Renal Consequences of Gestational Diabetes Mellitus in Term Neonates: A Multidisciplinary Approach to the DOHaD Perspective in the Prevention and Early Recognition of Neonates of GDM Mothers at Risk of Hypertension and Chronic Renal Diseases in Later Life

 and
and
Abstract
:1. Introduction
2. Experimental Section
2.1. Study Design
2.2. Neonates
2.3. GDM Mothers
- (a)
- Class 1: including mothers characterised by both pre-gestational and gestational BMI < 30;
- (b)
- Class 2: including mothers characterised by pre-gestational BMI < 30 and gestational BMI > 30;
- (c)
- Class 3: including mothers characterised by both pre-gestational and gestational BMI > 30.
2.4. Renal Mass Parameters
2.5. Urinary Biomarkers
2.6. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Renal Mass Parameters and Urinary Biomarkers in Neonates of GDM Group, Compliant, and Noncompliant GDM Mother Subgroups and Control
3.3. Evaluation of Urinary β-Glucuronidase and Legumain Activities in the Subgroups of Compliant and Noncompliant GDM Mother Neonates and Control
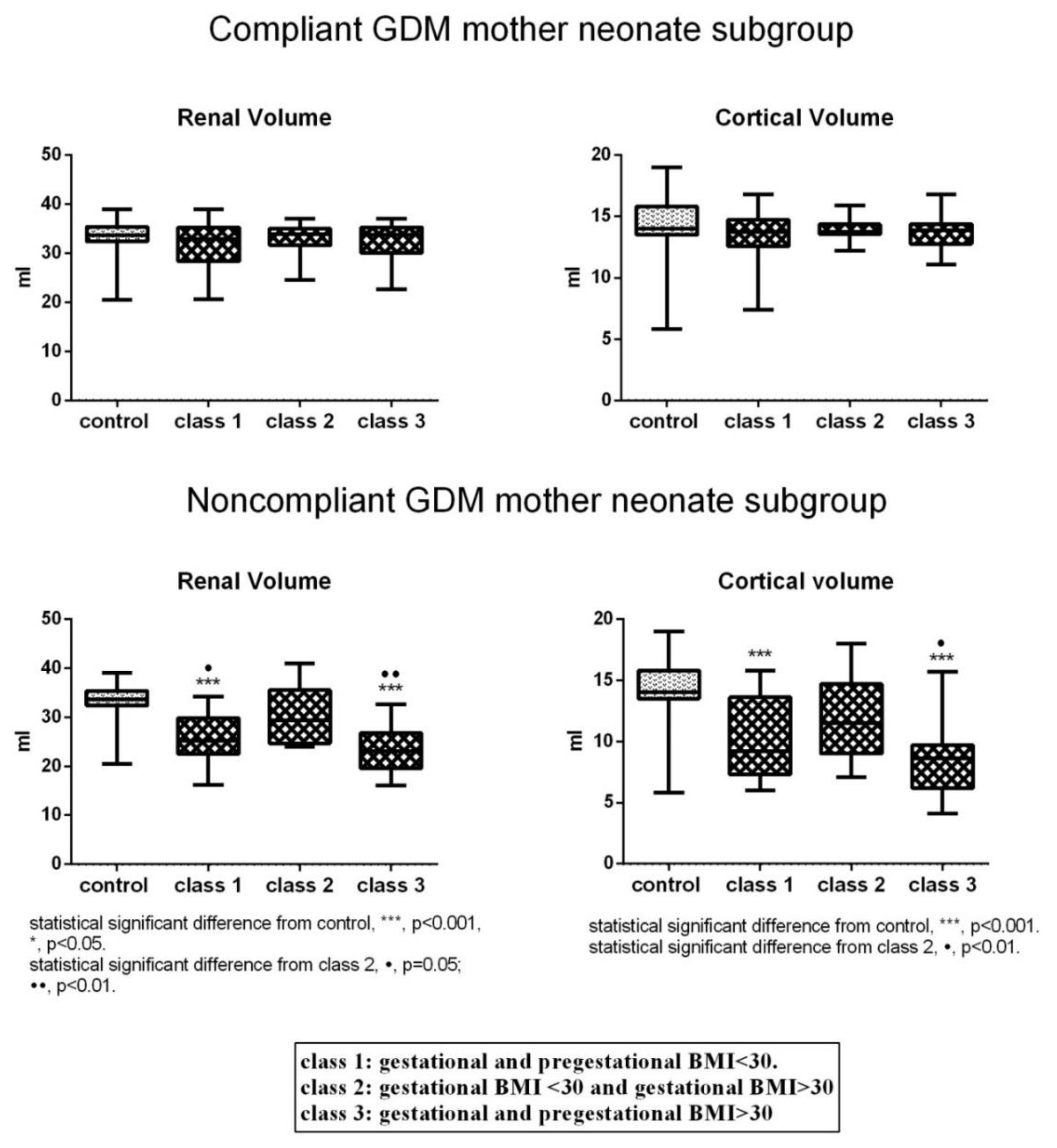
3.4. Recognition of Three Classes in Each Subgroup of GDM Neonates Based on the Presence or Absence of Maternal Pre-gestational and Gestational Obesity and Multiple Comparison of the Parameters Investigated
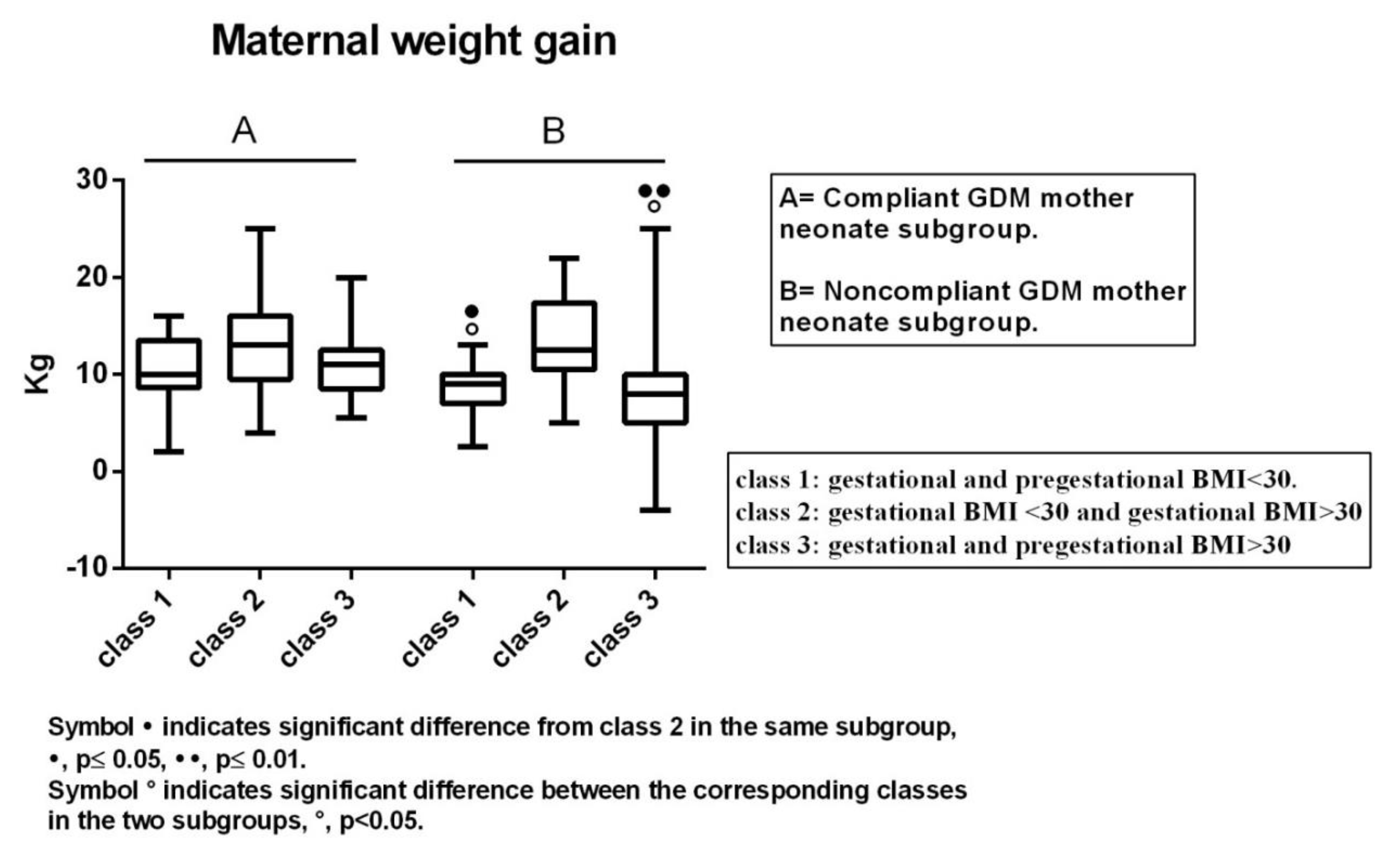
3.5. Maternal Weight Gain in Classes 1–3 of Both Subgroups of GDM Neonates
3.6. ROC Curve Analysis of Renal Volume, Cortical Volume, N-acetyl-β-Glucosaminidase, and Cathepsin B Activity
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hales, C.N.; Barker, D.J. The thrifty phenotype hypothesis. Br. Med. Bull. 2001, 60, 5–20. [Google Scholar] [CrossRef]
- Hanson, M.; Gluckman, P. Developmental origins of noncommunicable disease: Population and public health implications. Am. J. Clin. Nutr. 2011, 94, 1754–1758. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; Amann, M.; Anderson, H.R.; Andrews, K.G.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef]
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; Alvarado, M.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- Luyckx, V.A.; Bertram, J.F.; Brenner, B.M.; Fall, C.; Hoy, W.E.; Ozanne, S.E.; Vikse, B.E. Effect of fetal and child health on kidney development and long-term risk of hypertension and kidney disease. Lancet 2013, 382, 273–283. [Google Scholar] [CrossRef]
