Efficacy and Safety of Ceftaroline for the Treatment of Community-Acquired Pneumonia: A Systemic Review and Meta-Analysis of Randomized Controlled Trials


Abstract
:1. Introduction
2. Methods
2.1. Study Search and Selection
2.2. Definitions and Outcomes
2.3. Data Analysis
3. Results
3.1. Study Characteristics and Study Quality
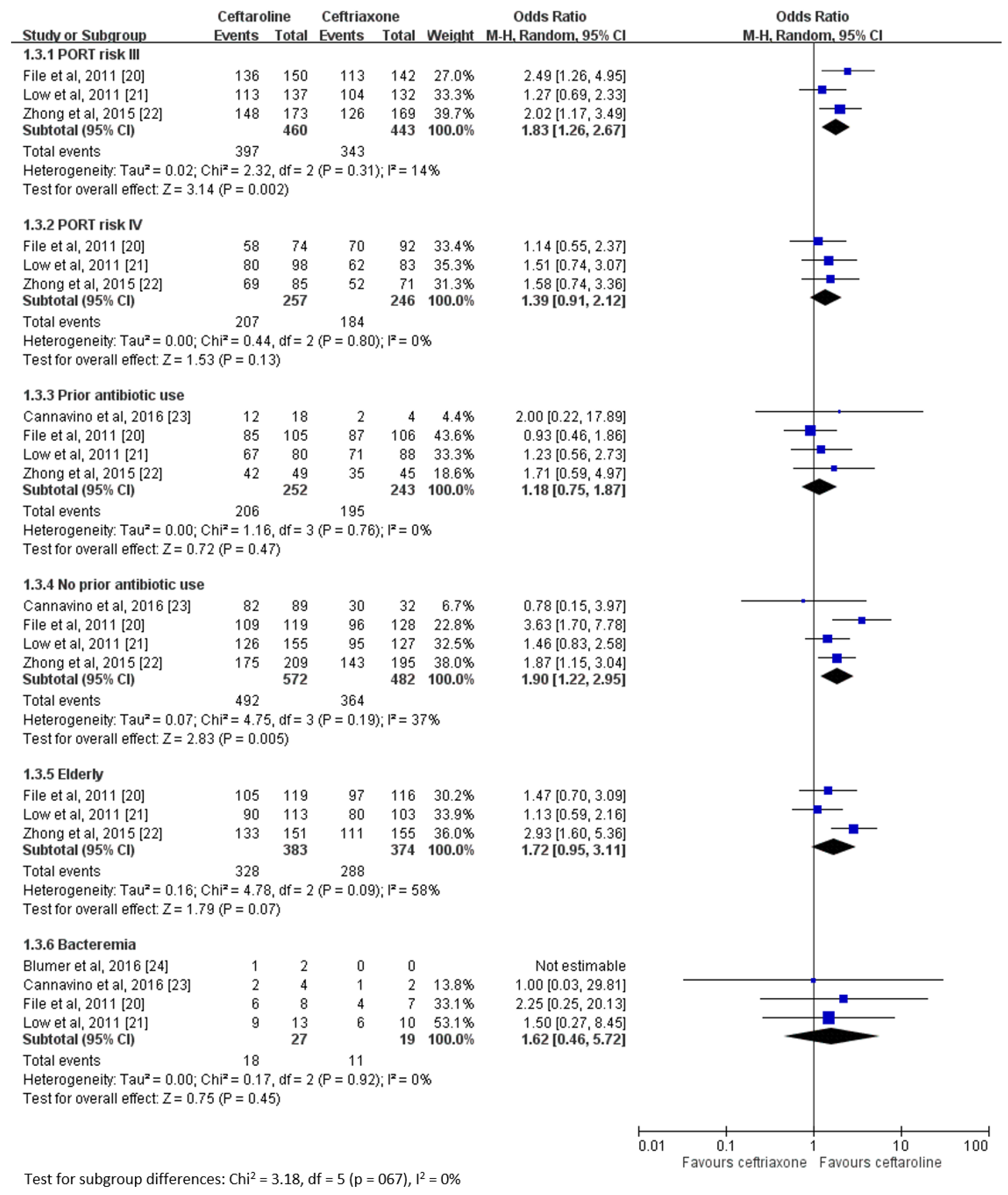
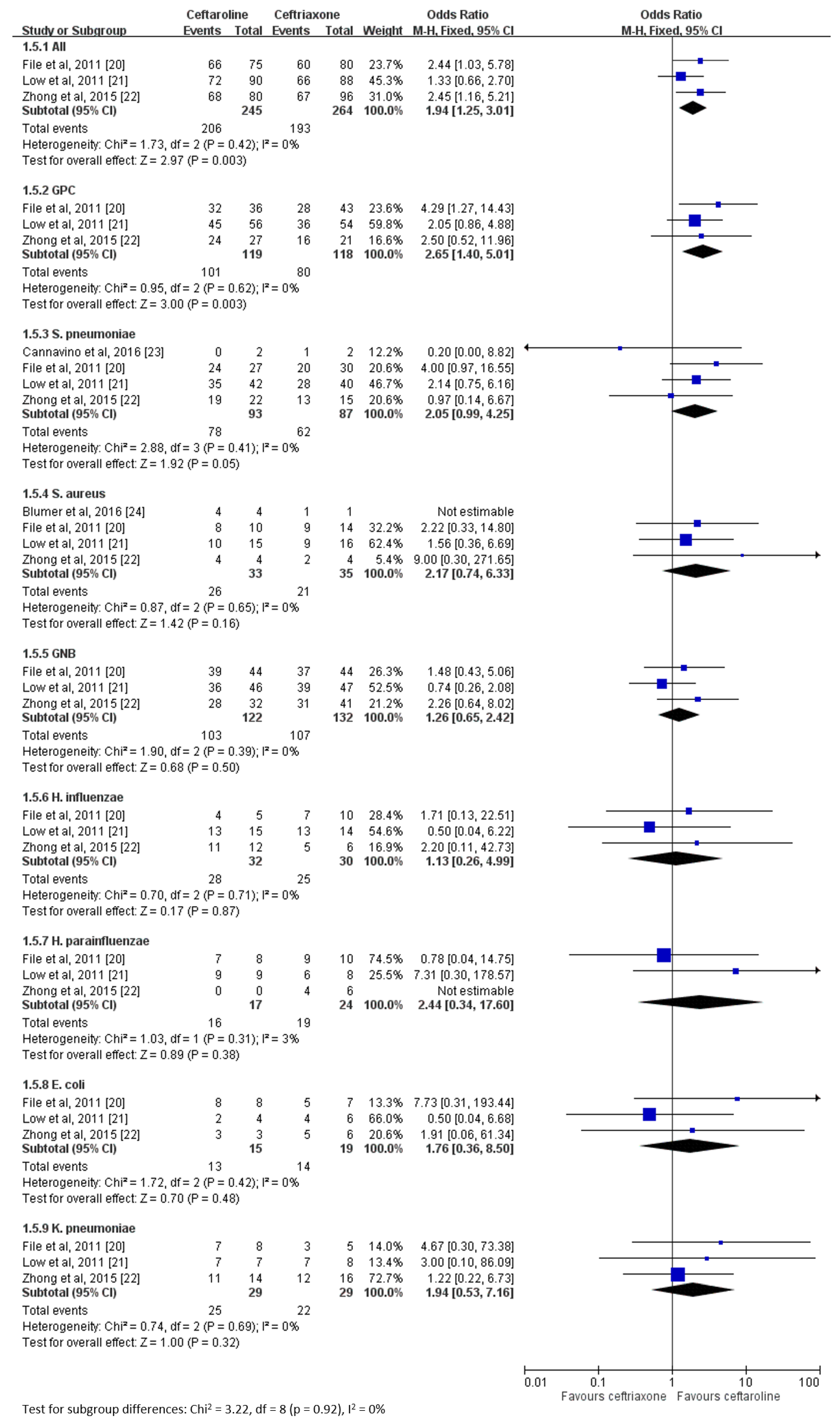
3.2. Clinical Efficacy
3.3. Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Le Roux, D.M.; Zar, H.J. Community-acquired pneumonia in children—A changing spectrum of disease. Pediatr. Radiol. 2017, 47, 1392–1398. [Google Scholar] [CrossRef] [PubMed]
- Musher, D.M.; Thorner, A.R. Community-acquired pneumonia. N. Engl. J. Med. 2014, 37, 1619–1628. [Google Scholar] [CrossRef] [PubMed]
- Peyrani, P.; Mandell, L.; Torres, A.; Tillotson, G.S. The burden of community-acquired bacterial pneumonia in the era of antibiotic resistance. Expert Rev. Respir. Med. 2019, 13, 139–152. [Google Scholar] [CrossRef] [PubMed]
- Cilloniz, C.; Dominedo, C.; Garcia-Vidal, C.; Torres, A. Community-acquired pneumonia as an emergency condition. Curr. Opin. Crit. Care 2018, 24, 531–539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leoni, D.; Rello, J. Severe community-acquired pneumonia: Optimal management. Curr. Opin. Infect. Dis. 2017, 30, 240–247. [Google Scholar] [CrossRef] [PubMed]
- Pereira, J.M.; Goncalves-Pereira, J.; Ribeiro, O.; Baptista, J.P.; Froes, F.; Paiva, J.A. Impact of antibiotic therapy in severe community-acquired pneumonia: Data from the Infauci study. J. Crit. Care 2018, 43, 183–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wunderink, R.G.; Yin, Y. Antibiotic Resistance in Community-Acquired Pneumonia Pathogens. Semin. Respir. Crit. Care Med. 2016, 37, 829–838. [Google Scholar]
- Cilloniz, C.; Dominedo, C.; Nicolini, A.; Torres, A. PES Pathogens in Severe Community-Acquired Pneumonia. Microorganisms 2019, 7, 49. [Google Scholar] [CrossRef]
- Torres, A.; Chalmers, J.D.; Dela Cruz, C.S.; Dominedo, C.; Kollef, M.; Martin-Loeches, I.; Niederman, M.; Wunderink, R.G. Challenges in severe community-acquired pneumonia: A point-of-view review. Intensiv. Care Med. 2019, 45, 159–171. [Google Scholar] [CrossRef]
