Non-Invasive Assessment of Breast Cancer Molecular Subtypes with Multiparametric Magnetic Resonance Imaging Radiomics

 ,
,  and
and 
Abstract
:1. Introduction
2. Material and Methods
2.1. Patients
2.2. MR Imaging
2.3. Radiomics Analysis
2.4. Statistical Analysis
2.5. Histopathological Analysis
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cortazar, P.; Zhang, L.; Untch, M.; Mehta, K.; Costantino, J.P.; Wolmark, N.; Bonnefoi, H.; Cameron, D.; Gianni, L.; Valagussa, P.; et al. Pathological complete response and long-term clinical benefit in breast cancer: The ctneobc pooled analysis. Lancet 2014, 384, 164–172. [Google Scholar] [CrossRef] [Green Version]
- Curigliano, G.; Burstein, H.J.; Winer, E.P.; Gnant, M.; Dubsky, P.; Loibl, S.; Colleoni, M.; Regan, M.M.; Piccart-Gebhart, M.; Senn, H.J.; et al. De-escalating and escalating treatments for early-stage breast cancer: The st. Gallen international expert consensus conference on the primary therapy of early breast cancer 2017. Ann. Oncol. Off. J. Eur. Soc. Med Oncol. 2017, 28, 1700–1712. [Google Scholar] [CrossRef] [PubMed]
- Goldhirsch, A.; Winer, E.P.; Coates, A.S.; Gelber, R.D.; Piccart-Gebhart, M.; Thurlimann, B.; Senn, H.J. Personalizing the treatment of women with early breast cancer: Highlights of the st gallen international expert consensus on the primary therapy of early breast cancer 2013. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2013, 24, 2206–2223. [Google Scholar] [CrossRef] [PubMed]
- Waks, A.G.; Winer, E.P. Breast cancer treatment: A review. JAMA 2019, 321, 288–300. [Google Scholar] [CrossRef] [PubMed]
- Comprehensive molecular portraits of human breast tumours. Nature 2012, 490, 61–70. [CrossRef] [PubMed] [Green Version]
- Prat, A.; Perou, C.M. Deconstructing the molecular portraits of breast cancer. Mol. Oncol. 2011, 5, 5–23. [Google Scholar] [CrossRef] [PubMed]
- Zardavas, D.; Irrthum, A.; Swanton, C.; Piccart, M. Clinical management of breast cancer heterogeneity. Nat. Rev. Clin. Oncol. 2015, 12, 381–394. [Google Scholar] [CrossRef]
- Mann, G.B.; Fahey, V.D.; Feleppa, F.; Buchanan, M.R. Reliance on hormone receptor assays of surgical specimens may compromise outcome in patients with breast cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2005, 23, 5148–5154. [Google Scholar] [CrossRef]
- Burge, C.N.; Chang, H.R.; Apple, S.K. Do the histologic features and results of breast cancer biomarker studies differ between core biopsy and surgical excision specimens? Breast 2006, 15, 167–172. [Google Scholar] [CrossRef]
