Artificial Intelligence Prediction Model for the Cost and Mortality of Renal Replacement Therapy in Aged and Super-Aged Populations in Taiwan

 ,
,
Abstract
:1. Introduction
2. Method
2.1. Data Source and Sampled Participants
2.2. Data Availability Statement
2.3. Ethics Statement
2.4. Variables of Interest
2.5. Training Dataset Development
2.6. Algorithm Training
2.6.1. Cost Regression Model
2.6.2. Mortality Classification Model
2.6.3. Evaluation of Models
2.7. Statistical Analyses of Demographic Features
3. Results
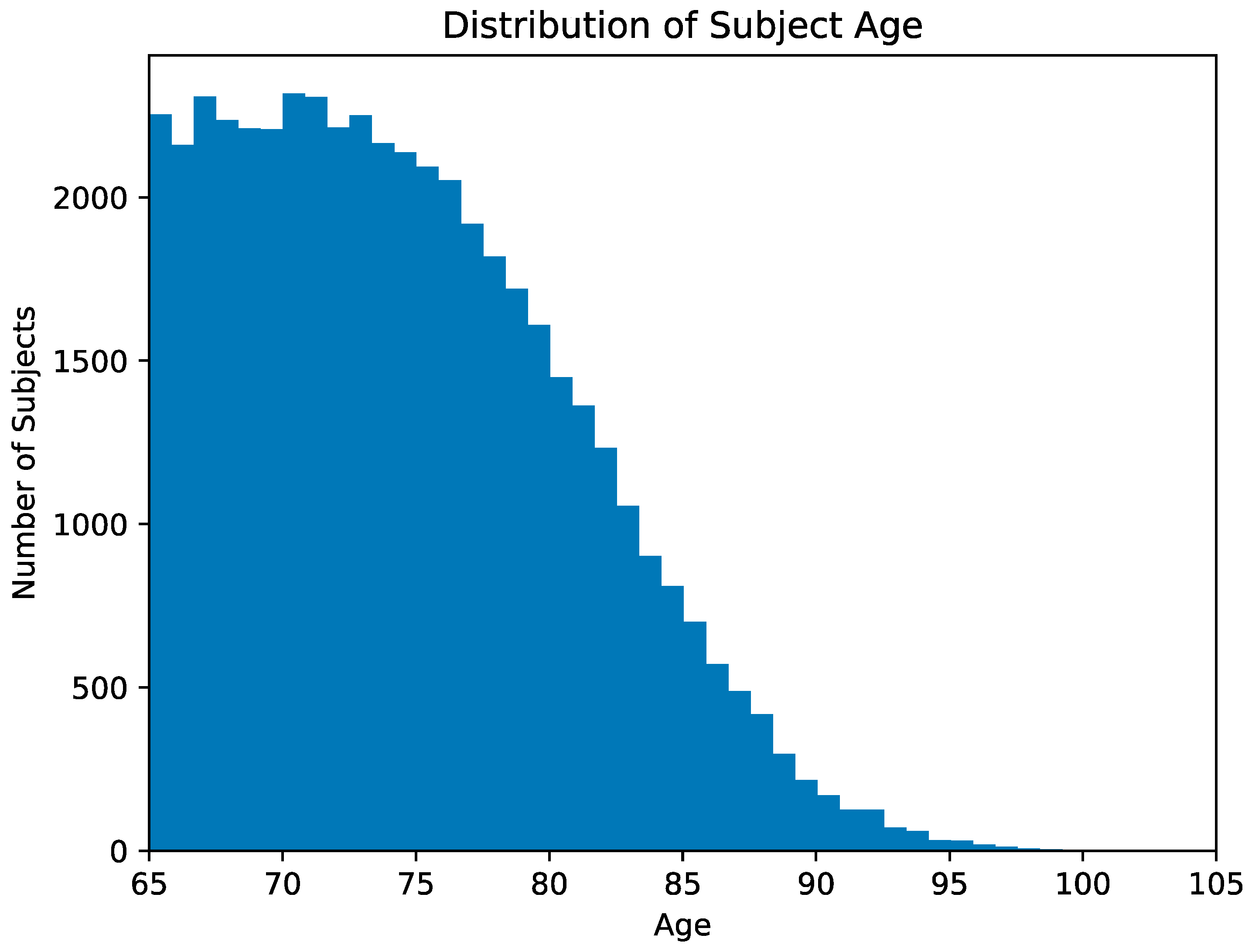
3.1. Demographic Features of Patients
3.2. Evaluation of Prediction Models
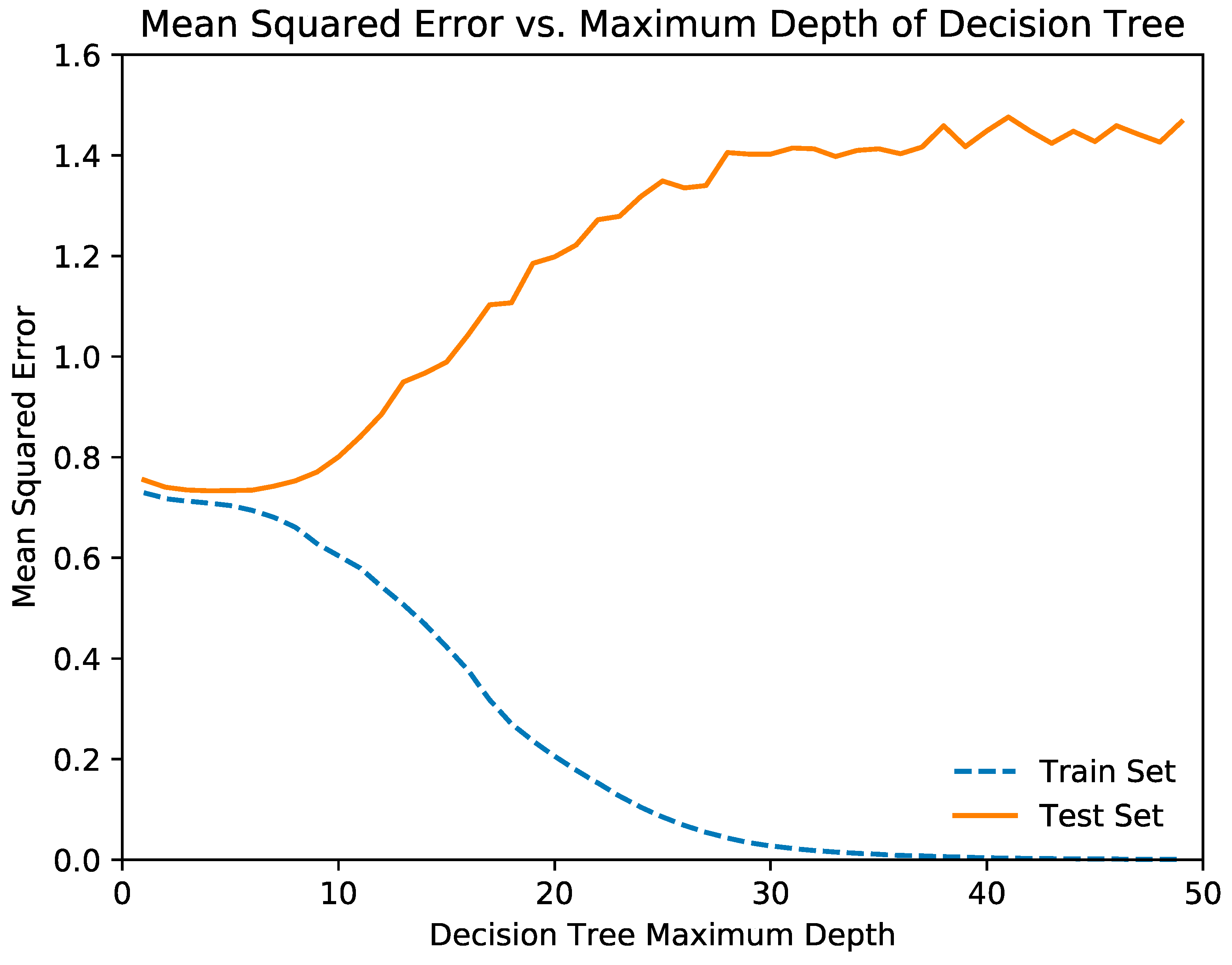
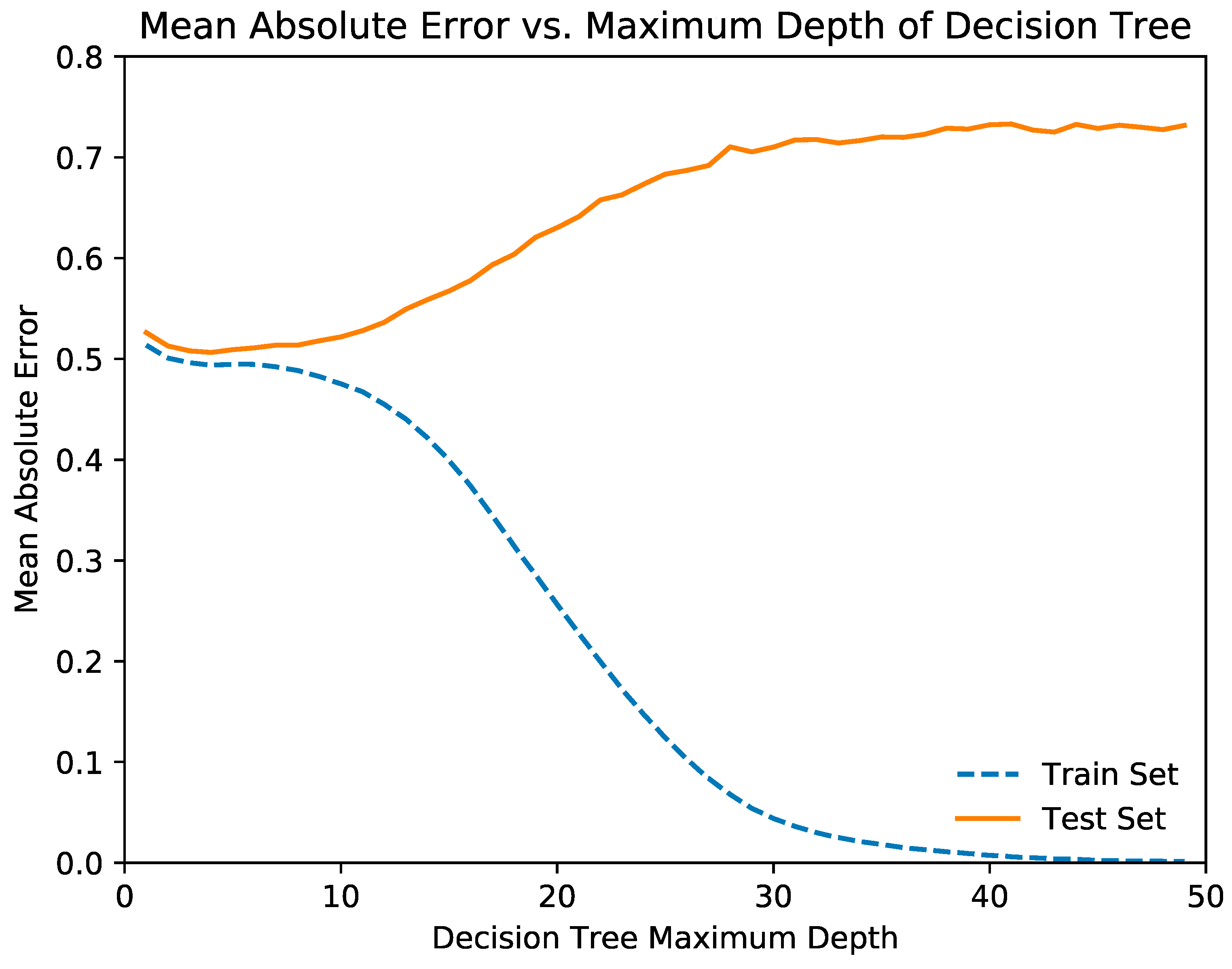
3.2.1. Cost Regression Model
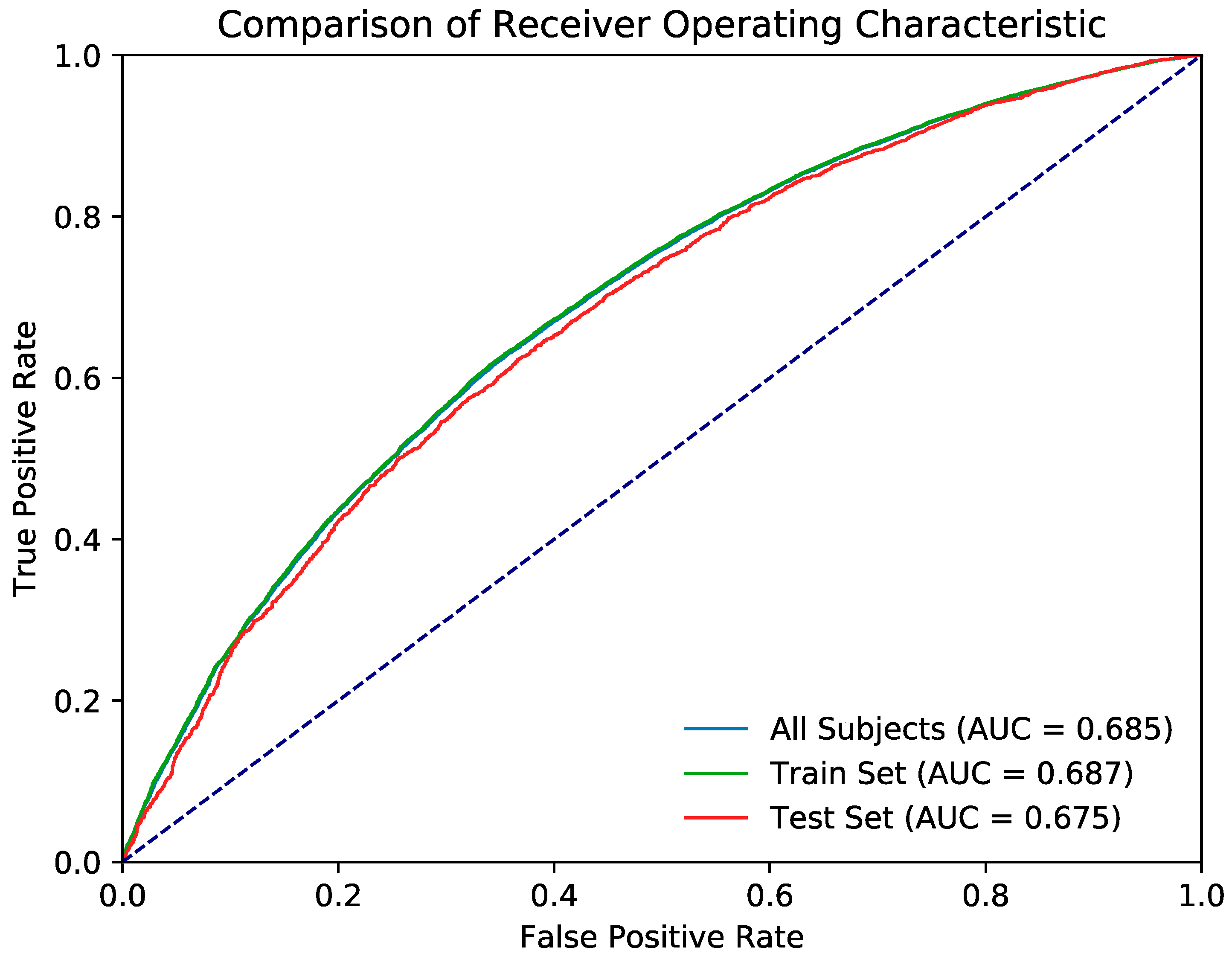
3.2.2. Mortality Classification Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Tonelli, M.; Riella, M. Chronic kidney disease and the aging population. Indian J. Nephrol. 2014, 24, 71–74. [Google Scholar] [CrossRef]
- Kurella, M.; Covinsky, K.E.; Collins, A.J.; Chertow, G.M. Octogenarians and nonagenarians starting dialysis in the United States. Ann. Intern. Med. 2007, 146, 177–183. [Google Scholar] [CrossRef]
