Cardiac and Respiratory Influences on Intracranial and Neck Venous Flow, Estimated Using Real-Time Phase-Contrast MRI

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. MRI Acquisitions
2.3. MRI Data Processing
2.4. Signal Analysis
2.5. Statistical Analysis
3. Results
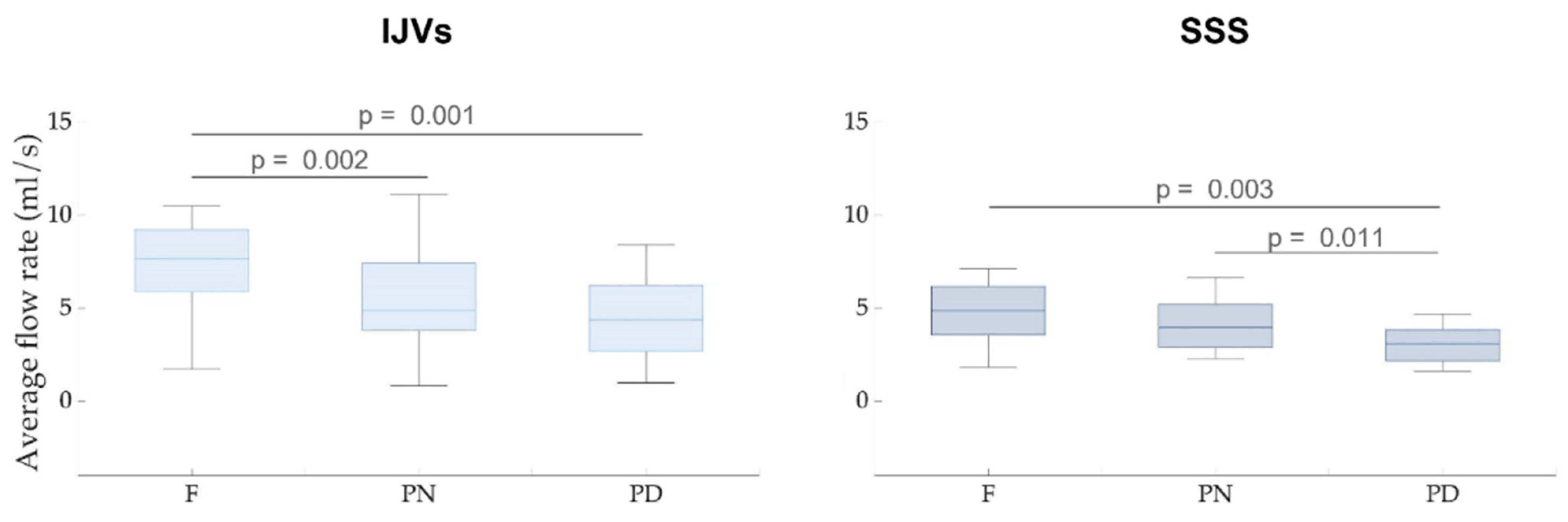
3.1. Average Flow Rate and Cross-Sectional Area: Changes with Types of Breathing (Aim 1)
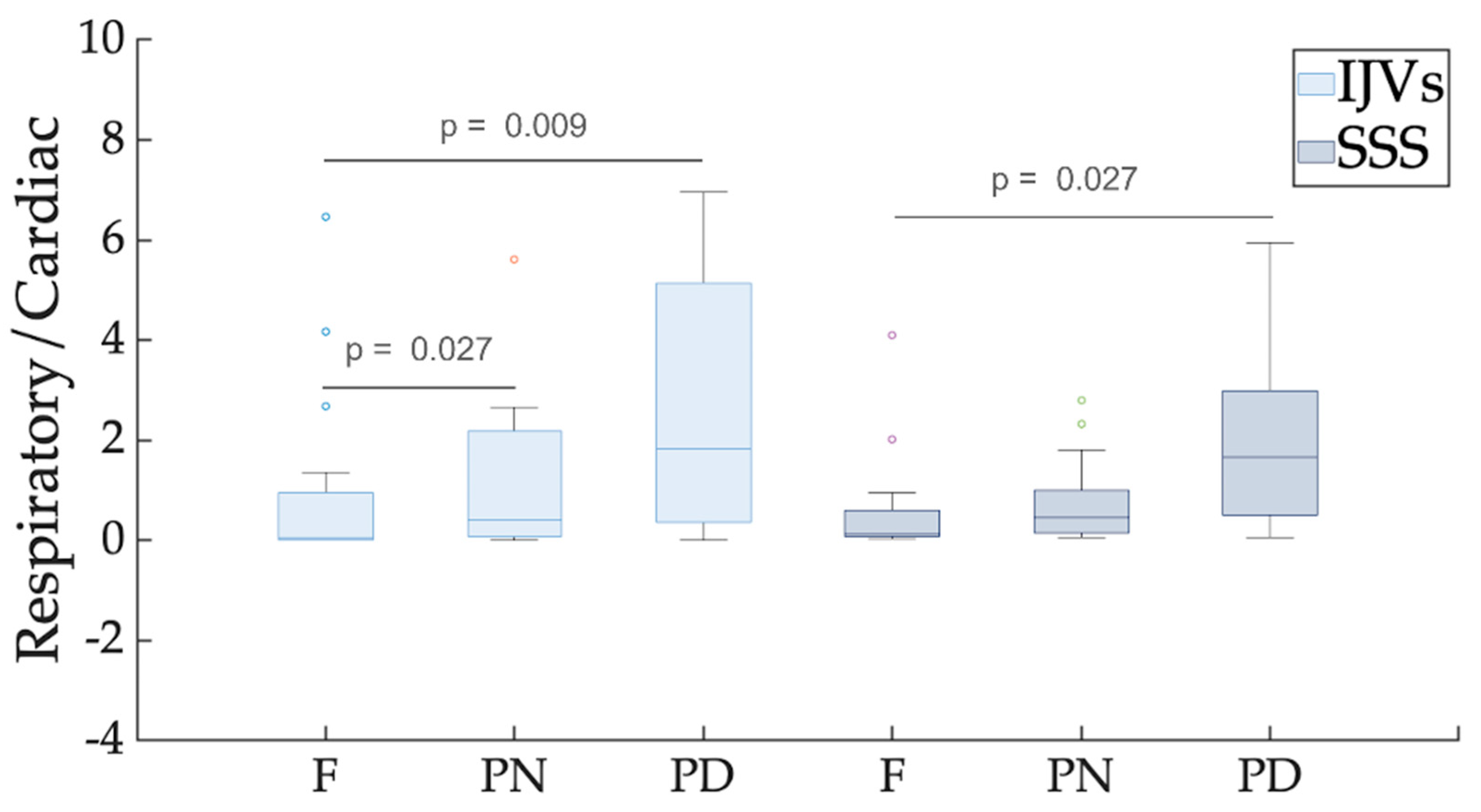
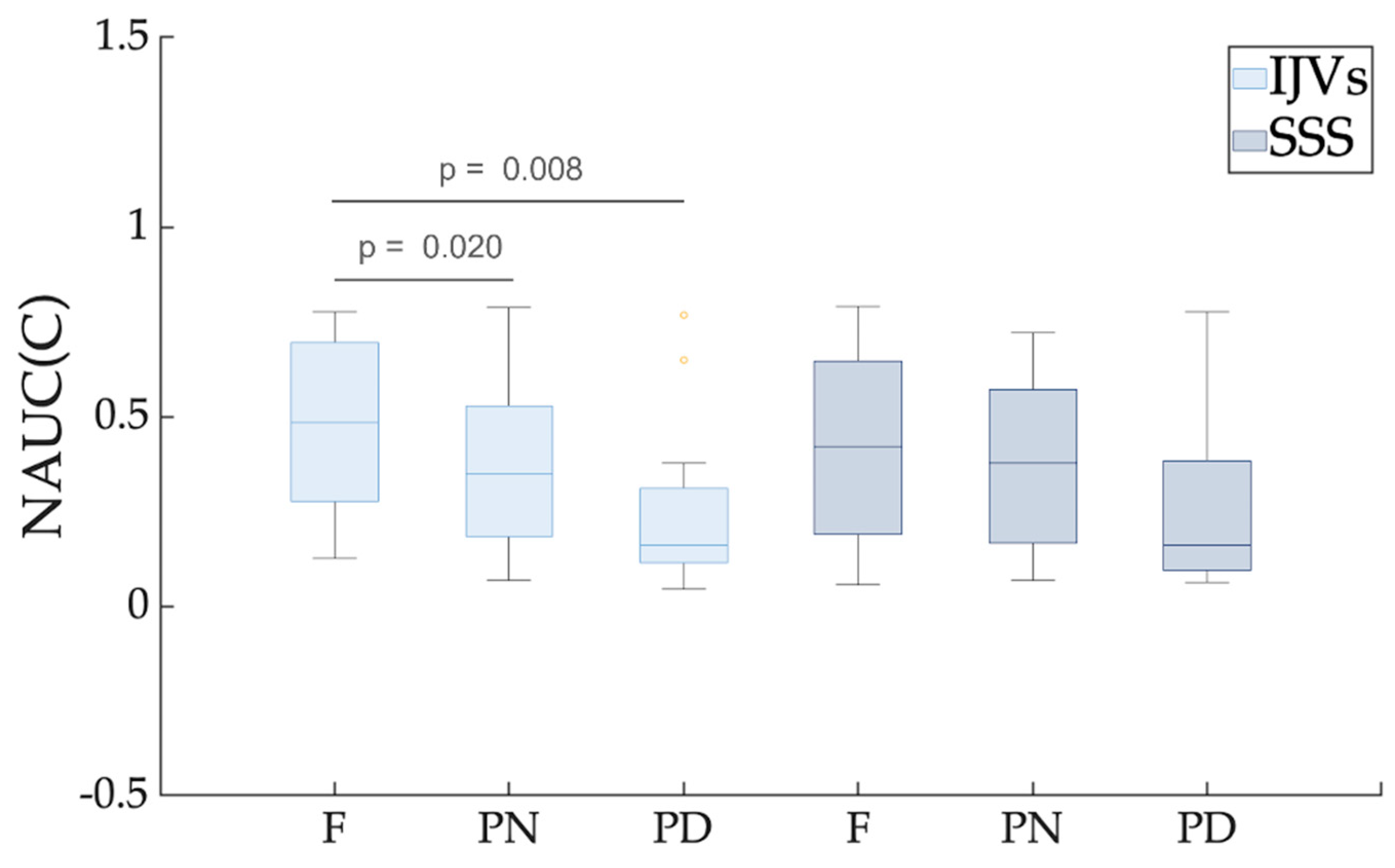
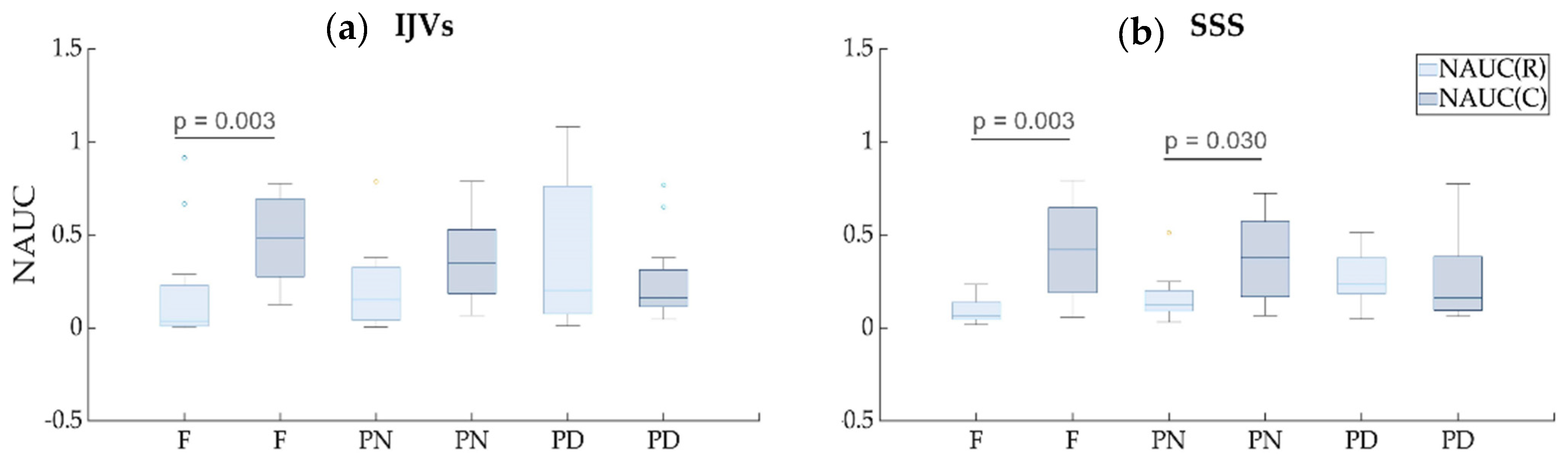
3.2. Respiratory and Cardiac Flow Rate Modulations (Aim 2)
4. Discussion
4.1. Free Compared to Forced Breathing: Flow Rate Decrement
4.2. Free Breathing Compared to Forced Breathing: Flow Rate Decrement and Respiratory Modulation Increment
4.3. Limitations
4.4. Clinical Applications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brecher, G.A.; Hubay, C.A. Pulmonary blood flow and venous return during spontaneous respiration. Circ. Res. 1955, 3, 210–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zamboni, P.; Menegatti, E.; Pomidori, L.; Morovic, S.; Taibi, A.; Malagoni, A.M.; Cogo, A.L.; Gambaccini, M. Does thoracic pump influence the cerebral venous return? J. Appl. Physiol. 2012, 112, 904–910. [Google Scholar] [CrossRef] [Green Version]
- Lagana, M.M.; Di Rienzo, M.; Rizzo, F.; Ricci, C.; D’Onofrio, S.; Forzoni, L.; Cecconi, P. Cardiac, Respiratory and Postural Influences on Venous Return of Internal Jugular and Vertebral Veins. Ultrasound Med. Biol. 2017, 43, 1195–1204. [Google Scholar] [CrossRef] [PubMed]
- Ohno, N.; Miyati, T.; Noda, T.; Alperin, N.; Hamaguchi, T.; Ohno, M.; Matsushita, T.; Mase, M.; Gabata, T.; Kobayashi, S. Fast Phase-Contrast Cine MRI for Assessing Intracranial Hemodynamics and Cerebrospinal Fluid Dynamics. Diagnostics 2020, 10, 241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kollmeier, J.M.; Gürbüz-Reiss, L.; Sahoo, P.; Badura, S.; Ellebracht, B.; Keck, M.; Gärtner, J.; Ludwig, H.-C.; Frahm, J.; Dreha-Kulaczewski, S. Deep breathing couples CSF and venous flow dynamics. Sci. Rep. 2022, 12, 2568. [Google Scholar] [CrossRef]
