The Optimal Range of Serum Uric Acid for Cardiometabolic Diseases: A 5-Year Japanese Cohort Study †

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
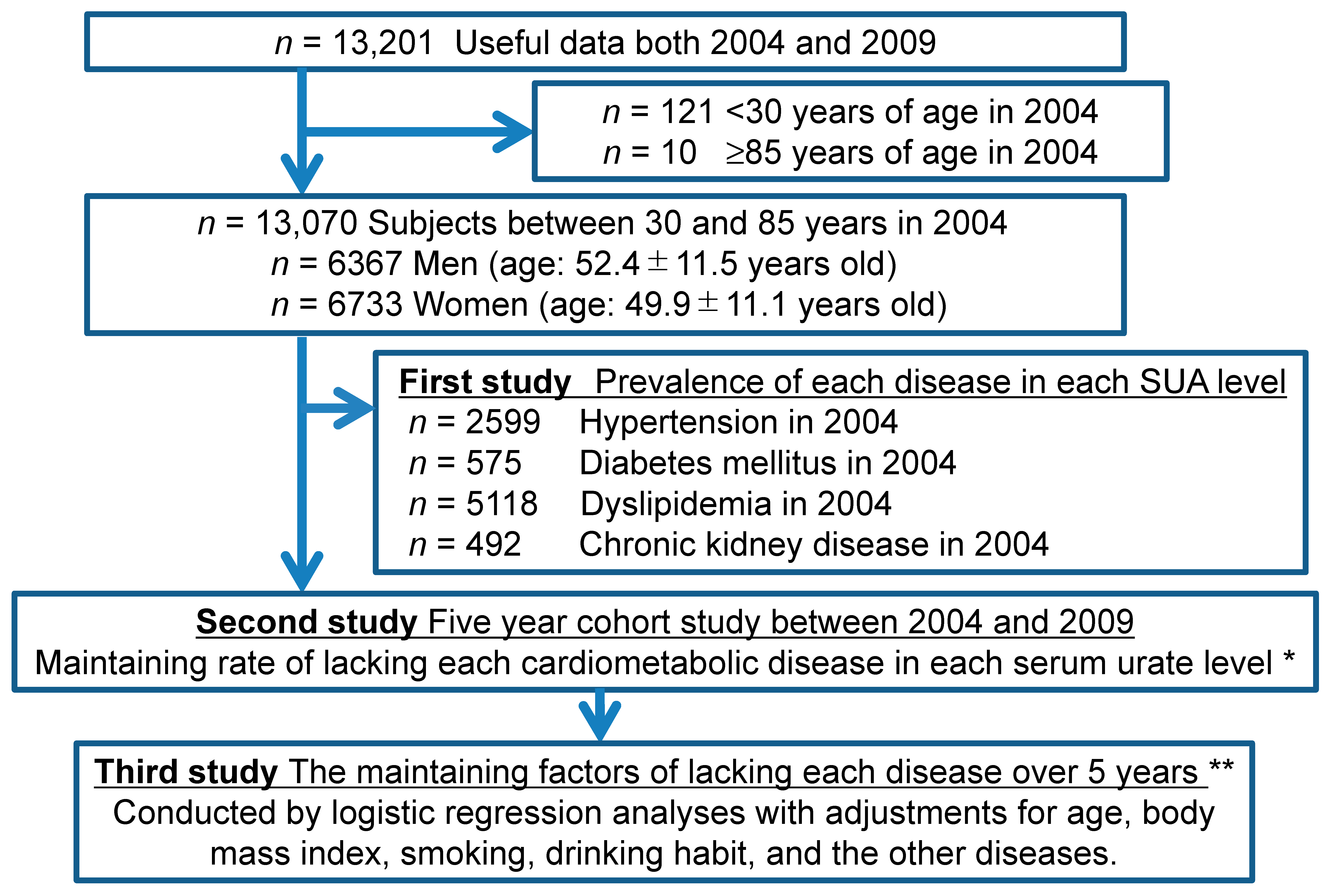
2.1. Study Design and Study Subjects
2.2. Definition of Hypertension, Diabetes, Dyslipidemia, CKD, and Hypouricemia
2.3. Statistical Analysis
2.4. Ethical Considerations
3. Results
3.1. Demographics of this Study’s Subjects
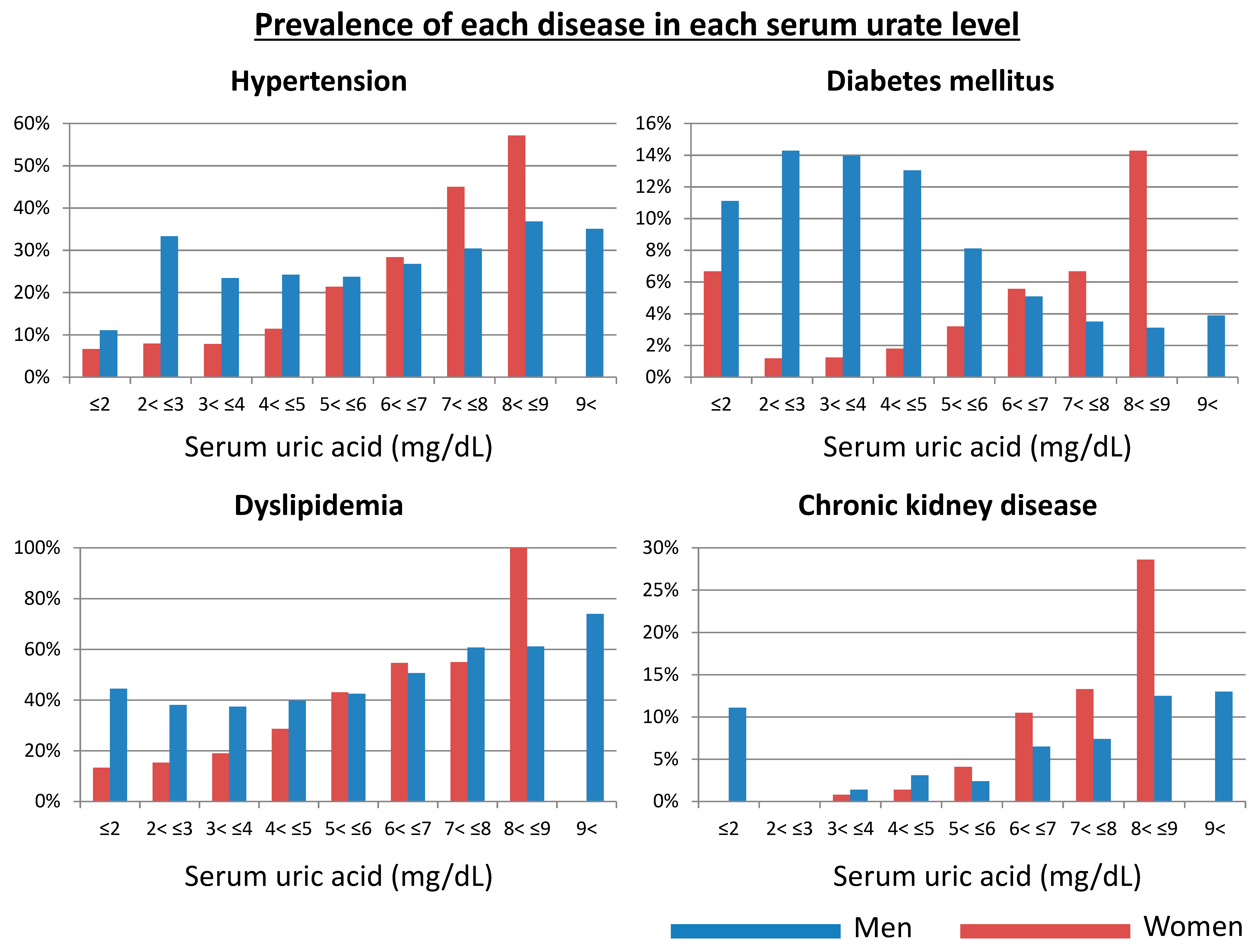
3.2. Prevalence of Cardiometabolic Disease in Each Serum Urate Level (A Cross-Sectional Study)
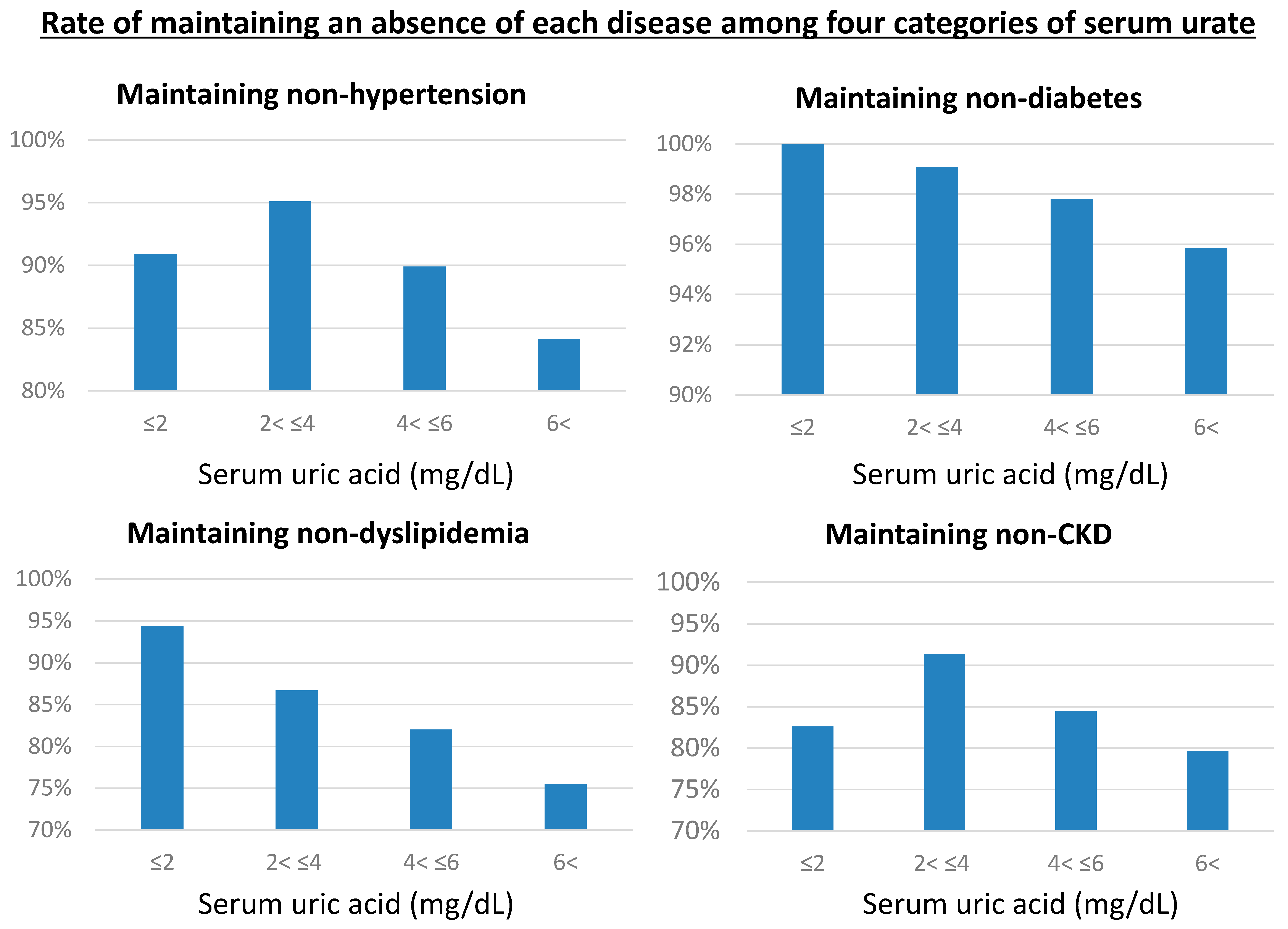
3.3. Rate of Being Free of Various Cardiometabolic Conditions According to Serum Urate Levels over Five Years (A Longitudinal Study)
3.4. Optimal Serum Urate Range Associated with the Lowest Risk of Cardiometabolic Diseases
3.5. Hypouricemia as a Risk of Cardiometabolic Diseases Compared with Normouricemia
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Freedman, D.S.; Williamson, D.F.; Gunter, E.W.; Byers, T. Relation of serum uric acid to mortality and ischemic heart disease. The NHANES I Epidemiologic Follow-up Study. Am. J. Epidemiol. 1995, 141, 637–644. [Google Scholar] [CrossRef] [PubMed]
- Ioachimescu, A.G.; Brennan, D.M.; Hoar, B.M.; Hazen, S.L.; Hoogwerf, B.J. Serum uric acid is an independent predictor of all-cause mortality in patients at high risk of cardiovascular disease: A preventive cardiology information system (PreCIS) database cohort study. Arthritis Rheumatol. 2008, 58, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Culleton, B.F.; Larson, M.G.; Kannel, W.B.; Levy, D. Serum uric acid and risk for cardiovascular disease and death: The Framingham Heart Study. Ann. Intern. Med. 1999, 131, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Moriarity, J.T.; Folsom, A.R.; Iribarren, C.; Nieto, F.J.; Rosamond, W.D. Serum uric acid and risk of coronary heart disease: Atherosclerosis Risk in Communities (ARIC) Study. Ann. Epidemiol. 2000, 10, 136–143. [Google Scholar] [CrossRef]