- Hemmelgarn, B.R.; James, M.T.; Manns, B.J.; O’Hare, A.M.; Muntner, P.; Ravani, P.; Quinn, R.R.; Turin, T.C.; Tan, Z.; Tonelli, M.; et al. Rates of treated and untreated kidney failure in older vs. younger adults. JAMA 2012, 307, 2507–2515. [Google Scholar] [CrossRef]
- Jassal, S.V.; Watson, D. Dialysis in Late Life: Benefit or Burden. Clin. J. Am. Soc. Nephrol. 2009, 4, 2008. [Google Scholar] [CrossRef]
- Shlipak, M.G.; Stehman-Breen, C.; Fried, L.F.; Song, X.; Siscovick, D.; Fried, L.P.; Psaty, B.M.; Newman, A.B. The presence of frailty in elderly persons with chronic renal insufficiency. Am. J. Kidney Dis. 2004, 43, 861–867. [Google Scholar] [CrossRef]
- Johansen, K.L.; Chertow, G.M.; Jin, C.; Kutner, N.G. Significance of Frailty among Dialysis Patients. J. Am. Soc. Nephrol. 2007, 18, 2960. [Google Scholar] [CrossRef]
- Cook, W.L.; Jassal, S.V. Functional dependencies among the elderly on hemodialysis. Kidney Int. 2008, 73, 1289–1295. [Google Scholar] [CrossRef] [Green Version]
- Murray, A.M. Cognitive impairment in the aging dialysis and chronic kidney disease populations: An occult burden. Adv. Chronic Kidney Dis. 2008, 15, 123–132. [Google Scholar] [CrossRef]
