GLP-1 Limits Adipocyte Inflammation and Its Low Circulating Pre-Operative Concentrations Predict Worse Type 2 Diabetes Remission after Bariatric Surgery in Obese Patients

 , , and
, , and
Abstract
:1. Introduction
2. Material and Methods
2.1. Patient Selection
2.2. Analytical Procedures
2.3. Oral Glucose Tolerance Test
2.4. RNA Extraction and Real-Time PCR
2.5. Adipocyte Culture
2.6. Statistical Analysis
3. Results
3.1. Decreased GLP-1 Circulating Levels in Human Obesity-Associated T2D
3.2. GLP-1 Circulating Levels in Patients with T2D Increase after RYGB
3.3. Increased Pre-Operative GLP-1 Circulating Levels in Patients with T2D Remission
3.4. Exendin-4 Downregulates the Expression of Pro-Inflammatory Markers in Human Visceral Adipocytes
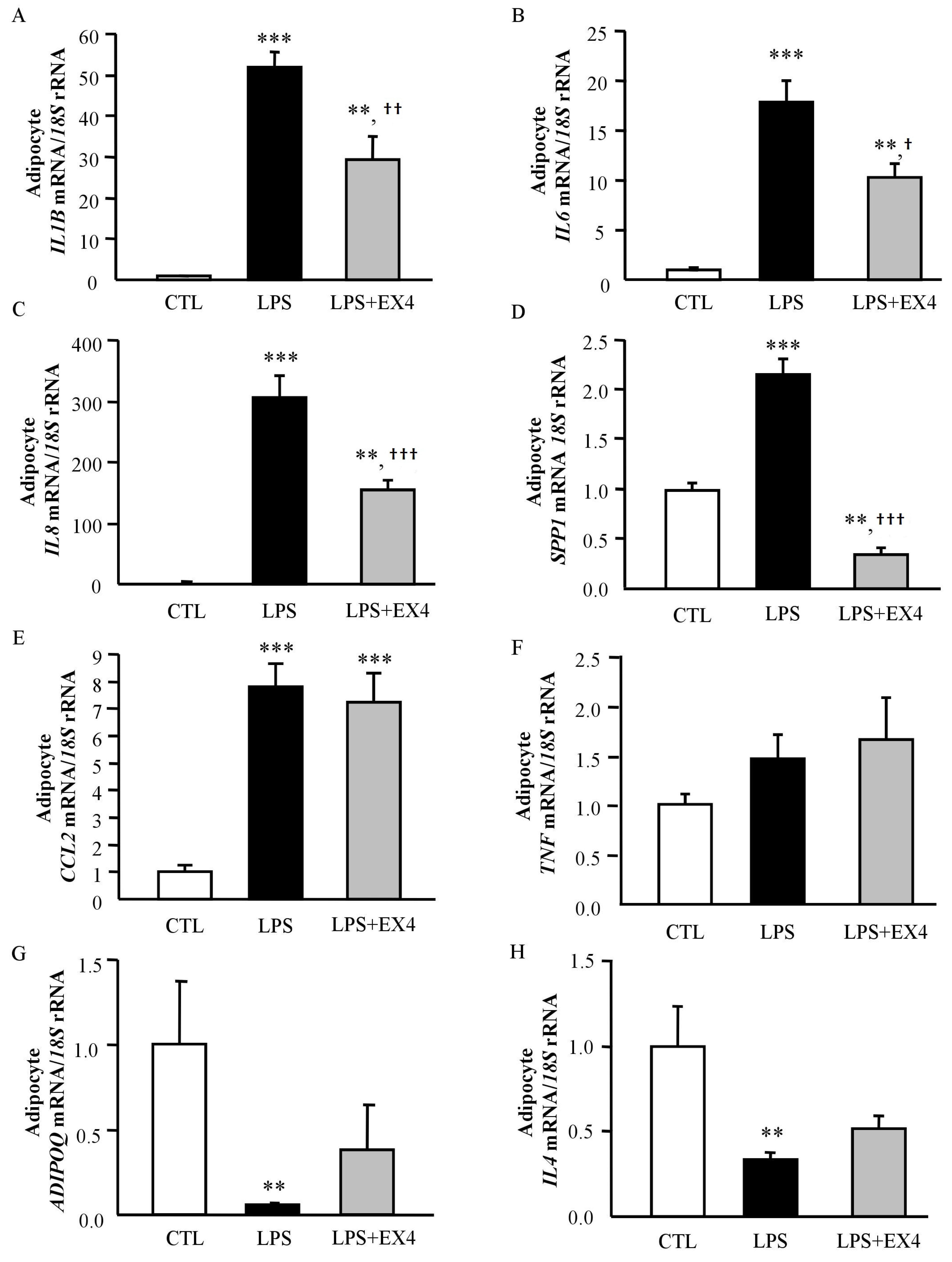
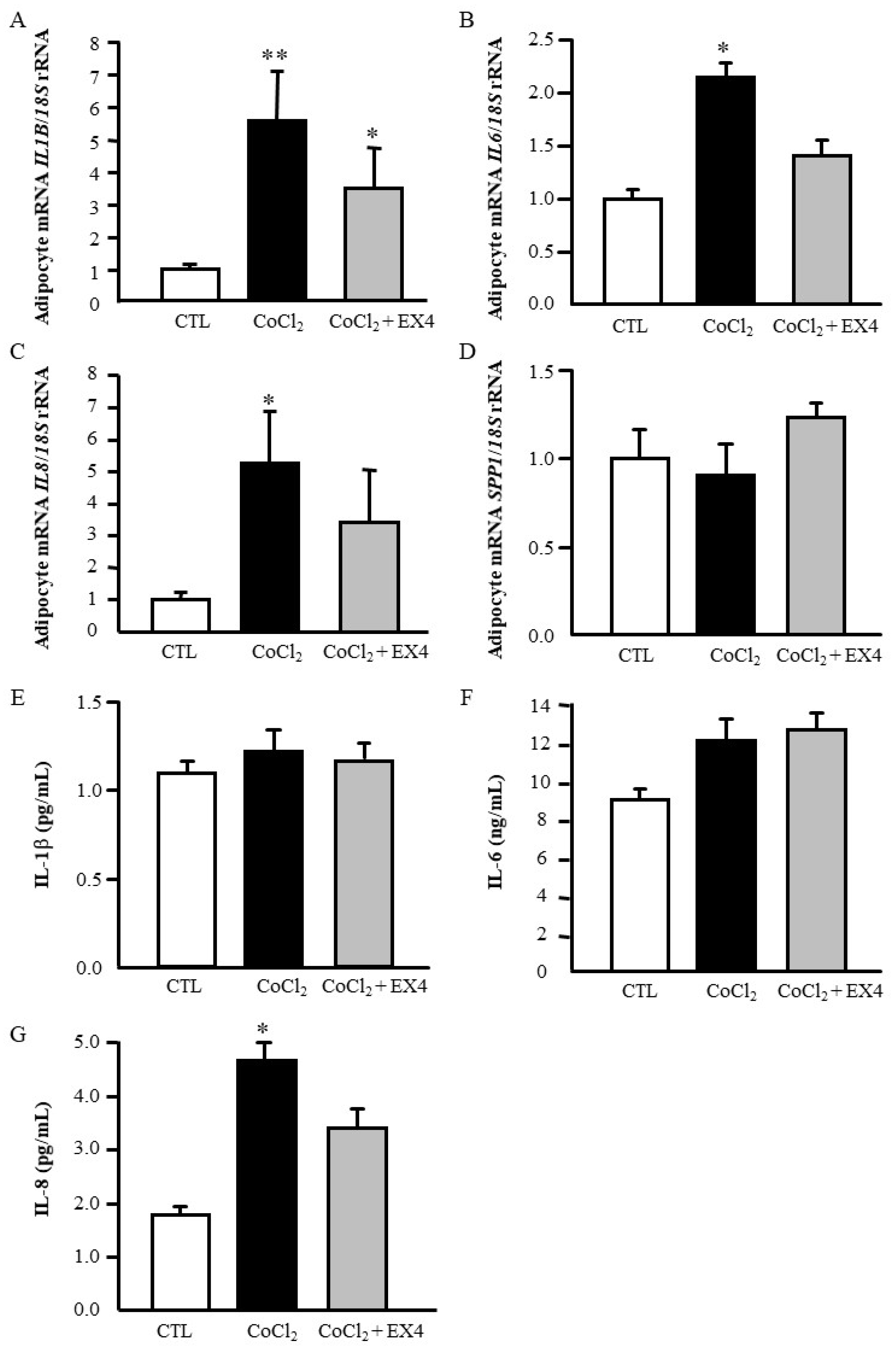
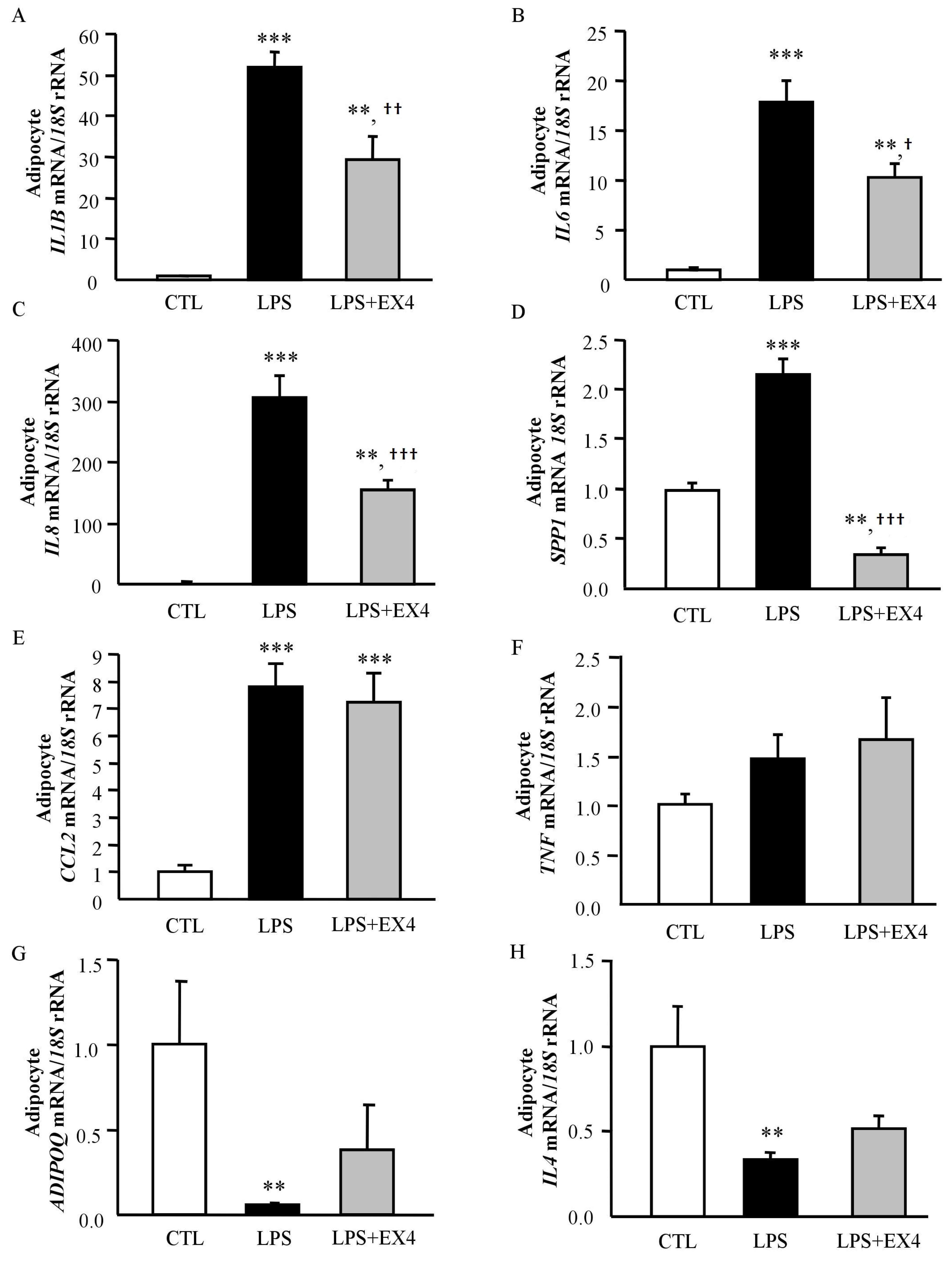
3.5. Exendin-4 Inhibits LPS- and Hypoxia-Induced Inflammation in Human Visceral Adipocytes
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ADIOPQ | adiponectin |
| ALP | alkaline phosphatase |
| ALT | alanine aminotransferase |
| ARG1 | arginase 1 |
| AST | aspartate aminotransferase |
| BMI | body mass index |
| CCL2 | monocyte chemoattractant protein-1 |
| CRP | C-reactive protein |
| DBP | diastolic blood pressure |
| γ-GT | γ-glutamyltransferase |
| GLP-1 | glucagon-like peptide-1 |
| HOMA | homeostasis model assessment |
| IL | interleukin |
| KLF4 | kruppel-like factor 4 |
| LPS | lipopolysaccharide |
| NG | normoglycemic |
| OGTT | oral glucose tolerance test |
| PARG | peroxisome proliferator-activated receptor-γ |
| QUICKI | quantitative insulin sensitivity check index |
| RYGB | Roux-en-Y gastric bypass |
| SBP | systolic blood pressure; |
| SVFC | stroma-vascular fraction cells; |
| TNF | tumour necrosis factor-α |
| T2D | type 2 diabetes |
| VAT | visceral adipose tissue |
References
- James, W.P.T. Obesity: A global public health challenge. Clin. Chem. 2018, 64, 24–29. [Google Scholar] [CrossRef]
- Reilly, S.M.; Saltiel, A.R. Adapting to obesity with adipose tissue inflammation. Nat. Rev. Endocrinol. 2017, 13, 633–643. [Google Scholar] [CrossRef]
- Frühbeck, G. Bariatric and metabolic surgery: A shift in eligibility and success criteria. Nat. Rev. Endocrinol. 2015, 11, 465–477. [Google Scholar] [CrossRef]
- Batterham, R.L.; Cummings, D.E. Mechanisms of diabetes improvement following bariatric/metabolic surgery. Diabetes Care 2016, 39, 893–901. [Google Scholar] [CrossRef]
