Does Emotional Intelligence Matter in Tough Times? A Moderated Mediation Model for Explaining Health and Suicide Risk amongst Short- and Long-Term Unemployed Adults





Abstract
:1. Introduction
1.1. Emotional Intelligence as a Psychological Resource Explaining Stress and Health Outcomes in Unemployed Individuals
1.2. Purpose, Objectives and Hypotheses of the Research
2. Materials and Methods
2.1. Participants
2.2. Design and Procedure
2.3. Measures
3. Results
3.1. Descriptive Analyses and Correlations
3.2. Testing of Control Variables
3.3. Conditional Process Analyses and Hypotheses Testing
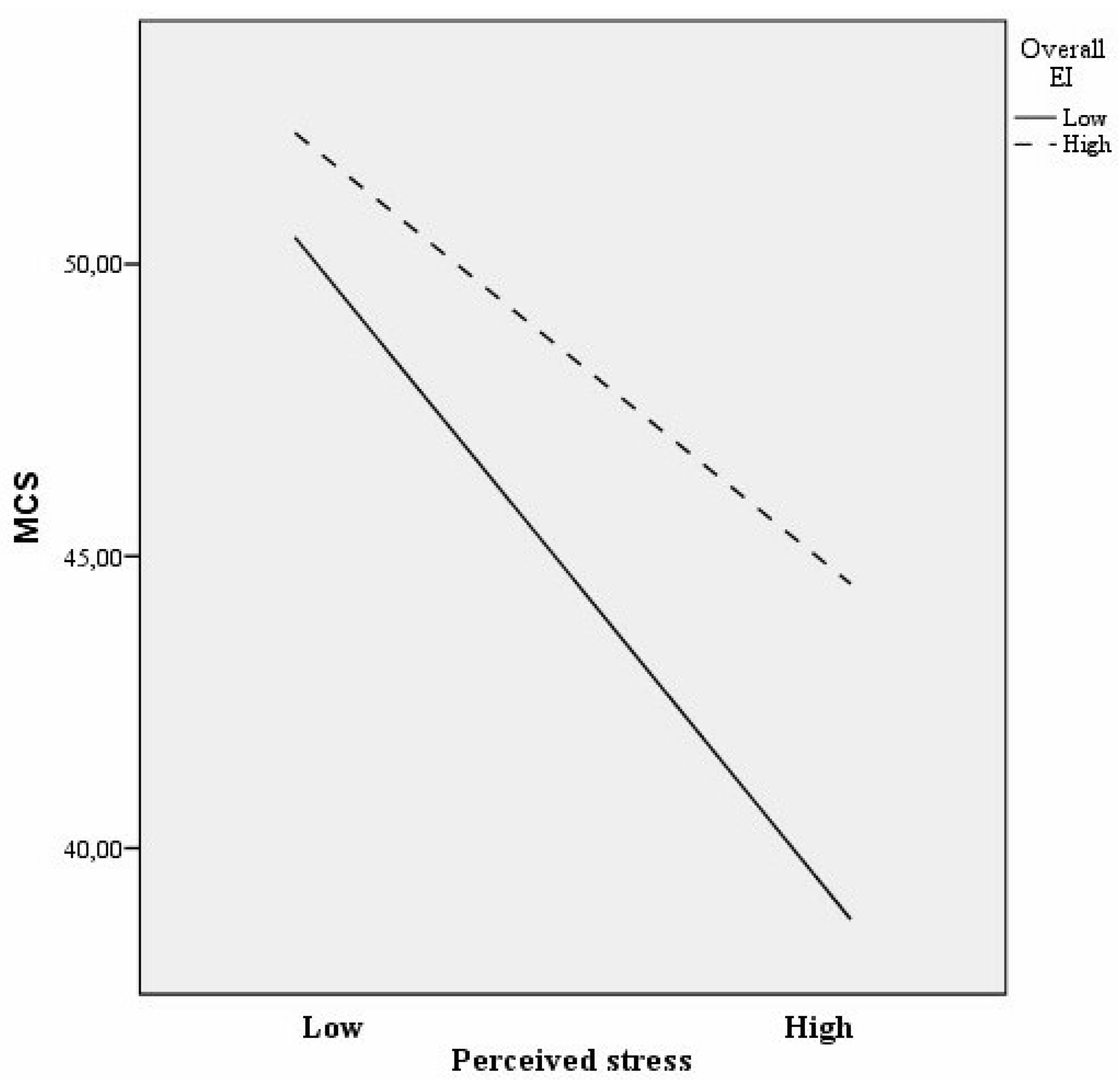
3.3.1. General Mental Health
3.3.2. General Physical Health
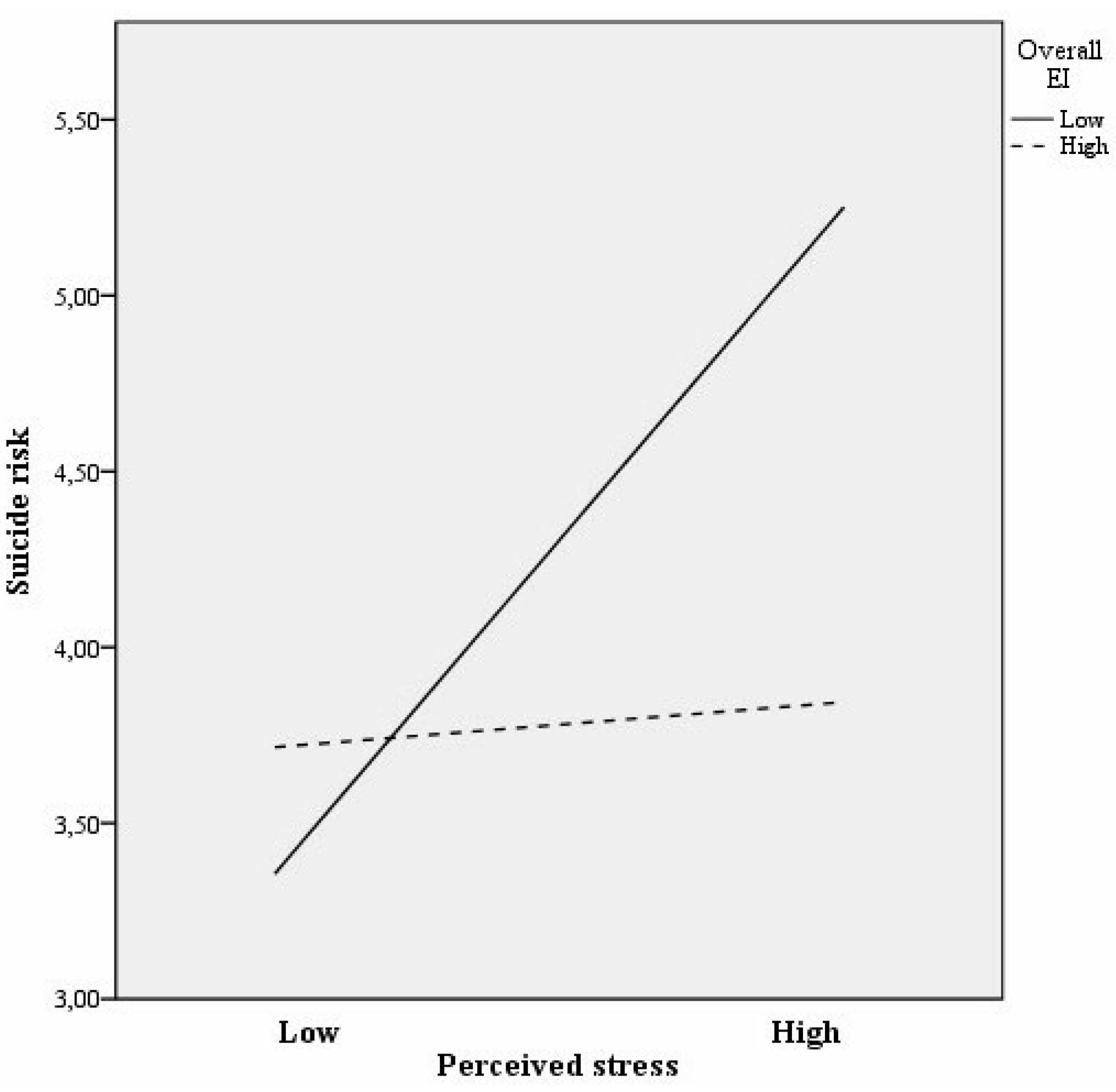
3.3.3. Suicide Risk
4. Discussion
4.1. Limitations
4.2. Implications
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Wanberg, C.R. The Individual Experience of Unemployment. Annu. Rev. Psychol. 2012, 63, 369–396. [Google Scholar] [CrossRef] [PubMed]
- Huppert, F.A. Psychological Well-being: Evidence Regarding its Causes and Consequences. Appl. Psychol. Heal. Well-Being 2009, 1, 137–164. [Google Scholar] [CrossRef]
- Jahoda, M. Employment and Unemployment: A Social-Psychological Analysis; Cambridge University Press: New York, NY, USA, 1982. [Google Scholar]
- McKee-Ryan, F.M.; Song, Z.; Wanberg, C.R.; Kinicki, A.J. Psychological and physical well-being during unemployment: A meta-analytic study. J. Appl. Psychol. 2005, 90, 53–76. [Google Scholar] [CrossRef] [PubMed]
- Paul, K.I.; Moser, K. Unemployment impairs mental health: Meta-analyses. J. Vocat. Behav. 2009, 74, 264–282. [Google Scholar] [CrossRef]
- Béland, F.; Birch, S.; Stoddart, G. Unemployment and health: contextual-level influences on the production of health in populations. Soc. Sci. Med. 2002, 55, 2033–2052. [Google Scholar] [CrossRef]
- Farré, L.; Fasani, F.; Mueller, H. Feeling useless: The effect of unemployment on mental health in the Great Recession. IZA J. Labor Econ. 2018, 7, 8. [Google Scholar] [CrossRef]
- Milner, A.; Page, A.; LaMontagne, A.D. Cause and effect in studies on unemployment, mental health and suicide: A meta-analytic and conceptual review. Psychol. Med. 2014, 44, 909–917. [Google Scholar] [CrossRef] [PubMed]
- Korpi, T. Accumulating disadvantage: Longitudinal analyses of unemployment and physical health in representative samples of the Swedish population. Eur. Sociol. Rev. 2001, 17, 255–273. [Google Scholar] [CrossRef]
