Visual Verticality Perception in Spinal Diseases: A Systematic Review and Meta-Analysis

 ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Methods
2.1. Protocol
2.2. Data Sources and Search Strategy
2.3. Study Selection and Inclusion Criteria
2.4. Data Extraction
2.5. Quality Assessment
2.6. Statistical Analysis
3. Results
3.1. Study Selection
3.2. Characteristics of Studies Included in the Meta-Analysis
3.3. Quality Assessment of Studies Included in the Meta-Analysis
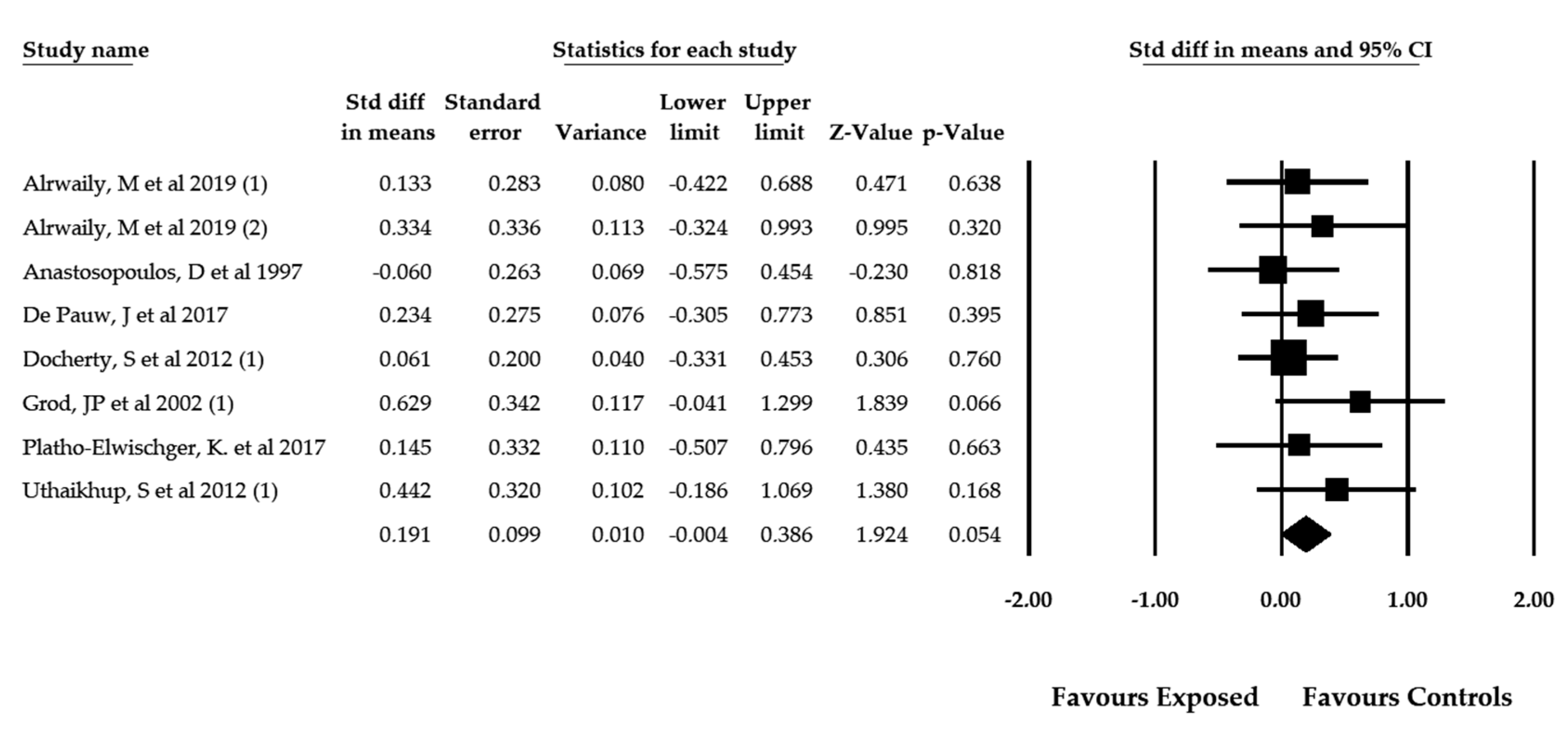
3.4. Results of the Overall Meta-Analysis about Perception of Visual Verticality in Spinal Pain Patients Measured with the SVV Test
3.5. Results of the Overall Meta-Analysis about Perception of Visual Verticality Measured with RFT in Patients with Different Spinal Pain
3.6. Results of the Overall Meta-Analysis about Perception of Visual Verticality in Patients with Idiopathic Scoliosis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ferreira, M.L.; de Luca, K. Spinal pain and its impact on older people. Best Pract. Res. Clin. Rheumatol. 2017, 31, 192–202. [Google Scholar] [CrossRef] [PubMed]
- Connelly, L.B.; Woolf, A.; Brooks, P. Cost-Effectiveness of Interventions for Musculoskeletal Conditions; Jamison, D.T., Breman, J.G., Measham, A.R., Alleyne, G., Claeson, M., Evans, D.B., Jha, P., Mills, A., Musgrove, P., Eds.; Oxford University Press: Washington, DC, USA, 2006; ISBN 0-8213-6179-1. [Google Scholar]
- Friedly, J.; Standaert, C.; Chan, L. Epidemiology of spine care: The back pain dilemma. Phys. Med. Rehabil. Clin. N. Am. 2010, 21, 659–677. [Google Scholar] [CrossRef] [Green Version]
- Hoy, D.G.; Protani, M.; De, R.; Buchbinder, R. The epidemiology of neck pain. Best Pract. Res. Clin. Rheumatol. 2010, 24, 783–792. [Google Scholar] [CrossRef] [PubMed]
- Hoy, D.; Brooks, P.; Blyth, F.; Buchbinder, R. The Epidemiology of low back pain. Best Pract. Res. Clin. Rheumatol. 2010, 24, 769–781. [Google Scholar] [CrossRef] [PubMed]
- Vos, T.; Barber, R.M.; Bell, B.; Bertozzi-Villa, A.; Biryukov, S.; Bolliger, I.; Charlson, F.; Davis, A.; Degenhardt, L.; Dicker, D.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet (London, England) 2015, 386, 743–800. [Google Scholar] [CrossRef] [Green Version]
- March, L.; Smith, E.U.R.; Hoy, D.G.; Cross, M.J.; Sanchez-Riera, L.; Blyth, F.; Buchbinder, R.; Vos, T.; Woolf, A.D. Burden of disability due to musculoskeletal (MSK) disorders. Best Pract. Res. Clin. Rheumatol. 2014, 28, 353–366. [Google Scholar] [CrossRef]
- Lardon, A.; Dubois, J.-D.; Cantin, V.; Piche, M.; Descarreaux, M. Predictors of disability and absenteeism in workers with non-specific low back pain: A longitudinal 15-month study. Appl. Ergon. 2018, 68, 176–185. [Google Scholar] [CrossRef]
- de Luca, K.E.; Parkinson, L.; Haldeman, S.; Byles, J.E.; Blyth, F. The Relationship Between Spinal Pain and Comorbidity: A Cross-sectional Analysis of 579 Community-Dwelling, Older Australian Women. J. Manip. Physiol. Ther. 2017, 40, 459–466. [Google Scholar] [CrossRef]