- Thomas, R.; Ferguson, J.; Coombs, G.; Gibson, P.G. Community-acquired methicillin-resistant Staphylococcus aureus pneumonia: A clinical audit. Respirology 2011, 16, 926–931. [Google Scholar] [CrossRef]
- Chou, C.C.; Shen, C.F.; Chen, S.J.; Chen, H.M.; Wang, Y.C.; Chang, W.S.; Chang, Y.T.; Chen, W.Y.; Huang, C.Y.; Kuo, C.C.; et al. Recommendations and guidelines for the treatment of pneumonia in Taiwan. J. Microbiol. Immunol. Infect. 2019, 52, 172–199. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Bayer, A.; Cosgrove, S.E.; Daum, R.S.; Fridkin, S.K.; Gorwitz, R.J.; Kaplan, S.L.; Karchmer, A.W.; Levine, D.P.; Murray, B.E.; et al. Clinical practice guidelines by the infectious diseases society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin. Infect. Dis. 2011, 52, e18–e55. [Google Scholar] [CrossRef] [PubMed]
- Lim, W.S.; Baudouin, S.V.; George, R.C.; Hill, A.T.; Jamieson, C.; Le Jeune, I.; Macfarlane, J.T.; Read, R.C.; Roberts, H.J.; Levy, M.L.; et al. BTS guidelines for the management of community acquired pneumonia in adults: Update 2009. Thorax 2009, 64 (Suppl. 3), iii1–55. [Google Scholar] [CrossRef]
- Pfaller, M.A.; Mendes, R.E.; Duncan, L.R.; Flamm, R.K.; Sader, H.S. In Vitro Activities of Ceftaroline and Comparators against Streptococcus pneumoniae Isolates from U.S. Hospitals: Results from Seven Years of the AWARE Surveillance Program (2010 to 2016). Antimicrob. Agents Chemother. 2018, 62, e01555-17. [Google Scholar] [CrossRef] [PubMed]
- Pfaller, M.A.; Mendes, R.E.; Castanheira, M.; Flamm, R.K.; Jones, R.N.; Sader, H.S. Ceftaroline Activity Tested Against Bacterial Isolates Causing Community-acquired Respiratory Tract Infections and Skin and Skin Structure Infections in Pediatric Patients From United States Hospitals: 2012–2014. Pediatr. Infect. Dis. J. 2017, 36, 486–491. [Google Scholar] [CrossRef]
- Karlowsky, J.A.; Biedenbach, D.J.; Bouchillon, S.K.; Hackel, M.; Iaconis, J.P.; Sahm, D.F. In vitro activity of Ceftaroline against bacterial pathogens isolated from patients with skin and soft tissue and respiratory tract infections in African and Middle Eastern countries: AWARE global surveillance program 2012–2014. Diagn. Microbiol. Infect. Dis. 2016, 86, 194–199. [Google Scholar] [CrossRef]
