
PNPLA3 Single Nucleotide Polymorphism Prevalence and Association with Liver Disease in a Diverse Cohort of Persons Living with HIV

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Study Cohort
2.2. PNPLA3 SNPs
2.3. Determination of Hepatic Steatosis and Fibrosis
2.4. Laboratory Assessments
2.5. Insulin Resistance
2.6. Statistical Methods
3. Results
3.1. Study Participants
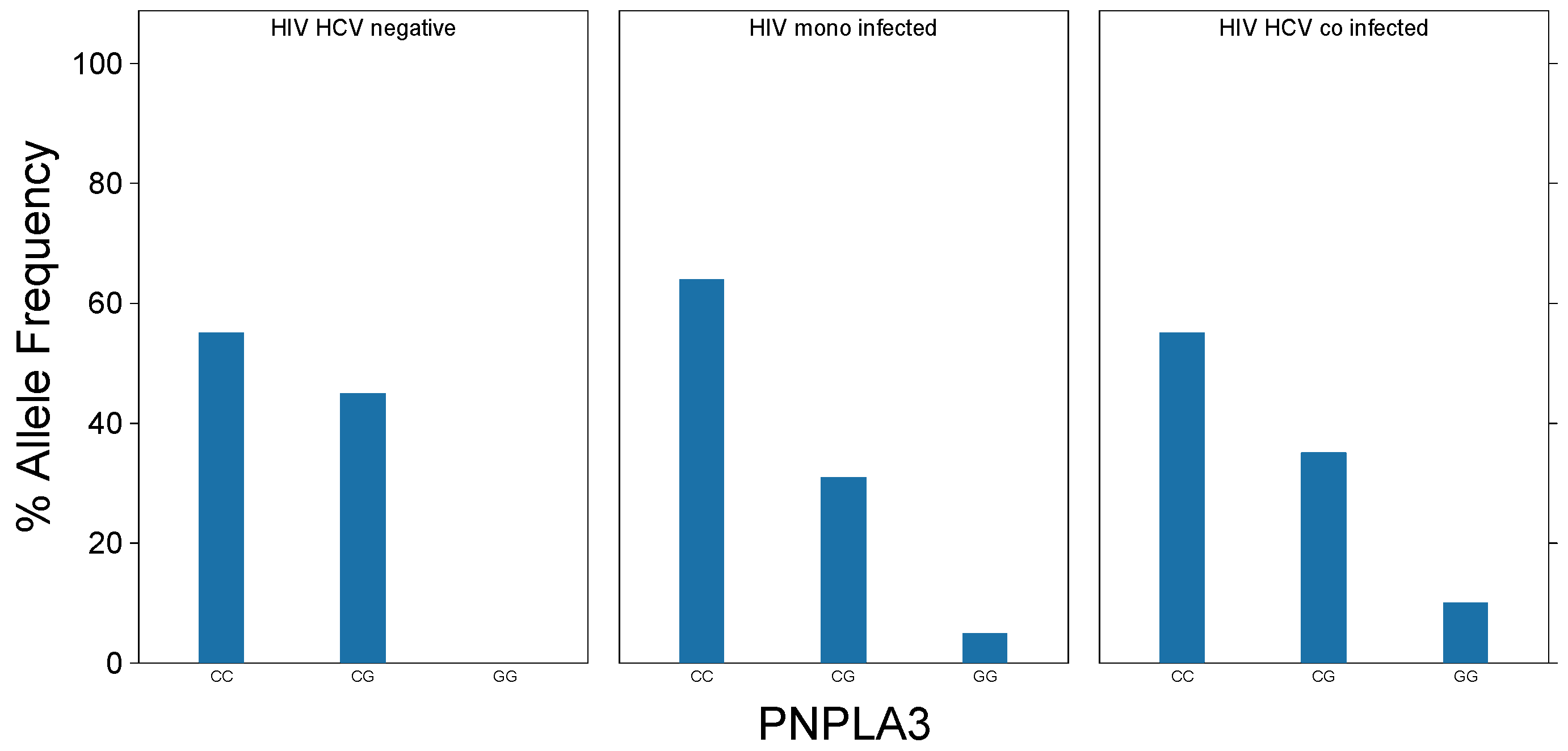
3.2. PNPLA3 Genotype Distibution
3.3. Steatosis, Fibrosis, and HIV
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Romeo, S.; Huang-Doran, I.; Baroni, M.G.; Kotronen, A. Unravelling the pathogenesis of fatty liver disease: Patatin-like phospholipase domain-containing 3 protein. Curr. Opin. Lipidol. 2010, 21, 247–252. [Google Scholar] [CrossRef]
- Tian, C.; Stokowski, R.P.; Kershenobich, D.; Ballinger, D.G.; Hinds, D.A. Variant in PNPLA3 is associated with alcoholic liver disease. Nat. Genet. 2009, 42, 21–23. [Google Scholar] [CrossRef]
- Sharpton, S.R.; Ajmera, V.; Loomba, R. Emerging Role of the Gut Microbiome in Nonalcoholic Fatty Liver Disease: From Composition to Function. Clin. Gastroenterol. Hepatol. 2019, 17, 296–306. [Google Scholar] [CrossRef] [PubMed]
- Sherman, K.E.; Peters, M.G.; Thomas, D.L. HIV and the Liver. Top. Antivir. Med. 2019, 27, 101–110. [Google Scholar] [PubMed]
- Klein, M.B.; Althoff, K.N.; Jing, Y.; Lau, B.; Kitahata, M.M.; Freeman, A.M.; Kirk, G.D.; Hull, M.; Kim, H.N.; Sebastiani, G.; et al. Risk of End-Stage Liver Disease in HIV-Viral Hepatitis Coinfected Persons in North America From the Early to Modern Antiretroviral Therapy Eras. Clin. Infect. Dis. 2016, 63, 1160–1167. [Google Scholar] [CrossRef] [PubMed]
- Calza, L.; Colangeli, V.; Borderi, M.; Bon, I.; Borioni, A.; Volpato, F.; Re, M.C.; Viale, P. Weight gain in antiretroviral therapy-naive HIV-1-infected patients starting a regimen including an integrase strand transfer inhibitor or darunavir/ritonavir. Infection 2019, 48, 213–221. [Google Scholar] [CrossRef]
- Calza, L.; Colangeli, V.; Borderi, M.; Coladonato, S.; Tazza, B.; Fornaro, G.; Badia, L.; Guardigni, V.; Verucchi, G.; Viale, P. Improvement in liver steatosis after the switch from a ritonavir-boosted protease inhibitor to raltegravir in HIV-infected patients with non-alcoholic fatty liver disease. Infect. Dis. 2019, 51, 593–601. [Google Scholar] [CrossRef] [PubMed]
- Price, J.C.; Seaberg, E.C.; Latanich, R.; Budoff, M.J.; Kingsley, L.A.; Palella, F.J.; Witt, M.D.; Post, W.S.; Thio, C.L. Risk Factors for Fatty Liver in the Multicenter AIDS Cohort Study. Am. J. Gastroenterol. 2014, 109, 695–704. [Google Scholar] [CrossRef] [Green Version]
- Sherman, K.E.; For the ACTG 5294 BIRTH Study Team; Rouster, S.D.; Kang, M.; Umbleja, T.; Sterling, R.; Butt, A.A. PNPLA3 Gene Polymorphisms in HCV/HIV-Coinfected Individuals. Dig. Dis. Sci. 2018, 63, 2969–2974. [Google Scholar] [CrossRef]
