Coagulation Parameters: An Efficient Measure for Predicting the Prognosis and Clinical Management of Patients with COVID-19

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participants
2.1.1. Main Variables
2.1.2. Secondary Variables
2.2. Procedures and Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Novel Coronavirus—China World Health Organization. Available online: https://www.who.int/csr/don/12-january-2020-novel-coronavirus-china/en/ (accessed on 25 September 2020).
- Coronavirus Outbreak. Available online: https://www.worldometers.info/coronavirus/ (accessed on 25 September 2020).
- Gupta, A.; Madhavan, M.V.; Sehgal, K.; Nair, N.; Mahajan, S.; Sehrawat, T.S.; Bikdeli, B.; Ahluwalia, N.; Ausiello, J.C.; Wan, E.Y.; et al. Extrapulmonary manifestations of COVID-19. Nat. Med. 2020, 26, 1017–1032. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.; Cao, J.; Wang, Q.; Shi, Q.; Liu, K.; Luo, Z.; Chen, X.; Chen, S.; Yu, K.; Huang, Z.; et al. D-dimer as a biomarker for disease severity and mortality in COVID-19 patients: A case control study. J. Intensive Care 2020, 8, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panigada, M.; Bottino, N.; Tagliabue, P.; Grasselli, G.; Novembrino, C.; Chantarangkul, V.; Pesenti, A.; Peyvandi, F.; Tripodi, A. Hypercoagulability of COVID-19 patients in intensive care unit: A report of thromboelastography findings and other parameters of hemostasis. J. Thromb. Haemost. 2020, 18, 1738–1742. [Google Scholar] [CrossRef]