- Boubred, F.; Saint-Faust, M.; Buffat, C.; Ligi, I.; Grandvuillemin, I.; Simeoni, U. Developmental origins of chronic renal disease: An integrative hypothesis. Int. J. Nephrol. 2013, 2013, 346067. [Google Scholar] [CrossRef]
- Luyckx, V.A.; Brenner, B.M. Birth weight, malnutrition and kidney-associated outcomes-A global concern. Nat. Rev. Nephrol. 2015, 11, 135–149. [Google Scholar] [CrossRef]
- Low Birth Weight and Nephron Number Working Group. The impact of kidney development on the life course: A consensus document for action. Nephron 2017, 136, 3–49. [Google Scholar] [CrossRef] [PubMed]
- Brenner, B.M.; Mackenzie, H.S. Nephron mass as a risk factor for progression of renal disease. Kidney Intern. Suppl. 1997, 63, 124–127. [Google Scholar]
- Hoy, W.E.; Bertram, J.F.; Denton, R.D.; Zimanyi, M.; Samuel, T.; Hughson, M.D. Nephron number, glomerular volume, renal disease and hypertension. Curr. Opin. Nephrol. Hypertens. 2008, 17, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Schreuder, M.F. Safety in glomerular numbers. Pediatr. Nephrol. 2012, 27, 1881–1987. [Google Scholar] [CrossRef]
- Amri, K.; Freund, N.; Vilar, J.; Merlet-Bénichou, C.; Lelièvre-Pégorier, M. Adverse effects of hyperglycemia on kidney development in rats: In vivo and in vitro studies. Diabetes 1999, 48, 2240–2245. [Google Scholar] [CrossRef] [PubMed]
- Abi Khalil, C.; Travert, F.; Fetita, S.; Rouzet, F.; Porcher, R.; Riveline, J.P.; Hadjadj, S.; Larger, E.; Roussel, R.; Vexiau, P.; et al. Fetal exposure to maternal type 1 diabetes is associated with renal dysfunction at adult age. Diabetes 2010, 59, 2631–2636. [Google Scholar] [CrossRef]
- Davis, E.M.; Peck, J.D.; Thompson, D.; Wild, R.A.; Langlois, P. Maternal diabetes and renal agenesis/dysgenesis. Birth Defects Res. A Clin. Mol. Teratol. 2010, 88, 722–727. [Google Scholar] [CrossRef]
- Nelson, R.G.; Morgenstern, H.; Bennett, P.H. Birth weight and renal disease in Pima Indians with type 2 diabetes mellitus. Am. J. Epidemiol. 1998, 148, 650–656. [Google Scholar] [CrossRef] [PubMed]
- Cappuccini, B.; Torlone, E.; Ferri, C.; Arnone, S.; Troiani, S.; Bini, V.; Bellomo, G.; Barboni, G.; Di Renzo, G.C. Echo 3D and microalbuminuria in children of diabetic mothers. J. Dev. Orig. Health Dis. 2013, 4, 285–289. [Google Scholar] [CrossRef]