- Alperin, N.; Hushek, S.G.; Lee, S.H.; Sivaramakrishnan, A.; Lichtor, T. MRI study of cerebral blood flow and CSF flow dynamics in an upright posture: The effect of posture on the intracranial compliance and pressure. Acta Neurochir. Suppl. 2005, 95, 177–181. [Google Scholar] [CrossRef]
- Muccio, M.; Chu, D.; Minkoff, L.; Kulkarni, N.; Damadian, B.; Damadian, R.V.; Ge, Y. Upright versus supine MRI: Effects of body position on craniocervical CSF flow. Fluids Barriers CNS 2021, 18, 61. [Google Scholar] [CrossRef]
- Greitz, D. Cerebrospinal fluid circulation and associated intracranial dynamics. A radiologic investigation using MR imaging and radionuclide cisternography. Acta Radiol. Suppl. 1993, 386, 1–23. [Google Scholar]
- Tain, R.W.; Alperin, N. Noninvasive intracranial compliance from MRI-based measurements of transcranial blood and CSF flows: Indirect versus direct approach. IEEE Trans. Biomed. Eng. 2009, 56, 544–551. [Google Scholar] [CrossRef]
- Daouk, J.; Bouzerar, R.; Baledent, O. Heart rate and respiration influence on macroscopic blood and CSF flows. Acta Radiol. 2017, 58, 977–982. [Google Scholar] [CrossRef]
- Dreha-Kulaczewski, S.; Joseph, A.A.; Merboldt, K.D.; Ludwig, H.C.; Gartner, J.; Frahm, J. Identification of the Upward Movement of Human CSF In Vivo and its Relation to the Brain Venous System. J. Neurosci. 2017, 37, 2395–2402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beggs, C.B.; Shepherd, S.J.; Cecconi, P.; Lagana, M.M. Predicting the aqueductal cerebrospinal fluid pulse: A statistical approach. Appl. Sci. 2019, 9, 2131. [Google Scholar] [CrossRef] [Green Version]