- Sakata, K.; Hashimoto, T.; Ueshima, H.; Okayama, A.; Group, N.D.R. Absence of an association between serum uric acid and mortality from cardiovascular disease: NIPPON DATA 80, 1980-1994. National Integrated Projects for Prospective Observation of Non-communicable Diseases and its Trend in the Aged. Eur. J. Epidemiol. 2001, 17, 461–468. [Google Scholar] [CrossRef] [PubMed]
- De Leeuw, P.W.; Thijs, L.; Birkenhager, W.H.; Voyaki, S.M.; Efstratopoulos, A.D.; Fagard, R.H.; Leonetti, G.; Nachev, C.; Petrie, J.C.; Rodicio, J.L.; et al. Prognostic significance of renal function in elderly patients with isolated systolic hypertension: Results from the Syst-Eur trial. J. Am. Soc. Nephrol. 2002, 13, 2213–2222. [Google Scholar] [CrossRef] [Green Version]
- Kuwabara, M.; Hisatome, I.; Niwa, K.; Hara, S.; Roncal-Jimenez, C.A.; Bjornstad, P.; Nakagawa, T.; Andres-Hernando, A.; Sato, Y.; Jensen, T.; et al. Uric Acid Is a Strong Risk Marker for Developing Hypertension From Prehypertension: A 5-Year Japanese Cohort Study. Hypertension 2018, 71, 78–86. [Google Scholar] [CrossRef]
- Kuwabara, M.; Niwa, K.; Hisatome, I.; Nakagawa, T.; Roncal-Jimenez, C.A.; Andres-Hernando, A.; Bjornstad, P.; Jensen, T.; Sato, Y.; Milagres, T.; et al. Asymptomatic Hyperuricemia Without Comorbidities Predicts Cardiometabolic Diseases: Five-Year Japanese Cohort Study. Hypertension 2017, 69, 1036–1044. [Google Scholar] [CrossRef]
- Kuwabara, M.; Kuwabara, R.; Hisatome, I.; Niwa, K.; Roncal-Jimenez, C.A.; Bjornstad, P.; Andres-Hernando, A.; Sato, Y.; Jensen, T.; Garcia, G.; et al. “Metabolically Healthy” Obesity and Hyperuricemia Increase Risk for Hypertension and Diabetes: 5-year Japanese Cohort Study. Obesity (Silver Spring) 2017, 25, 1997–2008. [Google Scholar] [CrossRef]
- Kuwabara, M.; Hisatome, I.; Roncal-Jimenez, C.A.; Niwa, K.; Andres-Hernando, A.; Jensen, T.; Bjornstad, P.; Milagres, T.; Cicerchi, C.; Song, Z.; et al. Increased Serum Sodium and Serum Osmolarity Are Independent Risk Factors for Developing Chronic Kidney Disease; 5 Year Cohort Study. PLoS ONE 2017, 12, e0169137. [Google Scholar] [CrossRef] [Green Version]