- Biedenbach, D.J.; Iaconis, J.P.; Sahm, D.F. Comparative in vitro activities of ceftaroline and ceftriaxone against bacterial pathogens associated with respiratory tract infections: Results from the AWARE surveillance study. J. Antimicrob. Chemother. 2016, 71, 3459–3464. [Google Scholar] [CrossRef]
- Sader, H.S.; Farrell, D.J.; Mendes, R.E.; Flamm, R.K.; Castanheira, M.; Jones, R.N. Antimicrobial activity of ceftaroline tested against bacterial isolates causing respiratory tract and skin and skin structure infections in US medical centers in 2013. Diagn. Microbiol. Infect. Dis. 2015, 82, 78–84. [Google Scholar] [CrossRef]
- Poon, H.; Chang, M.H.; Fung, H.B. Ceftaroline fosamil: A cephalosporin with activity against methicillin-resistant Staphylococcus aureus. Clin. Ther. 2012, 34, 743–765. [Google Scholar] [CrossRef]
- File, T.M., Jr.; Low, D.E.; Eckburg, P.B.; Talbot, G.H.; Friedland, H.D.; Lee, J.; Llorens, L.; Critchley, I.A.; Thye, D.A.; Pullman, J.; et al. FOCUS 1: A randomized, double-blinded, multicentre, Phase III trial of the efficacy and safety of ceftaroline fosamil versus ceftriaxone in community-acquired pneumonia. J. Antimicrob. Chemother. 2011, 66 (Suppl. 3), iii19–32. [Google Scholar] [CrossRef]
- Low, D.E.; File, T.M., Jr.; Eckburg, P.B.; Talbot, G.H.; David Friedland, H.; Lee, J.; Llorens, L.; Critchley, I.A.; Thye, D.A.; Corral, J.; et al. FOCUS 2: A randomized, double-blinded, multicentre, Phase III trial of the efficacy and safety of ceftaroline fosamil versus ceftriaxone in community-acquired pneumonia. J. Antimicrob. Chemother. 2011, 66 (Suppl. 3), iii33–44. [Google Scholar] [CrossRef] [PubMed]
- Zhong, N.S.; Sun, T.; Zhuo, C.; D’Souza, G.; Lee, S.H.; Lan, N.H.; Chiang, C.-H.; Wilson, D.; Sun, F.; Iaconis, J.; et al. Ceftaroline fosamil versus ceftriaxone for the treatment of Asian patients with community-acquired pneumonia: A randomised, controlled, double-blind, phase 3, non-inferiority with nested superiority trial. Lancet Infect. Dis. 2015, 15, 161–171. [Google Scholar] [CrossRef]
