1. Introduction
Gonorrhoea is a major public health concern worldwide. The infection has a short incubation period of a few days, as well as a high transmission efficiency, and leads to a fivefold increase in HIV transmission and complications such as pelvic inflammatory disease and infertility, which compound the global health burden [
1]. The World Health Organisation (WHO) 2012 prevalence data for curable sexually transmitted infections revealed that the estimated global prevalence of gonorrhoea among women aged 15–49 years was 0.8% (95% uncertainty interval 0.6–1.0%) and among males aged 15–49 years old the prevalence was 0.6% (0.4–0.9%) [
2]. These estimates corresponded to an incidence of 78 million (53–110 million) new cases of gonorrhoea.
Neisseria gonorrhoeae, which is an obligate human pathogen, has displayed an alarming propensity to acquire resistance through genetic mechanisms (both chromosomal and plasmid-mediated) to all sequential first-line antimicrobial agents used over the years [
3]. Penicillin was first used in the 1940s and tetracycline from the 1950s to the 1980s, but high-level plasmid-mediated resistance to both agents was being described by the 1980s. Quinolones were introduced in the early 1980s, but resistance emerged in the Asia-Pacific region and spread globally [
4]. Antimicrobial resistance does not appear to confer a fitness cost as resistant strains continue to predominate globally following withdrawal of the antimicrobial from clinical use [
4]. Extended-spectrum cephalosporins (ESCs) were regarded as the last antimicrobial class suitable for widespread single-dose single-agent treatment. Cefixime is the most potent oral ESC and was also considered effective for the treatment of pharyngeal gonorrhoea [
4,
5]. In Japan in the 1990s, use of a variety of oral ESCs with suboptimal efficacies and inadequate dosing regimens led to ultimate treatment failure with cefixime [
6]. By 2010, clinically confirmed cefixime treatment failures had been described in Europe and North America [
7]. In 2007, reports of ceftriaxone treatment failure emerged from Australia, and by 2010 were being described in Japan and Western Europe [
7]. Importantly, all were cases of pharyngeal gonorrhoea. Spectinomycin, an aminocyclitol, was used in the 1980s as first-line therapy for the treatment of gonorrhoea. However, clinical treatment failures and in vitro resistance were being reported within a few years of use [
4]. Azithromycin is usually recommended only in dual combination therapy for gonorrhoea, as azithromycin monotherapy may result in high-level resistance to the antimicrobial via sequential point mutations in 23S rRNA [
8].
In South Africa, sexually transmitted infections (STIs) are managed through a syndromic approach at primary healthcare centres (PHCs), which ensures that treatment is given for the major causative pathogens based on clinical manifestations. Data showing the distribution of STI syndromes among males and females attending PHCs in South Africa reveal that male urethritis syndrome (MUS) and vaginal discharge syndrome (VDS) comprise the bulk of STI presentations [
9]. Syndromic management of STIs has resulted in a loss of specimen-taking skills among healthcare workers as well as a lack of development of optimised and standardised laboratory protocols for microbial culture and antimicrobial resistance testing. It has also led to a lack of ongoing investment in laboratory infrastructure in many regions. Periodic aetiological surveillance of STI syndromes is essential to update and validate the existing syndromic management guidelines. The Centre for HIV and STIs (CHIVSTI) at the National Institute for Communicable Diseases (NICD) in Johannesburg has co-ordinated microbiological surveillance in patients presenting to sentinel PHCs since 2006. Results indicate that
Neisseria gonorrhoea is the predominant cause of MUS (70–85%) and is present in 10–20% of symptomatic VDS cases [
10].
The WHO Global Gonococcal Antimicrobial Surveillance Program (GASP) was relaunched in 2009 to timely monitor the trends of antimicrobial resistance in
Neisseria gonorrhoeae and improve knowledge on potential resistance mechanisms through laboratory testing [
11]. South Africa is a participating country, and the STI laboratory at CHIVSTI has conducted gonococcal resistance surveys annually in Johannesburg since 2008. In May 2015, following endorsement by the 68th World Health Assembly for a Global Action Plan that aims to enhance global antimicrobial resistance surveillance activities, the WHO developed the Global Antimicrobial Resistance Surveillance System (GLASS) and listed
Neisseria gonorrhoeae as a priority pathogen.