- Cook, W.L.; Jassal, S.V. Prevalence of falls among seniors maintained on hemodialysis. Int. Urol. Nephrol. 2005, 37, 649–652. [Google Scholar] [CrossRef]
- US Renal Data System. USRDS 2009 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States; Bethesda: Rockville, MD, USA, 2009. [Google Scholar]
- Davis, J.L.; Davison, S.N. Hard choices, better outcomes: a review of shared decision-making and patient decision aids around dialysis initiation and conservative kidney management. Curr. Opin. Nephrol. Hypertens. 2017, 26, 205–213. [Google Scholar] [CrossRef]
- Eneanya, N.D.; Goff, S.L.; Martinez, T.; Gutierrez, N.; Klingensmith, J.; Griffith, J.L.; Garvey, C.; Kitsen, J.; Germain, M.J.; Marr, L.; et al. Shared decision-making in end-stage renal disease: a protocol for a multi-center study of a communication intervention to improve end-of-life care for dialysis patients. BMC Palliat. Care 2015, 14, 30. [Google Scholar] [CrossRef]
- Moss, A.H. Revised dialysis clinical practice guideline promotes more informed decision-making. Clin. J. Am. Soc. Nephrol. 2010, 5, 2380–2383. [Google Scholar] [CrossRef]
- Galla, J.H. Clinical practice guideline on shared decision-making in the appropriate initiation of and withdrawal from dialysis. J. Am. Soc. Nephrol. 2000, 11, 1340–1342. [Google Scholar]
- Barry, M.J.; Edgman-Levitan, S. Shared decision making—the pinnacle of patient-centered care. N. Engl. J. Med. 2012, 366, 780–781. [Google Scholar] [CrossRef]
- Li, M.; Tomlinson, G.; Naglie, G.; Cook, W.L.; Jassal, S.V. Geriatric comorbidities, such as falls, confer an independent mortality risk to elderly dialysis patients. Nephrol. Dial. Transplant. 2007, 23, 1396–1400. [Google Scholar] [CrossRef] [Green Version]
- Foote, C.; Ninomiya, T.; Gallagher, M.; Perkovic, V.; Cass, A.; McDonald, S.P.; Jardine, M. Survival of elderly dialysis patients is predicted by both patient and practice characteristics. Nephrol. Dial. Transplant. 2012, 27, 3581–3587. [Google Scholar] [CrossRef] [Green Version]
- Thamer, M.; Kaufman, J.S.; Zhang, Y.; Zhang, Q.; Cotter, D.J.; Bang, H. Predicting early death among elderly dialysis patients: development and validation of a risk score to assist shared decision making for dialysis initiation. Am. J. Kidney Dis. 2015, 66, 1024–1032. [Google Scholar] [CrossRef]