- Cannavino, C.R.; Nemeth, A.; Korczowski, B.; Bradley, J.S.; O’Neal, T.; Jandourek, A.; Friedland, H.D.; Kaplan, S.L. A Randomized, Prospective Study of Pediatric Patients with Community-acquired Pneumonia Treated with Ceftaroline Versus Ceftriaxone. Pediatr. Infect. Dis. J. 2016, 35, 752–759. [Google Scholar] [CrossRef] [PubMed]
- Blumer, J.L.; Ghonghadze, T.; Cannavino, C.; O’Neal, T.; Jandourek, A.; Friedland, H.D.; Bradley, J. A Multicenter, Randomized, Observer-blinded, Active-controlled Study Evaluating the Safety and Effectiveness of Ceftaroline Compared with Ceftriaxone Plus Vancomycin in Pediatric Patients With Complicated Community-acquired Bacterial Pneumonia. Pediatr. Infect. Dis. J. 2016, 35, 760–766. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Fine, M.J.; Auble, T.E.; Yealy, D.M.; Hanusa, B.H.; Weissfeld, L.A.; Singer, D.E.; Coley, C.M.; Marrie, T.J.; Kapoor, W.N. A prediction rule to identify low-risk patients with community-acquired pneumonia. N. Engl. J. Med. 1997, 336, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Rhedin, S.; Lindstrand, A.; Hjelmgren, A.; Ryd-Rinder, M.; Öhrmalm, L.; Tolfvenstam, T.; Örtqvist, Å.; Rotzén-Östlund, M.; Zweygberg-Wirgart, B.; Henriques-Normark, B.; et al. Respiratory viruses associated with community-acquired pneumonia in children: Matched case-control study. Thorax 2015, 70, 847–853. [Google Scholar] [CrossRef]
- Sotgiu, G.; Aliberti, S.; Gramegna, A.; Mantero, M.; Di Pasquale, M.; Trogu, F.; Saderi, L.; Blasi, F. Efficacy and effectiveness of Ceftaroline Fosamil in patients with pneumonia: A systematic review and meta-analysis. Respir. Res. 2018, 19, 205. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study, Published Year | Study Design | Study Period | Study Population | No of Patients | Dose Regimen | ||
|---|---|---|---|---|---|---|---|
| Ceftaroline | Comparator | Ceftaroline | Comparator | ||||
| File et al., 2011 [20] | Multicenter, multinational, double-blinded, randomized trial | January 2008 to December 2008 | Adult patients with PORT risk class III or IV CAP requiring hospitalization and IV therapy | 304 | 309 | 600 mg q12 h | Ceftriaxone 1 g q24 h |