- Eng, C.; Kramer, C.K.; Zinman, B.; Retnakaran, R. Glucagon-like peptide-1 receptor agonist and basal insulin combination treatment for the management of type 2 diabetes: A systematic review and meta-analysis. Lancet 2014, 384, 2228–2234. [Google Scholar] [CrossRef]
- Hutch, C.R.; Sandoval, D. The role of GLP-1 in the metabolic success of bariatric surgery. Endocrinology 2017, 158, 4139–4151. [Google Scholar] [CrossRef] [PubMed]
- Marso, S.P.; Holst, A.G.; Vilsboll, T. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N. Engl. J. Med. 2017, 376, 891–892. [Google Scholar] [CrossRef]
- Campbell, J.E.; Drucker, D.J. Pharmacology, physiology, and mechanisms of incretin hormone action. Cell Metab. 2013, 17, 819–837. [Google Scholar] [CrossRef]
- Sharma, D.; Verma, S.; Vaidya, S.; Kalia, K.; Tiwari, V. Recent updates on GLP-1 agonists: Current advancements & challenges. Biomed. Pharmacother. 2018, 108, 952–962. [Google Scholar]
- DeFronzo, R.A.; Ratner, R.E.; Han, J.; Kim, D.D.; Fineman, M.S.; Baron, A.D. Effects of exenatide (exendin-4) on glycemic control and weight over 30 weeks in metformin-treated patients with type 2 diabetes. Diabetes Care 2005, 28, 1092–1100. [Google Scholar] [CrossRef]
- Frühbeck, G.; Nogueiras, R. GLP-1: The oracle for gastric bypass? Diabetes 2014, 63, 399–401. [Google Scholar] [CrossRef] [PubMed]
- Habegger, K.M.; Heppner, K.M.; Amburgy, S.E.; Ottaway, N.; Holland, J.; Raver, C.; Bartley, E.; Muller, T.D.; Pfluger, P.T.; Berger, J.; et al. GLP-1r responsiveness predicts individual gastric bypass efficacy on glucose tolerance in rats. Diabetes 2014, 63, 505–513. [Google Scholar] [CrossRef] [PubMed]
- Nannipieri, M.; Baldi, S.; Mari, A.; Colligiani, D.; Guarino, D.; Camastra, S.; Barsotti, E.; Berta, R.; Moriconi, D.; Bellini, R.; et al. Roux-en-y gastric bypass and sleeve gastrectomy: Mechanisms of diabetes remission and role of gut hormones. J. Clin. Endocrinol. Metab. 2013, 98, 4391–4399. [Google Scholar] [CrossRef]
- Jimenez, A.; Casamitjana, R.; Flores, L.; Delgado, S.; Lacy, A.; Vidal, J. Glp-1 and the long-term outcome of type 2 diabetes mellitus after roux-en-y gastric bypass surgery in morbidly obese subjects. Ann. Surg. 2013, 257, 894–899. [Google Scholar] [CrossRef]
- Lee, Y.S.; Park, M.S.; Choung, J.S.; Kim, S.S.; Oh, H.H.; Choi, C.S.; Ha, S.Y.; Kang, Y.; Kim, Y.; Jun, H.S. Glucagon-like peptide-1 inhibits adipose tissue macrophage infiltration and inflammation in an obese mouse model of diabetes. Diabetologia 2012, 55, 2456–2468. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.S.; Jun, H.S. Anti-inflammatory effects of GLP-1-based therapies beyond glucose control. Mediat. Inflamm. 2016, 2016, 3094642. [Google Scholar] [CrossRef] [PubMed]