- Cohen, S.; Janicki-Deverts, D.; Miller, G.E. Psychological Stress and Disease. JAMA 2007, 298, 1685. [Google Scholar] [CrossRef]
- Schneiderman, N.; Ironson, G.; Siegel, S.D. Stress and Health: Psychological, Behavioral, and Biological Determinants. Annu. Rev. Clin. Psychol. 2005, 1, 607–628. [Google Scholar] [CrossRef] [Green Version]
- Turecki, G.; Brent, D.A. Suicide and suicidal behaviour. Lancet 2016, 387, 1227–1239. [Google Scholar] [CrossRef]
- Langens, T.A.; Mose, E. Coping with unemployment: Relationships between duration of unemployment, coping styles, and subjective well-being. J. Appl. Biobehav. Res. 2006, 11, 189–208. [Google Scholar] [CrossRef]
- Elsby, M.W.; Hobijn, B.; Sahin, A. The labor market in the Great Recession. Brookings Pap. Econ. Act. 2010. [Google Scholar] [CrossRef]
- Bentolila, S.; García-Pérez, J.I.; Jansen, M. Are the Spanish long-term unemployed unemployable? SERIEs 2017, 8, 1–41. [Google Scholar] [CrossRef] [Green Version]
- Griep, Y.; Baillien, E.; Vleugels, W.; Rothmann, S.; De Witte, H. Do they adapt or react? A comparison of the adaptation model and the stress reaction model among South African unemployed. Econ. Ind. Democr. 2014, 35, 717–736. [Google Scholar] [CrossRef]
- De Witte, H.; Hooge, J.; Vanbelle, E. Do the long-term unemployed adapt to unemployment? Rom. J. Pplied Psychol. 2010, 12, 8–14. [Google Scholar]
- Creed, P.A.; Lehmann, K.; Hood, M. The relationship between core self-evaluations, employment commitment and well-being in the unemployed. Pers. Individ. Dif. 2009, 47, 310–315. [Google Scholar] [CrossRef] [Green Version]
- Extremera, N.; Rey, L. Attenuating the Negative Impact of Unemployment: The Interactive Effects of Perceived Emotional Intelligence and Well-Being on Suicide Risk. PLoS ONE 2016, 11, e0163656. [Google Scholar] [CrossRef]
- McKee-Ryan, F.M.; Kinicki, A.J. The personal meaning of job loss: Appraisal and coping at the facet level. Int. Rev. Ind. Organ. Psychol. 2002, 17, 5–45. [Google Scholar]
- Matthews, G.; Zeidner, M.; Roberts, R.D. Emotional Intelligence, Health, and Stress. In The Handbook of Stress and Health: A Guide to Research and Practice; Cooper, C.L., Quick, J.C., Eds.; Wiley-Blackwell: Chichester, UK, 2017; pp. 312–326. [Google Scholar]
- Martins, A.; Ramalho, N.; Morin, E. A comprehensive meta-analysis of the relationship between Emotional Intelligence and health. Pers. Individ. Dif. 2010, 49, 554–564. [Google Scholar] [CrossRef]