- Bosh, K.A.; Johnson, A.S.; Hernandez, A.L.; Prejean, J.; Taylor, J.; Wingard, R.; Valleroy, L.A.; Hall, H.I. Vital Signs: Deaths Among Persons with Diagnosed HIV Infection, United States, 2010–2018. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 1717–1724. [Google Scholar] [CrossRef]
- Allen, J.P.; Litten, R.Z.; Fertig, J.B.; Babor, T. A review of research on the Alcohol Use Disorders Identification Test (AUDIT). Alcohol. Clin. Exp. Res. 1997, 21, 613–619. [Google Scholar] [CrossRef]
- Singh, S.; Venkatesh, S.K.; Loomba, R.; Wang, Z.; Sirlin, C.B.; Chen, J.; Yin, M.; Miller, F.H.; Low, R.N.; Hassanein, T.; et al. Magnetic resonance elastography for staging liver fibrosis in non-alcoholic fatty liver disease: A diagnostic accuracy systematic review and individual participant data pooled analysis. Eur. Radiol. 2016, 26, 1431–1440. [Google Scholar] [CrossRef]
- Angulo, P.; Hui, J.M.; Marchesini, G.; Bugianesi, E.; George, J.; Farrell, G.C.; Enders, F.; Saksena, S.; Burt, A.D.; Bida, J.P.; et al. The NAFLD fibrosis score: A noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology 2007, 45, 846–854. [Google Scholar] [CrossRef]
- Sánchez-García, A.; Rodríguez-Gutiérrez, R.; Mancillas-Adame, L.; González-Nava, V.; González-Colmenero, A.D.; Solis, R.C.; Álvarez-Villalobos, N.A.; González-González, J.G. Diagnostic Accuracy of the Triglyceride and Glucose Index for Insulin Resistance: A Systematic Review. Int. J. Endocrinol. 2020, 2020, 1–7. [Google Scholar] [CrossRef]
- Saab, S.; Manne, V.; Nieto, J.; Schwimmer, J.B.; Chalasani, N.P. Nonalcoholic Fatty Liver Disease in Latinos. Clin. Gastroenterol. Hepatol. 2016, 14, 5–12. [Google Scholar] [CrossRef] [Green Version]
- Davis, J.N.; Lê, K.-A.; Walker, R.W.; Vikman, S.; Spruijt-Metz, N.; Weigensberg, M.J.; Allayee, H.; Goran, M.I. Increased hepatic fat in overweight Hispanic youth influenced by interaction between genetic variation in PNPLA3 and high dietary carbohydrate and sugar consumption. Am. J. Clin. Nutr. 2010, 92, 1522–1527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seth, A.; Sherman, K.E. Fatty liver disease in persons with HIV infection. Top. Antivir. Med. 2019, 27, 75–82. [Google Scholar]
- Qu, Y.; Li, M.; Hamilton, G.; Zhang, Y.N.; Song, B. Diagnostic accuracy of hepatic proton density fat fraction measured by magnetic resonance imaging for the evaluation of liver steatosis with histology as reference standard: A meta-analysis. Eur. Radiol. 2019, 29, 5180–5189. [Google Scholar] [CrossRef] [PubMed]
- Lui, G.; Wong, V.W.-S.; Wong, G.L.-H.; Chu, W.C.-W.; Wong, C.-K.; Yung, I.M.H.; Wong, R.Y.K.; Yeung, S.-L.; Yeung, D.K.-W.; Cheung, C.S.K.; et al. Liver fibrosis and fatty liver in Asian HIV-infected patients. Aliment. Pharmacol. Ther. 2016, 44, 411–421. [Google Scholar] [CrossRef] [PubMed]