- Lee, C.-H.; Chung, C.K.; Kim, C.H.; Kwon, J.-W. Health Care Burden of Spinal Diseases in the Republic of Korea: Analysis of a Nationwide Database from 2012 through 2016. Neurospine 2018, 15, 66–76. [Google Scholar] [CrossRef] [Green Version]
- Patel, E.A.; Perloff, M.D. Radicular Pain Syndromes: Cervical, Lumbar, and Spinal Stenosis. Semin. Neurol. 2018, 38, 634–639. [Google Scholar] [CrossRef]
- Dieleman, J.L.; Baral, R.; Birger, M.; Bui, A.L.; Bulchis, A.; Chapin, A.; Hamavid, H.; Horst, C.; Johnson, E.K.; Joseph, J.; et al. US Spending on Personal Health Care and Public Health, 1996–2013. JAMA 2016, 316, 2627–2646. [Google Scholar] [CrossRef] [PubMed]
- Green, B.N.; Johnson, C.D.; Haldeman, S.; Kane, E.J.; Clay, M.B.; Griffith, E.A.; Castellote, J.M.; Smuck, M.; Rajasekaran, S.; Hurwitz, E.L.; et al. The Global Spine Care Initiative: Public health and prevention interventions for common spine disorders in low- and middle-income communities. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2018, 27, 838–850. [Google Scholar] [CrossRef] [PubMed]
- Buchbinder, R.; van Tulder, M.; Öberg, B.; Costa, L.M.; Woolf, A.; Schoene, M.; Croft, P. Low back pain: A call for action. Lancet (London, England) 2018, 391, 2384–2388. [Google Scholar] [CrossRef]
- Treleaven, J. Dizziness, Unsteadiness, Visual Disturbances, and Sensorimotor Control in Traumatic Neck Pain. J. Orthop. Sports Phys. Ther. 2017, 47, 492–502. [Google Scholar] [CrossRef] [PubMed]
- Thornes, E.; Robinson, H.S.; Vollestad, N.K. Dynamic balance in patients with degenerative lumbar spinal stenosis; a cross-sectional study. BMC Musculoskelet. Disord. 2018, 19, 192. [Google Scholar] [CrossRef] [PubMed]
- Iversen, M.D.; Kale, M.K.; Sullivan, J.T.J. Pilot case control study of postural sway and balance performance in aging adults with degenerative lumbar spinal stenosis. J. Geriatr. Phys. Ther. 2009, 32, 15–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saadat, M.; Salehi, R.; Negahban, H.; Shaterzadeh, M.J.; Mehravar, M.; Hessam, M. Postural stability in patients with non-specific chronic neck pain: A comparative study with healthy people. Med. J. Islam. Repub. Iran 2018, 32, 33. [Google Scholar] [CrossRef]
- Treleaven, J. Sensorimotor disturbances in neck disorders affecting postural stability, head and eye movement control—Part 2: Case studies. Man. Ther. 2008, 13, 266–275. [Google Scholar] [CrossRef]
- Johanson, E.; Brumagne, S.; Janssens, L.; Pijnenburg, M.; Claeys, K.; Paasuke, M. The effect of acute back muscle fatigue on postural control strategy in people with and without recurrent low back pain. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2011, 20, 2152–2159. [Google Scholar] [CrossRef] [Green Version]
- Dufvenberg, M.; Adeyemi, F.; Rajendran, I.; Oberg, B.; Abbott, A. Does postural stability differ between adolescents with idiopathic scoliosis and typically developed? A systematic literature review and meta-analysis. Scoliosis Spinal Disord. 2018, 13, 19. [Google Scholar] [CrossRef]
- Haddas, R.; Lieberman, I.H. The Change in Sway and Neuromuscular Activity in Adult Degenerative Scoliosis Patients Pre and Post Surgery Compared With Controls. Spine (Phila Pa 1976) 2019, 44, E899–E907. [Google Scholar] [CrossRef] [PubMed]
