Quantified Vascular Calcification at the Dialysis Access Site: Correlations with the Coronary Artery Calcium Score and Survival Analysis of Access and Cardiovascular Outcomes

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Patients
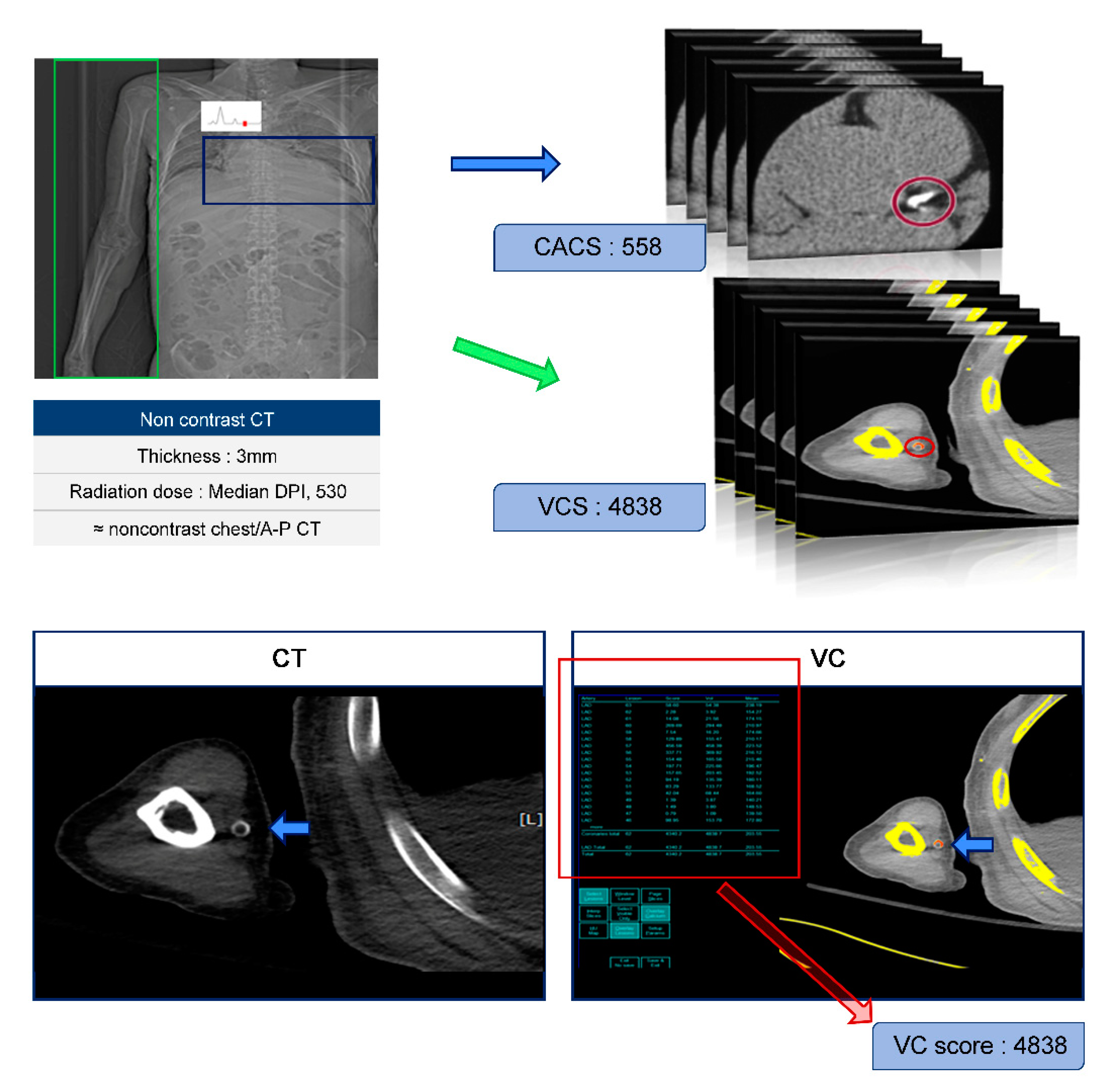
2.2. Protocols of CT and Calculation of CACS and VCS
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Subjects
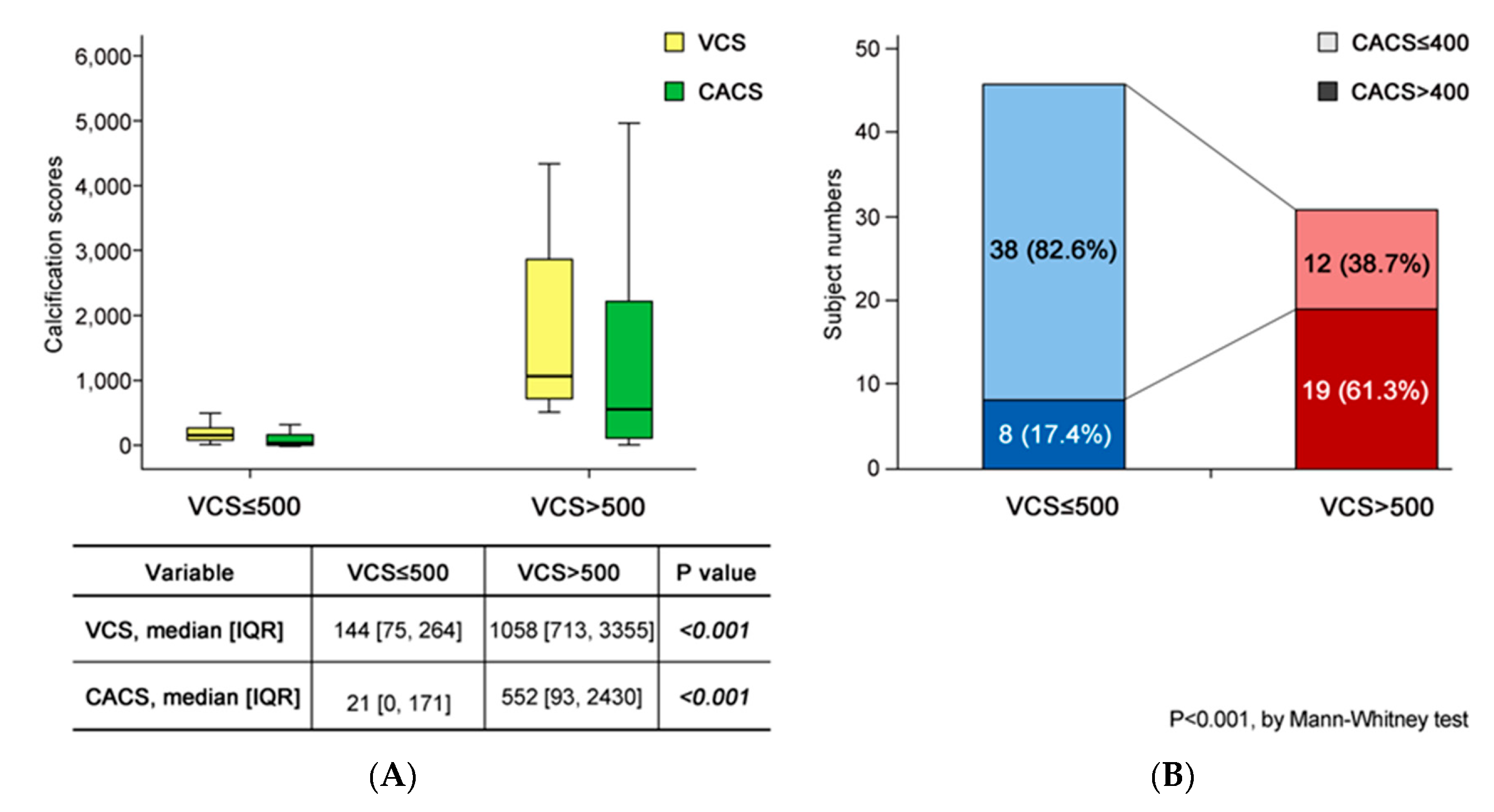
3.2. CACS in the Two Groups Defined by VCS
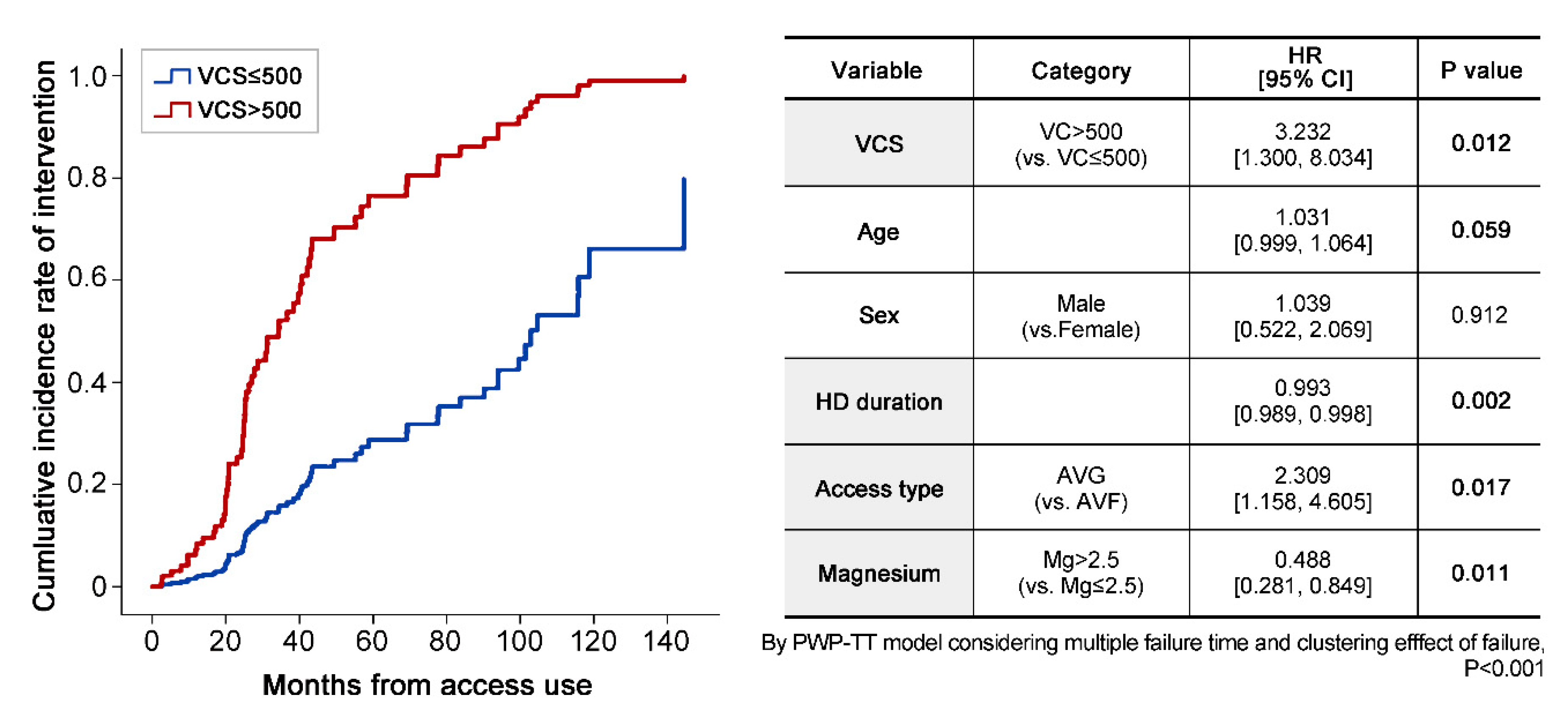
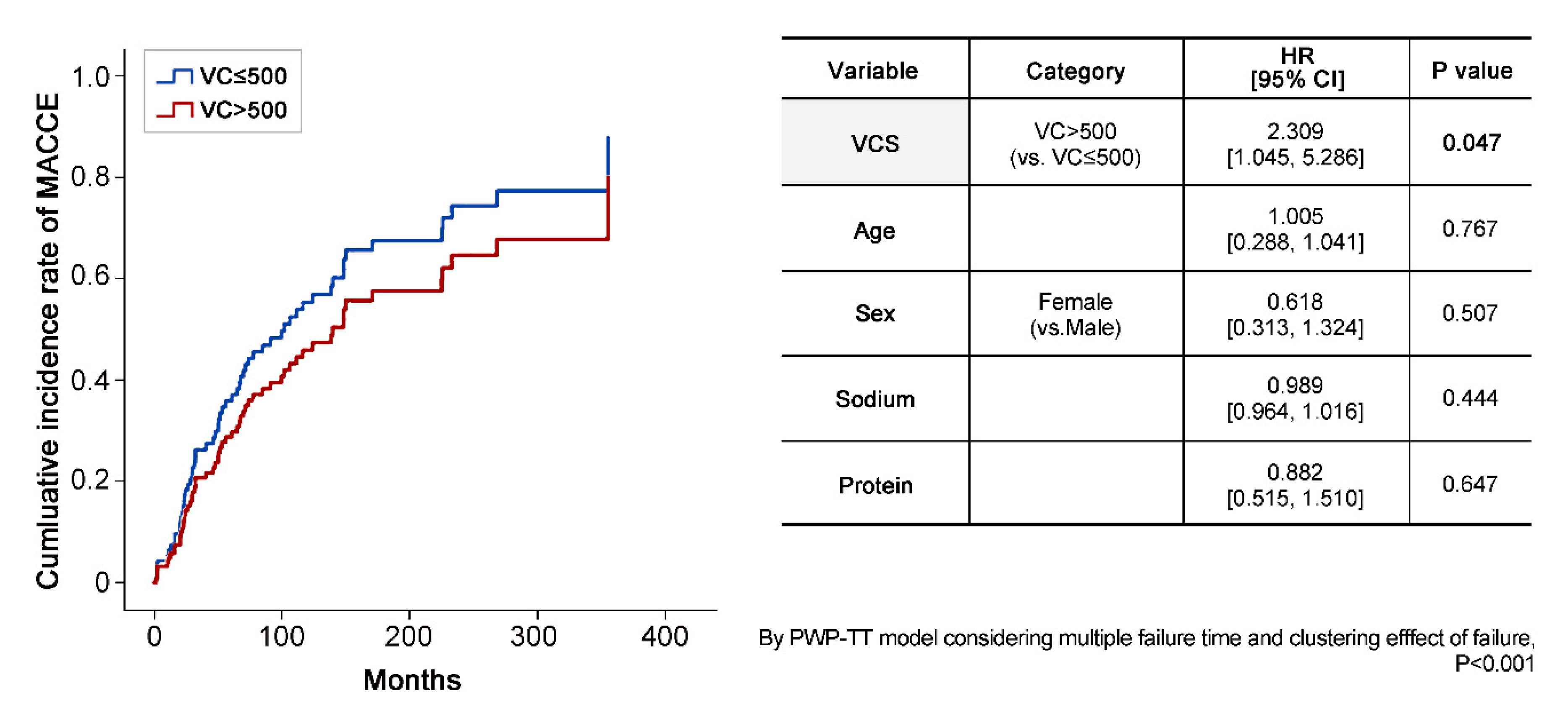
3.3. Prevalence of Events in the Two Groups Defined by VCS
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Blaha, M.J.; Mortensen, M.B.; Kianoush, S.; Tota-Maharaj, R.; Cainzos-Achirica, M. Coronary artery calcium scoring: Is it time for a change in methodology? JACC Cardiovasc. Imaging 2017, 10, 923–937. [Google Scholar]
- Schlieper, G.; Krüger, T.; Djuric, Z.; Damjanovic, T.; Markovic, N.; Schurgers, L.J.; Brandenburg, V.M.; Westenfeld, R.; Dimkovic, S.; Ketteler, M. Vascular access calcification predicts mortality in hemodialysis patients. Kidney Int. 2008, 74, 1582–1587. [Google Scholar] [CrossRef] [PubMed]
- London, G.M.; Guerin, A.P.; Marchais, S.J.; Metivier, F.; Pannier, B.; Adda, H. Arterial media calcification in end-stage renal disease: Impact on all-cause and cardiovascular mortality. Nephrol. Dial. Transpl. 2003, 18, 1731–1740. [Google Scholar] [CrossRef]
