Value of SUVmax for the Prediction of Bone Invasion in Oral Squamous Cell Carcinoma

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Patient and Tumor Characteristics
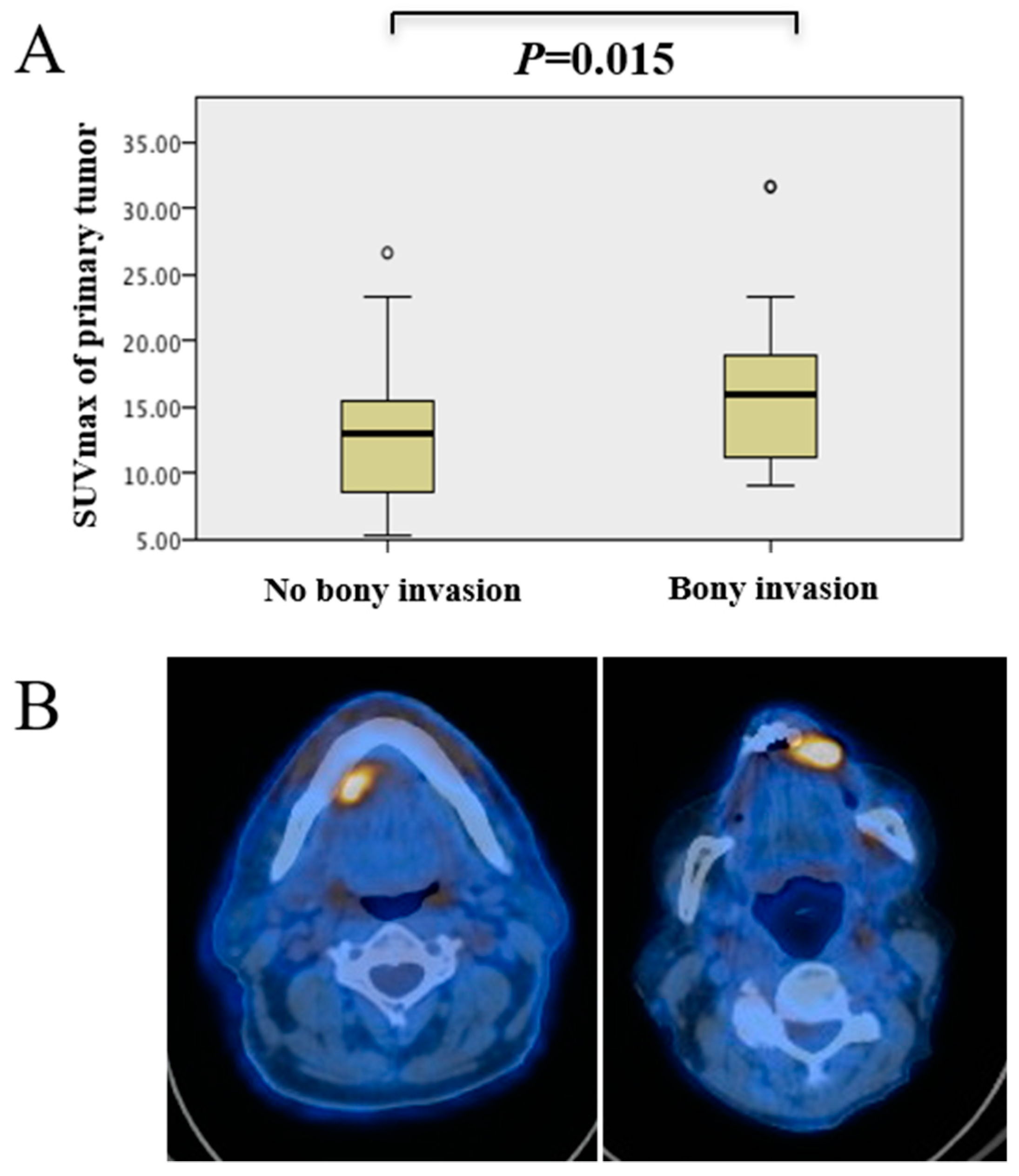
2.2. Patients with Bone Invasion Had Higher SUVmax of Primary Tumor
2.3. Prediction of Mandibular Infiltration Using Clinical Examination, Computed Tomography (CT), and Magnetic Resonance Imaging (MRI)
2.4. Prediction of Bone Invasion Using Metabolic Tumor Imaging
2.5. Enhanced Diagnostic Accuracy Using Metabolic Imaging
2.6. Survival Outcomes
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. FDG-PET/CT or -/MR Image Acquisition
4.3. Image Assessment
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Morand, G.B.; Broglie, M.A. Therapie des Mundhölenkarzinoms: Tumorkontrolle und Funktionalität; MedEdition: Hirzel, Switzerland, 2019. [Google Scholar]
- Shah, J.P.; Gil, Z. Current concepts in management of oral cancer--surgery. Oral Oncol. 2009, 45, 394–401. [Google Scholar] [CrossRef] [Green Version]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Mascitti, M.; Rubini, C.; De Michele, F.; Balercia, P.; Girotto, R.; Troiano, G.; Lo Muzio, L.; Santarelli, A. American Joint Committee on Cancer staging system 7th edition versus 8th edition: Any improvement for patients with squamous cell carcinoma of the tongue? Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 126, 415–423. [Google Scholar] [CrossRef]
- Morand, G.B.; Broglie, M.A.; Schüler-Garcia, H.I. Radiotherapie versus Chirurgie für Kopf-Hals-Tumoren (Mundhöhle, Oropharynx, Larynx, Hypopharynx). Trill. Krebsmed. 2018, 27, 426–434. [Google Scholar]
- Gu, D.H.; Yoon, D.Y.; Park, C.H.; Chang, S.K.; Lim, K.J.; Seo, Y.L.; Yun, E.J.; Choi, C.S.; Bae, S.H. CT, MR, (18)F-FDG PET/CT, and their combined use for the assessment of mandibular invasion by squamous cell carcinomas of the oral cavity. Acta Radiol. 2010, 51, 1111–1119. [Google Scholar] [CrossRef] [PubMed]
