1. Introduction
Urinary tract infections (UTIs) are a leading cause of patient visits to healthcare providers, accounting for approximately 150 million cases annually worldwide [
1]. This includes one million emergency department visits and over 626,000 hospitalizations, with an estimated annual healthcare spending of USD 3.5 billion in the United States alone [
2]. While simple UTI rapidly resolves with treatment, a subset of patients present with or develop complicated UTI (cUTI), which is more likely to be associated with adverse outcomes, including a protracted therapeutic course, increased morbidity, and even mortality [
3]. Because of the potential for serious and long-term complications and adverse effects on the GU tract or other organ systems in cUTI, it is crucial that pathogen identification is both rapid and correct [
4].
Traditional urine culture (UC) has been the cornerstone of pathogen identification in UTI for over a century. UC is challenged by time and technical limitations and requires both selective and non-selective media and technical personnel to interpret the results [
5,
6]. Tradition diagnosis of UTI requires a growth threshold of 10
5 CFU/mL, although the guidelines have been modified to lower the threshold value based on patient history, presentation, and other factors [
7]. False-negative UC results may also occur due to various technical reasons [
8]. In addition, pre-analytic factors such as faulty specimen handling may result in inappropriate false-positive or false-negative urine culture results [
9]. While the literature suggests that
E. coli is responsible for up to 80 percent of uncomplicated UTIs, reports suggest that this organism is responsible for as little as one-third of cUTIs [
2,
10]. In addition,
E. coli grows rapidly in standard culture media and can competitively suppress coincident pathogens, leading to non-detection of the organism. Recently, several pioneering studies have suggested that there may be substantial improvements in identifying polymicrobial pathogens using syndromic molecular assays with polymerase chain reaction (PCR) technology, [