- Chen, J.; Budoff, M.J.; Reilly, M.P.; Yang, W.; Rosas, S.E.; Rahman, M.; Zhang, X.; Roy, J.A.; Lustigova, E.; Nessel, L. Coronary artery calcification and risk of cardiovascular disease and death among patients with chronic kidney disease. JAMA Cardiol. 2017, 2, 635–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sigrist, M.K.; Taal, M.W.; Bungay, P.; McIntyre, C.W. Progressive vascular calcification over 2 years is associated with arterial stiffening and increased mortality in patients with stages 4 and 5 chronic kidney disease. Clin. J. Am. Soc. Nephrol. 2007, 2, 1241–1248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuoka, M.; Iseki, K.; Tamashiro, M.; Fujimoto, N.; Higa, N.; Touma, T.; Takishita, S. Impact of high coronary artery calcification score (CACS) on survival in patients on chronic hemodialysis. J. Clin. Exp. Nephrol. 2004, 8, 54–58. [Google Scholar] [CrossRef]
- Moe, S.M.; Chen, N.X. Pathophysiology of vascular calcification in chronic kidney disease. Circ. Res. 2004, 95, 560–567. [Google Scholar] [CrossRef] [Green Version]
- Reynolds, J.L.; Joannides, A.J.; Skepper, J.N.; McNair, R.; Schurgers, L.J.; Proudfoot, D.; Jahnen-Dechent, W.; Weissberg, P.L.; Shanahan, C.M. Human vascular smooth muscle cells undergo vesicle-mediated calcification in response to changes in extracellular calcium and phosphate concentrations: A potential mechanism for accelerated vascular calcification in ESRD. J. Am. Soc. Nephrol. 2004, 15, 2857–2867. [Google Scholar] [CrossRef] [Green Version]
- Ketteler, M. Fetuin-A and extraosseous calcification in uremia. Curr. Opin. Nephrol. Hypertens. 2005, 14, 337–342. [Google Scholar] [CrossRef]