- Kuwabara, M.; Bjornstad, P.; Hisatome, I.; Niwa, K.; Roncal-Jimenez, C.A.; Andres-Hernando, A.; Jensen, T.; Milagres, T.; Sato, Y.; Garcia, G.; et al. Elevated Serum Uric Acid Level Predicts Rapid Decline in Kidney Function. Am. J. Nephrol. 2017, 45, 330–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuwabara, M.; Niwa, K.; Nishihara, S.; Nishi, Y.; Takahashi, O.; Kario, K.; Yamamoto, K.; Yamashita, T.; Hisatome, I. Hyperuricemia is an independent competing risk factor for atrial fibrillation. Int. J. Cardiol. 2017, 231, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Kuwabara, M.; Niwa, K.; Nishi, Y.; Mizuno, A.; Asano, T.; Masuda, K.; Komatsu, I.; Yamazoe, M.; Takahashi, O.; Hisatome, I. Relationship between serum uric acid levels and hypertension among Japanese individuals not treated for hyperuricemia and hypertension. Hypertens. Res. 2014, 37, 785–789. [Google Scholar] [CrossRef] [PubMed]
- Kuwabara, M.; Motoki, Y.; Sato, H.; Fujii, M.; Ichiura, K.; Kuwabara, K.; Nakamura, Y. Low frequency of toothbrushing practices is an independent risk factor for diabetes mellitus in male and dyslipidemia in female: A large-scale, 5-year cohort study in Japan. J. Cardiol. 2017, 70, 107–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuwabara, M.; Motoki, Y.; Ichiura, K.; Fujii, M.; Inomata, C.; Sato, H.; Morisawa, T.; Morita, Y.; Kuwabara, K.; Nakamura, Y. Association between toothbrushing and risk factors for cardiovascular disease: A large-scale, cross-sectional Japanese study. BMJ Open 2016, 6, e009870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimamoto, K.; Ando, K.; Fujita, T.; Hasebe, N.; Higaki, J.; Horiuchi, M.; Imai, Y.; Imaizumi, T.; Ishimitsu, T.; Ito, M.; et al. The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2014). Hypertens. Res. 2014, 37, 253–390. [Google Scholar] [CrossRef] [Green Version]
- Black, H.R.; Sica, D.; Ferdinand, K.; White, W.B. Eligibility and Disqualification Recommendations for Competitive Athletes With Cardiovascular Abnormalities: Task Force 6: Hypertension: A Scientific Statement from the American Heart Association and the American College of Cardiology. J. Am. Coll. cardiol. 2015, 66, 2393–2397. [Google Scholar] [CrossRef] [Green Version]