- Antoniadou, N.; Hatzitaki, V.; Stavridis, S.I.; Samoladas, E. Verticality perception reveals a vestibular deficit in adolescents with idiopathic scoliosis. Exp. Brain Res. 2018, 236, 1725–1734. [Google Scholar] [CrossRef] [PubMed]
- Dieterich, M.; Brandt, T. Perception of Verticality and Vestibular Disorders of Balance and Falls. Front. Neurol. 2019, 10, 172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Min, K.K.; Ha, J.S.; Kim, M.J.; Cho, C.H.; Cha, H.E.; Lee, J.H. Clinical use of subjective visual horizontal and vertical in patients of unilateral vestibular neuritis. Otol. Neurotol. 2007, 28, 520–525. [Google Scholar] [CrossRef] [PubMed]
- Mazibrada, G.; Tariq, S.; Perennou, D.; Gresty, M.; Greenwood, R.; Bronstein, A.M. The peripheral nervous system and the perception of verticality. Gait Posture 2008, 27, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Piscicelli, C.; Barra, J.; Davoine, P.; Chrispin, A.; Nadeau, S.; Pérennou, D. Inter- and Intra-Rater Reliability of the Visual Vertical in Subacute Stroke. Stroke 2015, 46, 1979–1983. [Google Scholar] [CrossRef] [Green Version]
- Piscicelli, C.; Nadeau, S.; Barra, J.; Perennou, D. Assessing the visual vertical: How many trials are required? BMC Neurol. 2015, 15, 215. [Google Scholar] [CrossRef] [Green Version]
- Funabashi, M.; Santos-Pontelli, T.E.G.; Colafêmina, J.F.; Pavan, T.Z.; Carneiro, A.A.O.; Takayanagui, O.M. A newmethod to analyze the subjective visual vertical in patients with bilateral vestibular dysfunction. Clinics 2012, 67, 1127–1131. [Google Scholar] [CrossRef]
- Bagust, J.; Docherty, S.; Haynes, W.; Telford, R.; Isableu, B. Changes in rod and frame test scores recorded in schoolchildren during development--a longitudinal study. PLoS ONE 2013, 8, e65321. [Google Scholar] [CrossRef] [Green Version]
- Perennou, D.; Piscicelli, C.; Barbieri, G.; Jaeger, M.; Marquer, A.; Barra, J. Measuring verticality perception after stroke: Why and how? Neurophysiol. Clin. 2014, 44, 25–32. [Google Scholar] [CrossRef]
- Humphreys, B.K. Cervical outcome measures: Testing for postural stability and balance. J. Manip. Physiol. Ther. 2008, 31, 540–546. [Google Scholar] [CrossRef]
- Bronstein, A.M. The interaction of otolith and proprioceptive information in the perception of verticality. The effects of labyrinthine and CNS disease. Ann. N. Y. Acad. Sci. 1999, 871, 324–333. [Google Scholar] [CrossRef]
- Lubeck, A.J.A.; Bos, J.E.; Stins, J.F. Framing visual roll-motion affects postural sway and the subjective visual vertical. Atten. Percept. Psychophys. 2016, 78, 2612–2620. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Intervention Version 5.1.0; updated March 2011; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bagust, J.; Docherty, S.; Abdul Razzak, R. Re: High variability of the subjective visual vertical test of vertical perception, in some people with neck pain—Should this be a standard measure of cervical proprioception? Man. Ther. 2015, 20, e18. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 13 May 2020).