- Jeloka, T.; Sanwaria, P.; Periera, A.; Pawar, S. Survival of elderly dialysis patients is not dependent on modality or “older” age. Indian J. Nephrol. 2016, 26, 23–26. [Google Scholar] [CrossRef]
- Kurella Tamura, M.; Covinsky, K.E.; Chertow, G.M.; Yaffe, K.; Landefeld, C.S.; McCulloch, C.E. Functional status of elderly adults before and after initiation of dialysis. N. Engl. J. Med. 2009, 361, 1539–1547. [Google Scholar] [CrossRef]
- Derrett, S.; Samaranayaka, A.; Schollum, J.B.W.; McNoe, B.; Marshall, M.R.; Williams, S.; Wyeth, E.H.; Walker, R.J. Predictors of Health Deterioration Among Older Adults After 12 Months of Dialysis Therapy: A Longitudinal Cohort Study from New Zealand. Am. J. Kidney Dis. 2017, 70, 798–806. [Google Scholar] [CrossRef]
- Wingard, R.L.; Chan, K.E.; Lazarus, J.M.; Hakim, R.M. The “Right” of Passage: Surviving the First Year of Dialysis. Clin. J. Am. Soc. Nephrol. 2009, 4, S114–S120. [Google Scholar] [CrossRef]
- Ministry of Health and Welfare. Available online: https://www.mohw.gov.tw/cp-115-33347-2.html (accessed on 20 June 2018).