- Teramoto, T.; Sasaki, J.; Ishibashi, S.; Birou, S.; Daida, H.; Dohi, S.; Egusa, G.; Hiro, T.; Hirobe, K.; Iida, M.; et al. Executive summary of the Japan Atherosclerosis Society (JAS) guidelines for the diagnosis and prevention of atherosclerotic cardiovascular diseases in Japan-2012 version. J. Atheroscler. Thromb. 2013, 20, 517–523. [Google Scholar] [CrossRef] [Green Version]
- Matsuo, S.; Imai, E.; Horio, M.; Yasuda, Y.; Tomita, K.; Nitta, K.; Yamagata, K.; Tomino, Y.; Yokoyama, H.; Hishida, A.; et al. Revised equations for estimated GFR from serum creatinine in Japan. Am. J. Kidney Dis. 2009, 53, 982–992. [Google Scholar] [CrossRef]
- Kuwabara, M.; Niwa, K.; Ohtahara, A.; Hamada, T.; Miyazaki, S.; Mizuta, E.; Ogino, K.; Hisatome, I. Prevalence and complications of hypouricemia in a general population: A large-scale cross-sectional study in Japan. PLoS ONE 2017, 12, e0176055. [Google Scholar] [CrossRef] [Green Version]
- Verdecchia, P.; Schillaci, G.; Reboldi, G.; Santeusanio, F.; Porcellati, C.; Brunetti, P. Relation between serum uric acid and risk of cardiovascular disease in essential hypertension. The PIUMA study. Hypertension 2000, 36, 1072–1078. [Google Scholar] [CrossRef] [PubMed]
- Mazza, A.; Zamboni, S.; Rizzato, E.; Pessina, A.C.; Tikhonoff, V.; Schiavon, L.; Casiglia, E. Serum uric acid shows a J-shaped trend with coronary mortality in non-insulin-dependent diabetic elderly people. The CArdiovascular STudy in the ELderly (CASTEL). Acta Diabetol. 2007, 44, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Sugihara, S.; Hisatome, I.; Kuwabara, M.; Niwa, K.; Maharani, N.; Kato, M.; Ogino, K.; Hamada, T.; Ninomiya, H.; Higashi, Y.; et al. Depletion of Uric Acid Due to SLC22A12 (URAT1) Loss-of-Function Mutation Causes Endothelial Dysfunction in Hypouricemia. Circ. J. 2015, 79, 1125–1132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waring, W.S.; McKnight, J.A.; Webb, D.J.; Maxwell, S.R. Uric acid restores endothelial function in patients with type 1 diabetes and regular smokers. Diabetes 2006, 55, 3127–3132. [Google Scholar] [CrossRef]