- Block, G.; Raggi, P.; Bellasi, A.; Kooienga, L.; Spiegel, D. Mortality effect of coronary calcification and phosphate binder choice in incident hemodialysis patients. Kidney Int. 2007, 71, 438–441. [Google Scholar] [CrossRef] [Green Version]
- Derici, U.; El Nahas, A.M. Vascular calcifications in uremia: Old concepts and new insights. Semin. Dial. 2006, 19, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Corpataux, J.M.; Haesler, E.; Silacci, P.; Ris, H.B.; Hayoz, D. Low-pressure environment and remodelling of the forearm vein in Brescia-Cimino haemodialysis access. Nephrol. Dia. Transplan. 2002, 17, 1057–1062. [Google Scholar] [CrossRef] [Green Version]
- Wong, V.; Ward, R.; Taylor, J.; Selvakumar, S.; How, T.; Bakran, A. Factors associated with early failure of arteriovenous fistulae for haemodialysis access. Eur. J. Vasc. Endovasc. Surg. 1996, 12, 207–213. [Google Scholar] [CrossRef] [Green Version]
- Toussaint, N.D.; Lau, K.K.; Polkinghorne, K.R.; Kerr, P.G. Measurement of vascular calcification using CT fistulograms. Nephrol. Dial. Transplant. 2006, 22, 484–490. [Google Scholar] [CrossRef] [Green Version]
- Cano-Megias, M.; Guisado-Vasco, P.; Bouarich, H.; de Arriba-de la Fuente, G.; de Sequera-Ortiz, P.; Alvarez-Sanz, C.; Rodriguez-Puyol, D. Coronary calcification as a predictor of cardiovascular mortality in advanced chronic kidney disease: A prospective long-term follow-up study. BMC Nephrol. 