We describe Neisseria gonorrhoeae antimicrobial resistance patterns and trends from Johannesburg STI sentinel surveillance over a ten-year period spanning 2008–2017.
3. Discussion
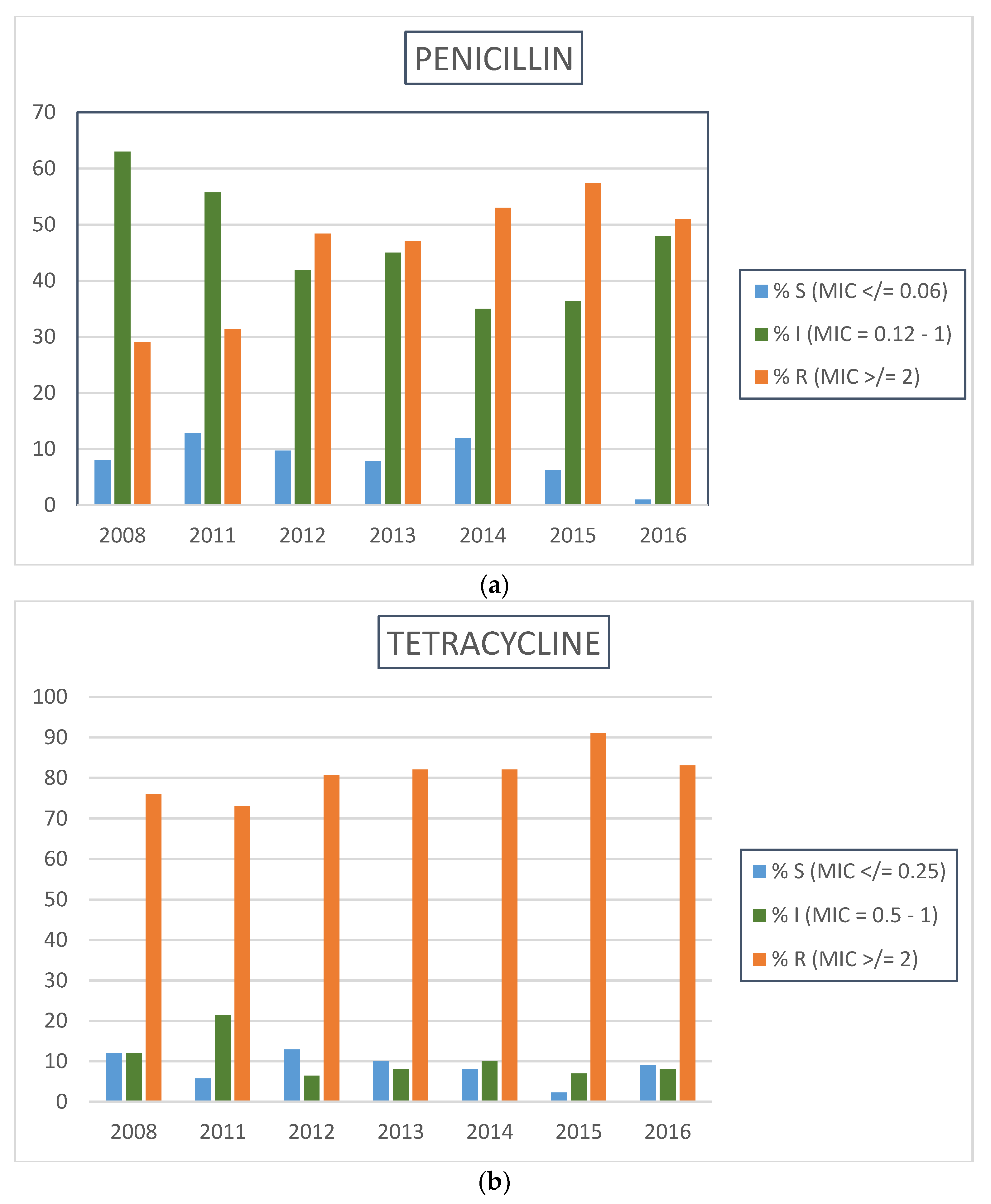
This surveillance report describes resistance trends to various antimicrobials used in past and current gonorrhoea treatment regimens over a ten-year surveillance period at a large primary healthcare centre in Johannesburg. Participants were mostly young adults, with the majority self-reporting heterosexual orientation, and belonged to a high risk-population for STI—a significant proportion had a history of recent STI and were HIV-infected.