- Leybovitz-Haleluya, N.; Wainstock, T.; Landau, D.; Sheiner, E. Maternal gestational diabetes mellitus and the risk of subsequent pediatric cardiovascular diseases of the offspring: A population-based cohort study with up to 18 years of follow up. Acta Diabetol. 2018, 55, 1037–1042. [Google Scholar] [CrossRef] [PubMed]
- International Association of Diabetes and Pregnancy Study Groups Consensus Panel. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 2010, 33, 676–682. [Google Scholar] [CrossRef]
- World Health Organization. Diagnostic Criteria and Classification of Hyperglycaemia First Detected in Pregnancy; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- Italian Diabetologist Association, Italian Society of Diabetology. Italian Standard of Diabetes Mellitus Care. Available online: http://www.siditalia.it/ (accessed on 5 February 2019).
- Tsuboi, N.; Kanzaki, G.; Koike, K.; Kawamura, T.; Ogura, M.; Yokoo, T. Clinicopathological assessment of the nephron number. Clin. Kidney J. 2014, 7, 107–114. [Google Scholar] [CrossRef]
- Charlton, J.R.; Springsteen, C.H.; Carmody, J.B. Nephron number and its determinants in early life: A primer. Pediatr. Nephrol. 2014, 29, 2299–2308. [Google Scholar] [CrossRef] [PubMed]
- Rowe, D.J.F.; Dawnay, A.; Watts, G.F. Microalbuminuria in diabetes mellitus: Review and recommendations for the measurement of albumin in urine. Ann. Clin. Biochem. 1990, 27, 297–312. [Google Scholar] [CrossRef] [PubMed]
- Shihabi, Z.K.; Konen, J.C.; O’Connor, M.L. Albuminuria vs. urinary total protein for detecting chronic renal disorders. Clin. Chem. 1991, 37, 621–624. [Google Scholar]
- Iseki, K.; Ikemiya, Y.; Iseki, C.; Takishita, S. Proteinuria and the risk of developing end-stage renal disease. Kidney Int. 2003, 63, 1468–1474. [Google Scholar] [CrossRef] [PubMed]
- Maack, T.; Johnson, V.; Kau, S.T.; Figueiredo, J.; Sigulem, D. Renal filtration, transport, and metabolism of low-molecular-weight proteins: A review. Kidney Int. 1979, 16, 251–270. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, F.A.; Hardell, L.I.; Hellsing, K. A prospective study of urinary proteins in early infancy. Acta Paediatr. Scand. 1979, 68, 663–667. [Google Scholar] [CrossRef] [PubMed]