- Klambauer, G.; Unterthiner, T.; May, A.; Hochreiter, S. Self-normalizing neural networks. In Advances in Neural Information Processing Systems; The MIT Press: Cambridge, MA, USA, 2017. [Google Scholar]
- Kingma, D.; Ba, J.A. A method for stochastic optimization. In Proceedings of the 3rd International Conference on Learning Representations (ICLR), San Diego, CA, USA, 7–9 May 2015. [Google Scholar]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine learning in Python. J. Mach. Learn. Res. 2011, 2825–2830. [Google Scholar]
- Abadi, M.; Barham, P.; Chen, J.; Chen, Z.; Davis, A.; Dean, J.; Devin, M.; Ghemawat, S.; Irving, G.; Isard, M.; et al. Tensorflow: A System for Large-Scale Machine Learning; OSDI: Carlsbad, CA, USA, 2016. [Google Scholar]
- Shih, C.J.; Chen, Y.T.; Ou, S.M.; Yang, W.C.; Kuo, S.C.; Tarng, D.C. Taiwan Geriatric Kidney Disease Research (TGKD) Group. The impact of dialysis therapy on older patients with advanced chronic kidney disease: A nationwide population-based study. BMC Med. 2014, 12, 169. [Google Scholar] [CrossRef]
- Couchoud, C.; Labeeuw, M.; Moranne, O.; Allot, V.; Esnault, V.; Frimat, L.; Stengel, B. French Renal Epidemiology and Information Network (REIN) registry. A clinical score to predict 6-month prognosis in elderly patients starting dialysis for end-stage renal disease. Nephrol. Dial. Transplant. 2009, 24, 1553–1561. [Google Scholar] [CrossRef]
- Cohen, L.M.; Ruthazer, R.; Moss, A.H.; Germain, M.J. Predicting six-month mortality for patients who are on maintenance hemodialysis. Clin. J. Am. Soc. Nephrol. 2010, 5, 72–79. [Google Scholar] [CrossRef]
- Leavey, S.F.; McCullough, K.; Hecking, E.; Goodkin, D.; Port, F.K.; Young, E.W. Body mass index and mortality in ‘healthier’as compared with ‘sicker’haemodialysis patients: results from the Dialysis Outcomes and Practice Patterns Study (DOPPS). Nephrol. Dial. Transplant. 2001, 16, 2386–2394. [Google Scholar] [CrossRef]
- Carleo, G.; Troyer, M. Solving the quantum many-body problem with artificial neural networks. Science 2017, 355, 602–606. [Google Scholar] [CrossRef] [Green Version]
- Søreide, K.; Thorsen, K.; Søreide, J.A. Predicting outcomes in patients with perforated gastroduodenal ulcers: Artificial neural network modelling indicates a highly complex disease. Eur. J. Trauma Emerg. Surg. 2015, 41, 91–98. [Google Scholar]
- Badnjević, A.; Gurbeta, L.; Cifrek, M.; Marjanovic, D. Classification of asthma using artificial neural network. In Proceedings of the 39th International Convention on Information and Communication Technology, Electronics and Microelectronics (MIPRO), Opatija, Croatia, 30 May–3 June 2016; pp. 387–390. [Google Scholar]
- Greenspan, H.; Van Ginneken, B.; Summers, R.M. Guest editorial deep learning in medical imaging: Overview and future promise of an exciting new technique. IEEE Trans. Med. Imaging 2016, 35, 1153–1159. [Google Scholar] [CrossRef]
- Wise, E.S.; Hocking, K.M.; Brophy, C.M. Prediction of in-hospital mortality after ruptured abdominal aortic aneurysm repair using an artificial neural network. J. Vasc. Surg. 2015, 62, 8–15. [Google Scholar] [CrossRef] [Green Version]
- Liaw, A.; Wiener, M. Classification and regression by random. For. R. News 2002, 2, 18–22. [Google Scholar]
- Dreiseitl, S.; Ohno-Machado, L. Logistic regression and artificial neural network classification models: A methodology review. J. Biomed. Inform. 2002, 35, 352–359. [Google Scholar] [CrossRef]