- Levi, M.; Thachil, J.; Iba, T.; Levy, J.H. Coagulation abnormalities and thrombosis in patients with COVID-19. Lancet Haematol. 2020, 7, e438–e440. [Google Scholar] [CrossRef]
- Adam, E.; Zacharowski, K.; Miesbach, W. A comprehensive assessment of the coagulation profile in critically ill COVID-19 patients. Thromb. Res. 2020, 194, 42–44. [Google Scholar] [CrossRef]
- Violi, F.; Pastori, D.; Cangemi, R.; Pignatelli, P.; Loffredo, L. Hypercoagulation and Antithrombotic Treatment in Coronavirus 2019: A New Challenge. Thromb. Haemost. 2020, 120, 949–956. [Google Scholar] [CrossRef]
- Zhai, Z.; Li, C.; Chen, Y.; Gerotziafas, G.; Zhang, Z.; Wan, J.; Liu, P.; Elalamy, I.; Wang, C. Prevention and Treatment of Venous Thromboembolism Associated with Coronavirus Disease 2019 Infection: A Consensus Statement before Guidelines. Thromb. Haemost. 2020, 120, 937–948. [Google Scholar] [CrossRef]
- Poissy, J.; Goutay, J.; Caplan, M.; Parmentier, E.; Duburcq, T.; Lassalle, F.; Jeanpierre, E.; Rauch, A.; Labreuche, J.; Susen, S.; et al. Pulmonary Embolism in Patients with COVID-19. Circulation 2020, 142, 184–186. [Google Scholar] [CrossRef]
- Abou-Ismail, M.Y.; Diamond, A.; Kapoor, S.; Arafah, Y.; Nayak, L. The hypercoagulable state in COVID-19: Incidence, pathophysiology, and management. Thromb. Res. 2020, 194, 101–115. [Google Scholar] [CrossRef]