- Li, X.; Meng, X.; Timofeeva, M.; Tzoulaki, I.; Tsilidis, K.K.; Ioannidis, J.P.; Campbell, H.; Theodoratou, E. Serum uric acid levels and multiple health outcomes: Umbrella review of evidence from observational studies, randomised controlled trials, and Mendelian randomisation studies. BMJ 2017, 357, j2376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jordan, D.M.; Choi, H.K.; Verbanck, M.; Topless, R.; Won, H.H.; Nadkarni, G.; Merriman, T.R.; Do, R. No causal effects of serum urate levels on the risk of chronic kidney disease: A Mendelian randomization study. PLoS Med. 2019, 16, e1002725. [Google Scholar] [CrossRef] [Green Version]
- Rasheed, H.; Hughes, K.; Flynn, T.J.; Merriman, T.R. Mendelian randomization provides no evidence for a causal role of serum urate in increasing serum triglyceride levels. Circ. Cardiovasc. Genet. 2014, 7, 830–837. [Google Scholar] [CrossRef] [Green Version]
- Kottgen, A.; Albrecht, E.; Teumer, A.; Vitart, V.; Krumsiek, J.; Hundertmark, C.; Pistis, G.; Ruggiero, D.; O’Seaghdha, C.M.; Haller, T.; et al. Genome-wide association analyses identify 18 new loci associated with serum urate concentrations. Nat. Genet. 2013, 45, 145–154. [Google Scholar] [CrossRef] [Green Version]
- Yang, Q.; Kottgen, A.; Dehghan, A.; Smith, A.V.; Glazer, N.L.; Chen, M.H.; Chasman, D.I.; Aspelund, T.; Eiriksdottir, G.; Harris, T.B.; et al. Multiple genetic loci influence serum urate levels and their relationship with gout and cardiovascular disease risk factors. Circ. Cardiovasc. Genet. 2010, 3, 523–530. [Google Scholar] [CrossRef]
- Johnson, R.J.; Segal, M.S.; Sautin, Y.; Nakagawa, T.; Feig, D.I.; Kang, D.H.; Gersch, M.S.; Benner, S.; Sanchez-Lozada, L.G. Potential role of sugar (fructose) in the epidemic of hypertension, obesity and the metabolic syndrome, diabetes, kidney disease, and cardiovascular disease. Am. J. Clin. Nutr. 2007, 86, 899–906. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Women | Men | p | |