11,
12,
13] and in addition, that PCR testing is best accomplished by a relatively expanded panel size [
14]. While important, the literature is limited either due to a relatively small number of patients, or in the case of multi-center studies, the possibility that there was variance between sites in either patient selection, PCR protocols, or both.
In our multisite urology practice, we developed practice guidelines that govern the use of PCR testing and sought to ascertain whether there was a difference in overall pathogen detection between PCR and conventional UC testing, specifically in patients who met these guidelines. Furthermore, we sought to evaluate whether this difference, if present, extends to the identification of fastidious organisms (FOs) or UTIs where polymicrobial organisms (PMOs) are present. To further assess the clinical utility on an individual specimen basis, we performed a line-item analysis for each sample to determine whether PCR or UC uniquely identified potentially pathogenic organisms not found in the other test.
3. Results
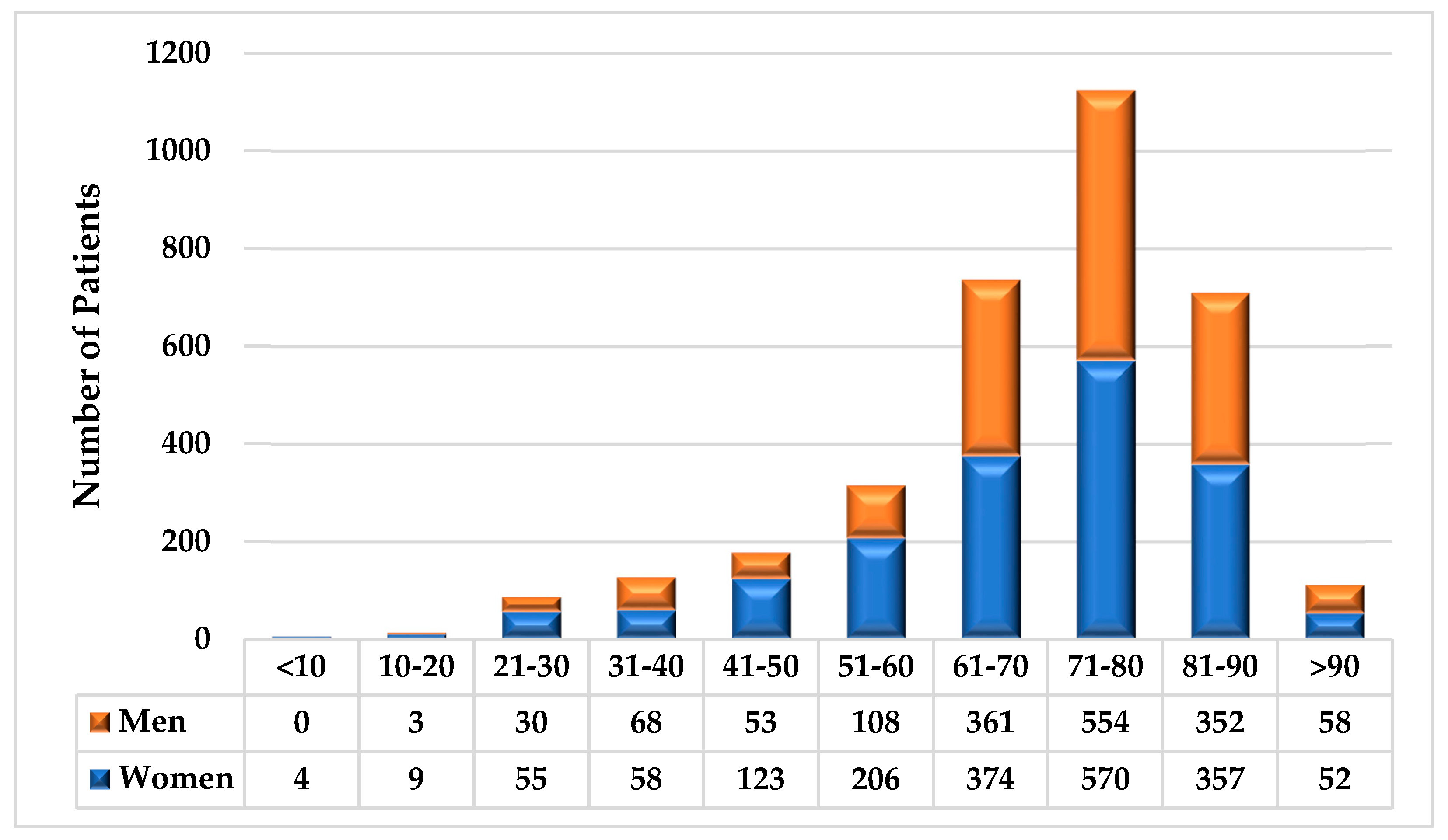
The age and sex distributions of the patients are shown in
Figure 1. Of the 3395 patients who met the inclusion criteria, 53.3% (1808) were female and 46.7% (1587) were male (D6.6%%,
p < 0.01). Most patients (78.9%,
p < 0.01) were older than 60 years, and gender differences were influenced by age. For patients younger than 60 years, our population included 63.5% women and 36.5% men (D26.9%,
p < 0.01); however, for those older than 60 years, the gender difference in our population was nominal (50.5% female, 49.5% male, D1.0%,
p = 0.96). In total, 66/3395 (1.9%) patients had specimens collected via straight catheter (34 males, 32 females). As per practice protocol, no patient who underwent PCR testing had their specimen collected via indwelling catheter.