- Gustafson, D.; Raju, S.; Wu, R.; Ching, C.; Veitch, S.; Rathnakumar, K.; Boudreau, E.; Howe, K.L.; Fish, J.E. Overcoming Barriers: The Endothelium as a Linchpin of Coronavirus Disease 2019 Pathogenesis? Arterioscler. Thromb. Vasc. Biol. 2020, 40, 1818–1829. [Google Scholar] [CrossRef] [PubMed]
- Tang, N.; Bai, H.; Chen, X.; Gong, J.; Li, D.; Sun, Z. Anticoagulant treatment is associated with decreased mortality in severe coronavirus disease 2019 patients with coagulopathy. J. Thromb. Haemost. 2020, 18, 1094–1099. [Google Scholar] [CrossRef] [PubMed]
- Helms, J.; Tacquard, C.; Severac, F.; Leonard-Lorant, I.; Ohana, M.; Delabranche, X.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Gandet, F.F.; et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: A multicenter prospective cohort study. Intensive Care Med. 2020, 46, 1089–1098. [Google Scholar] [CrossRef] [PubMed]
- Klok, F.; Kruip, M.; Van Der Meer, N.; Arbous, M.; Gommers, D.; Kant, K.; Kaptein, F.; Van Paassen, J.; Stals, M.; Huisman, M.; et al. Confirmation of the high cumulative incidence of thrombotic complications in critically ill ICU patients with COVID-19: An updated analysis. Thromb. Res. 2020, 191, 148–150. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72,314 cases from the Chinese Center for Disease Control and Prevention. JAMA J. Am. Med. Assoc. 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Wong, S.-Y.; Kwong, R.-S.; Wu, T.; Chan, J.; Chu, M.; Lee, S.; Wong, H.; Lung, D. Risk of nosocomial transmission of coronavirus disease 2019: An experience in a general ward setting in Hong Kong. J. Hosp. Infect. 