- Laganà, M.M.; Shepherd, S.J.; Cecconi, P.; Beggs, C.B. Intracranial volumetric changes govern cerebrospinal fluid flow in the Aqueduct of Sylvius in healthy adults. Biomed. Signal Process. Control 2017, 36, 84–92. [Google Scholar] [CrossRef]
- Baselli, G.; Fasani, F.; Pelizzari, L.; Cazzoli, M.; Baglio, F.; Laganà, M.M. Real-Time Phase-Contrast MRI to Monitor Cervical Blood and Cerebrospinal Fluid Flow Beat-by-Beat Variability. Biosensors 2022, 12, 417. [Google Scholar] [CrossRef]
- Sunohara, S.; Yatsushiro, S.; Takizawa, K.; Matsumae, M.; Kajihara, N.; Kuroda, K. Investigation of driving forces of cerebrospinal fluid motion by power and frequency mapping based on asynchronous phase contrast technique. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 1232–1235. [Google Scholar]
- Patchana, T.; Zampella, B.; Berry, J.A.; Lawandy, S.; Sweiss, R.B. Superior sagittal sinus: A review of the history, surgical considerations, and pathology. Cureus 2019, 11, e4597. [Google Scholar] [CrossRef] [Green Version]
- Richard, L.D.; Vogl, A.W.; Mitchell, A.J.P.C.L. Gray’s Atlas of Anatomy; Elsevier Health Sciences: Amsterdam, The Netherlands, 2008. [Google Scholar]
- Letchuman, V.; Donohoe, C. Neuroanatomy, Superior Sagittal Sinus; StatPearls Publishing: Treasure Island, FL, USA, 2019. [Google Scholar]
- Molnár, A.Á.; Nádasy, G.L.; Dörnyei, G.; Patai, B.B.; Delfavero, J.; Fülöp, G.Á.; Kirkpatrick, A.C.; Ungvári, Z.; Merkely, B. The aging venous system: From varicosities to vascular cognitive impairment. Geroscience 2021, 43, 2761–2784. [Google Scholar] [CrossRef]
- Ghali, M.G.Z.; Marchenko, V.; Yaşargil, M.G.; Ghali, G.Z. Structure and function of the perivascular fluid compartment and vertebral venous plexus: Illumining a novel theory on mechanisms underlying the pathogenesis of Alzheimer’s, cerebral small vessel, and neurodegenerative diseases. Neurobiol. Dis. 2020, 144, 105022. [Google Scholar] [CrossRef]