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [Green Version]
- Lo, C.K.-L.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef] [Green Version]
- Luchini, C.; Stubbs, B.; Solmi, M.; Veronese, N. Assessing the quality of studies in meta-analyses: Advantages and limitations of the Newcastle Ottawa Scale. World J. Meta-Anal. 2017, 5, 80. [Google Scholar] [CrossRef]
- Meader, N.; King, K.; Llewellyn, A.; Norman, G.; Brown, J.; Rodgers, M.; Moe-Byrne, T.; Higgins, J.P.; Sowden, A.; Stewart, G. A checklist designed to aid consistency and reproducibility of GRADE assessments: Development and pilot validation. Syst. Rev. 2014, 3, 82. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borenstein, M.; Hedges, L.; Higgins, J.; Rothstein, H. Comprehensive Meta-Analysis Software Version 3; Biostat, Inc.: Englewood, NJ, USA, 2020. [Google Scholar]
- Cooper, H.; Hedges, L.V.; Valentine, J.C. The Handbook of Research Synthesis and Meta-Analysis; Russell Sage Foundation: New York, NY, USA, 2009. [Google Scholar]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: New York, NY, USA, 1977. [Google Scholar]
- Faraone, S.V. Interpreting estimates of treatment effects: Implications for managed care. Pharm. Ther. 2008, 33, 700. [Google Scholar]
- Rücker, G.; Schwarzer, G. Beyond the forest plot: The drapery plot. Res. Synth. Methods 2020. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Egger, M. Funnel plots for detecting bias in meta-analysis: Guidelines on choice of axis. J. Clin. Epidemiol. 2001, 54, 1046–1055. [Google Scholar] [CrossRef]
- Peters, J.L.; Sutton, A.J.; Jones, D.R.; Abrams, K.R.; Rushton, L. Comparison of two methods to detect publication bias in meta-analysis. JAMA 2006, 295, 676–680. [Google Scholar] [CrossRef] [Green Version]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Shi, L.; Lin, L.; Omboni, S. The trim-and-fill method for publication bias: Practical guidelines and recommendations based on a large database of meta-analyses. Medicine 2019, 98, e15987. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Alrwaily, M.; Sparto, P.J.; Whitney, S.L. Perception of verticality is altered in people with severe chronic low back pain compared to healthy controls: A cross-sectional study. Musculoskelet. Sci. Pract. 2020, 45, 102074. [Google Scholar] [CrossRef] [PubMed]
- Anastasopoulos, D.; Bhatia, K.; Bronstein, A.M.; Marsden, C.D.; Gresty, M.A. Perception of spatial orientation in spasmodic torticollis. Part 2: The visual vertical. Mov. Disord. 1997, 12, 709–714. [Google Scholar] [CrossRef]
- Hiengkaew, V.; Panichaporn, W.; Thanungkul, S. Postural balance, visual verticality perception, and its association in individuals with and without neck pain. J. Med. Assoc. Thail. 2014, 97, S70–S74. [Google Scholar]
- Le Berre, M.; Pradeau, C.; Brouillard, A.; Coget, M.; Massot, C.; Catanzariti, J.-F. Do Adolescents With Idiopathic Scoliosis Have an Erroneous Perception of the Gravitational Vertical? Spine Deform. 2019, 7, 71–79. [Google Scholar] [CrossRef]
- Platho-Elwischger, K.; Kranz, G.; Sycha, T.; Dunkler, D.; Rommer, P.; Mueller, C.; Auff, E.; Wiest, G. Plasticity of static graviceptive function in patients with cervical dystonia. J. Neurol. Sci. 2017, 373, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Treleaven, J.; Takasaki, H. High variability of the subjective visual vertical test of vertical perception, in some people with neck pain—Should this be a standard measure of cervical proprioception? Man. Ther. 2015, 20, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Uthaikhup, S.; Jull, G.; Sungkarat, S.; Treleaven, J. The influence of neck pain on sensorimotor function in the elderly. Arch. Gerontol. Geriatr. 2012, 55, 667–672. [Google Scholar] [CrossRef]