Our data reveal that penicillin and tetracycline are unlikely to be included in any future genital discharge treatment algorithms in South Africa. In South African isolates, high-level penicillin resistance in
Neisseria gonorrhoeae was found to be plasmid-mediated: a novel beta-lactamase producing the “Johannesburg” plasmid was identified and these penicillinase-producing isolates were discovered to be clonally related [
14]. Similarly, both American- and Dutch-type tetracycline-resistant
Neisseria gonorrhoeae (TRNG) plasmids have been detected in South African isolates, and confer high-level resistance to the drug [
15].
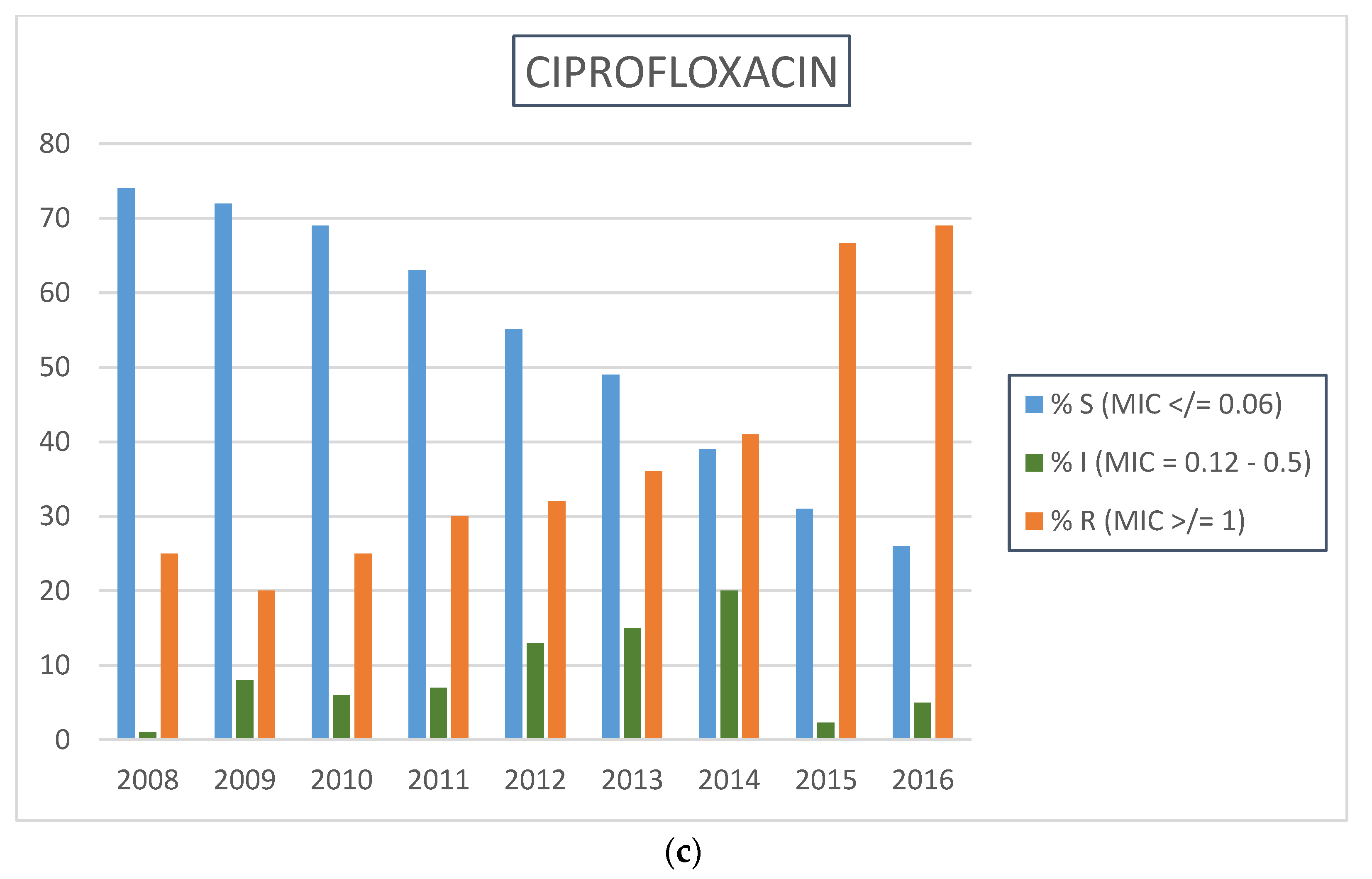
Escalating
N. gonorrhoeae ciprofloxacin resistance was seen in Johannesburg and Cape Town when data from 2004 and 2007 were compared [
16]. In Johannesburg, there was a 1.9-fold increase in resistance prevalence from 11% to 32%; and in Cape Town, a 2.9-fold increase from 7% to 27%. The World Health Organization (WHO) recommends a change of empirical treatment for gonorrhoea when the resistance threshold reaches 5% [
17]. In 2008, the South African syndromic management guidelines for genital discharge were formally revised to incorporate oral cefixime as first-line therapy for gonorrhoea [
18]. A sustained increase in high-prevalence resistance to ciprofloxacin was observed during our surveillance period, despite withdrawal of the antibiotic as a treatment option for genital discharge in 2008. This likely represents a fitness benefit conferred by type II topoisomerase mutations associated with ciprofloxacin resistance [
4], as well as antimicrobial selection pressure from continued use of ciprofloxacin at PHCs for other indications, such as acute cystitis.
The primary resistance determinant for extended-spectrum cephalosporins (ESCs) is a specific alteration in the
penA gene encoding penicillin binding protein 2 (PBP2). This is thought to occur through acquisition and recombination into its genome of foreign gene sequences from commensal