- Aperia, A.; Broberger, U. Beta-2-microglobulin, an indicator of renal tubular maturation and dysfunction in the newborn. Acta Peadiatr. Scand. 1979, 68, 669–676. [Google Scholar] [CrossRef]
- Skálová, S. The Diagnostic role of urinary N-Acetyl-B-D-Glucosaminidase [NAG) activity in the detection of renal tubular impairment. Acta Med. 2005, 48, 75–80. [Google Scholar] [CrossRef]
- Schaefer, L.; Gilge, U.; Heidland, A.; Schaefer, R.M. Urinary excretion of cathepsin B and cystatins as parameters of tubular damage. Kidney Intern. Suppl. 1994, 46, 64–67. [Google Scholar]
- Liu, W.J.; Xu, B.H.; Ye, L.; Liang, D.; Wu, H.L.; Zheng, Y.Y.; Deng, J.K.; Li, B.; Liu, H.F. Urinary proteins induce lysosomal membrane permeabilization and lysosomal dysfunction in renal tubular epithelial cells. Am. J. Physiol. Ren. Physiol. 2015, 308, 639–649. [Google Scholar] [CrossRef]
- Aisa, M.C.; Cappuccini, B.; Barbati, A.; Orlacchio, A.; Baglioni, M.; Di Renzo, G.C. Biochemical parameters of renal impairment /injury and surrogate markers of nephron numbers in intrauterine growth restricted and preterm neonates at 30–40 days of postnatal corrected age. Pediatr. Nephrol. 2016, 31, 2277–2287. [Google Scholar] [CrossRef]
- Gonick, H.C.; Kramer, H.J.; Schapiro, A.E. Urinary ß-Glucuronidase Activity in Renal Disease. Arch. Intern. Med. 1973, 132, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Miller, G.; Matthews, S.P.; Reinheckel, T.; Fleming, S.; Watts, C. Asparagine endopeptidase is required for normal kidney physiology and homeostasis. FASEB J. 2011, 25, 1606–1617. [Google Scholar] [CrossRef] [PubMed]
- Morita, Y.; Araki, H.; Sugimoto, T.; Takeuchi, K.; Yamane, T.; Maeda, T.; Yamamoto, Y.; Nishi, K.; Asano, M.; Shirahama-Noda, K.; et al. Legumain/asparaginyl endopeptidase controls extracellular matrix remodeling through the degradation of fibronectin in mouse renal proximal tubular cells. FEBS Lett. 2007, 581, 1417–1424. [Google Scholar] [CrossRef] [PubMed]
- Zohdi, V.; Sutherland, M.R.; Lim, K.; Gubhaju, L.; Zimanyi, M.A.; Black, M.J. Low Birth Weight due to Intrauterine Growth Restriction and/or Preterm Birth: Effects on Nephron Number and Long-Term Renal Health. Int. J. Nephrol. 2012, 2012, 136942. [Google Scholar] [CrossRef] [PubMed]
- Rousian, M.; Verwoerd-Dikkeboom, C.M.; Koning, A.H.J.; Hop, W.C.; van der Spek, P.J.; Exalto, N.; Steegers, E.A. Early pregnancy volume measurements: Validation of ultrasound techniques and new perspectives. BJOG 2009, 116, 278–285. [Google Scholar] [CrossRef]