2020, 105, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Rivett, L.; Sridhar, S.; Sparkes, D.; Routledge, M.; Jones, N.K.; Forrest, S.; Young, J.; Pereira-Dias, J.; Hamilton, W.L.; Ferris, M.; et al. Screening of healthcare workers for SARS-CoV-2 highlights the role of asymptomatic carriage in COVID-19 transmission. eLife 2020, 9. [Google Scholar] [CrossRef] [PubMed]
- Black, J.R.M.; Bailey, C.; Przewrocka, J.; Dijkstra, K.K.; Swanton, C. COVID-19: The case for health-care worker screening to prevent hospital transmission. Lancet 2020, 395, 1418–1420. [Google Scholar] [CrossRef]
- Boreskie, K.F.; Boreskie, P.E.; Melady, D. Age is just a number—And so is frailty: Strategies to inform resource allocation during the COVID-19 pandemic. Can. J. Emerg. Med. 2020, 22, 411–413. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061. [Google Scholar] [CrossRef]
- Shah, S.; Shah, K.; Patel, S.B.; Patel, F.S.; Osman, M.; Velagapudi, P.; Turagam, M.K.; Lakkireddy, D.; Garg, J. Elevated D-Dimer Levels are Associated with Increased Risk of Mortality in COVID-19. Cardiol. Rev. 2020. [Google Scholar] [CrossRef]
- Artifoni, M.; Danic, G.; Gautier, G.; Gicquel, P.; Boutoille, D.; Raffi, F.; Néel, A.; LeComte, R. Systematic assessment of venous thromboembolism in COVID-19 patients receiving thromboprophylaxis: Incidence and role of D-dimer as predictive factors. J. Thromb. Thrombolysis 2020, 50, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Medcalf, R.L.; Keragala, C.B.; Myles, P.S. Fibrinolysis and COVID-19: A plasmin paradox. J. Thromb. Haemost. 2020, 18, 2118–2122. [Google Scholar] [CrossRef]