- Orlando, L.; Viale, G.; Bria, E.; Lutrino, E.S.; Sperduti, I.; Carbognin, L.; Schiavone, P.; Quaranta, A.; Fedele, P.; Caliolo, C.; et al. Discordance in pathology report after central pathology review: Implications for breast cancer adjuvant treatment. Breast 2016, 30, 151–155. [Google Scholar] [CrossRef]
- Pisco, A.O.; Huang, S. Non-genetic cancer cell plasticity and therapy-induced stemness in tumour relapse: ‘What does not kill me strengthens me’. Br. J. Cancer 2015, 112, 1725–1732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, H.; Zhu, Y.; Burnside, E.S.; Huang, E.; Drukker, K.; Hoadley, K.A.; Fan, C.; Conzen, S.D.; Zuley, M.; Net, J.M.; et al. Quantitative mri radiomics in the prediction of molecular classifications of breast cancer subtypes in the tcga/tcia data set. NPJ Breast Cancer 2016, 2, 16012. [Google Scholar] [CrossRef] [PubMed]
- Grimm, L.J.; Zhang, J.; Mazurowski, M.A. Computational approach to radiogenomics of breast cancer: Luminal a and luminal b molecular subtypes are associated with imaging features on routine breast mri extracted using computer vision algorithms. J. Magn. Reson. Imaging JMRI 2015, 42, 902–907. [Google Scholar] [CrossRef] [PubMed]
- Waugh, S.A.; Purdie, C.A.; Jordan, L.B.; Vinnicombe, S.; Lerski, R.A.; Martin, P.; Thompson, A.M. Magnetic resonance imaging texture analysis classification of primary breast cancer. Eur. Radiol. 2016, 26, 322–330. [Google Scholar] [CrossRef]
- Baltzer, P.; Mann, R.M.; Iima, M.; Sigmund, E.E.; Clauser, P.; Gilbert, F.J.; Martincich, L.; Partridge, S.C.; Patterson, A.; Pinker, K.; et al. Diffusion-weighted imaging of the breast-a consensus and mission statement from the eusobi international breast diffusion-weighted imaging working group. Eur. Radiol. 2020, 30, 1436–1450. [Google Scholar] [CrossRef] [Green Version]
- Parekh, V.S.; Jacobs, M.A. Integrated radiomic framework for breast cancer and tumor biology using advanced machine learning and multiparametric mri. NPJ Breast Cancer 2017, 3, 43. [Google Scholar] [CrossRef] [Green Version]
- Bickelhaupt, S.; Paech, D.; Kickingereder, P.; Steudle, F.; Lederer, W.; Daniel, H.; Gotz, M.; Gahlert, N.; Tichy, D.; Wiesenfarth, M.; et al. Prediction of malignancy by a radiomic signature from contrast agent-free diffusion mri in suspicious breast lesions found on screening mammography. J. Magn. Reson. Imaging JMRI 2017, 46, 604–616. [Google Scholar] [CrossRef]