2019, 20, 188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrauskiene, V.; Vaiciuniene, R.; Bumblyte, I.A.; Kuzminskis, V.; Ziginskiene, E.; Grazulis, S.; Jonaitiene, E. Association between vascular calcification assessed by simple radiography and non-fatal cardiovascular events in hemodialysis patients. Nephrol. Ther. 2016, 12, 503–507. [Google Scholar] [CrossRef]
- Amorim, L.D.; Cai, J. Modelling recurrent events: A tutorial for analysis in epidemiology. Int. J. Epidemiol. 2015, 44, 324–333. [Google Scholar] [CrossRef]
- Guedes, M.M.; Botelho, C.; Maia, P.; Ibeas, J.; Ponce, P. Doppler ultrasound and calcification score: Improving vascular access surveillance. R. Fail. 2015, 37, 1425–1429. [Google Scholar] [CrossRef] [Green Version]
- Baktiroglu, S.; Yanar, F.; Ozata, I.H.; Oner, G.; Ercan, D. Arterial disease and vascular access in diabetic patients. J. Vasc. Access 2016, 17 (Suppl. S69), 1–71. [Google Scholar] [CrossRef]
- Ter Braake, A.D.; Shanahan, C.M.; de Baaij, J.H.F. Magnesium Counteracts Vascular Calcification: Passive Interference or Active Modulation? Arteriosclerosis Thrombosis Vasc. Bio. 2017, 37, 1431–1445. [Google Scholar] [CrossRef] [Green Version]
- Del Gobbo, L.C.; Imamura, F.; Wu, J.H.; de Oliveira Otto, M.C.; Chiuve, S.E.; Mozaffarian, D. Circulating and dietary magnesium and risk of cardiovascular disease: A systematic review and meta-analysis of prospective studies. Am. J. Clin. Nutr. 2013, 98, 160–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costello, R.B.; Elin, R.J.; Rosanoff, A.; Wallace, T.C.; Guerrero-Romero, F.; Hruby, A.; Lutsey, P.L.; Nielsen, F.H.; Rodriguez-Moran, M.; Song, Y.; et