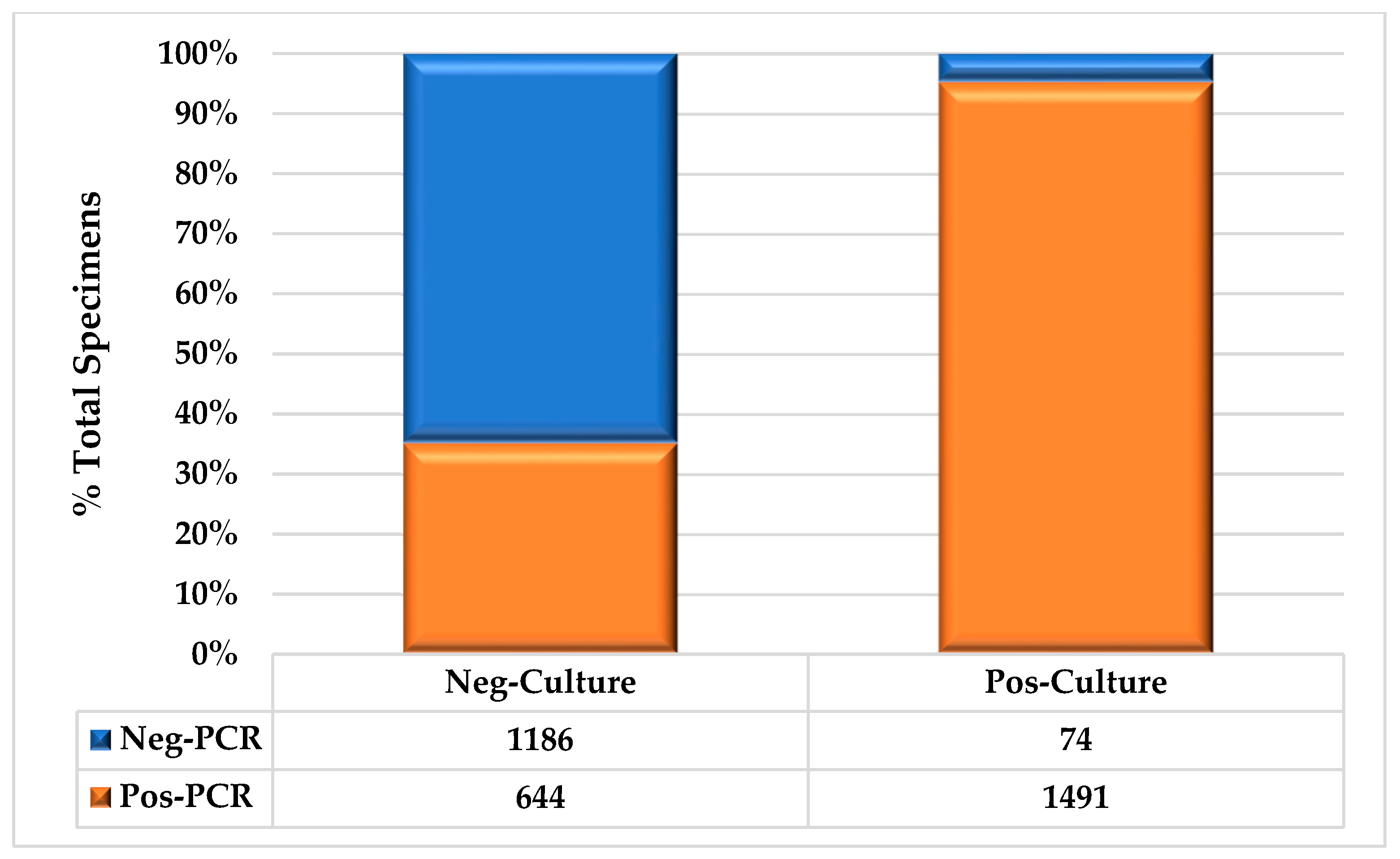
The overall test results are shown in
Figure 2. Based on PCR, 95.3% of the positive urine cultures were also identified as positive. Of the positive UCs that were determined to be negative based on PCR, 48.6% (36/74) were due to organisms that were not present on the PCR panel. More than one-third (35.2%) of the UC samples tested positive by PCR (
p < 0.01). Of the UC specimens, 46.1% (1565/3395) and 62.8% (2135/3395) were positive by PCR (16.8%;
p < 0.01).
We also reviewed the UC and PCR results based on the method of collection (
Table 4). We observed that in both UC and PCR, test positivity was higher in catheterized vs. clean-catch collections. For PCR, 49/66 (74.2%) vs. 2086/3329 (62.7%) catheterized and clean-catch samples, respectively, were positive (difference: 11.6%,
p = 0.07). For UC, 38/66 (57.6%) vs. 1527/3329 (45.9%) samples were positive (difference: 11.7%,
p = 0.08).