- Sun, X.; He, B.; Luo, X.; Li, Y.; Cao, J.; Wang, J.; Dong, J.; Sun, X.; Zhang, G. Preliminary study on molecular subtypes of breast cancer based on magnetic resonance imaging texture analysis. J. Comput. Assist. Tomogr. 2018, 42, 531–535. [Google Scholar] [CrossRef]
- Xie, T.; Zhao, Q.; Fu, C.; Bai, Q.; Zhou, X.; Li, L.; Grimm, R.; Liu, L.; Gu, Y.; Peng, W. Differentiation of triple-negative breast cancer from other subtypes through whole-tumor histogram analysis on multiparametric mr imaging. Eur. Radiol. 2019, 29, 2535–2544. [Google Scholar] [CrossRef]
- Collewet, G.; Strzelecki, M.; Mariette, F. Influence of mri acquisition protocols and image intensity normalization methods on texture classification. Magn. Reson. Imaging 2004, 22, 81–91. [Google Scholar] [CrossRef]
- Benoit-Cattin, H. Texture Analysis for Magnetic Resonance Imaging; Med4 Publishing s.r.o.: Prague, Czech Republic, 2006. [Google Scholar]
- Hon, J.D.; Singh, B.; Sahin, A.; Du, G.; Wang, J.; Wang, V.Y.; Deng, F.M.; Zhang, D.Y.; Monaco, M.E.; Lee, P. Breast cancer molecular subtypes: From tnbc to qnbc. Am. J. Cancer Res. 2016, 6, 1864–1872. [Google Scholar] [PubMed]
- Gibbs, P.; Onishi, N.; Sadinski, M.; Gallagher, K.M.; Hughes, M.; Martinez, D.F.; Morris, E.A.; Sutton, E.J. Characterization of sub-1 cm breast lesions using radiomics analysis. J. Magn. Reson. Imaging JMRI 2019, 50, 1468–1477. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Zhang, Y.; Chang, K.T.; Lee, K.E.; Wang, O.; Li, J.; Lin, Y.; Pan, Z.; Chang, P.; Chow, D.; et al. Diagnosis of benign and malignant breast lesions on dce-mri by using radiomics and deep learning with consideration of peritumor tissue. J. Magn. Reson. Imaging JMRI 2020, 51, 798–809. [Google Scholar] [CrossRef] [PubMed]
- Aghaei, F.; Tan, M.; Hollingsworth, A.B.; Zheng, B. Applying a new quantitative global breast mri feature analysis scheme to assess tumor response to chemotherapy. J. Magn. Reson. Imaging JMRI 2016, 44, 1099–1106. [Google Scholar] [CrossRef] [Green Version]
- Mazurowski, M.A.; Zhang, J.; Grimm, L.J.; Yoon, S.C.; Silber, J.I. Radiogenomic analysis of breast cancer: Luminal b molecular subtype is associated with enhancement dynamics at mr imaging. Radiology 2014, 273, 365–372. [Google Scholar] [CrossRef]