- Mayer, J.D.; Salovey, P. What is emotional intelligence? In Emotional Development and Emotional Intelligence: Implications for Educators; Salovey, P., Sluyter, D., Eds.; Basic Books: New York, NY, USA, 1997; pp. 3–31. ISBN 0465095879. [Google Scholar]
- Domínguez-García, E.; Fernández-Berrocal, P. The Association Between Emotional Intelligence and Suicidal Behavior: A Systematic Review. Front. Psychol. 2018, 9, 2380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikolajczak, M.; Roy, E.; Luminet, O.; Fillée, C.; de Timary, P. The moderating impact of emotional intelligence on free cortisol responses to stress. Psychoneuroendocrinology 2007, 32, 1000–1012. [Google Scholar] [CrossRef] [PubMed]
- Salovey, P.; Stroud, L.R.; Woolery, A.; Epel, E.S. Perceived Emotional Intelligence, Stress Reactivity, and Symptom Reports: Further Explorations Using the Trait Meta-Mood Scale. Psychol. Health 2002, 17, 611–627. [Google Scholar] [CrossRef]
- Berrios, M.P.; Extremera, N.; Nieto-Flores, M.P. Exploring the socio-emotional factors associated with subjective well-being in the unemployed. PeerJ 2016, 4, e2506. [Google Scholar] [CrossRef] [PubMed]
- Knopp, K.A. Exploring the relationship of emotional intelligence with mental health status in polish unemployed persons–differences between men and women. Polish Psychol. Bull. 2016, 47, 436–444. [Google Scholar] [CrossRef]
- Hodzic, S.; Ripoll, P.; Bernal, C.; Zenasni, F. The Effects of Emotional Competences Training among Unemployed Adults: A Longitudinal Study. Appl. Psychol. Heal. Well-Being 2015, 7, 275–292. [Google Scholar] [CrossRef]
- O’Connell, P.J.; Mcguinness, S.; Kelly, E. The transition from short- to long-term unemployment: A statistical profiling model for Ireland. Econ. Soc. Rev. 2012, 43, 135–164. [Google Scholar]
- Maier, R.; Egger, A.; Barth, A.; Winker, R.; Osterode, W.; Kundi, M.; Wolf, C.; Ruediger, H. Effects of short- and long-term unemployment on physical work capacity and on serum cortisol. Int. Arch. Occup. Environ. Health 2006, 79, 193–198. [Google Scholar] [CrossRef]
- Hendricks, V.M.; Blanken, P. Snowball sampling: Theoretical and practical considerations. In Snowball Sampling: A Pilot Study on Cocaine Use; Hendricks, V.M., Blanken, P., Adriaans, N., Eds.; Instituut Voor Onderzoek IVO: Rotterdam, The Netherlands, 1992; pp. 17–35. [Google Scholar]