- Bi, X.; Su, Z.; Yan, H.; Du, J.; Wang, J.; Chen, L.; Peng, M.; Chen, S.; Shen, B.; Li, J. Prediction of severe illness due to COVID-19 based on an analysis of initial Fibrinogen to Albumin Ratio and Platelet count. Platelets 2020, 31, 674–679. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | |
|---|---|
| Sex, n (%) | |
| Male | 1725 (48.94) |
| Female | 1800 (51.06) |
| Median age, years (IQR) | 62 (47–78) |
| Healthcare workers, n (%) | 668 (19.80) |
| Housing, n (%) | |
| Uncrowded house conditions | 3163 (90.60) |
| Nursing homes | 314 (8.99) |
| Shelter residences | 13 (0.37) |
| Prison | 1 (0.03) |
| Direct/close contact with a confirmed COVID-19 patient, n (%) | 554 (17.09) |
| Suspected nosocomial transmission, n (%) | 1064 (30.56) |
| Functional dependence, n (%) | |
| Dependence in daily activities | 252 (7.44) |
| Partial dependence in daily activities | 190 (5.61) |
| Independence in daily activities | 2943 (86.94) |
| Severity scales, score (range) | |
| CURB 65 | 1 (0–2) |
| Fine | 2 (1–4) |
| Q–SOFA | 0 (0–1) |
| SOFA | 0 (0–1) |
| PSI | 1 (0–4) |
| Oxygen therapy, n (%) | 2178 (63.22) |
| Delivery methods of oxygen therapy, n (%) | |
| Venturi mask | 178 (8.18) |
| Simple face mask | 14 (0.64) |
| Nasal cannula/Nasal prongs | 1170 (53.79) |