- Laganà, M.M.; Pirastru, A.; Pelizzari, L.; Rossetto, F.; Di Tella, S.; Bergsland, N.; Nemni, R.; Meloni, M.; Baglio, F. Multimodal evaluation of neurovascular functionality in early Parkinson’s disease. Front. Neurol. 2020, 11, 831. [Google Scholar] [CrossRef]
- Pelizzari, L.; Di Tella, S.; Rossetto, F.; Lagana, M.M.; Bergsland, N.; Pirastru, A.; Meloni, M.; Nemni, R.; Baglio, F. Parietal Perfusion Alterations in Parkinson’s Disease Patients Without Dementia. Front. Neurol. 2020, 11, 562. [Google Scholar] [CrossRef]
- Pelizzari, L.; Laganà, M.M.; Rossetto, F.; Bergsland, N.; Galli, M.; Baselli, G.; Clerici, M.; Nemni, R.; Baglio, F. Cerebral blood flow and cerebrovascular reactivity correlate with severity of motor symptoms in Parkinson’s disease. J. Ther. Adv. Neurol. Disord. 2019, 12, 1756286419838354. [Google Scholar] [CrossRef] [Green Version]
- Jakimovski, D.; Topolski, M.; Genovese, A.V.; Weinstock-Guttman, B.; Zivadinov, R. Vascular aspects of multiple sclerosis: Emphasis on perfusion and cardiovascular comorbidities. Expert Rev. Neurother. 2019, 19, 445–458. [Google Scholar] [CrossRef] [PubMed]
- Jakimovski, D.; Zivadinov, R.; Weinstock-Guttman, B.; Bergsland, N.; Dwyer, M.G.; Lagana, M.M. Longitudinal analysis of cerebral aqueduct flow measures: Multiple sclerosis flow changes driven by brain atrophy. Fluids Barriers CNS 2020, 17, 9. [Google Scholar] [CrossRef] [PubMed]
- Laganà, M.M.; Mendozzi, L.; Pelizzari, L.; Bergsland, N.P.; Pugnetti, L.; Cecconi, P.; Baselli, G.; Clerici, M.; Nemni, R.; Baglio, F. Are cerebral perfusion and atrophy linked in multiple sclerosis? Evidence for a multifactorial approach to assess neurodegeneration. Curr. Neurovasc. Res. 2018, 15, 282–291. [Google Scholar] [CrossRef] [PubMed]