- Juma, S.; Taabazuing, M.-M.; Montero-Odasso, M. Clinical Frailty Scale in an Acute Medicine Unit: A Simple Tool That Predicts Length of Stay. Can. Geriatr. J. 2016, 19, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Chernbumroong, S.; Cang, S.; Atkins, A.; Yu, H. Elderly activities recognition and classification for applications in assisted living. Expert Syst. Appl. 2013, 40, 1662–1674. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | One-Year Medical Expenditures, n = 48,153 |
|---|---|
| n (%) | |
| Age, year | |
| 65–79 | 26,732 (55.5) |
| 80+ | 21,421 (44.5) |
| Median (IQR, interquartile range) | 74.0 (69.5, 79.0) |
| Sex | |
| Female | 25,994 (54.0) |
| Male | 22,159 (46.0) |
| Urbanization level & | |
| 1 (Highest urbanization) | 11,708 (24.3) |
| 2 | 12,842 (26.7) |
| 3 | 8162 (15441) |
| 4(Lowest urbanization) | 15,441 (32.1) |
| Occupation | |
| Housekeeping | 21,924 (45.5) |
| White collar | 931 (1.93) |
| Blue collar | 15,013 (31.2) |
| Others ‡ | 10,285 (21.4) |
| One-year expenditures | |
| Median (25th and 75th percentile) | US$20,846 (US$12,468–US$22,802) |
| Total duration of hospitalization in days stay within one year after ESRD diagnosis Median (IQR, interquartile range) | 7 (0–26) |
| Frequency of medical visits within one year after ESRD diagnosis Median (IQR, interquartile range) | 35 (21–51) |
| Comorbidity | |
| Diabetes | 25,759 (53.5) |
| Hypertension | 45,371 (94.2) |
| Hyperlipidemia | 23,329 (48.5) |
| Liver disease and cirrhosis | 9982 (20.7) |
| Coronary artery disease | 28,396 (59.0) |
| Obesity | 433 (0.90) |
| Cancer | 4497 (9.34) |
| Alcohol–related disease | 1232 (2.56) |
| Cirrhosis | 11,927 (24.8) |
| Stroke | 12,469 (25.9) |
| GI bleeding | 26,775 (55.6) |
| COPD | 13,818 (28.7) |
| Previous hip fracture | 8245 (17.1) |
| Osteoporosis | 9717 (20.2) |
| Dementia | 3198 (6.64) |
| Previous herpes | 2558 (5.31) |
| Previous respiratory failure | 2560 (5.32) |
| Number of comorbidities | |
| ≤5 | 22,884 (47.5) |
| >5 | 25,269 (52.5) |
| Variable | One-Year Mortality after ESRD Entrance | Odds Ratio (95% CI) | p-Value | |
|---|---|---|---|---|
| No, n = 37742 | Yes, n = 10411 | |||
| n (%) | n (%) | |||
| Age, year | <0.001 | |||
| 65–79 | 22447(59.5) | 4285(41.2) | 1.00 | |
| 80+ | 15295(40.5) | 6126(58.8) | 2.10(2.01, 2.19) | |
| Mean ± SD † | 74.1(6.08) | 77.0(6.79) | <0.001 | |
| Sex | <0.001 | |||
| Female | 20702(54.9) | 5292(50.8) | 1.00 | |
| Male | 17040(45.2) | 5119(49.2) | 1.18(1.13, 1.23) | |
| Urbanization level & | 0.66 | |||
| 1 (Highest urbanization) | 9155(24.3) | 2553(24.5) | 1.03(0.97, 1.09) | |
| 2 | 10051(26.6) | 2791(26.8) | 1.03(0.97, 1.09) | |
| 3 | 6381(16.9) | 1781(17.1) | 1.03(0.97, 1.10) | |
| 4 (Lowest urbanization) | 12155(32.2) | 3286(31.6) | 1.00 | |
| Occupation | <0.001 | |||
| Housekeeping | 17279(45.8) | 4645(44.6) | 1.02(0.97, 1.07) | |
| White collar | 744(1.97) | 187(1.80) | 0.95(0.81, 1.13) | |
| Blue collar | 11881(31.5) | 3132(30.1) | 1.00 | |
| Others ‡ | 7838(20.8) | 2447(23.5) | 1.18(1.12, 1.26) | |
| Comorbidity | ||||
| Diabetes | 19965(52.9) | 5794(55.7) | 1.12(1.07, 1.17) | <0.001 |
| Hypertension | 35660(94.5) | 9711(93.3) | 0.81(0.74, 0.89) | <0.001 |
| Hyperlipidemia | 18768(49.7) | 4561(43.8) | 0.79(0.76, 0.82) | <0.001 |
| Liver disease and cirrhosis | 7853(20.8) | 2129(20.5) | 0.98(0.93, 1.03) | 0.43 |
| Coronary artery disease | 22294(59.1) | 6102(58.6) | 0.98(0.94, 1.03) | 0.40 |
| Obesity * | 371(0.98) | 62(0.60) | 0.60(0.46, 0.79) | <0.001 |
| Cancer | 3146(8.14) | 1720(12.9) | 1.71(1.60, 1.83) | <0.001 |
| Alcohol–related disease | 902(2.39) | 330(3.17) | 1.34(1.18, 1.52) | <0.001 |
| Cirrhosis | 9391(24.9) | 2536(24.4) | 0.97(0.92, 1.02) | 0.01 |