- Blau, G.; Petrucci, T.; McClendon, J. Correlates of life satisfaction and unemployment stigma and the impact of length of unemployment on a unique unemployed sample. Career Dev. Int. 2013, 18, 257–280. [Google Scholar] [CrossRef]
- Extremera, N.; Rey, L. Health-related quality of life and cognitive emotion regulation strategies in the unemployed: a cross-sectional survey. Health Qual. Life Outcomes 2014, 12, 172. [Google Scholar] [CrossRef]
- Mérida-López, S.; Extremera, N.; Rey, L. Understanding the Links Between Self-Report Emotional Intelligence and Suicide Risk: Does Psychological Distress Mediate This Relationship Across Time and Samples? Front. Psychiatry 2018, 9, 184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Extremera, N.; Rey, L.; Sánchez-Álvarez, N. Validation of the Spanish version of Wong Law Emotional Intelligence Scale (WLEIS-S). Psicothema 2019, 31, 94–100. [Google Scholar] [CrossRef]
- Law, K.S.; Wong, C.-S.; Song, L.J. The construct and criterion validity of emotional intelligence and its potential utility for management studies. J. Appl. Psychol. 2004, 89, 483–496. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A Global Measure of Perceived Stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Remor, E.; Carrobles, J. Versión Española de la Escala de Estrés Percibido (PSS-14): Estudio psicométrico en una muestra VIH+. Ansiedad y Estrés 2001, 7, 195–201. [Google Scholar]
- Extremera, N.; Rey, L. The moderator role of emotion regulation ability in the link between stress and well-being. Front. Psychol. 2015, 6, 1632. [Google Scholar] [CrossRef] [PubMed]
- Vilagut, G.; Valderas, J.M.; Ferrer, M.; Garin, O.; López-García, E.; Alonso, J. Interpretación de los cuestionarios de salud SF-36 y SF-12 en España: Componentes físico y mental. Med. Clin. 2008, 130, 726–735. [Google Scholar] [CrossRef]
- Ware, J.E.; Kosinski, M.; Keller, S.D. A 12-Item Short-Form Health Survey. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osman, A.; Bagge, C.L.; Gutierrez, P.M.; Konick, L.C.; Kopper, B.A.; Barrios, F.X. The Suicidal Behaviors Questionnaire-Revised (SBQ-R):Validation with Clinical and Nonclinical Samples. Assessment 2001, 8, 443–454. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-based Approach; Guilford Press: New York, NY, USA, 2013; ISBN 9781609182304. [Google Scholar]