al. Perspective: The Case for an Evidence-Based Reference Interval for Serum Magnesium: The Time Has Come. Adv. Nutr. 2016, 7, 977–993. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | VCS ≤ 500 | VCS > 500 | p-Value |
|---|---|---|---|
| N (%) | 46 (59.7) | 31 (40.3) | |
| Male sex, n (%) | 23 (50.0) | 21 (67.7) | 0.564 |
| Age, years, median [IQR] | 64.3 [57.0, 74.0] | 63.0 [55.0, 67.0] | 0.125 |
| Etiology, n (%) | 0.836 | ||
| Diabetes | 23 (50) | 17 (54.8) | |
| HTN | 17 (37) | 9 (29.0) | |
| CGN | 0 (0) | 1 (3.2) | |
| PKD | 2 (4.3) | 0 (0) | |
| Others | 4 (8.7) | 4 (12.9) | |
| Baseline comorbidity | |||
| HTN | 35 (76.1) | 25 (80.6) | 0.638 |
| Stroke | 2 (4.3) | 0 (0) | 0.243 |
| Myocardial infarction or PAD | 0 (0) | 0 (0) | |
| SBP, mmHg, median [IQR] | 150 [130, 170] | 145 [120, 170] | 0.457 |
| DBP, mmHg, median [IQR] | 70 [70, 80] | 70 [60, 80] | 0.308 |
| AVF (vs. AVG), n (%) | 43 (93.5) | 23 (74.2) | 0.018 |
| HD vintage, months, median [IQR] | 36.6 [20.9, 60.2] | 89.1 [46.8, 137.6] | <0.001 |
| UF volume, kg, median [IQR] | 2.1 [1.5, 3.0] | 2.2 [1.5, 3.0] | 0.569 |
| Height, cm, median [IQR] | 161.7 [154.9, 169.1] | 164.0 [154.0, 170.5] | 0.884 |
| Dry weight, kg, median [IQR] | 60.5 [53.8, 70.1] | 57.5 [48.0, 61.5] | 0.149 |
| spKt/V, median [IQR] | 1.74 [1.49, 2.09] | 1.81 [1.63, 2.10] | 0.399 |
| URR, %, median [IQR] | 77.0 [71.8, 81.3] | 77.7 [74.3, 82.3] | 0.443 |