| Mask with an oxygen reservoir bag | 567 (26.07) |
| Non-invasive mechanical ventilation | 109 (5.01) |
| Invasive mechanical ventilation | 137 (6.30) |
| Prone position, n (%) | 188 (6.43) |
| Positive and expiratory pressure | 10.50 (9.50–14.00) |
| Inspired positive airway pressure | 18.00 (14.00–40.00) |
| Respiratory frequency, bpm | 18.00 (18.00–20.00) |
| ICU admission, n (%) | 173 (5.08) |
| Survivors | Non-Survivors | ||
|---|---|---|---|
| n = 2731 | n = 642 | p | |
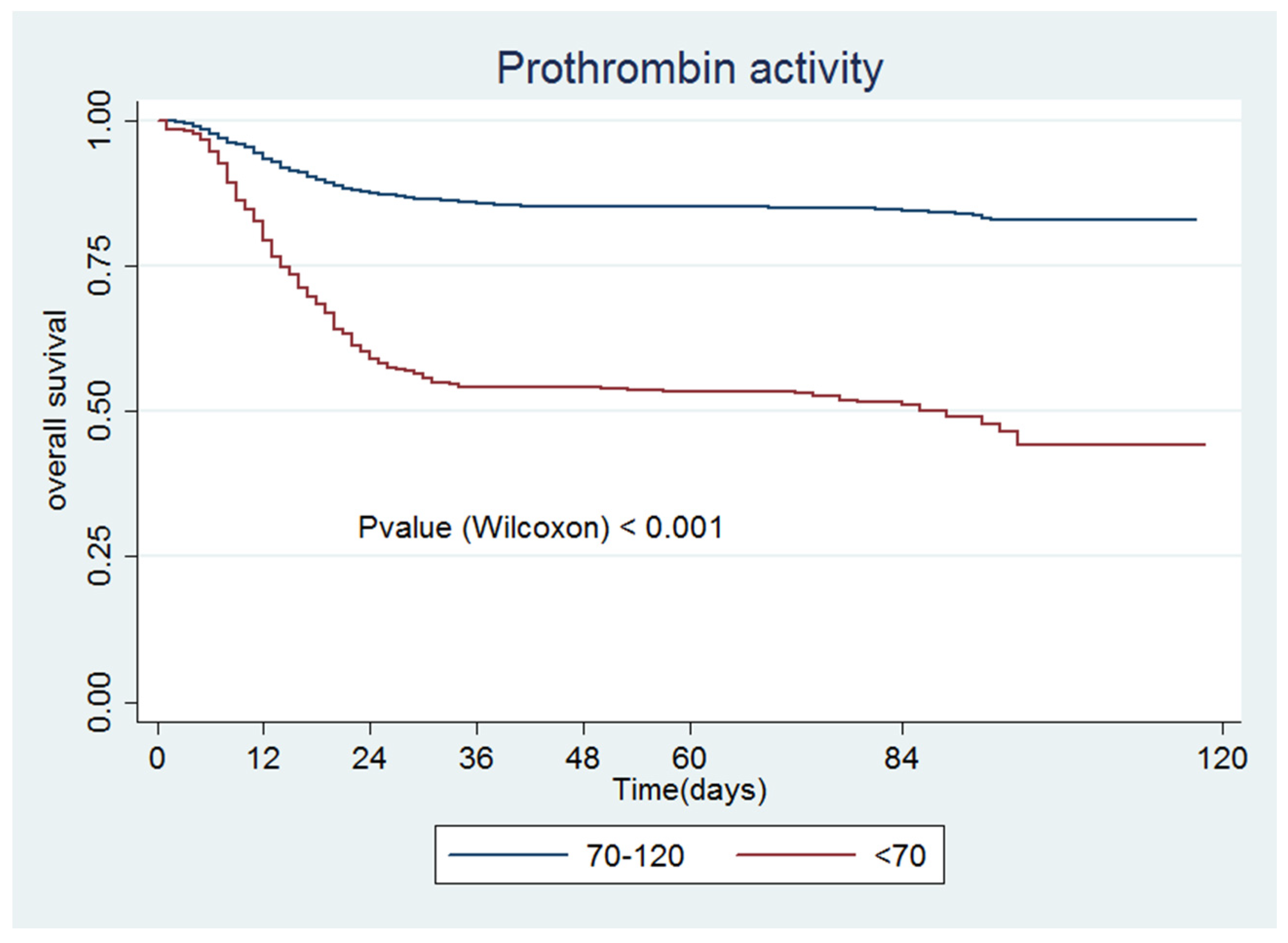
| Prothrombin activity, % (IQR) | 95.25 (87.00–104.00) | 82.5 (67.0–95.0) | <0.001 |
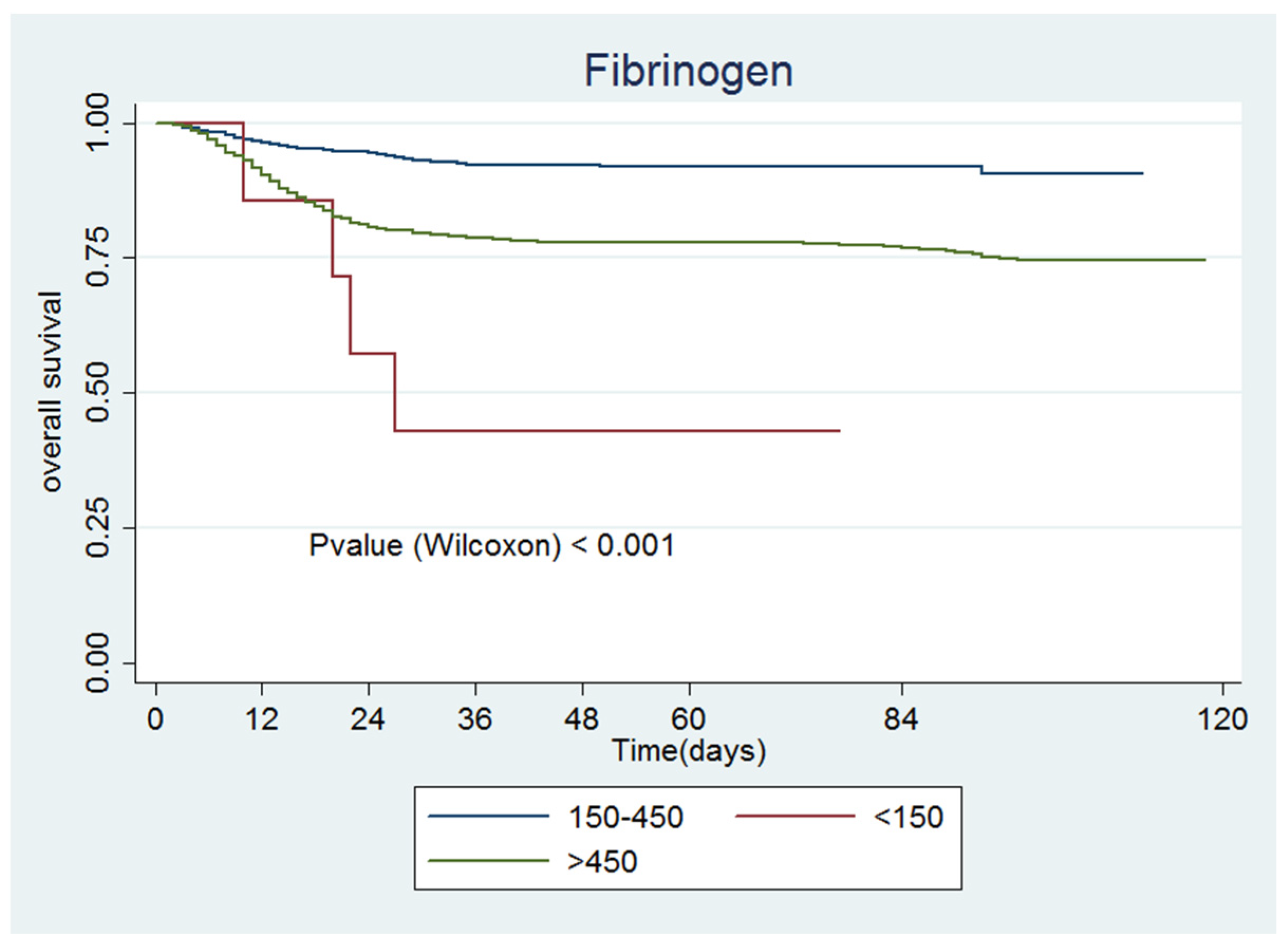
| Fibrinogen, mg/dL (IQR) | 572.75 (417.00–758.00) | 748.5 (557.0–960.8) | <0.001 |
| INR | 1.0 (1.0–1.1) | 1.1 (1.0–1.2) | <0.001 |
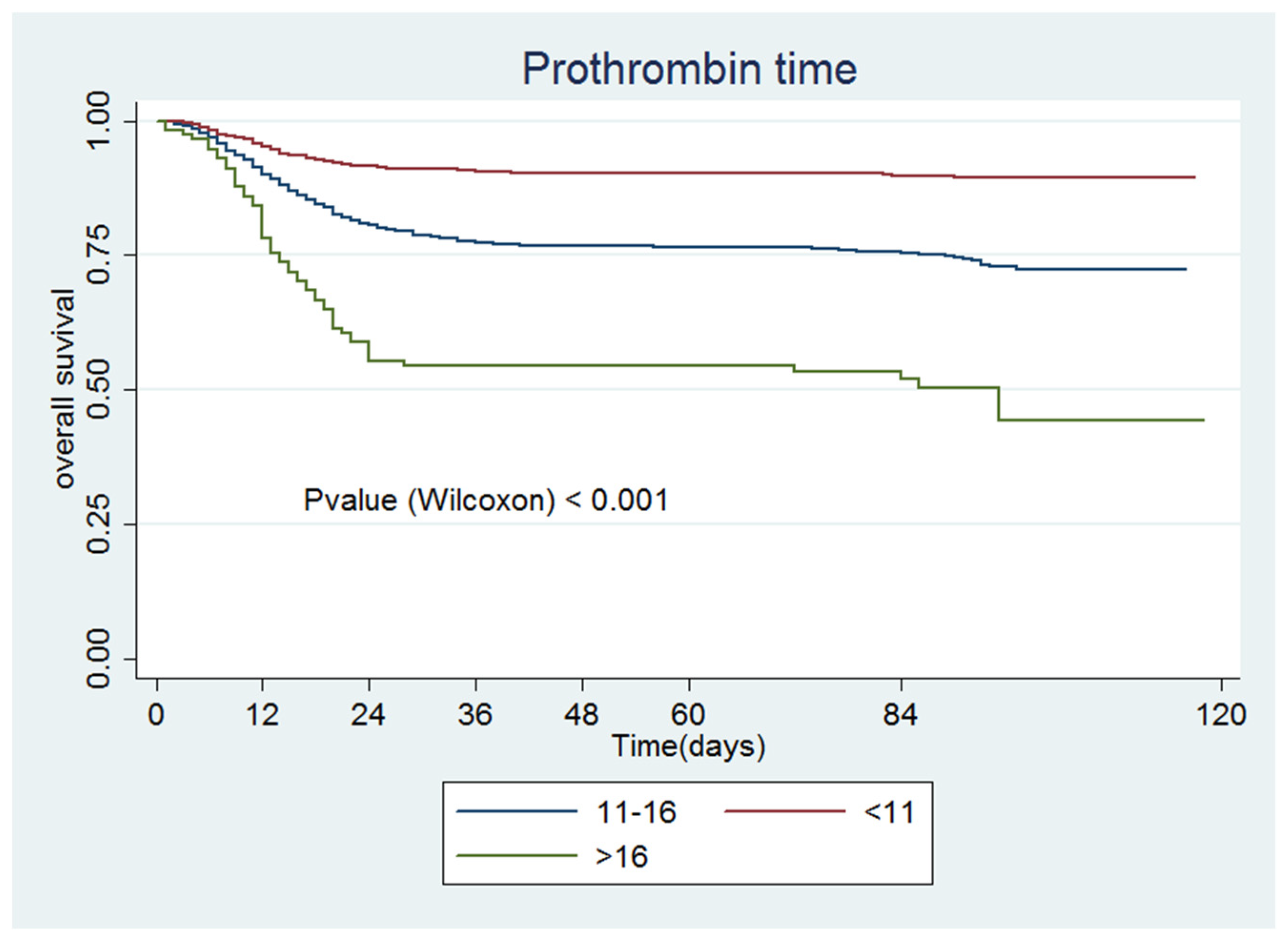
| Prothrombin time, s (IQR) | 11.0 (10.6–11.4) | 11.65 (11.03–12.70) | <0.001 |
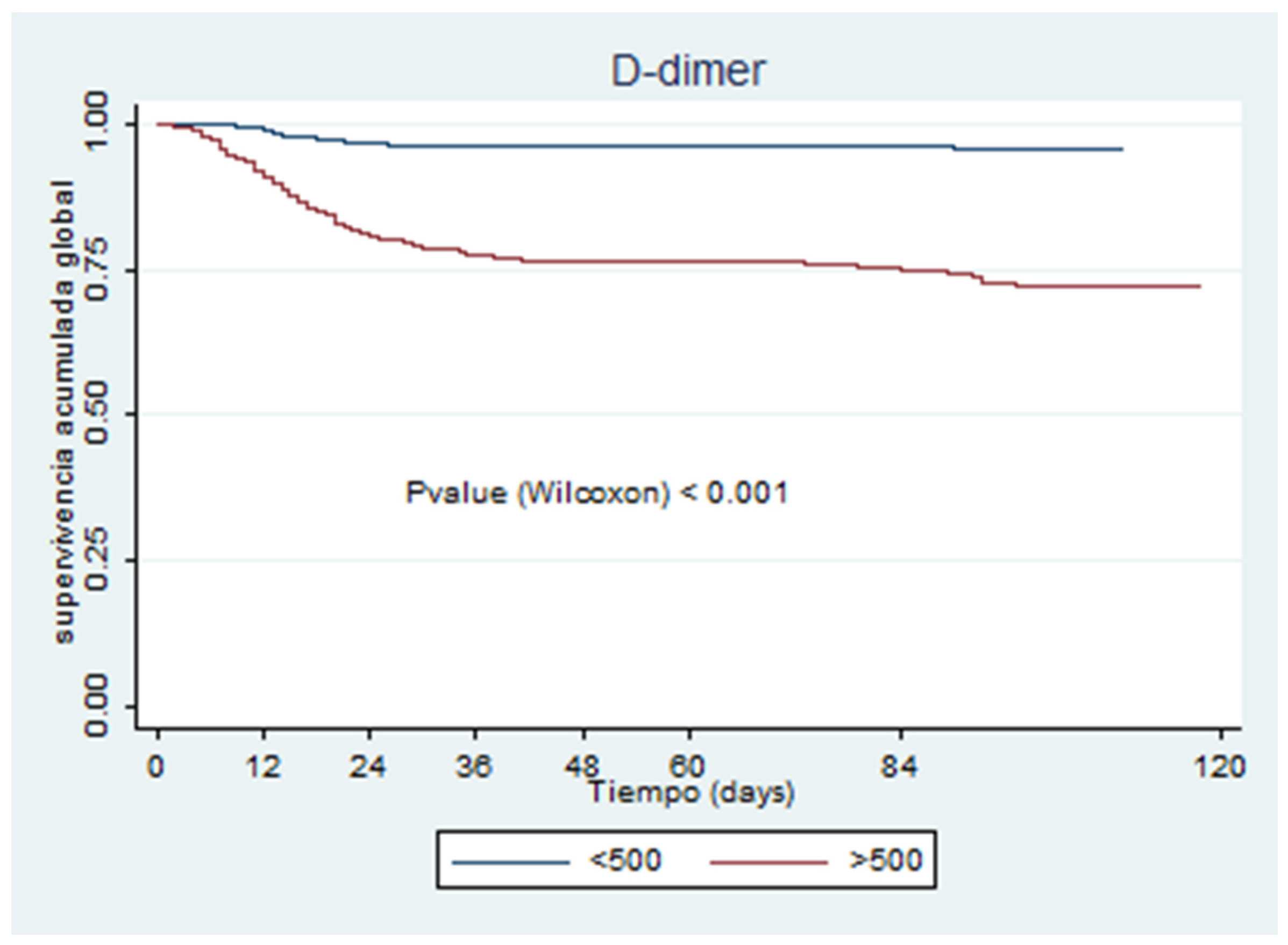
| D-dimer, ng/mL (IQR) | 635.5 (385.5–1194.87) | 2329 (1086.12–5670.4) | <0.001 |
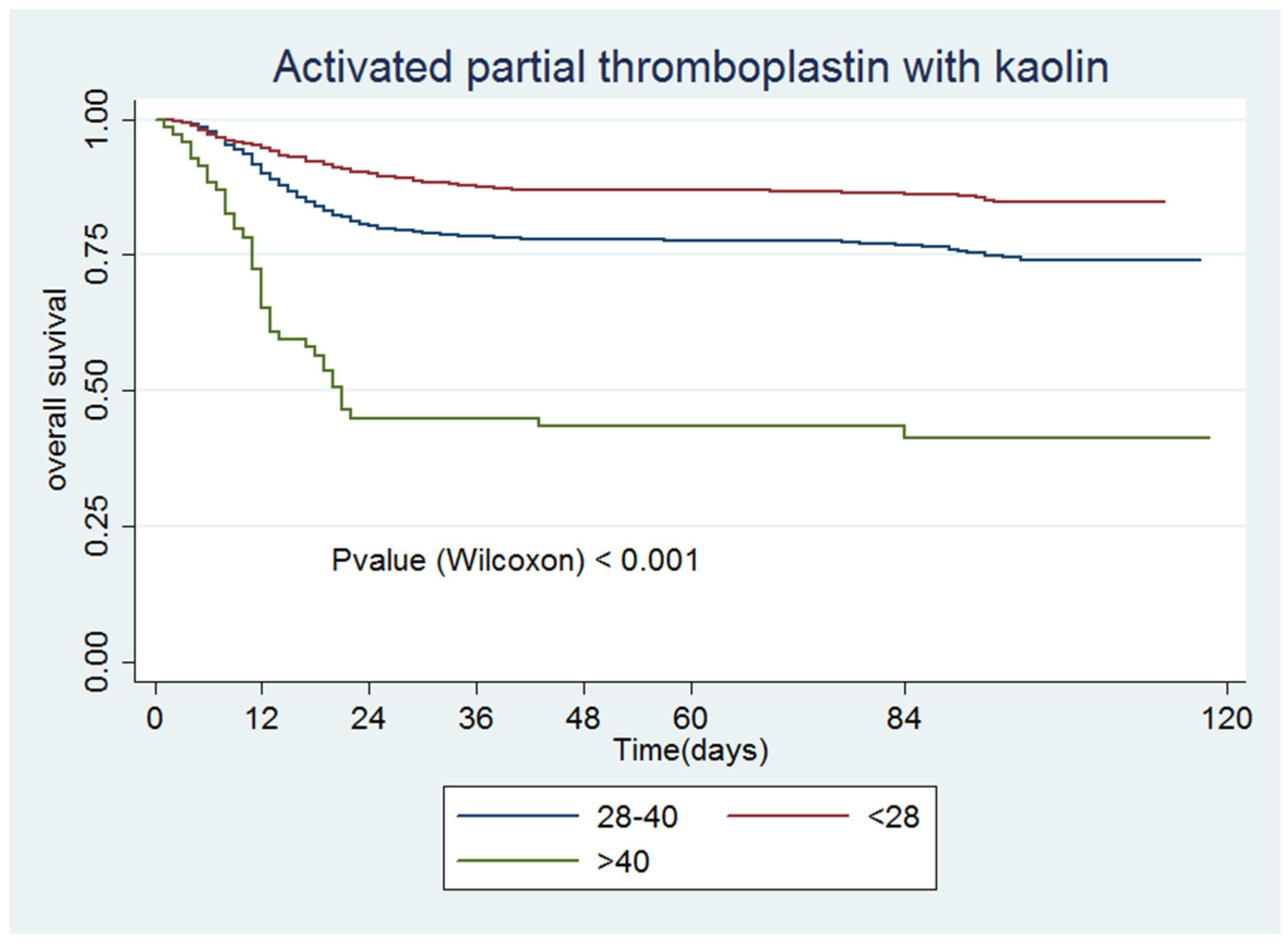
| Partial thromboplastin time with kaolin, s (IQR) | 27.8 (26.25–29.60) | 29.3 (27.0–32.2) | <0.001 |
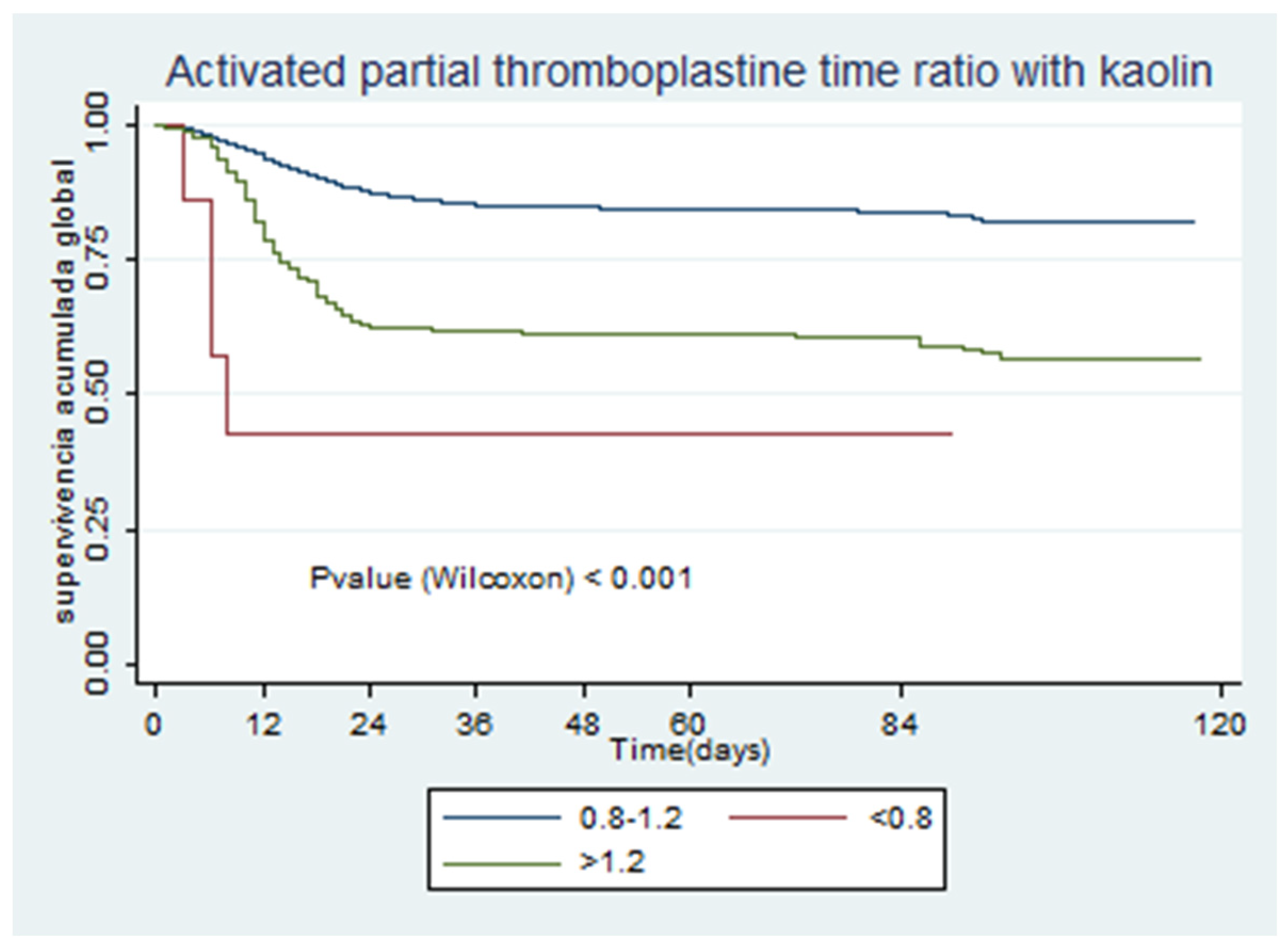
| Activated partial thromboplastin time ratio with kaolin, s (IQR) | 1.04 (0.98–1.11) | 1.1 (1.01–1.21) | <0.001 |
| Variable | No (n = 3420) | Yes (n = 161) | p |
|---|---|---|---|
| Prothrombin activity, % (IQR) | 93.5 (83.0–103.5) | 87.0 (76.0–98.0) % | <0.001 |