- Overholser, J.C.; Braden, A.; Dieter, L. Understanding suicide risk: Identification of high-risk groups during high-risk times. J. Clin. Psychol. 2012, 68, 349–361. [Google Scholar] [CrossRef]
- Hayes, A.F. An Index and Test of Linear Moderated Mediation. Multivariate Behav. Res. 2015, 50, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Mikolajczak, M.; Avalosse, H.; Vancorenland, S.; Verniest, R.; Callens, M.; van Broeck, N.; Fantini-Hauwel, C.; Mierop, A. A nationally representative study of emotional competence and health. Emotion 2015, 15, 653–667. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.H. Review of the psychometric evidence of the perceived stress scale. Asian Nurs. Res. 2012, 6, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Goldman, S.L.; Kraemer, D.T.; Salovey, P. Beliefs about mood moderate the relationship of stress to illness and symptom reporting. J. Psychosom. Res. 1996, 41, 115–128. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| M | SD | α | 1 | 2 | 3 | 4 | 5 | |
|---|---|---|---|---|---|---|---|---|
| Sample 1 (n = 364) | ||||||||
| 1. Emotional Intelligence | 5.06 | 0.96 | 0.92 | - | ||||
| 2. Perceived stress | 1.59 | 0.66 | 0.66 | −0.38 ** | - | |||
| 3. MCS | 47.64 | 10.19 | 0.76 | 0.31 ** | −0.47 ** | - | ||
| 4. PCS | 52.02 | 6.95 | 0.67 | 0.19 ** | −0.20 ** | 0.11 * | - | |
| 5. Suicide risk | 4.21 | 2.18 | 0.77 | −0.26 ** | 0.25 ** | −0.35 ** | −0.19 ** | - |
| Sample 2 (n = 594) | ||||||||
| 1. Emotional Intelligence | 5.00 | 1.02 | 0.92 | - | ||||
| 2. Perceived stress | 1.70 | 0.71 | 0.68 | −0.40 ** | - | |||
| 3. MCS | 46.11 | 10.95 | 0.76 | 0.36 ** | −0.51 ** | - | ||
| 4. PCS | 50.87 | 8.36 | 0.76 | 0.12 ** | −0.12 ** | 0.04 | - | |
| 5. Suicide risk | 4.22 | 2.44 | 0.80 | −0.24 ** | 0.25 ** | −0.36 ** | −0.11 ** | - |
| B | SE b | R2 | 95% CI | |
|---|---|---|---|---|
| Mental Composite Summary | 0.28 ** | |||
| Constant | 54.13 ** | 1.98 | 50.24 to 58.02 | |
| Gender | −3.16 ** | 0.93 | −4.98 to −1.34 | |
| Age | −0.04 | 0.04 | −0.13 to 0.05 | |
| EI | 1.43 ** | 0.52 | 0.40 to 2.45 | |
| Perceived stress | −6.45 ** | 0.76 | −7.93 to −4.96 | |
| EI x perceived stress | 1.14 | 0.67 | −0.17 to 2.45 | |
| Physical Composite Summary | 0.08 ** | |||
| Constant | 56.98 ** | 1.52 | 53.99 to 59.97 | |
| Gender | −1.18 | 0.71 | −2.58 to 0.22 | |
| Age | −0.09 | 0.03 | −0.16 to −0.03 | |
| EI | 0.93 | 0.40 | 0.14 to 1.72 | |
| Perceived stress | −1.38 | 0.58 | −2.52 to −0.23 | |