| Low et al., 2011 [21] | Multicenter, multinational, double-blinded, randomized trial | 2007–2009 | Patients (aged ≥18 years) with PORT risk class III or IV CAP requiring hospitalization and IV therapy | 317 | 310 | 600 mg q12 h | Ceftriaxone 1 g q24 h |
| Zhong et al., 2015 [22] | Multicenter, multinational, double-blinded, randomized trial | 2011–2013 | Adult Asian patients with PORT risk class III–IV CAP | 381 | 382 | 600 mg q12 h | Ceftriaxone 2 g q24 h |
| Cannavino et al., 2016 [23] | Multicenter, multinational, randomized | 2012–2014 | Ages of 2 months and <18 years with CAP requiring hospitalization and IV antibacterial therapy | 121 | 39 | Age < 6 m, 8 mg/kg q8 h; aged ≥ 6 m, 12 mg/kg q8 h for those weighing ≤ 33 kg or 400 mg q8 h for those weighing >33 kg | Ceftriaxone 75 mg/kg/d to a maximum 4g/d q12 h |
| Blumer et al., 2016 [24] | Multicenter, multinational randomized, observe-blinded | 2012–2014 | Pediatric patients between 2 months and 17 years of age with complicated CAP | 30 | 10 | 15 mg/kg or 600 mg q8 h if weight > 40 kg if ≥6 m or 10 mg/kg q8 h if <6 m | Ceftriaxone, 75 mg/kg/d q12 h, and vancomycin 15 mg/kg q6 h |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lan, S.-H.; Chang, S.-P.; Lai, C.-C.; Lu, L.-C.; Chao, C.-M. Efficacy and Safety of Ceftaroline for the Treatment of Community-Acquired Pneumonia: A Systemic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2019, 8, 824. https://doi.org/10.3390/jcm8060824
Lan S-H, Chang S-P, Lai C-C, Lu L-C, Chao C-M. Efficacy and Safety of Ceftaroline for the Treatment of Community-Acquired Pneumonia: A Systemic Review and Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine. 2019; 8(6):824. https://doi.org/10.3390/jcm8060824
Chicago/Turabian StyleLan, Shao-Huan, Shen-Peng Chang, Chih-Cheng Lai, Li-Chin Lu, and Chien-Ming Chao. 2019. "Efficacy and Safety of Ceftaroline for the Treatment of Community-Acquired Pneumonia: A Systemic Review and Meta-Analysis of Randomized Controlled Trials" Journal of Clinical Medicine 8, no. 6: 824. https://doi.org/10.3390/jcm8060824