- Lagana, M.M.; Pelizzari, L.; Baglio, F. Relationship between MRI perfusion and clinical severity in multiple sclerosis. Neural Regen. Res. 2020, 15, 646–652. [Google Scholar] [CrossRef]
- Jakimovski, D.; Topolski, M.; Kimura, K.; Marr, K.; Gandhi, S.; Ramasamy, D.P.; Bergsland, N.; Hagemeier, J.; Weinstock-Guttman, B.; Zivadinov, R. Abnormal venous postural control: Multiple sclerosis-specific change related to gray matter pathology or age-related neurodegenerative phenomena? Clin. Auton. Res. 2019, 29, 329–338. [Google Scholar] [CrossRef]
- Fulop, G.A.; Tarantini, S.; Yabluchanskiy, A.; Molnar, A.; Prodan, C.I.; Kiss, T.; Csipo, T.; Lipecz, A.; Balasubramanian, P.; Farkas, E.; et al. Role of age-related alterations of the cerebral venous circulation in the pathogenesis of vascular cognitive impairment. Am. J. Physiol.-Heart Circ. Physiol. 2019, 316, H1124–H1140. [Google Scholar] [CrossRef]
- Yildiz, S.; Thyagaraj, S.; Jin, N.; Zhong, X.; Heidari Pahlavian, S.; Martin, B.A.; Loth, F.; Oshinski, J.; Sabra, K.G. Quantifying the influence of respiration and cardiac pulsations on cerebrospinal fluid dynamics using real-time phase-contrast MRI. J. Magn. Reson. Imaging 2017, 46, 431–439. [Google Scholar] [CrossRef]
- Lagana, M.M.; Di Tella, S.; Pelizzari, L.; Cazzoli, M.; Alperin, N.; Jin, N.; Zacà, D.; Baselli, G.; Baglio, F. Blood and cerebrospinal fluid flow oscillations measured with real-time phase-contrast MRI: Breathing mode matters. Res. Sq. 2022. [Google Scholar] [CrossRef]
- Jiang, J.; Kokeny, P.; Ying, W.; Magnano, C.; Zivadinov, R.; Haacke, E.M. Quantifying errors in flow measurement using phase contrast magnetic resonance imaging: Comparison of several boundary detection methods. J. Magn. Reson. Imaging 2015, 33, 185–193. [Google Scholar] [CrossRef] [Green Version]
- Rasmussen, M.K.; Mestre, H.; Nedergaard, M. Fluid transport in the brain. Physiol. Rev. 2022, 102, 1025–1151. [Google Scholar] [CrossRef]