Neisseria species residing in the oropharynx [
19]. This transformation gives rise to a mosaic
penA gene encoding a mosaic PBP2 with reduced target affinity for ESCs: the MICs of cefixime are increased proportionately more than those of ceftriaxone [
20].
In South Africa, in 2012, the first two cases of cefixime resistance associated with cefixime treatment failure were described in two patients presenting with persistent urethral discharge [
21]. Genetic characterization of the two isolates using
Neisseria gonorrhoeae multi-antigen sequence typing (NG-MAST) and multi-locus sequence typing (MLST), revealed identical sequence types (NG-MAST ST4822 and MLST ST1901) which represent a multi-drug resistant clone associated with cefixime treatment failure and global spread. Both patients were in the men-who-have-sex-with-men (MSM) risk group. There are two factors that could lead to the spread of resistance in this key population: high risk sexual behaviour and participation in international sexual networks; and the presence of pharyngeal gonorrhoea, which is typically asymptomatic. Gonococci residing in the pharynx are at a survival advantage due to differential concentrations of antimicrobials at this site, and the opportunity for genetic exchange with oropharyngeal commensal
Neisseria species. An additional two cases of resistance to cefixime were identified in MSM residing in Cape Town and East London, respectively (D. Lewis, unpublished data).
In 2009, the world’s first confirmed extensively-drug resistant (XDR)
Neisseria gonorrhoeae infection was reported in Japan [
22]. The gonococcal strain, isolated from the pharynx of a commercial sex worker (CSW), displayed high-level resistance to both cefixime (MIC = 8 µg/mL) and ceftriaxone (MIC = 2–4 µg/mL). It was also resistant to several other classes of antimicrobials, including fluoroquinolones, macrolides, and tetracycline.