- Ceriello, A.; Novials, A.; Canivell, S.; La Sala, L.; Pujadas, G.; Esposito, K.; Testa, R.; Bucciarelli, L.; Rondinelli, M.; Genovese, S. Simultaneous GLP-1 and insulin administration acutely enhances their vasodilatory, antiinflammatory, and antioxidant action in type 2 diabetes. Diabetes Care 2014, 37, 1938–1943. [Google Scholar] [CrossRef]
- Mazidi, M.; Karimi, E.; Rezaie, P.; Ferns, G.A. Treatment with GLP1 receptor agonists reduce serum crp concentrations in patients with type 2 diabetes mellitus: A systematic review and meta-analysis of randomized controlled trials. J. Diabetes Complicat. 2017, 31, 1237–1242. [Google Scholar] [CrossRef]
- Daousi, C.; Pinkney, J.H.; Cleator, J.; Wilding, J.P.; Ranganath, L.R. Acute peripheral administration of synthetic human glp-1 (7-36 amide) decreases circulating il-6 in obese patients with type 2 diabetes mellitus: A potential role for GLP-1 in modulation of the diabetic pro-inflammatory state? Regul. Pept. 2013, 183, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Drucker, D.J. The cardiovascular biology of glucagon-like peptide-1. Cell Metab. 2016, 24, 15–30. [Google Scholar] [CrossRef]
- American Diabetes Association. Classification and diagnosis of diabetes: Standards of medical care in diabetes-2018. Diabetes Care 2018, 41, 13–27. [Google Scholar] [CrossRef]
- Still, C.D.; Wood, G.C.; Benotti, P.; Petrick, A.T.; Gabrielsen, J.; Strodel, W.E.; Ibele, A.; Seiler, J.; Irving, B.A.; Celaya, M.P.; et al. Preoperative prediction of type 2 diabetes remission after roux-en-y gastric bypass surgery: A retrospective cohort study. Lancet Diabetes Endocrinol. 2014, 2, 38–45. [Google Scholar] [CrossRef]
- Gómez-Ambrosi, J.; Silva, C.; Catalán, V.; Rodríguez, A.; Galofré, J.C.; Escalada, J.; Valentí, V.; Rotellar, F.; Romero, S.; Ramírez, B.; et al. Clinical usefulness of a new equation for estimating body fat. Diabetes Care 2012, 35, 383–388. [Google Scholar] [CrossRef]
- Catalán, V.; Gómez-Ambrosi, J.; Rotellar, F.; Silva, C.; Rodríguez, A.; Salvador, J.; Gil, M.J.; Cienfuegos, J.A.; Frühbeck, G. Validation of endogenous control genes in human adipose tissue: Relevance to obesity and obesity-associated type 2 diabetes mellitus. Horm. Metab. Res. 2007, 39, 495–500. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, A.; Gómez-Ambrosi, J.; Catalán, V.; Rotellar, F.; Valentí, V.; Silva, C.; Mugueta, C.; Pulido, M.R.; Vazquez, R.; Salvador, J.; et al. The ghrelin o-acyltransferase-ghrelin system reduces TNF-alpha-induced apoptosis and autophagy in human visceral adipocytes. Diabetologia 2012, 55, 3038–3050. [Google Scholar] [CrossRef]