- Sutton, E.J.; Dashevsky, B.Z.; Oh, J.H.; Veeraraghavan, H.; Apte, A.P.; Thakur, S.B.; Morris, E.A.; Deasy, J.O. Breast cancer molecular subtype classifier that incorporates mri features. J. Magn. Reson. Imaging JMRI 2016, 44, 122–129. [Google Scholar] [CrossRef] [Green Version]
- Holli-Helenius, K.; Salminen, A.; Rinta-Kiikka, I.; Koskivuo, I.; Bruck, N.; Bostrom, P.; Parkkola, R. Mri texture analysis in differentiating luminal a and luminal b breast cancer molecular subtypes—A feasibility study. BMC Med. Imaging 2017, 17, 69. [Google Scholar] [CrossRef] [Green Version]
- Runge, V.M. Critical questions regarding gadolinium deposition in the brain and body after injections of the gadolinium-based contrast agents, safety, and clinical recommendations in consideration of the ema’s pharmacovigilance and risk assessment committee recommendation for suspension of the marketing authorizations for 4 linear agents. Investig. Radiol. 2017, 52, 317–323. [Google Scholar]
- Gulani, V.; Calamante, F.; Shellock, F.G.; Kanal, E.; Reeder, S.B. Gadolinium deposition in the brain: Summary of evidence and recommendations. Lancet. Neurol. 2017, 16, 564–570. [Google Scholar] [CrossRef]
- Leithner, D.; Bernard-Davila, B.; Martinez, D.F.; Horvat, J.V.; Jochelson, M.S.; Marino, M.A.; Avendano, D.; Ochoa-Albiztegui, R.E.; Sutton, E.J.; Morris, E.A.; et al. Radiomic signatures derived from diffusion-weighted imaging for the assessment of breast cancer receptor status and molecular subtypes. Mol. Imaging Biol. 2020, 22, 453–461. [Google Scholar] [CrossRef] [Green Version]
- Kato, F.; Kudo, K.; Yamashita, H.; Wang, J.; Hosoda, M.; Hatanaka, K.C.; Mimura, R.; Oyama-Manabe, N.; Shirato, H. Differences in morphological features and minimum apparent diffusion coefficient values among breast cancer subtypes using 3-tesla mri. Eur. J. Radiol. 2016, 85, 96–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Youk, J.H.; Son, E.J.; Chung, J.; Kim, J.A.; Kim, E.K. Triple-negative invasive breast cancer on dynamic contrast-enhanced and diffusion-weighted mr imaging: Comparison with other breast cancer subtypes. Eur. Radiol. 2012, 22, 1724–1734. [Google Scholar] [CrossRef] [PubMed]
- Yun, J.; Park, J.E.; Lee, H.; Ham, S.; Kim, N.; Kim, H.S. Radiomic features and multilayer perceptron network classifier: A robust mri classification strategy for distinguishing glioblastoma from primary central nervous system lymphoma. Sci. Rep. 2019, 9, 5746. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Training Accuracy Median (Range) % | Test Accuracy Median (Range) % | AUC Median (Range) % | |