- Woreta, T.A.; Sutcliffe, C.G.; Mehta, S.H.; Brown, T.T.; Higgins, Y.; Thomas, D.L.; Torbenson, M.S.; Moore, R.D.; Sulkowski, M.S. Incidence and Risk Factors for Steatosis Progression in Adults Coinfected With HIV and Hepatitis C Virus. Gastroenterology 2011, 140, 809–817. [Google Scholar] [CrossRef] [Green Version]
- Sterling, R.K.; Smith, P.G.; Brunt, E.M. Hepatic Steatosis in Human Immunodeficiency Virus. J. Clin. Gastroenterol. 2013, 47, 182–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crum-Cianflone, N.; Dilay, A.; Collins, G.; Asher, D.; Campin, R.; Medina, S.; Goodman, Z.; Parker, R.; Lifson, A.; Capozza, T.; et al. Nonalcoholic Fatty Liver Disease Among HIV-Infected Persons. JAIDS J. Acquir. Immune Defic. Syndr. 2009, 50, 464–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| HIV | HCV/HIV | HCV & HIV Negative | p-Value | |
|---|---|---|---|---|
| (n = 100) | (n = 20) | (n = 20) | ||
| Age (years, median, range) | 53 (23–69) | 52 (27–65) | 52 (40–62) | n.s |
| Sex (% male at birth) | 63 | 60 | 35 | n.s |
| Race/Ethnicity (%) | n.s. | |||
| Black, non-Hispanic | 66 | 65 | 70 | |
| White, Hispanic | 18 | 20 | 20 | |
| White, non-Hispanic | 10 | 0 | 5 | |
| Other | 6 | 15 | 5 | |
| ALT (Median, range) | 18 (7–72) | 25 (8–120) | 19 (8–77) | n.s. |
| AST (Median, range) | 21 (11–58) | 30 (14–103) | 26 (13–41) | 0.03 |
| BMI (Median) | 28.1 | 30 | 31.6 | n.s. |
| AUDIT (Median) | 3.0 | 2.5 | 4.5 | n.s. |
| CD4 (Median) | 556 | 580 | n/a | n.s. |
| HIV Viral Load (Median Copies/ml) | 19 | 19 | n/a | n.s. |
| TyG Index (median) | 4.62 | 4.57 | 4.64 | n.s. |
| Steatosis (>5% fat) | 13.3% | 20% | 55% | 0.001 |
| Hepatic Fibrosis (%) | 10.1 | 35.0 | 0 | 0.0016 |
| PNPLA3 Genotype (%) | ||||
| CC | 64 | 55 | 55 | |
| CG | 31 | 35 | 45 | |
| GG | 5 | 10 | 0 |
| Characteristic | p-Value |
|---|---|
| Ethnicity/Race | 0.88 |
| BMI | 0.0001 |
| Diabetes | 0.65 |
| HIV | 0.007 |
| Sex (at birth) | 0.85 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sherman, K.E.; Rouster, S.D.; Meeds, H.; Tamargo, J.; Chen, J.; Ehman, R.; Baum, M. PNPLA3 Single Nucleotide Polymorphism Prevalence and Association with Liver Disease in a Diverse Cohort of Persons Living with HIV. Biology 2021, 10, 242. https://doi.org/10.3390/biology10030242
Sherman KE, Rouster SD, Meeds H, Tamargo J, Chen J, Ehman R, Baum M. PNPLA3 Single Nucleotide Polymorphism Prevalence and Association with Liver Disease in a Diverse Cohort of Persons Living with HIV. Biology. 2021; 10(3):242. https://doi.org/10.3390/biology10030242
Chicago/Turabian StyleSherman, Kenneth E., Susan D. Rouster, Heidi Meeds, Javier Tamargo, Jun Chen, Richard Ehman, and Marianna Baum. 2021. "PNPLA3 Single Nucleotide Polymorphism Prevalence and Association with Liver Disease in a Diverse Cohort of Persons Living with HIV" Biology 10, no. 3: 242. https://doi.org/10.3390/biology10030242