- Bray, G.A.; Frühbeck, G.; Ryan, D.H.; Wilding, J.P. Management of obesity. Lancet 2016, 387, 1947–1956. [Google Scholar] [CrossRef] [Green Version]
- Nauck, M.A.; Vardarli, I.; Deacon, C.F.; Holst, J.J.; Meier, J.J. Secretion of glucagon-like peptide-1 (GLP-1) in type 2 diabetes: What is up, what is down? Diabetologia 2011, 54, 10–18. [Google Scholar] [CrossRef]
- Faerch, K.; Torekov, S.S.; Vistisen, D.; Johansen, N.B.; Witte, D.R.; Jonsson, A.; Pedersen, O.; Hansen, T.; Lauritzen, T.; Sandbaek, A.; et al. GLP-1 response to oral glucose is reduced in prediabetes, screen-detected type 2 diabetes, and obesity and influenced by sex: The addition-pro study. Diabetes 2015, 64, 2513–2525. [Google Scholar] [CrossRef]
- Alssema, M.; Rijkelijkhuizen, J.M.; Holst, J.J.; Teerlink, T.; Scheffer, P.G.; Eekhoff, E.M.; Gastaldelli, A.; Mari, A.; Hart, L.M.; Nijpels, G.; et al. Preserved GLP-1 and exaggerated GIP secretion in type 2 diabetes and relationships with triglycerides and alt. Eur. J. Endocrinol. 2013, 169, 421–430. [Google Scholar] [CrossRef]
- Cavin, J.B.; Couvelard, A.; Lebtahi, R.; Ducroc, R.; Arapis, K.; Voitellier, E.; Cluzeaud, F.; Gillard, L.; Hourseau, M.; Mikail, N.; et al. Differences in alimentary glucose absorption and intestinal disposal of blood glucose after roux-en-y gastric bypass vs sleeve gastrectomy. Gastroenterology 2016, 150, 454–464. [Google Scholar] [CrossRef] [PubMed]
- Laferrere, B. Diabetes remission after bariatric surgery: Is it just the incretins? Int. J. Obes. 2011, 35, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Sandoval, D.A.; Bagnol, D.; Woods, S.C.; D’Alessio, D.A.; Seeley, R.J. Arcuate glucagon-like peptide 1 receptors regulate glucose homeostasis but not food intake. Diabetes 2008, 57, 2046–2054. [Google Scholar] [CrossRef]
- Beiroa, D.; Imbernon, M.; Gallego, R.; Senra, A.; Herranz, D.; Villarroya, F.; Serrano, M.; Ferno, J.; Salvador, J.; Escalada, J.; et al. GLP-1 agonism stimulates brown adipose tissue thermogenesis and browning through hypothalamic ampk. Diabetes 2014, 63, 3346–3358. [Google Scholar] [CrossRef] [PubMed]
- Carr, R.D.; Larsen, M.O.; Jelic, K.; Lindgren, O.; Vikman, J.; Holst, J.J.; Deacon, C.F.; Ahren, B. Secretion and dipeptidyl peptidase-4-mediated metabolism of incretin hormones after a mixed meal or glucose ingestion in obese compared to lean, nondiabetic men. J. Clin. Endocrinol. Metab. 2010, 95, 872–878. [Google Scholar] [CrossRef] [PubMed]