Following these reports, in accordance with WHO recommendations, there was a national change in recommended first-line therapy for gonorrhoea from oral cefixime to injectable ceftriaxone (250 mg single-dose) in 2014. Additional dual therapy with oral azithromycin (1 g stat) was recommended [
23]. This was a pro-active and pre-emptive approach, endorsed by the WHO, to limit the emergence of XDR
Neisseria gonorrhoeae particularly in areas where there is a general lack of surveillance in key populations, such as MSM and CSW [
24].
High-level resistance to spectinomycin is relatively rare, and has been attributed to a single nucleotide polymorphism in 16S rRNA as well as mutated ribosomal protein S5 [
25]. Although spectinomycin appears to be a viable alternative in our setting, it is not listed on the South African Essential Medicines List for primary healthcare centres; and has reduced efficacy against pharyngeal gonorrhoea [
4]. We have identified low prevalence intermediate-resistance to azithromycin (MIC 0.5 µg/mL) among gonococcal isolates in recent years. Although clinical effectiveness of azithromycin for urethral and endocervical infections has been estimated to be >95% [
26], it is recommended only in dual therapy due to the ease of resistance development to macrolide monotherapy. Resistance has been described even with use of higher dose (2 g) azithromycin monotherapy [
27], and this dose is associated with increased gastro-intestinal side-effects. Successful and sustained spread of a high-level azithromycin-resistant (MIC ≥ 256 µg/mL) clone of
Neisseria gonorrhoeae (NG MAST ST 9768) has been described in England [
28]. The outbreak, which began among young heterosexuals in Leeds in November 2014, had by 2016 become geographically dispersed to the North and South of the country and spread to MSM sexual networks. Whole genome sequencing revealed the presence of mutations in all four alleles of the 23S rRNA gene in the majority of isolates, and raised concerns that high-level resistance may develop stepwise from low-level resistance characterised by the presence of mutation in a single allele, especially in the setting of azithromycin selection pressure.
Failure of dual ceftriaxone–azithromycin therapy has been described from the United Kingdom, with persistence of asymptomatic pharyngeal gonorrhoea in a heterosexual man treated for urogenital symptoms in 2014 [
29]. The patient was infected with an XDR strain, which had acquired multiple resistance mechanisms to both ceftriaxone and azithromycin. Molecular epidemiology identified the isolate as MLST ST1901 and a new NG-MAST ST 12133, which belongs to a genogroup that is associated with extensive drug-resistance and is spreading in Japan. More recently, Public Health England issued a report of a heterosexual man with a test-of-cure pharyngeal gonococcal isolate showing resistance to ceftriaxone (MIC 0.5 µg/mL) and high-level resistance to azithromycin (MIC > 256 µg/mL), with possible links to a female sexual contact in South East Asia [
30].
The ease with which Neisseria gonorrhoeae develops drug resistance means that antimicrobial stewardship strategies are urgently needed: rational, standardized, and regulated prescription practice for genital discharge syndrome. Research and development initiatives should include funding for novel antimicrobials with unique mechanisms of action, facilitating their incorporation into appropriate therapeutic regimens.
Limitations of this surveillance study include the lack of in-depth information on behavioural risk characteristics of participants, as well as being conducted in largely heterosexual populations at a single clinical site. There is a need for accurate rapid diagnostics for gonorrhoea that would facilitate screening for asymptomatic and extra-genital infection in high-risk population groups such as MSM. Additionally, allocation of resources is required for enhanced local surveillance strategies in order to better understand transmission dynamics and inform control efforts. These would include the design and implementation of activities to increase detection of treatment failure cases and extragenital (pharyngeal) infections at primary and secondary healthcare level, as well as sustained antimicrobial surveys (including test-of-cure) in key populations.





{kind=link}
{kind=link}