|---|---|---|---|
| Number of Subjects | 6733 | 6337 | |
| Age | 49.9 ± 11.1 | 42.4 ± 11.5 | <0.001 |
| Body mass index (kg/m2) | 21.3 ± 3.0 | 23.8 ± 2.9 | <0.001 |
| Systolic blood pressure (mmHg) | 114.5 ± 17.5 | 124.2 ± 17.2 | <0.001 |
| Diastolic blood pressure (mmHg) | 70.8 ± 10.9 | 77.9 ± 10.9 | <0.001 |
| Pulse rate (bpm) | 75.2 ± 10.8 | 71.6 ± 10.5 | <0.001 |
| Smoking | 16.3% | 63.0% | <0.001 |
| Drinking habits | 26.0% | 61.5% | <0.001 |
| Hypertension | 13.4% | 26.8% | <0.001 |
| Diabetes mellitus | 2.1% | 6.8% | <0.001 |
| Dyslipidemia | 29.6% | 49.3% | <0.001 |
| Hypouricemia | 0.22% | 0.47% | 0.016 |
| Chronic kidney disease | 2.3% | 5.3% | <0.001 |
| eGFR (mL/min/1.73m2) | 88.2 ± 15.7 | 82.6 ± 15.5 | <0.001 |
| Serum uric acid (mg/dL) | 4.49 ± 0.95 | 6.24 ± 1.23 | <0.001 |
| Maintaining without Hypertension | Crude | Adjusted * | ||||||
|---|---|---|---|---|---|---|---|---|
| Women | OR | 95% CI | p | OR | 95% CI | p | ||
| Serum uric acid | per 1 mg/dL decreased | 1.755 | 1.587–1.941 | <0.001 | 1.306 | 1.169–1.459 | <0.001 | |
| Men | ||||||||
| Serum uric acid | per 1 mg/dL decreased | 1.180 | 1.099–1.266 | <0.001 | 1.153 | 1.068–1.245 | <0.001 | |
| Maintaining without diabetes mellitus | Crude | Adjusted † | ||||||
| Women | OR | 95% CI | p | OR | 95% CI | p | ||
| Serum uric acid | per 1 mg/dL decreased | 1.822 | 1.507–2.202 | <0.001 | 1.206 | 0.969–1.500 | 0.093 | |
| Men | ||||||||
| Serum uric acid | per 1 mg/dL decreased | 1.160 | 1.037–1.298 | 0.010 | 1.074 | 0.953–1.210 | 0.24 | |
| Maintaining without dyslipidemia | Crude | Adjusted ‡ | ||||||
| Women | OR | 95% CI | p | OR | 95% CI | p | ||
| Serum uric acid | per 1 mg/dL decreased | 1.311 | 1.202–1.429 | <0.001 | 1.121 | 1.022–1.230 | 0.015 | |
| Men | ||||||||
| Serum uric acid | per 1 mg/dL decreased | 1.205 | 1.120–1.296 | <0.001 | 1.164 | 1.077–1.258 | <0.001 | |
| Maintaining without chronic kidney disease | Crude | Adjusted ¶ | ||||||
| Women | OR | 95% CI | p | OR | 95% CI | p | ||
