L.; Arah, O.A.; Nissenson, A.R.; Kalantar-Zadeh, K. Patterns and predictors of early mortality in incident hemodialysis patients: New insights. Am. J. Nephrol. 2012, 35, 548–558. [Google Scholar] [CrossRef]
- Saran, R.; Robinson, B.; Abbott, K.C.; Agodoa, L.Y.C.; Albertus, P.; Ayanian, J.; Balkrishnan, R.; Bragg-Gresham, J.; Cao, J.; Chen, J.L.T.; et al. US renal data system 2016 annual data report: Epidemiology of kidney disease in the United States. Am. J. Kidney Dis. 2017, 69, A7–A8. [Google Scholar] [CrossRef]
- Wu, C.S.; Lai, M.S.; Gau, S.S.; Wang, S.C.; Tsai, H.J. Concordance between patient self-reports and claims data on clinical diagnoses, medication use, and health system utilization in Taiwan. PloS ONE 2014, 9, e112257. [Google Scholar] [CrossRef]
- Hsieh, C.Y.; Chen, C.H.; Li, C.Y.; Lai, M.L. Validating the diagnosis of acute ischemic stroke in a National Health Insurance claims database. J. Formos. Med. Assoc. 2015, 114, 254–259. [Google Scholar] [CrossRef]
- Austin, P.C. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat. Med. 2009, 28, 3083–3107. [Google Scholar] [CrossRef] [Green Version]
- Snyder, R.W.; Berns, J.S. Use of insulin and oral hypoglycemic medications in patients with diabetes mellitus and advanced kidney disease. Semin. Dial. 2004, 17, 365–370. [Google Scholar] [CrossRef]
- Biesenbach, G.; Raml, A.; Schmekal, B.; Eichbauer-Sturm, G. Decreased insulin requirement in relation to GFR in nephropathic Type 1 and insulin-treated Type 2 diabetic patients. Diabete Med. 2003, 20, 642–645. [Google Scholar]
- Papademetriou, V.; Lovato, L.; Doumas, M.; Nylen, E.; Mottl, A.; Cohen, R.M.; Applegate, W.B.; Puntakee, Z.; Yale, J.F.; Cushman, W.C.; et al. Chronic kidney disease and intensive glycemic control increase cardiovascular risk in patients with type 2 diabetes. Kidney Int. 2015, 87, 649–659. [Google Scholar] [CrossRef]
- Horton, E.S.; Johnson, C.; Lebovitz, H.E. Carbohydrate metabolism in uremia. Ann. Int. Med. 1986, 68, 63–74. [Google Scholar]
- Robinson, B.M.; Zhang, J.; Morgenstern, H.; Bradbury, B.D.; Ng, L.J.; McCullough, K.P.; Gillespie, B.W.; Hakim, R.; Rayner, H.; Fort, J.; et al. Worldwide, mortality risk is high soon after initiation of hemodialysis. Kidney Int. 2014, 85, 158–165. [Google Scholar] [CrossRef]
- Noordzij, M.; Jager, K.J. Increased mortality early after dialysis initiation: A universal phenomenon. Kidney Int. 2014, 85, 12–14. [Google Scholar] [CrossRef]
- Murray, A.M.; Seliger, S.; Lakshminarayan, K.; Herzog, C.A.; Solid, C.A. Incidence of stroke before and after dialysis initiation in older patients. J. Am. Soc. Nephrol. JASN 2013, 24, 1166–1173. [Google Scholar] [CrossRef]
- Borzi, V.; Frasson, S.; Gussoni, G.; Lillo, M.D.; Gerloni, R.; Augello, G.; Gulli, G.; Ceriello, A.; Solerte, B.; Bonizzoni, E.; et al. Risk factors for hypoglycemia in patients with type 2 diabetes, hospitalized in internal medicine wards: Findings from the FADOI-DIAMOND study. Diabetes Res. Clin. Pract. 2016, 115, 24–30. [Google Scholar] [CrossRef]