We also reviewed the difference between positive PCR and UC test results and the results of the corresponding test in patients that were and were not catheterized, as summarized in
Table 5. We found that in PCR-positive clean-catch samples, 1442/2025 (70.3%) UCs were positive, while 36/49 (73.5%) catheterized PCR-positive specimens were UC-positive (difference: 3.2%,
p = 0.75). Conversely, in positive UCs, 1455/1527 (95.3%) and 36/38 (94.7%) samples obtained by clean catch and catheter, respectively, were PCR-positive (difference: 0.6%,
p = 0.70).
We found that PCR was significantly more likely to detect both PMOs and FOs than UC was. With respect to multiple organisms, PMOs were found in 2.1% (33/1565) of UC+ specimens versus 42.0% (896/2135) of PCR+ specimens (difference: 39.9%, p < 0.01). All 33 PMOs found in the UC+ specimens grew into two organisms. Of the 896 PMOs identified by PCR, 63.5% (547) had 2 organisms, 26.6% (229) had 4 or more organisms, and 13.9% (120) had 4 or more organisms. When stratified by specimen collection methodology, we found that 20/49 (40.8%) and 876/2086 (42.0%) positive PCR results obtained by catheterization and clean catch, respectively, had PMOs (difference: 1.2%, p = 0.99). Simultaneously, we found that 1/38 (2.6%) and 32/1527 (2.1%) positive UC results obtained by catheterization and clean catch, respectively, grew multiple organisms (difference: 0.5%, p = 0.56).
Our analysis showed that FOs were found in 0.6% (9/1565) of UC+ specimens and 21.4% (456/2135) of PCR+ specimens (difference: 21.4%; p < 0.01). To assess the overlap between the PMOs and FOs in our patients with cUTI, we also evaluated the frequency with which patients tested by UC or PCR had either PMOs or FOs, and whether each test had both PMOs and FOs. For UC+ specimens, 2.7% (42/1565) showed either PMOs or FOs, compared with 46.8% (999/2135) for PCR+ specimens (difference: 44.1%, p < 0.01). In total, 16.5% (353/2135) of the PCR+ specimens had both PMOs and FOs; no UC+ specimens had both PMOs and FOs.
Individual organism counts, line-item organism concordance between the tests, and statistical analysis are shown in
Table 6. In total, 3571 instances of 50 unique organisms were identified in one or both tests: 34 (68%) were identified by PCR, whereas 41 (82%) were isolated in UC (difference: 14.0%,
p = 0.11). In total, there were 1454 instances of 25 unique organisms showing line-item concordance (LIC); this represented 40.7% of the organisms detected by PCR and 91.0% of the organisms identified by UC (difference: 50.3%,
p < 0.01). The percentage of LIC to total organism count for each test is also depicted in
Table 3. In total, 1595 UC+ specimens showed 1598 incidences of 41 organisms, whereas 2135 PCR+ samples identified 3571 instances of 34 organisms. Of the 41 organisms grown in UC, 39.0% were not identified by PCR, whereas 26.5% of the organisms identified by PCR were not isolated from UC (difference: 12.5%,
p = 0.25). There were 36 instances of the 16 organisms found in UC but not PCR, which represented 2.3% of the 1598 organisms found in UC; conversely, there were 666 instances of the 9 organisms found by PCR but not UC, which was 18.7% of the 3571 organisms identified by PCR (difference: 16.4%,
p < 0.01). Only 5.6% of the organisms in the PCR panel were not detected in any of the samples (
C. urealyticum and
M. tuberculosis).
The presence of organisms uniquely identified by UC and PCR is shown in
Table 7: 9.4% (147/1565) of UC+ and 62.4% (1333/2135) of PCR+ specimens had organisms that were not found in the other tests (difference: 53.0%,
p < 0.01). The specimens were further stratified according to the presence of one or more identified organisms: 36.8% (456/1239) of single-organism PCR+ samples revealed organisms not identified in UC; 7.9% (36/456) of these were UC+ for other organisms. A total of 8.4% (128/1532) single-organism UC+ samples were not detected by PCR (difference: 28.2%,
p < 0.01); of these, 43.4% (53/128) were PCR+ for organisms not identified in UC. Of the 128 samples, 30 (23.4%) were organisms that were not on the PCR panel.