| Fibrinogen, mg/dL (IQR) | 599.8 (432.5–788.6) | 681.0 (423.0–882.0) | 0.054 |
| INR, n (IQR) | 1.0 (1.0–1.1) | 1.1 (1.0–1.1) | <0.001 |
| Prothrombin time, s (IQR) | 11.1 (10.7–11.6) | 11.4 (10.9–12.0) | <0.001 |
| D-dimer, ng/mL (IQR) | 720.0 (410.0–1452.3) | 4190.0 (2347.12–9735.0) | <0.001 |
| Functional fibrinogen, mg/dL (IQR) | 101.0 (74.8–414.0) | 78.5 (72.6–88.0) | 0.176 |
| Partial thromboplastin time with kaolin, s (IQR) | 28.0 (26.4–30.0) | 27.95 (26.5–29.8) | 0.564 |
| Activated partial thromboplastin time ratio with kaolin, mg/dL (IQR) | 1.05 (0.99–1.12) | 1.05 (0.99–1.12) | 0.592 |
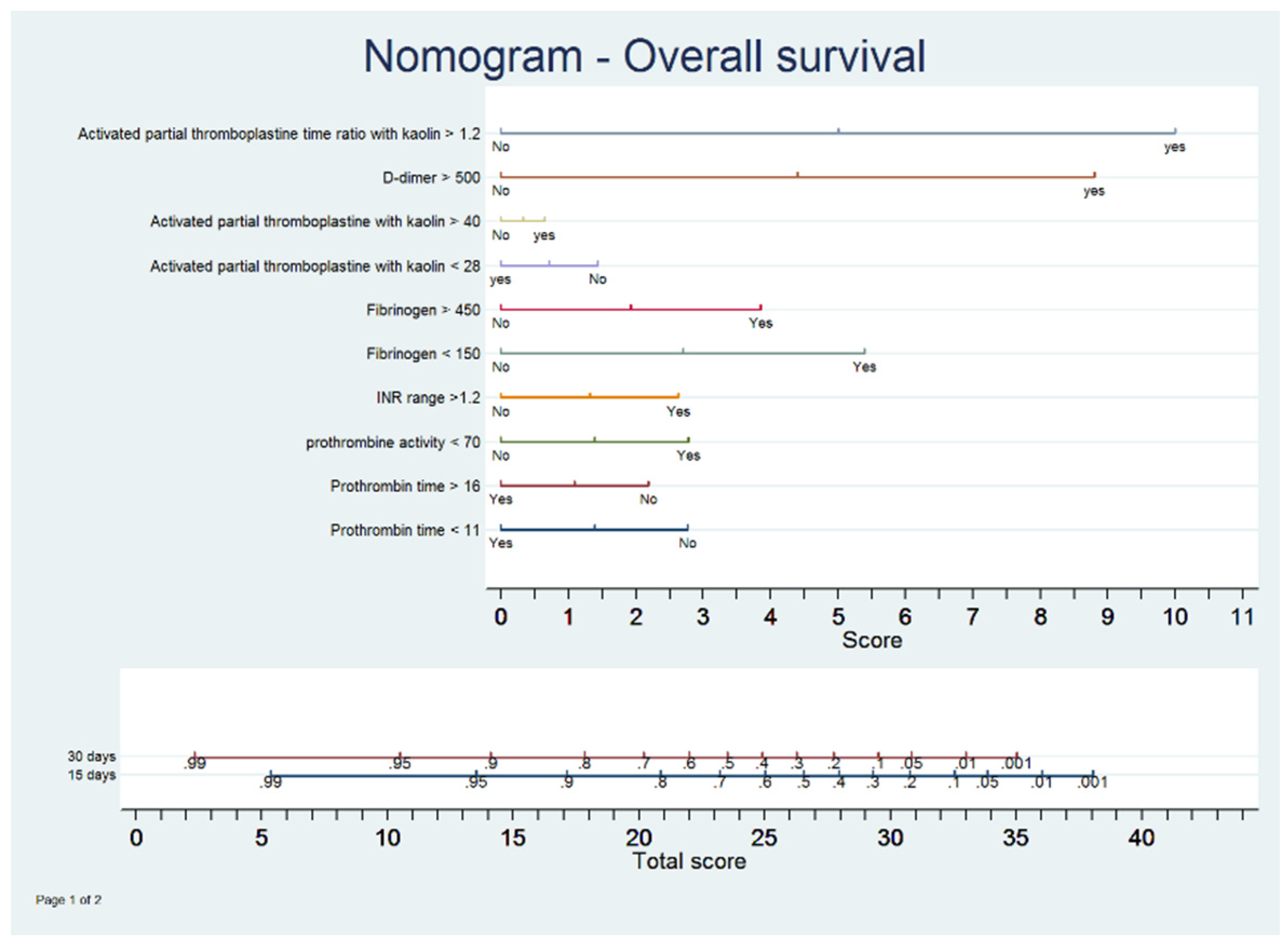
| Univariate Model | Multivariate Model | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | |
| Prothrombin activity | ||||||
| <70 | 3.91 | 3.27–4.68 | <0.001 | 1.74 | 1.21–2.51 | 0.003 |
| 70–120 | Ref | Ref | ||||
| Fibrinogen | ||||||
| <150 | 8.47 | 3.08–23.26 | <0.001 | 2.93 | 1.02–8.39 | 0.044 |
| 150–450 | Ref | Ref | ||||
| >450 | 3.03 | 2.34–3.92 | <0.001 | 2.16 | 1.58–2.95 | <0.001 |
| INR | ||||||
| 0.8–1.2 | Ref | Ref | ||||
| >1.2 | 4.17 | 3.43–5.07 | <0.001 | 1.69 | 1.11–2.57 | 0.014 |
| Prothrombin time, s | ||||||
| <11 | 0.37 | 0.30–0.45 | <0.001 | 0.57 | 0.45–0.73 | <0.001 |
| 11–16 | Ref | Ref | ||||
| >16 | 2.31 | 1.74–3.05 | <0.001 | 0.64 | 0.38–1.07 | <0.001 |
| D-dimer | ||||||
| ≤500 | Ref | Ref | ||||
| >500 | 7.03 | 4.93–10.02 | <0.001 | 5.81 | 4.05–8.33 | <0.001 |