- Abd El-Hafez, Y.G.; Chen, C.C.; Ng, S.H.; Lin, C.Y.; Wang, H.M.; Chan, S.C.; Chen, I.H.; Huan, S.F.; Kang, C.J.; Lee, L.Y.; et al. Comparison of PET/CT and MRI for the detection of bone marrow invasion in patients with squamous cell carcinoma of the oral cavity. Oral Oncol. 2011, 47, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.H.; Chien, C.Y.; Lin, W.C.; Fang, F.M.; Wang, P.W.; Lui, C.C.; Huang, Y.C.; Hung, B.T.; Tu, M.C.; Chang, C.C. A comparative study of fused FDG PET/MRI, PET/CT, MRI, and CT imaging for assessing surrounding tissue invasion of advanced buccal squamous cell carcinoma. Clin. Nuclear Med. 2011, 36, 518–525. [Google Scholar] [CrossRef]
- Pentenero, M.; Cistaro, A.; Brusa, M.; Ferraris, M.M.; Pezzuto, C.; Carnino, R.; Colombini, E.; Valentini, M.C.; Giovanella, L.; Spriano, G.; et al. Accuracy of 18F-FDG-PET/CT for staging of oral squamous cell carcinoma. Head Neck 2008, 30, 1488–1496. [Google Scholar] [CrossRef]
- Qiao, X.; Liu, W.; Cao, Y.; Miao, C.; Yang, W.; Su, N.; Ye, L.; Li, L.; Li, C. Performance of different imaging techniques in the diagnosis of head and neck cancer mandibular invasion: A systematic review and meta-analysis. Oral Oncol. 2018, 86, 150–164. [Google Scholar] [CrossRef]
- Liao, C.T.; Chang, J.T.; Wang, H.M.; Ng, S.H.; Hsueh, C.; Lee, L.Y.; Lin, C.H.; Chen, I.H.; Huang, S.F.; Cheng, A.J.; et al. Pretreatment primary tumor SUVmax measured by FDG-PET and pathologic tumor depth predict for poor outcomes in patients with oral cavity squamous cell carcinoma and pathologically positive lymph nodes. Int. J. Radiat. Oncol. Biol. Phys. 2009, 73, 764–771. [Google Scholar] [CrossRef]
- Morand, G.B.; Vital, D.G.; Kudura, K.; Werner, J.; Stoeckli, S.J.; Huber, G.F.; Huellner, M.W. Maximum Standardized Uptake Value (SUVmax) of Primary Tumor Predicts Occult Neck Metastasis in Oral Cancer. Sci. Rep. 2018, 8, 11817. [Google Scholar] [CrossRef] [PubMed]
- Werner, J.; Hullner, M.W.; Rupp, N.J.; Huber, A.M.; Broglie, M.A.; Huber, G.F.; Morand, G.B. Predictive Value of Pretherapeutic Maximum Standardized Uptake Value (Suvmax) In Laryngeal and Hypopharyngeal Cancer. Sci. Rep. 2019, 9, 8972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, W.; Zhang, W.B.; Yu, Y.; Wang, Y.; Mao, C.; Guo, C.B.; Yu, G.Y.; Peng, X. Risk factors for free flap failure: A retrospective analysis of 881 free flaps for head and neck defect reconstruction. Int. J. Oral Maxillofac. Surg. 2017, 46, 941–945. [Google Scholar] [CrossRef] [PubMed]