- Varin, E.M.; Mulvihill, E.E.; Beaudry, J.L.; Pujadas, G.; Fuchs, S.; Tanti, J.F.; Fazio, S.; Kaur, K.; Cao, X.; Baggio, L.L.; et al. Circulating levels of soluble dipeptidyl peptidase-4 are dissociated from inflammation and induced by enzymatic dpp4 inhibition. Cell Metab. 2018. [Google Scholar] [CrossRef]
- Yusta, B.; Baggio, L.L.; Koehler, J.; Holland, D.; Cao, X.; Pinnell, L.J.; Johnson-Henry, K.C.; Yeung, W.; Surette, M.G.; Bang, K.W.; et al. GLP-1r agonists modulate enteric immune responses through the intestinal intraepithelial lymphocyte GLP-1r. Diabetes 2015, 64, 2537–2549. [Google Scholar] [CrossRef] [PubMed]
- Kim Chung le, T.; Hosaka, T.; Yoshida, M.; Harada, N.; Sakaue, H.; Sakai, T.; Nakaya, Y. Exendin-4, a GLP-1 receptor agonist, directly induces adiponectin expression through protein kinase a pathway and prevents inflammatory adipokine expression. Biochem. Biophys. Res. Commun. 2009, 390, 613–618. [Google Scholar] [CrossRef]
- Vendrell, J.; El Bekay, R.; Peral, B.; Garcia-Fuentes, E.; Megia, A.; Macias-Gonzalez, M.; Fernandez Real, J.; Jimenez-Gomez, Y.; Escote, X.; Pachon, G.; et al. Study of the potential association of adipose tissue glp-1 receptor with obesity and insulin resistance. Endocrinology 2011, 152, 4072–4079. [Google Scholar] [CrossRef]
- Fletcher, M.M.; Halls, M.L.; Christopoulos, A.; Sexton, P.M.; Wootten, D. The complexity of signalling mediated by the glucagon-like peptide-1 receptor. Biochem. Soc. Trans. 2016, 44, 582–588. [Google Scholar] [CrossRef]
- Velmurugan, K.; Balamurugan, A.N.; Loganathan, G.; Ahmad, A.; Hering, B.J.; Pugazhenthi, S. Antiapoptotic actions of exendin-4 against hypoxia and cytokines are augmented by CREB. Endocrinology 2012, 153, 1116–1128. [Google Scholar] [CrossRef]
- Gómez-Ambrosi, J.; Salvador, J.; Rotellar, F.; Silva, C.; Catalán, V.; Rodríguez, A.; Gil, M.J.; Frühbeck, G. Increased serum amyloid A concentrations in morbid obesity decrease after gastric bypass. Obes. Surg. 2006, 16, 262–269. [Google Scholar] [CrossRef]
- Gómez-Ambrosi, J.; Salvador, J.; Páramo, J.A.; Orbe, J.; de Irala, J.; Diez-Caballero, A.; Gil, M.J.; Cienfuegos, J.A.; Frühbeck, G. Involvement of leptin in the association between percentage of body fat and cardiovascular risk factors. Clin. Biochem. 2002, 35, 315–320. [Google Scholar] [CrossRef] [Green Version]