- Beccari, T.; Mancuso, F.; Costanzi, E.; Tassi, C.; Barone, R.; Fiumara, A.; Orlacchio, A.; Aisa, M.C.; Orlacchio, A. Beta-hexosaminidase, alpha-D-mannosidase, and beta-mannosidase expression in serum from patients with carbohydrate-deficient glycoprotein syndrome type I. Clin. Chim. Acta 2000, 302, 125–132. [Google Scholar] [CrossRef]
- Aisa, M.C.; Rahman, S.; Senin, U.; Maggio, D.; Russell, R.G. Cathepsin B activity in normal human osteoblast-like cells and human osteoblastic osteosarcoma cells [MG-63): Regulation by interleukin-1 beta and parathyroid hormone. Biochim. Biophys. Acta 1996, 21, 29–36. [Google Scholar] [CrossRef]
- Coonrod, D.; Paterson, P.Y. Urine beta-glucuronidase in renal injury. I. Enzyme assay conditions and response to mercuric chloride in rats. Transl. Res. 1969, 73, 6–16. [Google Scholar]
- Stothard, K.J.; Tennant, P.W.; Bell, R.; Rankin, J. Maternal overweight and obesity and the risk of congenital anomalies: A systematic review and meta-analysis. AMA 2009, 301, 636–650. [Google Scholar] [CrossRef]
- Block, S.R.; Watkins, S.M.; Salemi, J.L.; Rutkowski, R.; Tanner, J.P.; Correia, J.A.; Kirby, R.S. Maternal pre-pregnancy body mass index and risk of selected birth defects: Evidence of a dose-response relationship. Paediatr. Perinat. Epidemiol. 2013, 27, 521–531. [Google Scholar] [CrossRef]
- Zhang, C.H.; Liu, X.Y.; Zhan, Y.W.; Zhang, L.; Huang, Y.J.; Zhou, H. Effects of prepregnancy Body Mass Index and Gestational Weight Gain on pregnancy outcomes. Asia Pac. J. Public Health 2015, 27, 620–630. [Google Scholar] [CrossRef]
- Cho, E.-H.; Hur, J.; Lee, K.-J. Early Gestational Weight Gain Rate and Adverse Pregnancy Outcomes in Korean Women. PLoS ONE 2015, 10, e0140376. [Google Scholar] [CrossRef]
- Yang, S.; Zhou, A.; Xiong, C.; Yang, R.; Bassig, B.A.; Hu, R.; Zhang, Y.; Yao, C.; Zhang, Y.; Qiu, L.; et al. Parental Body Mass Index, Gestational Weight Gain, and risk of macrosomia: A population-based case-control study in china. Paediatr. Perinat. Epidemiol. 2015, 29, 462–471. [Google Scholar] [CrossRef]
- Crane, J.M.G.; White, J.; Murphy, P.; Burrage, L.; Hutchens, D. The effect of gestational weight gain by body mass index on maternal and neonatal outcomes. J. Obstet. Gynaecol. Can. 2009, 31, 28–35. [Google Scholar] [CrossRef]