| Serum uric acid | per 1 mg/dL decreased | 1.655 | 1.545–1.795 | <0.001 | 1.424 | 1.311–1.547 | <0.001 | |
| Men | ||||||||
| Serum uric acid | per 1 mg/dL decreased | 1.144 | 1.082–1.210 | <0.001 | 1.226 | 1.152–1.306 | <0.001 | |
| Maintaining without hypertension | Crude | Adjusted * | ||||
|---|---|---|---|---|---|---|
| Serum uric acid | OR | 95% CI | P | OR | 95% CI | p |
| 2 mg/dL to 4 mg/dL | Reference | Reference | ||||
| 2 mg/dL and less | 1.922 | 0.444–8.328 | 0.38 | 1.705 | 0.385–7.564 | 0.48 |
| 4 mg/dL to 6 mg/dL | 2.170 | 1.756–2.682 | <0.001 | 1.543 | 1.237–1.926 | <0.001 |
| more than 6 mg/dL | 3.630 | 2.920–4.512 | <0.001 | 2.031 | 1.570–2.628 | <0.001 |
| Maintaining without diabetes mellitus | Crude | Adjusted † | ||||
| Serum uric acid | OR | 95% CI | P | OR | 95% CI | p |
| 2 mg/dL to 4 mg/dL | Reference | Reference | ||||
| 2 mg/dL and less | – | – | – | – | – | – |
| 4 mg/dL to 6 mg/dL | 2.404 | 1.530–3.779 | <0.001 | 1.405 | 0.881–2.238 | 0.153 |
| more than 6 mg/dL | 4.634 | 2.957–7.262 | <0.001 | 1.571 | 0.947–2.606 | 0.080 |
| Maintaining without dyslipidemia | Crude | Adjusted ‡ | ||||
| Serum uric acid | OR | 95% CI | P | OR | 95% CI | p |
| 2 mg/dL to 4 mg/dL | Reference | Reference | ||||
| 2 mg/dL and less | 0.384 | 0.051–2.896 | 0.35 | 0.346 | 0.046–2.622 | 0.30 |
| 4 mg/dL to 6 mg/dL | 1.437 | 1.233–1.674 | <0.001 | 1.259 | 1.073–1.478 | 0.005 |
| more than 6 mg/dL | 2.116 | 1.784–2.508 | <0.001 | 1.568 | 1.267–1.940 | <0.001 |
| Maintaining without chronic kidney disease | Crude | Adjusted ¶ | ||||
| Serum uric acid | OR | 95% CI | p | OR | 95% CI | p |
| 2 mg/dL to 4 mg/dL | Reference | Reference | ||||
| 2 mg/dL and less | 2.236 | 0.754–6.634 | 0.15 | 2.368 | 0.752–7.459 | 0.14 |
| 4 mg/dL to 6 mg/dL | 1.949 | 1.665–2.281 | <0.001 | 1.579 | 1.337–1.864 | <0.001 |
| more than 6 mg/dL | 2.716 | 2.307–3.199 | <0.001 | 2.345 | 1.927–2.854 | <0.001 |
| Hypertension | Crude | Adjusted * | |||||
|---|---|---|---|---|---|---|---|
| Women | Reference | OR | 95% CI | p | OR | 95% CI | p |
| Hypouricemia (n = 14) | Normouricemia (n = 2020) | 3.659 | 0.807–16.599 | 0.093 | 4.532 | 0.943–21.78 | 0.059 |