| Hb, g/dL, median [IQR] | 10.4 [9.8, 11.1] | 10.2 [9.6, 10.9] | 0.352 |
| Uric acid, mg/dL, median [IQR] | 7.2 [6.3, 8.6] | 6.9 [5.9, 7.8] | 0.253 |
| Total cholesterol, mg/dL, median [IQR] | 131.0 [108.5, 147.5] | 114.5 [105.3, 139.0] | 0.071 |
| Albumin, g/dL, median [IQR] | 3.8 [3.6, 3.9] | 3.6 [3.3, 4.0] | 0.043 |
| Triglycerides, mg/dL, median [IQR] | 115.5 [80.0, 182.3] | 102.0 [72.0, 116.0] | 0.086 |
| Ferritin, ng/mL, median [IQR] | 204.1 [115.7, 292.0] | 153.5 [67.7, 251.7] | 0.072 |
| B2 microglobulin, mg/L, median [IQR] | 2.6 [2.4, 2.8] | 2.7 [2.4, 2.9] | 0.602 |
| 25(OH) vitamin D, ng/mL, median [IQR] | 21.2 [14.7, 25.7] | 19.0 [12.0, 24.4] | 0.5 |
| Calcium, mg/dL, median [IQR] | 8.1 [7.6, 8.5] | 8.3 [7.8, 8.6] | 0.255 |
| Phosphorus, mg/dL, median [IQR] | 4.8 [3.9, 5.4] | 4.7 [3.9, 5.8] | 0.762 |
| iPTH, pg/mL, median [IQR] | 277.5 [142.3, 423.0] | 307.0 [70.2, 596.0] | 0.561 |
| Magnesium, mg/dL, median [IQR] | 2.6 [2.4, 2.8] | 2.7 [2.4, 2.9] | 0.602 |
| Variable | Total | VCS ≤ 500 | VCS > 500 | p-Value |
|---|---|---|---|---|
| N (%) | 77 | 46 (59.7) | 31 (40.3) | |
| VCS, median [IQR] | 307 [114, 874] | 144 [75, 264] | 1058 [713, 3355] | <0.001 |
| CACS = 0, n (%) | 19 (24.7) | 17 (37.0) | 2 (6.5) | 0.002 |
| CACS, median [IQR] | 101 [1, 673] | 21 [0, 171] | 552 [93, 2430] | <0.001 |
| VC on X-rays, n (%) | 77 | 38 (82.6) | 31 (100) | 0.015 |
| Variable | VCS ≤ 500 | VCS > 500 | p-Value |
|---|---|---|---|
| Intervention (PTA or surgery), n (%) | 9 (19.6) | 23 (74.2) | <0.001 |