- Reilly, J.B.; Berns, J.S. Selection and dosing of medications for management of diabetes in patients with advanced kidney disease. Semin. Dial. 2010, 23, 163–168. [Google Scholar] [CrossRef]
- Charpentier, G.; Riveline, J.P.; Varroud-Vial, M. Management of drugs affecting blood glucose in diabetic patients with renal failure. Diabetes Metab. 2000, 26, 73–85. [Google Scholar]
- McCaleb, M.L.; Izzo, M.S.; Lockwood, D.H. Characterization and partial purification of a factor from uremic human serum that induces insulin resistance. J. Clin. Investig. 1985, 75, 391–396. [Google Scholar] [CrossRef]
- Haneda, M.; Morikawa, A. Which hypoglycaemic agents to use in type 2 diabetic subjects with CKD and how? Nephrol. Dial. Transplant. 2009, 24, 338–341. [Google Scholar] [CrossRef]
- Holstein, A.; Plaschke, A.; Hammer, C.; Egberts, E.H. Characteristics and time course of severe glimepiride- versus glibenclamide-induced hypoglycaemia. Eur. J. Clin. Pharmacol. 2003, 59, 91–97. [Google Scholar] [CrossRef]
- Kong, A.P.S.; Yang, X.; Luk, A.; Ma, R.C.W.; So, W.Y.; Ozaki, R.; Ting, R.; Cheung, K.; Ho, C.S.; Chan, M.H.M.; et al. Severe hypoglycemia identifies vulnerable patients with type 2 diabetes at risk for premature death and all-site cancer: the Hong Kong diabetes registry. Diabetes Care 2014, 37, 1024–1031. [Google Scholar] [CrossRef]
- De Ferrari, G.M.; Sanzo, A.; Bertoletti, A.; Specchia, G.; Vanoli, E.; Schwartz, P.J. Baroreflex sensitivity predicts long-term cardiovascular mortality after myocardial infarction even in patients with preserved left ventricular function. J. Am. Coll. Cardiol. 2007, 50, 2285–2290. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Before Propensity Score Weighting | After Propensity Score Weighting | |||||
|---|---|---|---|---|---|---|
| HD | PD | ASMD | HD | PD | ASMD | |
| (n = 42,563) | (n = 4216) | (n = 42,563) | (n = 4216) | |||
| Age (years) | 65.83 ± 11.55 | 60.38 ± 12.89 | 0.4452 | 60.45 ± 3.96 | 60.38 ± 12.89 | 0.0072 |
| Male | 49.25% | 50.62% | 0.0274 | 50.76% | 50.62% | 0.0029 |
| Stroke | 43.93% | 33.37% | 0.2181 | 33.53% | 33.37% | 0.0032 |
| CAD | 57.63% | 48.58% | 0.1821 | 51.26% | 48.58% | 0.0033 |
| CHF | 61.32% | 49.95% | 0.2302 | 50.11% | 49.95% | 0.0032 |
| Hyperlipidemia | 73.73% | 75.88% | 0.0494 | 75.85% | 75.88% | 0.0006 |
| AF | 7.77% | 6.95% | 0.0314 | 6.98% | 6.95% | 0.0012 |
| Hypertension | 96.97% | 95.66% | 0.0696 | 95.69% | 95.66% | 0.0014 |
| LC | 17.57% | 14.54% | 0.0826 | 14.56% | 14.54% | 0.0006 |
| Use of sulfonylurea | 62.86% | 55.03% | 0.1598 | 55.27% | 55.03% | 0.0048 |
| Use of TZD | 21.45% | 22.06% | 0.0147 | 22.19% | 22.06% | 0.0031 |
| Use of glinide | 40.91% | 38.14% | 0.0567 | 38.32% | 38.14% | 0.0037 |
| Use of DPP4 | 5.52% | 6.19% | 0.0287 | 6.2% | 6.19% | 0.0004 |
| Use of acarbose | 27.79% | 27.35% | 0.0099 | 27.53% | 27.35% | 0.0042 |
| Use of insulin | 73.9% | 68.15% | 0.1272 | 68.29% | 68.15% | 0.0031 |
| One Year | ||||||
|---|---|---|---|---|---|---|
| Univariate | Multivariate | |||||
| HR | (95% CI) | p Value | HR | (95% CI) | p Value | |
| Dialysis (HD vs. PD) | 1.40 | (1.2–1.64) | <0.0001 | 1.29 | (1.12–1.30) | 0.0017 |