- Papazian, T.; Abi Tayeh, G.; Sibai, D.; Hout, H.; Melki, I.; Rabbaa Khabbaz, L. Impact of maternal body mass index and gestational weight gain on neonatal outcomes among healthy Middle-Eastern females. PLoS ONE 2017, 12, e0181255. [Google Scholar] [CrossRef]
- Nath, K.A. Tubulointerstitial changes as a major determinant in the progression of renal damage. Am. J. Kidney Dis. 1992, 20, 1–17. [Google Scholar] [CrossRef]
- Lappas, M.; Hiden, U.; Desoye, G.; Froehlich, J.; Hauguel-de Mouzon, S.; Jawerbaum, A. The role of oxidative stress in the pathophysiology of gestational diabetes mellitus. Antioxid. Redox Signal. 2011, 15, 3061–3100. [Google Scholar] [CrossRef]
- Neiger, R. Long-term effects of pregnancy complications on maternal health: A review. J. Clin. Med. 2017, 6, 76. [Google Scholar] [CrossRef]
- Charach, R.; Wolak, T.; Shoham-Vardi, I.; Sergienko, R.; Sheiner, E. Can slight glucose intolerance during pregnancy predict future maternal atherosclerotic morbidity? Diabet. Med. 2016, 33, 920–925. [Google Scholar] [CrossRef]
- Piccoli, G.B.; Attini, R.; Cabiddu, G. Kidney diseases and pregnancy: A multidisciplinary approach for improving care by involving nephrology, obstetrics, neonatology, urology, diabetology, bioethics, and internal medicine. J. Clin. Med. 2018, 7, 135. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type |
|
| Aims |
|
| |
| |
| Population |
|
| |
| |
| Inclusion Criteria |
|
| |
| |
| |
| |
| |
| Exclusion Criteria |
|
| |
| Primary Endpoints |
|
| |
| Secondary Endpoints |
|
| |
|
| Control | Compliant GDM Mother Neonate Subgroup | Noncompliant GDM Mother Neonate Subgroup | |
|---|---|---|---|
| Sex | 33 (m), 22 (f) | 32 (m), 33 (f) | 40 (m), 34 (f) |
| Birth weight (g) | 3308 ± 484.3 | 3326 ± 407 | 3318 ± 415 |
| Gestational weeks (week) | 39.04 ± 1.9 | 38.8 ± 1.12 | 38.9 ± 0.96 |
| Placenta weight (g) | 558 ± 92.7 | 563 ± 84.71 | 549 ± 89 |
| Maternal age (year) | 28.75 ± 4.5 | 27.5 ± 2.9 | 29.5 ± 4 |
| Diagnosis of GDM (week) | - | 26 ± 1.15 | 24.1 ± 1.5 |
| Subgroup | Class | Pre-Gestational BMI | Gestational BMI | |
|---|---|---|---|---|
| Compliant | Class 1 (n = 36) | median | 22 | 26 |
| IQR | 20.8–24 | 25.2–27.9 | ||
| min/max | 19–28 | 21–29 | ||
| mean ± sem | 22.3 ± 0.3 | 26.3 ± 0.3 | ||