- Conover, W.J. Practical Nonparametric Statistics; John Wiley & Sons: Hoboken, NJ, USA, 1999; Volume 350. [Google Scholar]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B (Methodol.) 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Marr, K.; Jakimovski, D.; Mancini, M.; Carl, E.; Zivadinov, R. Jugular venous flow quantification using doppler sonography. Ultrasound Med. Biol. 2018, 44, 1762–1769. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.; Barnes, S.; Haacke, E.; Grossman, R.; Ge, Y. Imaging the effects of oxygen saturation changes in voluntary apnea and hyperventilation on susceptibility-weighted imaging. Am. J. Neuroradiol. 2014, 35, 1091–1095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magnano, C.; Belov, P.; Krawiecki, J.; Hagemeier, J.; Beggs, C.; Zivadinov, R. Internal jugular vein cross-sectional area enlargement is associated with aging in healthy individuals. PLoS ONE 2016, 11, e0149532. [Google Scholar] [CrossRef] [PubMed]
- Selim, M.; Jones, R.; Novak, P.; Zhao, P.; Novak, V. The effects of body mass index on cerebral blood flow velocity. Clin. Auton. Res. 2008, 18, 331–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vlajinac, H.; Marinkovic, J.; Maksimovic, M.; Matic, P.; Radak, D. Body mass index and primary chronic venous disease—A cross-sectional study. Eur. J. Vasc. Endovasc. Surg. 2013, 45, 293–298. [Google Scholar] [CrossRef] [Green Version]
- Magnano, C.; Belov, P.; Krawiecki, J.; Hagemeier, J.; Zivadinov, R. Internal jugular vein narrowing and body mass index in healthy individuals and multiple sclerosis patients. Veins Lymphat. 2014, 3, 89–92. [Google Scholar] [CrossRef] [Green Version]
- Burley, C.V.; Bailey, D.M.; Marley, C.J.; Lucas, S.J. Brain train to combat brain drain; focus on exercise strategies that optimize neuroprotection. Exp. Physiol. 2016, 101, 1178–1184. [Google Scholar] [CrossRef] [Green Version]