| Activated partial thromboplastin time with kaolin, s | ||||||
| <28 | 0.56 | 0.47–0.66 | <0.001 | 0.75 | 0.60–0.93 | 0.010 |
| 28–40 | Ref | Ref | ||||
| >40 | 3.32 | 2.39–4.61 | <0.001 | 1.13 | 0.64–1.99 | 0.652 |
| Activated partial thromboplastin time ratio with kaolin | ||||||
| <0.8 | 6.54 | 2.44–17.51 | <0.001 | 7.37 | 1.01–53.50 | 0.048 |
| 0.8–1.2 | Ref | Ref | ||||
| >1.2 | 2.91 | 2.41–3.51 | <0.001 | 1.65 | 1.25–2.18 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quintana-Díaz, M.; Andrés-Esteban, E.M.; Ramírez-Cervantes, K.L.; Olivan-Blázquez, B.; Juárez-Vela, R.; Gea-Caballero, V. Coagulation Parameters: An Efficient Measure for Predicting the Prognosis and Clinical Management of Patients with COVID-19. J. Clin. Med. 2020, 9, 3482. https://doi.org/10.3390/jcm9113482
Quintana-Díaz M, Andrés-Esteban EM, Ramírez-Cervantes KL, Olivan-Blázquez B, Juárez-Vela R, Gea-Caballero V. Coagulation Parameters: An Efficient Measure for Predicting the Prognosis and Clinical Management of Patients with COVID-19. Journal of Clinical Medicine. 2020; 9(11):3482. https://doi.org/10.3390/jcm9113482
Chicago/Turabian StyleQuintana-Díaz, Manuel, Eva María Andrés-Esteban, Karen Lizzette Ramírez-Cervantes, Bárbara Olivan-Blázquez, Raúl Juárez-Vela, and Vicente Gea-Caballero. 2020. "Coagulation Parameters: An Efficient Measure for Predicting the Prognosis and Clinical Management of Patients with COVID-19" Journal of Clinical Medicine 9, no. 11: 3482. https://doi.org/10.3390/jcm9113482