- Bagust, J.; Rix, G.D.; Hurst, H.C. Use of a Computer Rod and Frame (CRAF) Test to assess errors in the perception of visual vertical in a clinical setting—A pilot study. Clin. Chiropr. 2005, 8, 134–139. [Google Scholar] [CrossRef]
- Cakrt, O.; Slabý, K.; Viktorinová, L.; Kolář, P.; Jeřábek, J. Subjective visual vertical in patients with idiopatic scoliosis. J. Vestib. Res. 2011, 21, 161–165. [Google Scholar] [CrossRef]
- Catanzariti, J.-F.; Le Berre, M.; Coget, M.; Guyot, M.; Agnani, O.; Donzé, C. Subjective Visual Vertical and Adolescent Idiopathic Scoliosis (AIS). Ann. Phys. Rehabil. Med. 2015, 58, e111. [Google Scholar] [CrossRef] [Green Version]
- Cheung, J.; Sluiter, W.J.; Veldhuizen, A.G.; Cool, J.C.; Van Horn, J.R. Perception of vertical and horizontal orientation in children with scoliosis. J. Orthop. Res. 2002, 20, 416–420. [Google Scholar] [CrossRef]
- De Pauw, J.; De Hertogh, W.; Mercelis, R.; Saeys, W.; Hallemans, A.; Michiels, S.; Truijen, S.; Cras, P. Is perception of visual verticality intact in patients with idiopathic cervical dystonia? Acta Neurol. Belg. 2018, 118, 77–84. [Google Scholar] [CrossRef]
- de Zoete, R.M.J.; Osmotherly, P.G.; Rivett, D.A.; Snodgrass, S.J. No Differences Between Individuals With Chronic Idiopathic Neck Pain and Asymptomatic Individuals on 7 Cervical Sensorimotor Control Tests: A Cross-sectional Study. J. Orthop. Sports Phys. Ther. 2020, 50, 33–43. [Google Scholar] [CrossRef]
- Docherty, S.; Schärer, R.; Bagust, J.; Humphreys, B.K. Perception of subjective visual vertical and horizontal in patients with chronic neck pain: A cross-sectional observational study. Man. Ther. 2012, 17, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Grod, J.P.; Diakow, P.R. Effect of neck pain on verticality perception: A cohort study. Arch. Phys. Med. Rehabil. 2002, 83, 412–415. [Google Scholar] [CrossRef] [PubMed]
- Piscicelli, C.; Perennou, D. Visual verticality perception after stroke: A systematic review of methodological approaches and suggestions for standardization. Ann. Phys. Rehabil. Med. 2017, 60, 208–216. [Google Scholar] [CrossRef] [PubMed]
- Molina, F.; Lomas-Vega, R.; Obrero-Gaitán, E.; Rus, A.; Almagro, D.R.; Del-Pino-Casado, R. Misperception of the subjective visual vertical in neurological patients with or without stroke: A meta-analysis. NeuroRehabilitation 2019, 44, 379–388. [Google Scholar] [CrossRef]
- Mansfield, A.; Fraser, L.; Rajachandrakumar, R.; Danells, C.J.; Knorr, S.; Campos, J. Is perception of vertical impaired in individuals with chronic stroke with a history of “pushing”? Neurosci. Lett. 2015, 590, 172–177. [Google Scholar] [CrossRef] [Green Version]
- Saeys, W.; Herssens, N.; Verwulgen, S.; Truijen, S. Sensory information and the perception of verticality in post-stroke patients. Another point of view in sensory reweighting strategies. PLoS ONE 2018, 13, e0199098. [Google Scholar] [CrossRef]
- Pereira, C.B.; Kanashiro, A.K.; Maia, F.M.; Barbosa, E.R. Correlation of impaired subjective visual vertical and postural instability in Parkinson’s disease. J. Neurol. Sci. 2014, 346, 60–65. [Google Scholar] [CrossRef]
- Schindlbeck, K.A.; Naumann, W.; Maier, A.; Ehlen, F.; Marzinzik, F.; Klostermann, F. Disturbance of verticality perception and postural dysfunction in Parkinson’s disease. Acta Neurol. Scand. 2018, 137, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Klatt, B.N.; Sparto, P.J.; Terhorst, L.; Winser, S.; Heyman, R.; Whitney, S.L. Relationship between subjective visual vertical and balance in individuals with multiple sclerosis. Physiother. Res. Int. 2019, 24, e1757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogawa, Y.; Otsuka, K.; Shimizu, S.; Inagaki, T.; Kondo, T.; Suzuki, M. Subjective visual vertical perception in patients with vestibular neuritis and sudden sensorineural hearing loss. J. Vestib. Res. 2012, 22, 205–211. [Google Scholar] [CrossRef]