- Minhas, G.; Mathur, D.; Ragavendrasamy, B.; Sharma, N.K.; Paanu, V.; Anand, A. Hypoxia in CNS pathologies: Emerging role of miRNA-based neurotherapeutics and yoga based alternative therapies. Front. Neurosci. 2017, 11, 386. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Breathing Modes | pFDR | |||||
|---|---|---|---|---|---|---|
| F | PN | PD | F vs. PN | F vs. PD | PN vs. PD | |
| Average flow rate IJVs (mL/s) | 7.66 [1.72–10.50] | 4.88 [0.82–11.10] | 4.39 [0.99–8.41] | 0.002 | 0.001 | 0.132 |
| Average flow rate SSS (mL/s) | 4.87 [1.84–7.13] | 3.97 [2.30–6.65] | 3.08 [1.64–4.69] | 0.380 | 0.003 | 0.011 |
| Variance flow rate IJVs (mL/s)2 | 1.97 [0.46–2.88] | 1.19 [2.73–9.68] | 1.50 [0.02–10.40] | 0.090 | 0.188 | 0.732 |
| Variance flow rate SSS (mL/s)2 | 0.21 [0.02–0.92] | 0.15 [0.02–0.59] | 0.16 [0.03–0.49] | 0.430 | 0.890 | 0.470 |
| Area IJVs (mm2) | 28.70 [21.50–40.70] | 22.20 [7.94–71.50] | 24.50 [5.14–69.20] | 0.914 | 0.914 | 0.913 |
| Area SSS (mm2) | 21.50 [14.50–43.50] | 27.30 [13.10–40.20] | 24.10 [14–47.20] | 0.913 | 0.963 | 0.914 |
| Respiratory/Cardiac IJVs | 0.056 [0.004–6.460] | 0.415 [0.004–26.900] | 1.830 [0.015–18.200] | 0.027 | 0.009 | 0.128 |
| Respiratory/cardiac SSS | 0.135 [0.029–4.090] | 0.451 [0.045–2.800] | 1.660 [0.062–5.950] | 0.430 | 0.027 | 0.128 |
| NAUC(R) IJVs | 0.27 [0.06–1.62] a | 0.32 [0.15–0.69] | 0.53 [0.27–0.79] | 0.070 | 0.005 | 0.175 |
| NAUC(R) SSS | 0.12 [0.04–0.38] b | 0.13 [0.04–0.31] c | 0.19 [0.07–0.32] | 0.138 | 0.005 | 0.140 |
| NAUC(C) IJVs | 0.48 [0.13–0.77] a | 0.35 [0.07–0.79] | 0.16 [0.05–0.77] | 0.020 | 0.008 | 0.150 |
| NAUC(C) SSS | 0.42 [0.06–0.79] b | 0.38 [0.06–0.72] c | 0.16 [0.06–0.78] | 0.520 | 0.087 | 0.250 |
| Breathing Mode | High-Frequency Peak | Respiratory Frequency | Respiratory Frequency vs. High-Frequency Peak pFDR | |