4. Discussion
Urinary molecular testing using either PCR amplification or next-generation sequencing has identified a multitude of organisms in the ‘healthy’ bladder, which challenges conventional wisdom that urine is sterile at baseline [
15]. It is now clear that the historical notion of sterility in urine is at least partially predicated on limitations of urine culture. Despite previously published data suggesting that organism detection is enhanced using PCR, concerns regarding the use of molecular testing to diagnose UTIs have been raised. These concerns include the possibility of identifying organisms that are not pathogenic in the presenting clinical episode, the lack of standardization of urinary molecular panels, and the costs associated with these novel tests. Our data suggest that these considerations are outweighed by the benefits for patients with cUTI; these patients have unique diagnostic and therapeutic challenges, and traditional UC may be an inadequate or insufficient diagnostic test.
This group of patients typically presents to the urology office or emergency room with failed previous treatment or experience of frequent or rapid recurrences or progression due to (1) incorrect or insufficient therapy, or (2) failure to identify and address an underlying anatomic or comorbid condition. Our data clearly showed that UC poorly identifies UTIs caused by FOs and is inadequate in identifying all causative organisms present in PMOs, limiting the utility of UC in this population who are at risk for the presence of either or both. As the management of patients with cUTI presents a difficult clinical challenge, it is imperative that urologists and other specialists have access to diagnostic tools that provide potentially actionable information, especially for the correct identification of pathogenic organisms. The provider can subsequently assimilate these data along with other clinical information to determine the most appropriate treatment course. Importantly, while we found that PCR was superior to UC in overall organism detection, as well as detection of FOs and PMOs, our data do not support the abandonment of UC in this set of patients. Over 8% of UC+ specimens had potential pathogens not found by PCR, with nearly a quarter of these (1.9% of all UC+ organisms) not part of the PCR panel.
Our data are consistent with those of previous studies, in terms of the overall sensitivity advantage of PCR over UC. This analysis differs in that we specifically studied patients who met the clinical criteria for cUTI, and for this subset of patients, PCR provided potentially clinically actionable information that was not available for UC. Unique, potentially actionable pathogenic organisms were found in over 60% of PCR specimens. Specifically, PCR was 20 times more likely to identify PMOs, and nearly 36 times more likely to identify FOs. While both findings are not unexpected given the technological difference between UC and PCR, the frequency with which PMOs and FOs were found in cUTI and the magnitude of the difference between the tests were profound. With respect to collection methodology, specimen positivity appeared higher in both UC and PCR in patients whose specimens were collected via catheterization or clean catch; however, in neither case were the results significant. This may be due to the relatively small number of patients (1.9%) who had their specimens obtained via catheterization vs. via clean-catch methods. Interestingly, although it could be surmised that PMOs would be more prevalent on clean-catch vs. catheterized specimens due to enhanced detection of contaminants, we did not observe any difference in the detection of PMOs based on specimen collection technique in either UC or PCR, and the difference in PMO detection between the two tests was consistent across collection technique. This may be because our urology practice has established protocols for collection of midstream clean-catch urine specimens, and as a specialty practice, our staff is highly trained in communicating this technique to the patient.