| Number of interventions/yr, median [IQR] | 0 [0, 0] | 0.46 [0, 1.25] | <0.001 |
| Number of admissions/yr, median [IQR] | 2.9 [1.7, 5.1] | 2.9 [2.0, 6.0] | 0.553 |
| Duration of admission/yr, median [IQR] | 15.3 [5.6, 26.7] | 18.4 [6.7, 54.3] | 0.114 |
| MACCE, n (%) | 19 (41.3) | 18 (58.1) | 0.149 |
| Number of MACCE/yr, median [IQR] | 0 [0, 0.1] | 0 [0, 0.1] | 0.968 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.; Lee, B.; Choi, G.; Jin, H.Y.; Jung, H.; Hwang, S.; Yoon, H.; Kim, S.h.; Park, H.S.; Lee, J.; et al. Quantified Vascular Calcification at the Dialysis Access Site: Correlations with the Coronary Artery Calcium Score and Survival Analysis of Access and Cardiovascular Outcomes. J. Clin. Med. 2020, 9, 1558. https://doi.org/10.3390/jcm9051558
Kim H, Lee B, Choi G, Jin HY, Jung H, Hwang S, Yoon H, Kim Sh, Park HS, Lee J, et al. Quantified Vascular Calcification at the Dialysis Access Site: Correlations with the Coronary Artery Calcium Score and Survival Analysis of Access and Cardiovascular Outcomes. Journal of Clinical Medicine. 2020; 9(5):1558. https://doi.org/10.3390/jcm9051558
Chicago/Turabian StyleKim, Hyunsuk, Bom Lee, Gwangho Choi, Ho Yong Jin, Houn Jung, Sunghyun Hwang, Hojung Yoon, Seok hyung Kim, Hoon Suk Park, Jongseok Lee, and et al. 2020. "Quantified Vascular Calcification at the Dialysis Access Site: Correlations with the Coronary Artery Calcium Score and Survival Analysis of Access and Cardiovascular Outcomes" Journal of Clinical Medicine 9, no. 5: 1558. https://doi.org/10.3390/jcm9051558