- Catalán, V.; Gómez-Ambrosi, J.; Rodríguez, A.; Silva, C.; Rotellar, F.; Gil, M.J.; Cienfuegos, J.A.; Salvador, J.; Frühbeck, G. Expression of caveolin-1 in human adipose tissue is upregulated in obesity and obesity-associated type 2 diabetes mellitus and related to inflammation. Clin. Endocrinol. 2008, 68, 213–219. [Google Scholar] [CrossRef]
- Gallego-Escuredo, J.M.; Gómez-Ambrosi, J.; Catalán, V.; Domingo, P.; Giralt, M.; Frühbeck, G.; Villarroya, F. Opposite alterations in FGF21 and FGF19 levels and disturbed expression of the receptor machinery for endocrine FGFs in obese patients. Int. J. Obes. 2015, 39, 121–129. [Google Scholar] [CrossRef]
- Gómez-Ambrosi, J.; Gallego-Escuredo, J.M.; Catalán, V.; Rodríguez, A.; Domingo, P.; Moncada, R.; Valentí, V.; Salvador, J.; Giralt, M.; Villarroya, F.; et al. FGF19 and FGF21 serum concentrations in human obesity and type 2 diabetes behave differently after diet- or surgically-induced weight loss. Clin. Nutr. 2017, 36, 861–868. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lean | Obese NG | Obese T2D | |
|---|---|---|---|
| n (males, females) | 30 (12, 18) | 30 (12, 18) | 33 (16, 17) |
| Age (years) | 46 ± 2 | 39 ± 2 | 51 ± 2 † |
| BMI (kg/m2) | 23.0 ± 0.2 | 46.0 ± 1.6 *** | 43.1 ± 1.2 *** |
| Body fat (%) | 29.1 ± 1.8 | 52.1 ± 1.1 *** | 48.7 ± 1.4 *** |
| Waist (cm) | 83 ± 1 | 130 ± 3 *** | 127 ± 2 *** |
| Waist-to-hip ratio | 0.87 ± 0.01 | 0.96 ± 0.02 *** | 1.00 ± 0.01 *** |
| SBP (mm Hg) | 109 ± 2 | 126 ± 3 *** | 129 ± 3 *** |
| DBP (mm Hg) | 67 ± 1 | 80 ± 2 *** | 80 ± 2 *** |
| Fasting glucose (mg/dL) | 92 ± 2 | 90 ± 2 | 151 ± 11 ***,††† |
| Glucose 2-h after OGTT (mg/dL) | 98 ± 8 | 119 ± 4 | 220 ± 21 ***,††† |
| Fasting insulin (μU/mL) | 6.1 ± 0.8 | 16.8 ± 3.8 | 28.2 ± 6.1 ** |
| HOMA | 1.4 ± 0.2 | 3.8 ± 0.9 | 8.2 ± 1.0 ***,††† |
| QUICKI | 0.375 ± 0.010 | 0.340 ± 0.010 | 0.296 ± 0.006 ***,††† |
| Triacylglycerol (mg/dL) | 80 ± 7 | 101 ± 6 | 156 ± 11 ***,†† |
| Total cholesterol (mg/dL) | 180 ± 6 | 199 ± 9 | 179 ± 6 |
| LDL-cholesterol (mg/dL) | 103 ± 5 | 128 ± 7 * | 104 ± 6 † |
| HDL-cholesterol (mg/dL) | 59 ± 2 | 50 ± 3 * | 44 ± 2 *** |
| Leptin (ng/mL) | 11.4 ± 3.0 | 50.2 ± 4.0 *** | 44.7 ± 5.2 *** |
| Adiponectin (µg/mL) | 13.1 ± 1.9 | 11.6 ± 1.6 | 6.7 ± 0.6 ***,†† |
| Uric acid (mg/dL) | 4.5 ± 0.2 | 5.7 ± 0.3 * | 5.8 ± 0.3 ** |
| Creatinine (mg/dL) | 0.8 ± 0.03 | 0.78 ± 0.03 | 0.82 ± 0.03 |
| CRP (mg/L) | 4.81 ± 1.74 | 9.23 ± 1.82 * | 8.27 ± 1.43 * |
| Fibrinogen (mg/dL) | 279 ± 18 | 394 ± 17 ** | 370 ± 20 * |
| von Willebrand factor (%) | 108 ± 4 | 115.1 ± 11.4 | 148.5 ± 9.2 |
| Homocysteine (μmol/L) | 9.7 ± 2.4 | 10.2 ± 1.7 | 10.4 ± 1.0 |