| Class 2 (n = 10) | median | 27.5 | 32 | |
| IQR | 26–29 | 30.8–35 | ||
| min/max | 24.7–29.6 | 30–35 | ||
| mean ± sem | 27.3 ± 0.4 | 32.2 ± 0.5 | ||
| Class 3 (n = 19) | median | 32 | 37 | |
| IQR | 30.5–34 | 34–37.5 | ||
| min/max | 30–36 | 33–39 | ||
| mean ± sem | 32.2 ± 0.7 | 36.2 ± 0.7 | ||
| Noncompliant | Class 1 (n = 30) | median | 24 | 27 |
| IQR | 22–25 | 25.25–29 | ||
| min/max | 15–27 | 18–29.9 | ||
| mean ± sem | 23.25 ± 0.4 | 26.5 ± 0.4 | ||
| Class 2 (n = 24) | median | 27 | 32 | |
| IQR | 25.7–28 | 31–33 | ||
| min/max | 24.6–29 | 30.1–33.8 | ||
| mean ± sem | 27 ± 0.4 | 32 ± 0.4 | ||
| Class 3 (n = 20) | median | 33 | 36.3 | |
| IQR | 31.2–35.25 | 34.8–38.4 | ||
| min/max | 30–45 | 31–46 | ||
| mean ± sem | 34 ± 0.7 | 37 ± 0.8 | ||
| a. Renal Mass Parameters. | |||||
| Control (n = 55) | GDM Group (n = 139) | Compliant GDM Mother Subgroup (n = 65) | Noncompliant GDM Mother Subgroup (n = 74) | ||
| Renal volume (mL) | median | 33.7 | 29.2 *** | 33.4 | 24.8 ***, °°° |
| IQR | 32.18–35.48 | 24.8–33.6 | 28.75–35 | 22.15–29.5 | |
| min/max | 27.8–39 | 16.1–41 | 20.6–39 | 16.1–41 | |
| mean ± sem | 33.69–0.33 | 29 ± 0.49 | 32 ± 0.55 | 25.6 ± 0.75 | |
| Cortical volume (mL) | median | 14.00 | 12.8 *** | 13.8 | 9.2 ***, °°° |
| IQR | 13.5–15.8 | 9.6–14 | 12.95–14.53 | 7.2–13.00 | |
| min/max | 5.8–19 | 4.1–18 | 7.4–16.8 | 4.1–18 | |
| mean ± sem | 14.4 ± 0.27 | 11.95 ± 0.27 | 13.67 ± 0.22 | 10.1 ± 0.47 | |
| b. Urinary Biomarkers | |||||
| Control (n = 55) | GDM Group (n = 139) | Compliant GDM Mother Subgroup (n = 65) | Noncompliant GDM Mother Subgroup (n = 74) | ||
| Albumin (mg/mmol creatinine) | median | 5.9 | 9.06 | 7.84 | 9.3 |
| IQR | 4.26–9.6 | 4.3–9.8 | 3.5–10.94 | 7.6–9.57 | |
| min/max | 2.2–20.5 | 2.7–18.5 | 2.72–18.49 | 6.96–10.33 | |
| mean ± sem | 7.45 ± 1.11 | 8.17 ± 0.79 | 7.99 ± 10.2 | 8.8 ± 0.5 | |
| β2microglobulin (μg/mmol creatinine) | median | 0.35 | 0.41 | 0.40 | 0.44 |
| IQR | 0.17–0.67 | 0.30–1 | 0.38–3.45 | 0.18–0.96 | |
| min/max | 0.5–1.05 | 0.05–3.45 | 0.38–3.45 | 0.05–0.96 | |
| mean ± sem | 0.44 ± 0.14 | 0.83 ± 0.35 | 1.41 ± 1.02 | 0.53 ± 0.17 | |
| Cathepsin B (IU/h mmol creatinine) | median | 0.99 | 1.41 * | 1.18 | 1.43 * |
| IQR | 0.88–1.2 | 1.04–1.86 | 0.68–1.7 | 1.37–1.98 | |
| min/max | 0.73–1.51 | 0.68–1.86 | 0.68–2.77 | 0.73–2.2 | |