|---|---|---|---|---|
| IJV | F | 0.24 [0.20–0.35] | 0.26 [0.22–0.31] | 0.126 |
| PN | 0.25 [0.20–0.40] | 0.25 [0.20–0.40] | 0.790 | |
| PD | 0.21 [0.16–0.35] | 0.22 [0.18–0.24] | 0.790 | |
| SSS | F | 0.26 [0.15–0.35] | 0.25 [0.19–0.32] | 0.493 |
| PN | 0.25 [0.20–0.28] | 0.25 [0.20–0.26] | 0.288 | |
| PD | 0.22 [0.17–0.25] | 0.22 [0.17–0.25] | 0.288 |
| Vein | Breathing Mode | Very High-Frequency Peak (Hz) | Cardiac Frequency (Hz) | Cardiac Frequency vs. Very High-Frequency Peak pFDR |
| IJV | F | 1.29 [0.80–2.82] | 1.22 [0.80–1.69] | 0.880 |
| PN | 1.27 [0.82–2.72] | 1.29 [0.81–1.65] | 0.900 | |
| PD | 1.21 [1.03–1.80] | 1.39 [0.83–1.90] | 0.889 | |
| SSS | F | 1.29 [0.79–1.74] | 1.32 [0.77–1.74] | 0.199 |
| PN | 1.24 [0.82–1.62] | 1.34 [0.85–1.64] | 0.190 | |
| PD | 1.39 [0.59–1.74] | 1.38 [0.55–1.52] | 0.190 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laganà, M.M.; Pirastru, A.; Ferrari, F.; Di Tella, S.; Cazzoli, M.; Pelizzari, L.; Jin, N.; Zacà, D.; Alperin, N.; Baselli, G.; et al. Cardiac and Respiratory Influences on Intracranial and Neck Venous Flow, Estimated Using Real-Time Phase-Contrast MRI. Biosensors 2022, 12, 612. https://doi.org/10.3390/bios12080612
Laganà MM, Pirastru A, Ferrari F, Di Tella S, Cazzoli M, Pelizzari L, Jin N, Zacà D, Alperin N, Baselli G, et al. Cardiac and Respiratory Influences on Intracranial and Neck Venous Flow, Estimated Using Real-Time Phase-Contrast MRI. Biosensors. 2022; 12(8):612. https://doi.org/10.3390/bios12080612
Chicago/Turabian StyleLaganà, Maria Marcella, Alice Pirastru, Francesca Ferrari, Sonia Di Tella, Marta Cazzoli, Laura Pelizzari, Ning Jin, Domenico Zacà, Noam Alperin, Giuseppe Baselli, and et al. 2022. "Cardiac and Respiratory Influences on Intracranial and Neck Venous Flow, Estimated Using Real-Time Phase-Contrast MRI" Biosensors 12, no. 8: 612. https://doi.org/10.3390/bios12080612