| Men | |||||||
| Hypouricemia (n = 22) | Normouricemia (n = 728) | 1.355 | 0.392–4.684 | 0.545 | 1.141 | 0.319–4.075 | 0.84 |
| Diabetes | Crude | Adjusted | |||||
| Women | Reference | OR | 95% CI | p | OR | 95% CI | p |
| Hypouricemia (n = 14) | normouricemia (n = 2165) | – | – | ||||
| Men | |||||||
| Hypouricemia (n = 26) | normouricemia (n = 831) | – | – | ||||
| Dyslipidemia | Crude | Adjusted † | |||||
| Women | Reference | OR | 95% CI | p | OR | 95% CI | p |
| Hypouricemia (n = 13) | normouricemia (n = 1789) | – | – | ||||
| Men | |||||||
| Hypouricemia (n = 18) | normouricemia (n = 582) | 0.28 | 0.037–2.129 | 0.219 | 0.238 | 0.031–1.847 | 0.17 |
| Chronic kidney disease | Crude | Adjusted ‡ | |||||
| Women | Reference | OR | 95% CI | p | OR | 95% CI | p |
| Hypouricemia (n = 15) | normouricemia (n = 1795) | 4.212 | 1.327–13.37 | 0.015 | 4.052 | 1.181–13.90 | 0.026 |
| Men | |||||||
| Hypouricemia (n = 29) | normouricemia (n = 932) | 0.396 | 0.093–1.681 | 0.209 | 0.303 | 0.068–1.351 | 0.117 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuwabara, M.; Hisatome, I.; Niwa, K.; Bjornstad, P.; Roncal-Jimenez, C.A.; Andres-Hernando, A.; Kanbay, M.; Johnson, R.J.; Lanaspa, M.A. The Optimal Range of Serum Uric Acid for Cardiometabolic Diseases: A 5-Year Japanese Cohort Study. J. Clin. Med. 2020, 9, 942. https://doi.org/10.3390/jcm9040942
Kuwabara M, Hisatome I, Niwa K, Bjornstad P, Roncal-Jimenez CA, Andres-Hernando A, Kanbay M, Johnson RJ, Lanaspa MA. The Optimal Range of Serum Uric Acid for Cardiometabolic Diseases: A 5-Year Japanese Cohort Study. Journal of Clinical Medicine. 2020; 9(4):942. https://doi.org/10.3390/jcm9040942
Chicago/Turabian StyleKuwabara, Masanari, Ichiro Hisatome, Koichiro Niwa, Petter Bjornstad, Carlos A. Roncal-Jimenez, Ana Andres-Hernando, Mehmet Kanbay, Richard J. Johnson, and Miguel A. Lanaspa. 2020. "The Optimal Range of Serum Uric Acid for Cardiometabolic Diseases: A 5-Year Japanese Cohort Study" Journal of Clinical Medicine 9, no. 4: 942. https://doi.org/10.3390/jcm9040942