| mean ± sem | 1.04 ± 0.05 | 1.47 ± 0.13 | 1.38 ± 0.23 | 1.65–0.12 | |
| N-acetyl-β-d-glucosaminidase (IU/min mmol creatinine) | median | 2.38 | 4.12 * | 3.95 | 4.28 * |
| IQR | 0.83–4.05 | 2.56–6.87 | 2.43–5.08 | 3.71–12.2 | |
| min/max | 0.71–6.39 | 1.36–12.71 | 1.36–12.19 | 1.63–12.71 | |
| mean ± sem | 2.66 ± 0.52 | 5.29 ± 0.78 | 4.47 ± 0.76 | 6.92 ± 1.71 | |
| Control (n = 55) | Compliant GDM Mother Neonate Subgroup (n = 65) | Noncompliant GDM Mother Neonate Subgroup (n = 74) | ||
|---|---|---|---|---|
| β-glucuronidase (IU/min mmol creatinine) | median | 0.97 | 0.98 | 1.12 |
| IQR | 0.45–1.7 | 0.71–1.6 | 0.78–1.65 | |
| min/max | 0.3–2.72 | 0.02–7.5 | 0.57–2.15 | |
| mean ± sem | 1.15 ± 1.19 | 1.38 ± 0.2 | 1.22 ± 0.13 | |
| legumain (IU/h mmol creatinine) | median | 1.77 | 0.18 | 0.186 |
| IQR | 0.15–0.27 | 0.1–0.27 | 0.13–0.5 | |
| min/max | 0.12–0.54 | 0.016–0.48 | 0.11–0.58 | |
| mean ± sem | 0.23 ± 0.05 | 0.2 ± 0.04 | 1.12 ± 0.13 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aisa, M.C.; Cappuccini, B.; Barbati, A.; Clerici, G.; Torlone, E.; Gerli, S.; Di Renzo, G.C. Renal Consequences of Gestational Diabetes Mellitus in Term Neonates: A Multidisciplinary Approach to the DOHaD Perspective in the Prevention and Early Recognition of Neonates of GDM Mothers at Risk of Hypertension and Chronic Renal Diseases in Later Life. J. Clin. Med. 2019, 8, 429. https://doi.org/10.3390/jcm8040429
Aisa MC, Cappuccini B, Barbati A, Clerici G, Torlone E, Gerli S, Di Renzo GC. Renal Consequences of Gestational Diabetes Mellitus in Term Neonates: A Multidisciplinary Approach to the DOHaD Perspective in the Prevention and Early Recognition of Neonates of GDM Mothers at Risk of Hypertension and Chronic Renal Diseases in Later Life. Journal of Clinical Medicine. 2019; 8(4):429. https://doi.org/10.3390/jcm8040429
Chicago/Turabian StyleAisa, Maria Cristina, Benito Cappuccini, Antonella Barbati, Graziano Clerici, Elisabetta Torlone, Sandro Gerli, and Gian Carlo Di Renzo. 2019. "Renal Consequences of Gestational Diabetes Mellitus in Term Neonates: A Multidisciplinary Approach to the DOHaD Perspective in the Prevention and Early Recognition of Neonates of GDM Mothers at Risk of Hypertension and Chronic Renal Diseases in Later Life" Journal of Clinical Medicine 8, no. 4: 429. https://doi.org/10.3390/jcm8040429