This study has several limitations owing to its retrospective nature and technical factors associated with the tests themselves. Our practice guidelines dictate when urinary molecular testing
can be performed, not that it
must be performed. The determination of whether any specific diagnostic test is utilized, while broadly determined by clinical guidelines, is up to the discretion of the treating provider. As this study was a laboratory analysis that did not involve chart review, it is possible that there were some patients with cUTI that did not receive PCR testing; however, all patients who had PCR and UC performed were captured in this analysis. A fundamental limitation in the use of PCR is that its sensitivity is primarily limited by the predefined panel of organism-specific primers in microarray chips. This concern was offset using a multi-organism panel that covered a substantial number of pathogenic organisms in the urinary tract [
14]. In addition, PCR can be affected by the presence of PCR inhibitors in the samples as well as technical issues, including low extraction efficiency and bubble formation in the OpenArray chip. These limitations were mitigated by utilizing a single, large-volume commercial laboratory with extensive experience in PCR testing. Conversely, the growth of organisms in UC may be affected by prior or recent antibiotic use, which may lead to exacerbating the apparent superiority of PCR. This limitation is mitigated as our purpose was specifically to compare PCR and UC in a subset of patients with cUTI—these patients often present having failed prior antibiotic therapy, and therefore our data illustrate the real-world challenges faced by clinicians managing this difficult-to-treat subset of patients. And while recent data suggest that genotypic antibiotic sensitivity detected by molecular techniques is similar to the phenotypic resistome [
16], to ensure that clinicians were provided optimal data for patient management, our protocol calls for UC, PCR, and antibiotic resistance testing to be performed in conjunction on the same sample. Thus, while patients with cUTI may have been previously treated with antibiotics, the identification of a pathogen by culture and/or PCR and the associated antibiotic susceptibility and antibiotic resistance gene profile in a symptomatic patient is likely indicative of an active infection regardless of methodology.
Although the detection of PMOs may be relevant in the management of cUTI, the presence of multiple organisms detected by PCR can be difficult to interpret. That said, the data strongly suggest that the presence of PMOs is associated with increased bacterial pathogenicity [
17] as well as adverse outcomes in patients with cUTI [
18]; therefore, identification of multiple pathogens in urine has prognostic value in addition to direct clinical utility. In addition, to ensure that the PCR report was meaningful, the reference laboratory utilized a cycle threshold limit for each organism that was defined as positive. With respect to FOs, the definition of an FO varies from laboratory to laboratory based on local technical considerations, particularly with respect to growth media, which was mitigated in this study as both PCR and UC testing were performed by the same commercial lab with consistent techniques during the study period; therefore, the data were internally consistent. Finally, this study did not include a review of antibiotic use or clinical courses on a patient–patient basis. As this was a comparative study on organism identification, chart review was not a component of this study; a prospective study to review the impact of PCR testing on patient care is in process.
This study did not include an analysis of next-generation sequencing (NGS) in this subset of patients as it is not, at present, a routine part of our clinical practice. Whole-genome shotgun sequencing is an excellent tool regarding unbiased pathogen detection in comparison to PCR, which has defined panels of pathogens to detect. While there is active research in the analysis of the urinary microbiome with over 350 publications per annum [
19], publications on next-generation sequencing in UTI are scarcer, averaging fewer than 10 per year [
20]. Indeed, the number of organisms identified by next-generation sequencing may be bewildering to the clinician—one analysis revealed a median 41 bacterial genera, 2 eukarya species, and 3 viral sequences
per sample [
21]. A recent meta-analysis comparing results of PCR and NGS found that PCR had a 99% sensitivity and a 94% specificity for diagnosing UTIs, while NGS was shown to have a 90% and 86% sensitivity and specificity, respectively, for identifying UTIs [
22]. Future studies comparing PCR and NGS are needed to better define the role of these tests, but at present, there is limited need for whole-genome sequencing of clinical isolates for pathogen identification on a large scale given the availability of alternative technologies that offer a faster turnaround time, greater cost efficiency, and lower complexity.
Finally, while this study was performed in a single independent specialty practice using a commercial laboratory, the management of cUTI and the prevalence of multi-drug-resistant organisms are international problems [
23,
24] that pose a substantial economic burden on individual institutions and healthcare systems [
25,
26]. The data suggest that this burden may be reduced by urinary molecular testing [
27]; therefore, we believe that the findings are relevant not only to independent specialty practices, but to institutional settings in the United States and abroad as well.



 ,
, 


{kind=link}
{kind=link}