| Male | 0.96 | (0.88–1.03) | 0.2651 | -- | -- | -- |
| Age (65+ vs. <65) | 1.03 | (0.95–1.11) | 0.4996 | -- | -- | -- |
| Stroke | 1.21 | (1.12–1.31) | <0.0001 | 1.16 | (1.07–1.25) | 0.0003 |
| CAD | 1.05 | (0.97–1.14) | 0.2391 | -- | -- | -- |
| CHF | 1.10 | (1.01–1.19) | 0.0234 | -- | -- | -- |
| Hyperlipidemia | 0.91 | (0.84–1.00) | 0.0415 | 0.85 | (0.78–0.93) | 0.0003 |
| AF | 1.00 | (0.87–1.14) | 0.9799 | -- | -- | -- |
| Hypertension | 0.81 | (0.65–1.02) | 0.0666 | 0.67 | (0.54–0.85) | 0.0007 |
| LC | 1.01 | (0.91–1.12) | 0.8813 | -- | -- | -- |
| sulfonylurea | 1.58 | (1.44–1.72) | <0.0001 | 1.31 | (1.20–1.44) | <0.0001 |
| TZD | 1.23 | (1.12–1.34) | <0.0001 | -- | -- | -- |
| Glinide | 1.42 | (1.31–1.54) | <0.0001 | 1.20 | (1.10–1.30) | <0.0001 |
| DPP4 | 1.02 | (0.86–1.2) | 0.8644 | -- | -- | -- |
| Acarbose | 1.26 | (1.16–1.37) | <0.0001 | -- | -- | -- |
| Insulin | 2.88 | (2.55–3.26) | <0.0001 | 2.63 | (2.32–2.98) | <0.0001 |
| One Year | ||||||
|---|---|---|---|---|---|---|
| Multivariate Model 1 | Multivariate Model 2 | |||||
| HR | (95% CI) | p Value | HR | (95% CI) | p Value | |
| Dialysis (HD vs. PD) | 1.64 | (1.44–1.87) | <0.0001 | 1.66 | (1.46–1.89) | <0.0001 |
| Male | -- | -- | -- | -- | -- | -- |
| Age (65+ vs. <65) | 2.21 | (2.07–2.36) | <0.0001 | 2.19 | (2.05–2.33) | <0.0001 |
| Stroke | 1.39 | (1.31–1.47) | <0.0001 | 1.40 | (1.32–1.48) | <0.0001 |
| CAD | 0.94 | (0.88–1.00) | 0.0487 | -- | -- | -- |
| CHF | 1.16 | (1.09–1.24) | <0.0001 | 1.15 | (1.08–1.22) | <0.0001 |
| Hyperlipidemia | 0.69 | (0.65–0.73) | <0.0001 | 0.69 | (0.65–0.73) | <0.0001 |
| AF | -- | -- | -- | -- | -- | -- |
| Hypertension | 0.56 | (0.48–0.65) | <0.0001 | 0.56 | (0.48–0.65) | <0.0001 |
| LC | 1.28 | (1.20–1.37) | <0.0001 | 1.28 | (1.20–1.37) | <0.0001 |
| Pre-ESRD hypoglycemia episodes | ||||||
| 1 versus none | 1.28 | (1.18–1.38) | <0.0001 | |||
| 2 versus none | 1.64 | (1.49–1.81) | <0.0001 | |||
| Post-ESRD hypoglycemia episodes | ||||||
| 1 versus none | 1 | 1.56 | (1.40–1.73) | <0.0001 | ||
| 2 versus none | 1.72 | (1.39–2.12) | <0.0001 | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsiao, C.-C.; Tu, H.-T.; Lin, C.-H.; Chen, K.-H.; Yeh, Y.-H.; See, L.-C. Temporal Trends of Severe Hypoglycemia and Subsequent Mortality in Patients with Advanced Diabetic Kidney Diseases Transitioning to Dialysis. J. Clin. Med. 2019, 8, 420. https://doi.org/10.3390/jcm8040420
Hsiao C-C, Tu H-T, Lin C-H, Chen K-H, Yeh Y-H, See L-C. Temporal Trends of Severe Hypoglycemia and Subsequent Mortality in Patients with Advanced Diabetic Kidney Diseases Transitioning to Dialysis. Journal of Clinical Medicine. 2019; 8(4):420. https://doi.org/10.3390/jcm8040420
Chicago/Turabian StyleHsiao, Ching-Chung, Hui-Tzu Tu, Chi-Hung Lin, Kuan-Hsing Chen, Yung-Hsin Yeh, and Lai-Chu See. 2019. "Temporal Trends of Severe Hypoglycemia and Subsequent Mortality in Patients with Advanced Diabetic Kidney Diseases Transitioning to Dialysis" Journal of Clinical Medicine 8, no. 4: 420. https://doi.org/10.3390/jcm8040420