|---|---|---|---|
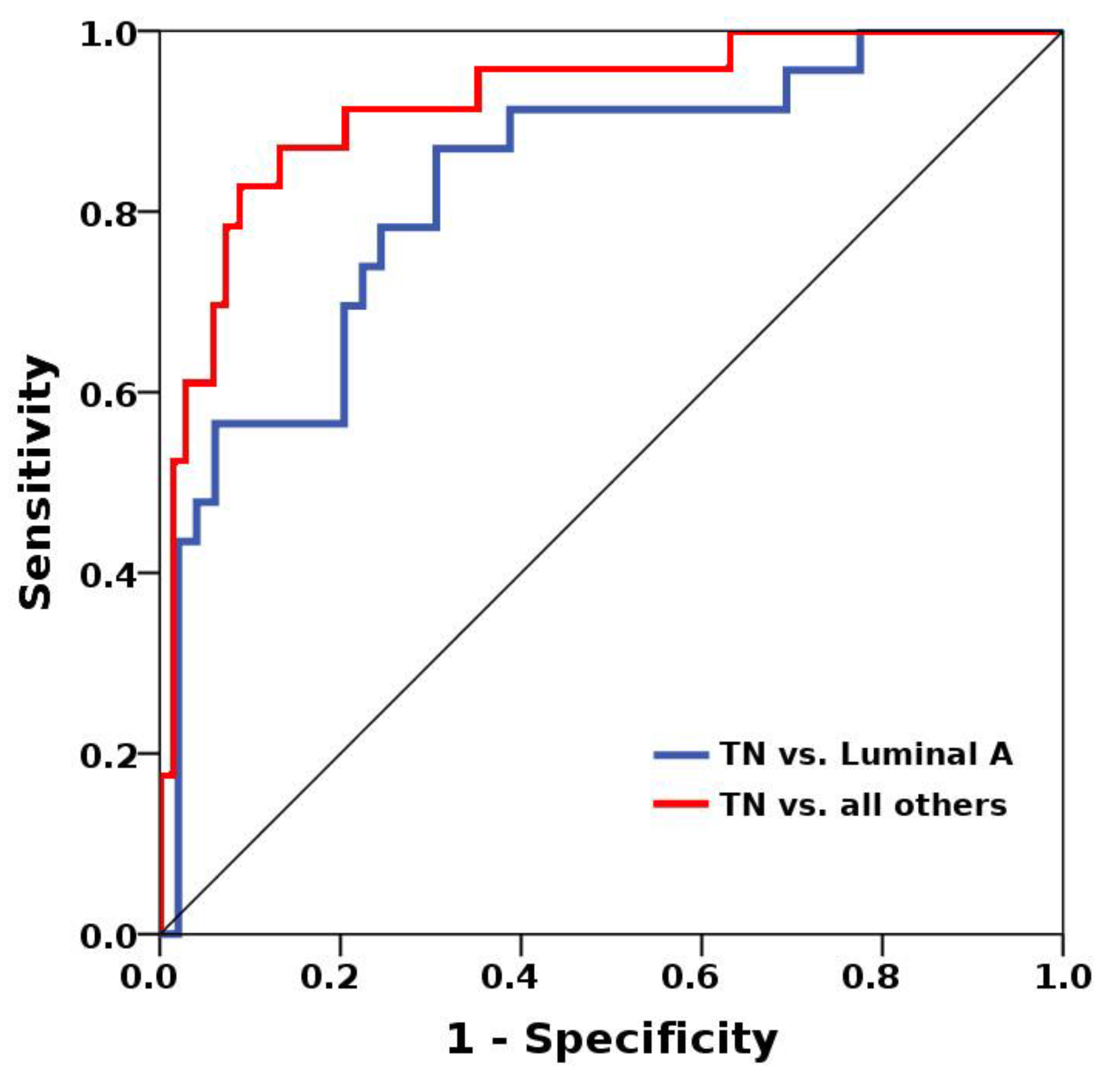
| Luminal A vs. TN | 74 (70–86) | 68.2 (63.6–81.8) | 0.8 (0.75–0.83) |
| Luminal A vs. all others | 65.6 (62.5–78.6) | 66.7 (59.3–74.1) | 0.72 (0.7–0.74) |
| TN vs. all others | 85.9 (78.1–91.3) | 85.2 (85.2–90.9) | 0.86 (0.77–0.92) |
| HR+ vs. HR− | 64.7 (63.2–80.9) | 60 (52.2–82.6) | 0.69 (0.63–0.89) |
| TN vs. All Others | Luminal A vs. TN | |
|---|---|---|
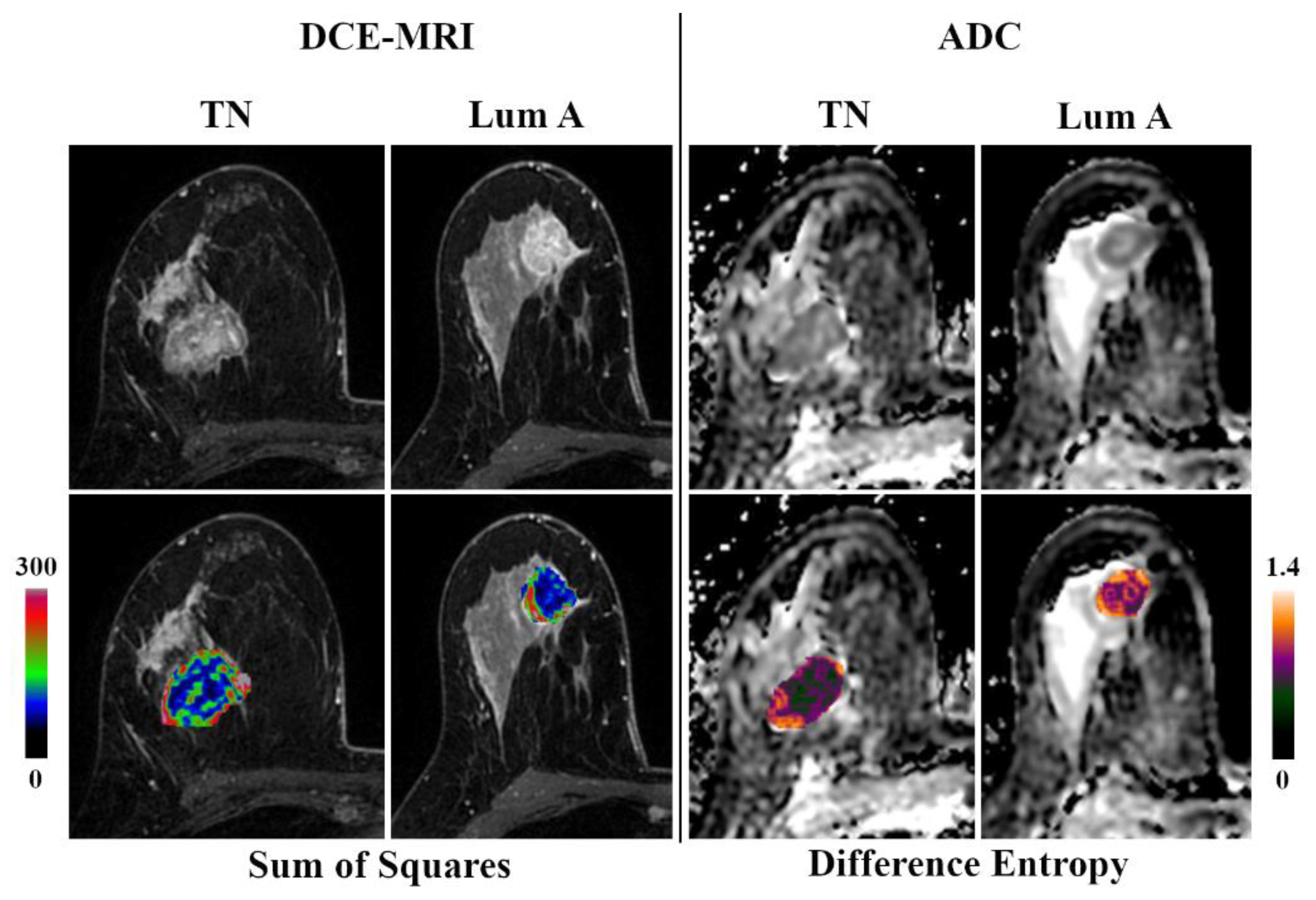
| DCE-MRI | Sum of squares | Sum of squares |
| Vertical coordinate of gravity centre | Theta 2 | |
| Vertical second order moment of inertia | GeoFmax/GeoFmin | |
| Theta 2 | Danielsson ratio | |
| Histogram’s variance | Histogram’s variance | |
| ADC map | Difference entropy | Sum of squares |
| Sum average | Difference variance | |
| Absolute gradient skewness | Theta 2 | |
| Difference variance | Difference variance | |
| Sum of squares | Histogram’s skewness |
| HER2 Negative | Luminal A | Luminal B | HER2-Enriched | TN | All Others | |
|---|---|---|---|---|---|---|
| HER2 positive | 67.7% | - | - | - | - | 67.7% |
| Luminal A | - | - | 52.6% | 56.7% | - | - |
| Luminal B | - | 52.6% | - | 57.9% | 38.7% | 58.2% |
| HER2-enriched | - | 56.7% | 57.9% | - | 70.3% | 54.9% |
| TN | - | - | 38.7% | 70.3% | - | - |
| All others | 67.7% | - | 58.2% | 54.9% | - | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leithner, D.; Mayerhoefer, M.E.; Martinez, D.F.; Jochelson, M.S.; Morris, E.A.; Thakur, S.B.; Pinker, K. Non-Invasive Assessment of Breast Cancer Molecular Subtypes with Multiparametric Magnetic Resonance Imaging Radiomics. J. Clin. Med. 2020, 9, 1853. https://doi.org/10.3390/jcm9061853
Leithner D, Mayerhoefer ME, Martinez DF, Jochelson MS, Morris EA, Thakur SB, Pinker K. Non-Invasive Assessment of Breast Cancer Molecular Subtypes with Multiparametric Magnetic Resonance Imaging Radiomics. Journal of Clinical Medicine. 2020; 9(6):1853. https://doi.org/10.3390/jcm9061853
Chicago/Turabian StyleLeithner, Doris, Marius E. Mayerhoefer, Danny F. Martinez, Maxine S. Jochelson, Elizabeth A. Morris, Sunitha B. Thakur, and Katja Pinker. 2020. "Non-Invasive Assessment of Breast Cancer Molecular Subtypes with Multiparametric Magnetic Resonance Imaging Radiomics" Journal of Clinical Medicine 9, no. 6: 1853. https://doi.org/10.3390/jcm9061853