- Nair, M.A.; Mulavara, A.P.; Bloomberg, J.J.; Sangi-Haghpeykar, H.; Cohen, H.S. Visual dependence and spatial orientation in benign paroxysmal positional vertigo. J. Vestib. Res. 2018, 27, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Goto, F.; Kobayashi, H.; Saito, A.; Hayashi, Y.; Higashino, K.; Kunihiro, T.; Kanzaki, J. Compensatory changes in static and dynamic subjective visual vertical in patients following vestibular schwanoma surgery. Auris Nasus Larynx 2003, 30, 29–33. [Google Scholar] [CrossRef]
- Pinar, H.S.; Ardic, F.N.; Topuz, B.; Kara, C.O. Subjective visual vertical and subjective visual horizontal measures in patients with chronic dizziness. J. Otolaryngol. 2005, 34, 121–125. [Google Scholar] [CrossRef]
- Razzak, R.A.; Bagust, J.; Docherty, S.; Hussein, W.; Al-Otaibi, A. Augmented asymmetrical visual field dependence in asymptomatic diabetics: Evidence of subclinical asymmetrical bilateral vestibular dysfunction. J. Diabetes Complicat. 2015, 29, 68–72. [Google Scholar] [CrossRef]
- Mittelstaedt, H. The role of the otoliths in perception of the vertical and in path integration. Ann. N. Y. Acad. Sci. 1999, 871, 334–344. [Google Scholar] [CrossRef]
- Barra, J.; Perennou, D. Is the sense of verticality vestibular? Neurophysiol. Clin. 2013, 43, 197–204. [Google Scholar] [CrossRef]
- Mori, L.; Putzolu, M.; Bonassi, G.; Galeoto, G.; Mezzarobba, S.; Trompetto, C.; Avanzino, L.; Marchese, R.; Abbruzzese, G.; Pelosin, E. Haptic perception of verticality correlates with postural and balance deficits in patients with Parkinson’s disease. Parkinsonism Relat. Disord. 2019, 66, 45–50. [Google Scholar] [CrossRef]
- Panic, H.; Panic, A.S.; DiZio, P.; Lackner, J.R. Direction of balance and perception of the upright are perceptually dissociable. J. Neurophysiol. 2015, 113, 3600–3609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vacherot, F.; Vaugoyeau, M.; Mallau, S.; Soulayrol, S.; Assaiante, C.; Azulay, J.P. Postural control and sensory integration in cervical dystonia. Clin. Neurophysiol. 2007, 118, 1019–1027. [Google Scholar] [CrossRef]
- Karlberg, M.; Johansson, R.; Magnusson, M.; Fransson, P.A. Dizziness of suspected cervical origin distinguished by posturographic assessment of human postural dynamics. J. Vestib. Res. 1996, 6, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Chetana, N.; Jayesh, R. Subjective Visual Vertical in Various Vestibular Disorders by Using a Simple Bucket Test. Indian J. Otolaryngol. Head Neck Surg. 2015, 67, 180–184. [Google Scholar] [CrossRef] [Green Version]
- Kristjansson, E.; Treleaven, J. Sensorimotor function and dizziness in neck pain: Implications for assessment and management. J. Orthop. Sports Phys. Ther. 2009, 39, 364–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Della Casa, E.; Affolter Helbling, J.; Meichtry, A.; Luomajoki, H.; Kool, J. Head-eye movement control tests in patients with chronic neck pain; inter-observer reliability and discriminative validity. BMC Musculoskelet. Disord. 2014, 15, 16. [Google Scholar] [CrossRef] [Green Version]
- Bove, M.; Courtine, G.; Schieppati, M. Neck muscle vibration and spatial orientation during stepping in place in humans. J. Neurophysiol. 2002, 88, 2232–2241. [Google Scholar] [CrossRef]
- Gosselin, G.; Rassoulian, H.; Brown, I. Effects of neck extensor muscles fatigue on balance. Clin. Biomech. (Bristol, Avon) 2004, 19, 473–479. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Gonzalez, M.C.; Perez-Cabezas, V.; Lopez-Izquierdo, I.; Gutierrez-Sanchez, E.; Ruiz-Molinero, C.; Rebollo-Salas, M.; Jimenez-Rejano, J.J. Is it possible to relate accommodative visual dysfunctions to neck pain? Ann. N. Y. Acad. Sci. 2018, 1421, 62–72. [Google Scholar] [CrossRef]