| Stroke | 8822(23.4) | 3647(35.0) | 1.77(1.69, 1.85) | <0.001 |
| GI bleeding | 20988(55.6) | 5787(55.6) | 1.00(0.96, 1.04) | 0.97 |
| COPD | 10410(27.6) | 3408(32.7) | 1.28(1.22, 1.34) | <0.001 |
| Previous Hip fracture | 6136(16.3) | 2109(20.3) | 1.31(1.24, 1.38) | <0.001 |
| Osteoporosis | 7477(19.8) | 2240(21.5) | 1.11(1.05, 1.17) | 0.001 |
| Dementia | 2060(5.46) | 1138(11.0) | 2.13(1.97, 2.29) | <0.001 |
| Previous herpes | 1996(5.29) | 562(5.40) | 1.02(0.93, 1.13) | 0.66 |
| Previous respiratory failure | 1344(3.56) | 1216(11.7) | 3.58(3.30, 3.88) | <0.001 |
| Number of comorbidities | <0.001 | |||
| ≤5 | 18530(49.1) | 4354(41.8) | 1.00 | |
| >5 | 19212(50.9) | 6057(58.2) | 1.34(1.28, 1.40) | |
| MSE | MAE | |
|---|---|---|
| All | 0.666 | 0.491 |
| Train | 0.652 | 0.487 |
| Test | 0.754 | 0.513 |
| MSE | MAE | |
|---|---|---|
| All | 4.42948 | 1.85189 |
| Train | 4.43229 | 1.85185 |
| Test | 4.33447 | 1.85346 |
| F1 | Precision | Recall | AUROC | AUROC SE | AUROC 95% CI | |
|---|---|---|---|---|---|---|
| All Subjects | 0.780 | 0.843 | 0.817 | 0.861 | 0.002 | 0.857–0.864 |
| Train Set | 0.800 | 0.863 | 0.832 | 0.656 | 0.007 | 0.643–0.669 |
| Test Set | 0.672 | 0.702 | 0.743 | 0.656 | 0.007 | 0.643–0.669 |
| F1 | Precision | Recall | AUROC | AUROC SE | AUROC 95% CI | |
|---|---|---|---|---|---|---|
| All Subjects | 0.661 | 0.717 | 0.640 | 0.685 | 0.003 | 0.680–0.691 |
| Train Set | 0.662 | 0.717 | 0.641 | 0.687 | 0.003 | 0.682–0.693 |
| Test Set | 0.658 | 0.715 | 0.634 | 0.675 | 0.007 | 0.662–0.688 |
| Cohort | Subjects | Subject Alive, n (%) | Subject Death, n (%) |
|---|---|---|---|
| Age < 70 | 13360 | 11513(86.2) | 1847(13.8) |
| 70 ≤ Age < 75 | 13372 | 10934(81.8) | 2438(18.2) |
| 75 ≤ Age < 80 | 11188 | 8579(76.7) | 2609(23.3) |
| 80 ≤ Age < 85 | 6852 | 4706(68.7) | 2146(31.3) |
| 85 ≤ Age < 90 | 2706 | 1681(62.1) | 1025(37.9) |
| Age > 90 | 675 | 329(48.7) | 346(51.3) |
| Cohort\Metric | F1 | Precision | Recall |
|---|---|---|---|
| Age < 70 | 0.738 | 0.805 | 0.699 |
| 70 ≤ Age < 75 | 0.680 | 0.752 | 0.642 |
| 75 ≤ Age < 80 | 0.633 | 0.705 | 0.604 |
| 80 ≤ Age < 85 | 0.583 | 0.641 | 0.567 |
| 85 ≤ Age < 90 | 0.548 | 0.599 | 0.545 |
| Age > 90 | 0.546 | 0.568 | 0.563 |
| Cohort\Metric | F1 | Precision | Recall |
|---|---|---|---|
| Age < 70 | 0.818 | 0.849 | 0.868 |
| 70 ≤ Age < 75 | 0.779 | 0.839 | 0.835 |
| 75 ≤ Age < 80 | 0.714 | 0.808 | 0.787 |
| 80 ≤ Age < 85 | 0.613 | 0.722 | 0.705 |
| 85 ≤ Age < 90 | 0.545 | 0.666 | 0.643 |
| Age > 90 | 0.430 | 0.645 | 0.530 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, S.-Y.; Hsieh, M.-H.; Lin, C.-L.; Hsieh, M.-J.; Hsu, W.-H.; Lin, C.-C.; Hsu, C.Y.; Kao, C.-H. Artificial Intelligence Prediction Model for the Cost and Mortality of Renal Replacement Therapy in Aged and Super-Aged Populations in Taiwan. J. Clin. Med. 2019, 8, 995. https://doi.org/10.3390/jcm8070995
Lin S-Y, Hsieh M-H, Lin C-L, Hsieh M-J, Hsu W-H, Lin C-C, Hsu CY, Kao C-H. Artificial Intelligence Prediction Model for the Cost and Mortality of Renal Replacement Therapy in Aged and Super-Aged Populations in Taiwan. Journal of Clinical Medicine. 2019; 8(7):995. https://doi.org/10.3390/jcm8070995
Chicago/Turabian StyleLin, Shih-Yi, Meng-Hsuen Hsieh, Cheng-Li Lin, Meng-Ju Hsieh, Wu-Huei Hsu, Cheng-Chieh Lin, Chung Y. Hsu, and Chia-Hung Kao. 2019. "Artificial Intelligence Prediction Model for the Cost and Mortality of Renal Replacement Therapy in Aged and Super-Aged Populations in Taiwan" Journal of Clinical Medicine 8, no. 7: 995. https://doi.org/10.3390/jcm8070995