| AST (IU/L) | 14 ± 1 | 17 ± 3 | 16 ± 1 |
| ALT (IU/L) | 17 ± 2 | 24 ± 3 * | 23 ± 2 |
| AST/ALT | 0.96 ± 0.08 | 0.76 ± 0.06 * | 0.73 ± 0.03 * |
| ALP (IU/L) | 82 ± 6 | 75 ± 6 | 67 ± 6 |
| γ-GT (IU/L) | 14 ± 1 | 17 ± 2 | 33 ± 5 ***,†† |
| Obese NG Before Surgery | Obese NG After Surgery | Obese T2D Before Surgery | Obese T2D After Surgery | |
|---|---|---|---|---|
| n (males, females) | 22 (6, 16) | 22 (6, 16) | 55 (22, 33) | 55 (22, 33) |
| BMI (kg/m2) | 44.0 ± 1.9 | 30.8 ± 1.7 *** | 45.7 ± 1.0 | 35.2 ± 1.0 *** |
| Body fat (%) | 52.3 ± 1.0 | 38.9 ± 2.6 *** | 51.6 ± 1.0 | 43.0 ± 1.5 *** |
| Waist (cm) | 123 ± 4 | 98 ± 4 *** | 130 ± 2 | 110 ± 2 *** |
| Waist-to-hip ratio | 0.94 ± 0.02 | 0.90 ± 0.02 * | 0.99 ± 0.01 | 0.96 ± 0.01 ** |
| SBP (mm Hg) | 123 ± 3 | 111 ± 3 *** | 130 ± 2 | 118 ± 2 ** |
| DBP (mm Hg) | 78 ± 2 | 70 ± 2 ** | 82 ± 1 | 73 ± 1 * |
| Fasting glucose (mg/dL) | 91 ± 2 | 87 ± 2 * | 122 ± 5 | 104 ± 5 ** |
| Fasting insulin (μU/mL) | 15.1 ± 5.2 | 6.8 ± 1.3 | 22.2 ± 1.8 | 10.2 ± 1.0 ** |
| HOMA | 3.7 ± 1.3 | 1.6 ± 0.3 | 6.5 ± 0.5 | 2.5 ± 0.3 *** |
| QUICKI | 0.35 ± 0.01 | 0.39 ± 0.01 ** | 0.30 ± 0.01 | 0.35 ± 0.01 *** |
| HbA1c (%) | - | - | 7.9 ± 0.4 | 6.7 ± 0.3 ** |
| Triacylglycerol (mg/dL) | 101 ± 9 | 72 ± 7 ** | 142 ± 13 | 94 ± 8 *** |
| Total cholesterol (mg/dL) | 201 ± 12 | 152 ± 7 *** | 185 ± 7 | 157 ± 5 ** |
| LDL-cholesterol (mg/dL) | 129 ± 10 | 83 ± 6 *** | 110 ± 6 | 88 ± 4 ** |
| HDL-cholesterol (mg/dL) | 51 ± 6 | 55 ± 3 | 46 ± 2 | 51 ± 2 * |
| Leptin (ng/mL) | 49.1 ± 5.2 | 12.5 ± 3.1 *** | 48.7 ± 4.6 | 17.7 ± 1.9 *** |
| Adiponectin | 11.6 ± 1.3 | 16.9 ± 1.3 *** | 7.2 ± 0.4 | 12.0 ± 0.7 *** |
| Uric acid (mg/dL) | 5.5 ± 0.3 | 4.8 ± 0.3 ** | 5.9 ± 0.2 | 5.3 ± 0.2 * |
| Creatinine (mg/dL) | 0.7 ± 0.1 | 0.7 ± 0.2 | 0.8 ± 0.1 | 1.0 ± 0.2 * |
| CRP (mg/L) | 10.23 ± 3.20 | 4.96 ± 0.30 * | 7.91 ± 1.99 | 2.48 ± 0.76 * |
| Fibrinogen (mg/dL) | 394 ± 23 | 342 ± 20 ** | 364 ± 17 | 350 ± 16 |
| von Willebrand factor (%) | 97 ± 18 | 91 ± 15 | 155 ± 13 | 127 ± 12 * |
| Homocysteine (μmol/L) | 14.1 ± 5.8 | 10.6 ± 2.8 | 10.1 ± 0.9 | 9.9 ± 0.7 |
| AST (IU/L) | 17 ± 4 | 14 ± 1 | 15 ± 1 | 18 ± 1 |
| ALT (IU/L) | 24 ± 4 | 16 ± 2 | 23 ± 2 | 26 ± 3 |
| AST/ALT | 0.74 ± 0.07 | 0.90 ± 0.04 ** | 0.75 ± 0.04 | 0.80 ± 0.04 |
| ALP (IU/L) | 78 ± 8 | 61 ± 5 ** | 70 ± 5 | 72 ± 5 |
| γ-GT (IU/L) | 17 ± 2 | 10 ± 2 *** | 31 ± 3 | 18 ± 1 *** |
| IL-1β (pg/mL) | 1.57 ± 0.18 | 1.41 ± 0.07 | 1.61 ± 0.10 | 1.42 ± 0.08 |
| IL-6 (pg/mL) | 19.8 ± 8.2 | 8.5 ± 0.4 * | 19.1 ± 2.6 | 11.1 ± 0.8 ** |
| IL-18 (pg/mL) | 126.8 ± 9.2 | 99.4 ± 7.6 * | 122.9 ± 6.7 | 112.5 ± 6.3 * |