- Lambert, F.M.; Malinvaud, D.; Glaunes, J.; Bergot, C.; Straka, H.; Vidal, P.-P. Vestibular asymmetry as the cause of idiopathic scoliosis: A possible answer from Xenopus. J. Neurosci. 2009, 29, 12477–12483. [Google Scholar] [CrossRef] [Green Version]
- Lambert, F.M.; Malinvaud, D.; Gratacap, M.; Straka, H.; Vidal, P.-P. Restricted neural plasticity in vestibulospinal pathways after unilateral labyrinthectomy as the origin for scoliotic deformations. J. Neurosci. 2013, 33, 6845–6856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suwa, H.; Gilland, E.; Baker, R. Otolith ocular reflex function of the tangential nucleus in teleost fish. Ann. N. Y. Acad. Sci. 1999, 871, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Shao, M.; Hirsch, J.C.; Peusner, K.D. Maturation of firing pattern in chick vestibular nucleus neurons. Neuroscience 2006, 141, 711–726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, S.; Gao, X.; Londono, D.; Devroy, S.E.; Mauldin, K.N.; Frankel, J.T.; Brandon, J.M.; Zhang, D.; Li, Q.-Z.; Dobbs, M.B.; et al. Genome-wide association studies of adolescent idiopathic scoliosis suggest candidate susceptibility genes. Hum. Mol. Genet. 2011, 20, 1456–1466. [Google Scholar] [CrossRef]
- Zhou, S.; Zhu, Z.; Qiu, X.; Wu, W.; Wang, W.; Liu, Z.; Lv, F.; Qiu, Y. Association study of IL-17RC, CHL1, DSCAM and CNTNAP2 genes polymorphisms with adolescent idiopathic scoliosis susceptibility in a Chinese Han population. Stud. Health Technol. Inform. 2012, 176, 47–51. [Google Scholar]
- Brunner, D.; Kabitzke, P.; He, D.; Cox, K.; Thiede, L.; Hanania, T.; Sabath, E.; Alexandrov, V.; Saxe, M.; Peles, E.; et al. Comprehensive Analysis of the 16p11.2 Deletion and Null Cntnap2 Mouse Models of Autism Spectrum Disorder. PLoS ONE 2015, 10, e0134572. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Databases | Bibliographic Search Strategy |
|---|---|
| MEDLINE PubMed | (sensory integration (tiab) OR vertical perception (tiab) OR vertical sense (tiab) OR subjective visual vertical (tiab) OR subjective visual vertical test (tiab) OR subjective visual vertical perception (tiab) OR “rod and frame” (tiab)) and (spine (mh) OR spine (tiab) OR musculoskeletal disease (mh) OR musculoskeletal diseases (tiab) OR spinal diseases (mh) OR spinal diseases (tiab) OR spinal curvatures (mh) OR spinal curvatures (tiab) OR neck pain (mh) OR neck pain (tiab) OR neck injuries (mh) OR neck injuries (tiab) OR scoliosis (mh) OR scoliosis (tiab) OR adolescent idiopathic scoliosis (tiab) OR low back pain (mh) OR low back pain (tiab) |
| Scopus | (TITLE-ABS-KEY ((“subjective visual vertical” OR “perception of verticality” OR “visual verticality” OR “verticality sense” OR “rod and frame”)) AND TITLE-ABS-KEY ((“spinal pain” OR “spinal diseases” OR “musculoskeletal disorders” OR “neck pain” OR “neck injuries” OR “idiopathic scoliosis” OR “low back pain”))) |
| Web of Science | TOPIC:((*subjective visual vertical* OR *perception of verticality* OR *visual verticality* OR *rod and frame*)) AND TOPIC: ((*spinal pain* OR *spinal diseases* OR *musculoskeletal disorders* OR *neck pain* OR *neck injuries* OR *idiopathic scoliosis* OR *low back pain*)) |
| SciELO | (subjective visual vertical or verticality perception or verticality or verticality sense) |
| CINAHL | (AB perception of verticality OR AB verticality sense OR AB subjective visual vertical OR AB visual vertical OR AB “rod and frame”) AND (AB musculoskeletal diseases OR AB neck pain OR AB idiopathic scoliosis OR AB low back pain) |
| Study____________________ | Exposed Group | Control Group | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Author and Year | Design | VV Measure | N | Nexp | Age (mean) | Gender (M/F) | Pathology | Onset | Nc | Age (mean) | Gender (M/F) |
| Alrwaily et al. 2020 [57] | CC | SVV/ RFT | 64 | 39 | 42.4 | 14/27 | LBP | C | 25 | 34 | 8/17 |
| Anastasopoulos et al. 1997 [58] | CC | SVV | 58 | 29 | 50.2 | NR | NP | C | 29 | 45.5 | NR |