| EI x perceived stress | 0.19 | 0.51 | −0.82 to 1.20 | |
| Suicide risk | 0.11 ** | |||
| Constant | 3.82 ** | 0.47 | 2.90 to 4.75 | |
| Gender | 0.24 | 0.22 | −0.19 to 0.67 | |
| Age | −0.00 | 0.01 | −0.02 to 0.02 | |
| EI | −0.39 ** | 0.12 | −0.64 to −0.15 | |
| Perceived stress | 0.62 ** | 0.18 | 0.27 to 0.98 | |
| EI x perceived stress | −0.32 | 0.16 | −0.63 to −0.00 |
| B | SE b | R2 | 95% CI | |
|---|---|---|---|---|
| Mental Composite Summary | 0.31 ** | |||
| Constant | 48.45 ** | 1.70 | 45.10 to 51.80 | |
| Gender | −2.09 ** | 0.76 | −3.59 to −0.60 | |
| Age | 0.03 | 0.03 | −0.03 to 0.10 | |
| EI | 1.85 ** | 0.42 | 1.04 to 2.67 | |
| Perceived stress | −6.81 ** | 0.58 | −7.95 to −5.67 | |
| EI x perceived stress | 1.37 ** | 0.46 | 0.46 to 2.27 | |
| Physical Composite Summary | 0.08 ** | |||
| Constant | 58.47 ** | 1.50 | 55.53 to 61.41 | |
| Gender | −0.81 | 0.67 | −2.12 to 0.51 | |
| Age | −0.17 ** | 0.03 | −0.23 to −0.12 | |
| EI | 0.98 ** | 0.37 | 0.27 to 1.70 | |
| Perceived stress | −0.65 | 0.51 | −1.66 to 0.35 | |
| EI x perceived stress | −0.24 | 0.41 | −1.04 to 0.56 | |
| Suicide risk | 0.13 ** | |||
| Constant | 4.71 ** | 0.43 | 3.88 to 5.55 | |
| Gender | −0.05 | 0.19 | −0.43 to 0.32 | |
| Age | −0.02 | 0.01 | −0.03 to 0.00 | |
| EI | −0.26 | 0.10 | −0.46 to −0.05 | |
| Perceived stress | 0.71 ** | 0.15 | 0.43 to 0.99 | |
| EI x perceived stress | −0.61 ** | 0.12 | −0.84 to −0.38 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mérida-López, S.; Extremera, N.; Quintana-Orts, C.; Rey, L. Does Emotional Intelligence Matter in Tough Times? A Moderated Mediation Model for Explaining Health and Suicide Risk amongst Short- and Long-Term Unemployed Adults. J. Clin. Med. 2019, 8, 797. https://doi.org/10.3390/jcm8060797
Mérida-López S, Extremera N, Quintana-Orts C, Rey L. Does Emotional Intelligence Matter in Tough Times? A Moderated Mediation Model for Explaining Health and Suicide Risk amongst Short- and Long-Term Unemployed Adults. Journal of Clinical Medicine. 2019; 8(6):797. https://doi.org/10.3390/jcm8060797
Chicago/Turabian StyleMérida-López, Sergio, Natalio Extremera, Cirenia Quintana-Orts, and Lourdes Rey. 2019. "Does Emotional Intelligence Matter in Tough Times? A Moderated Mediation Model for Explaining Health and Suicide Risk amongst Short- and Long-Term Unemployed Adults" Journal of Clinical Medicine 8, no. 6: 797. https://doi.org/10.3390/jcm8060797