| MCP-1 (pg/mL) | 221 ± 32 | 198 ± 21 | 247 ± 25 | 234 ± 20 |
| T2D-Responders | T2D-Non-Responders | |
|---|---|---|
| n (males, females) | 31 (16, 15) | 16 (8, 8) |
| DiaRem Score | 4.05 ± 0.74 | 11.00 ± 1.81 ** |
| Insulin treatment (%) | 6.5% | 31.5% |
| Other T2D treatment (%) | 19.4% | 87.5% |
| Age (years) | 48 ± 2 | 52 ± 2 |
| BMI (kg/m2) | 41.2 ± 1.8 | 39.3 ± 1.8 |
| Body fat (%) | 48.4 ± 1.3 | 44.8 ± 1.8 |
| Waist (cm) | 126 ± 2 | 121 ± 4 |
| Waist-to-hip ratio | 0.99 ± 0.01 | 0.99 ± 0.02 |
| SBP (mm Hg) | 132 ± 3 | 128 ± 4 |
| DBP (mm Hg) | 81 ± 2 | 77 ± 1 |
| HOMA | 7.8 ± 1.3 | 10.9 ± 2.7 |
| QUICKI | 0.296 ± 0.006 | 0.291 ± 0.014 |
| Triacylglycerol (mg/dL) | 126 ± 11 | 228 ± 39 * |
| Total cholesterol (mg/dL) | 184 ± 7 | 207 ± 27 |
| LDL-cholesterol (mg/dL) | 106 ± 7 | 97 ± 6 |
| HDL-cholesterol (mg/dL) | 49 ± 4 | 37 ± 3 |
| Uric acid (mg/dL) | 5.5 ± 0.3 | 6.2 ± 0.8 |
| Creatinine (mg/dL) | 0.82 ± 0.03 | 0.97 ± 0.09 * |
| CRP (mg/L) | 0.8. ± 0.1 | 0.6 ± 0.3 |
| Fibrinogen (mg/dL) | 391 ± 26 | 340 ± 68 |
| von Willebrand factor (%) | 135 ± 11 | 129 ± 21 |
| AST (UI/L) | 16 ± 1 | 20 ± 4 |
| ALT (UI/L) | 27 ± 3 | 31 ± 7 |
| ALP (UI/L) | 78 ± 9 | 69 ± 14 |
| γ-GT (UI/L) | 24 ± 3 | 48 ± 18 *** |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Izaguirre, M.; Gómez-Ambrosi, J.; Rodríguez, A.; Ramírez, B.; Becerril, S.; Valentí, V.; Moncada, R.; Unamuno, X.; Silva, C.; de la Higuera, M.; et al. GLP-1 Limits Adipocyte Inflammation and Its Low Circulating Pre-Operative Concentrations Predict Worse Type 2 Diabetes Remission after Bariatric Surgery in Obese Patients. J. Clin. Med. 2019, 8, 479. https://doi.org/10.3390/jcm8040479
Izaguirre M, Gómez-Ambrosi J, Rodríguez A, Ramírez B, Becerril S, Valentí V, Moncada R, Unamuno X, Silva C, de la Higuera M, et al. GLP-1 Limits Adipocyte Inflammation and Its Low Circulating Pre-Operative Concentrations Predict Worse Type 2 Diabetes Remission after Bariatric Surgery in Obese Patients. Journal of Clinical Medicine. 2019; 8(4):479. https://doi.org/10.3390/jcm8040479
Chicago/Turabian StyleIzaguirre, Maitane, Javier Gómez-Ambrosi, Amaia Rodríguez, Beatriz Ramírez, Sara Becerril, Víctor Valentí, Rafael Moncada, Xabier Unamuno, Camilo Silva, Magdalena de la Higuera, and et al. 2019. "GLP-1 Limits Adipocyte Inflammation and Its Low Circulating Pre-Operative Concentrations Predict Worse Type 2 Diabetes Remission after Bariatric Surgery in Obese Patients" Journal of Clinical Medicine 8, no. 4: 479. https://doi.org/10.3390/jcm8040479