| Bagust et al. 2005 [64] | CC | RFT | 88 | 71 | 38.97 | 24/47 | NP | C/A | 17 | 33.6 | 7/10 |
| Cakrt et al. 2011 [65] | CC | SVV | 46 | 23 | 14.5 | 5/18 | IS | C | 23 | 14 | 5/18 |
| Catanzariti et al. 2015 [66] | CC | SVV | 40 | 35 | 14.2 | 4/31 | NP | C | 5 | 14.9 | 5/0 |
| Cheung et al. 2002 [67] | CH | SVV | 129 | 89 | 15 | 15/74 | IS | C | 40 | 12 | 8/32 |
| De Pauw et al. 2017 [68] | CC | SVV | 54 | 24 | 59.2 | 4/20 | NP | C | 30 | 59.4 | 12/18 |
| De Zoete et al. 2020 [69] | CC | RFT | 100 | 50 | 35.5 | 20/30 | NP | C | 50 | NR | 23/27 |
| Docherty et al. 2012 [70] | CC | SVV/ RFT | 100 | 50 | 48.1 | 10/40 | NP | C | 50 | 47.9 | 10/40 |
| Grod et al. 2002 [71] | CH | SVV/ RFT | 36 | 19 | 38.5 | 8/11 | NP | A | 17 | 38.6 | 10/7 |
| Hiengkaew et al. 2014 [59] | CC | RFT | 28 | 14 | 44,4 | 3/11 | NP | C | 14 | 43,6 | 7/7 |
| Le Berre et al. 2019 [60] | CC | SVV | 60 | 30 | 14.2 | 30/0 | IS | C | 30 | 13.9 | 30/0 |
| Platho-Elwischger et al. 2017 [61] | CC | SVV | 43 | 30 | 59 | 11/19 | NP | C | 13 | 52,8 | 4/9 |
| Treleaven et al. 2015 [62] | CC | RFT | 126 | 78 | 33,5 | 31/47 | NP | C | 48 | 29,4 | 13/35 |
| Uthaikhup et al. 2012 [63] | CC | RFT | 40 | 20 | 73,2 | 6/14 | NP | C | 20 | 69,5 | 8/12 |
| Study | S1 | S2 | S3 | S4 | C1 | E1 | E2 | E3 | Total |
|---|---|---|---|---|---|---|---|---|---|
| Alrwaily et al. 2020 [57] | - | * | * | * | ** | - | * | - | 6 |
| Anastasopoulos et al. 1997 [58] | - | - | - | - | * | - | - | - | 1 |
| Bagust et al. 2005 [64] | - | - | * | * | ** | - | * | * | 6 |
| Cakrt et al. 2011 [65] | * | - | * | * | ** | * | - | - | 6 |
| Catanzariti et al. 2015 [66] | - | - | - | - | - | - | - | * | 1 |
| Cheung et al. 2002 [67] | - | * | * | * | * | - | - | - | 4 |
| De Pauw et al. 2017 [68] | - | - | - | * | * | * | - | - | 3 |
| De Zoete et al. 2020 [69] | - | - | * | * | * | - | * | - | 4 |
| Docherty et al. 2012 [70] | - | - | * | * | ** | - | - | * | 5 |
| Grod et al. 2002 [71] | - | - | - | - | * | - | - | - | 1 |
| Hiengkaew et al. 2014 [59] | - | - | * | * | ** | - | - | * | 5 |
| Le Berre et al. 2019 [60] | - | * | - | * | * | - | * | * | 5 |
| Platho-Elwischger et al. 2017 [61] | - | * | * | * | ** | - | - | * | 6 |
| Treleaven et al. 2015 [62] | - | - | - | * | * | - | - | * | 3 |
| Uthaikhup et al. 2012 [63] | - | - | * | * | - | - | * | - | 3 |
| Effect Size | Publication Bias | Heterogeneity | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Group | K | N | Ns | SMD | 95% CI | p-Value | Funnel Plot | Trim and Fill | q-Value | I2 | |
| Adjusted SMD | % of Change | ||||||||||
| SVV in spinal pain patients | 8 | 459 | 57.37 | 0.191 | −0.040; 0.386 | 0.054 | Asym. | 0.150 | 22% | 3.857 | 0% |
| RFT in spinal pain patients | 19 | 1308 | 68.84 | 0.339 | 0.181; 0.497 | 0.000 | Asym. | 0.248 | 28% | 16.124 | 0% |
| SVV in IS patients | 4 | 325 | 81.25 | 0.314 | −0.273; 0.901 | 0.294 | Sym. | 0.314 | 0% | 3.061 | 2% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Obrero-Gaitán, E.; Molina, F.; Del-Pino-Casado, R.; Ibáñez-Vera, A.J.; Rodríguez-Almagro, D.; Lomas-Vega, R. Visual Verticality Perception in Spinal Diseases: A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 1725. https://doi.org/10.3390/jcm9061725
Obrero-Gaitán E, Molina F, Del-Pino-Casado R, Ibáñez-Vera AJ, Rodríguez-Almagro D, Lomas-Vega R. Visual Verticality Perception in Spinal Diseases: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2020; 9(6):1725. https://doi.org/10.3390/jcm9061725
Chicago/Turabian StyleObrero-Gaitán, Esteban, Francisco Molina, Rafael Del-Pino-Casado, Alfonso Javier Ibáñez-Vera, Daniel Rodríguez-Almagro, and Rafael Lomas-Vega. 2020. "Visual Verticality Perception in Spinal Diseases: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 9, no. 6: 1725. https://doi.org/10.3390/jcm9061725