- Sekine, T.; Barbosa, F.G.; Delso, G.; Burger, I.A.; Stolzmann, P.; Ter Voert, E.E.; Huber, G.F.; Kollias, S.S.; von Schulthess, G.K.; Veit-Haibach, P.; et al. Local resectability assessment of head and neck cancer: Positron emission tomography/MRI versus positron emission tomography/CT. Head Neck 2017, 39, 1550–1558. [Google Scholar] [CrossRef]
- Brown, J.S.; Lowe, D.; Kalavrezos, N.; D’Souza, J.; Magennis, P.; Woolgar, J. Patterns of invasion and routes of tumor entry into the mandible by oral squamous cell carcinoma. Head Neck 2002, 24, 370–383. [Google Scholar] [CrossRef]
- da Silva, S.D.; Morand, G.B.; Alobaid, F.A.; Hier, M.P.; Mlynarek, A.M.; Alaoui-Jamali, M.A.; Kowalski, L.P. Epithelial-mesenchymal transition (EMT) markers have prognostic impact in multiple primary oral squamous cell carcinoma. Clin. exp. Metastasis 2015, 32, 55–63. [Google Scholar] [CrossRef]
- Morand, G.B.; Ikenberg, K.; Vital, D.G.; Cardona, I.; Moch, H.; Stoeckli, S.J.; Huber, G.F. Preoperative assessment of CD44-mediated depth of invasion as predictor of occult metastases in early oral squamous cell carcinoma. Head Neck 2019, 41, 950–958. [Google Scholar] [CrossRef]
- Ngo, D.C.; Ververis, K.; Tortorella, S.M.; Karagiannis, T.C. Introduction to the molecular basis of cancer metabolism and the Warburg effect. Mol. Biol. Rep. 2015, 42, 819–823. [Google Scholar] [CrossRef]
- Baschnagel, A.M.; Wobb, J.L.; Dilworth, J.T.; Williams, L.; Eskandari, M.; Wu, D.; Pruetz, B.L.; Wilson, G.D. The association of (18)F-FDG PET and glucose metabolism biomarkers GLUT1 and HK2 in p16 positive and negative head and neck squamous cell carcinomas. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2015, 117, 118–124. [Google Scholar] [CrossRef]
- Tian, M.; Zhang, H.; Nakasone, Y.; Mogi, K.; Endo, K. Expression of Glut-1 and Glut-3 in untreated oral squamous cell carcinoma compared with FDG accumulation in a PET study. Eur. J. Nucl. Med. Mol. Imaging 2004, 31, 5–12. [Google Scholar] [CrossRef]
- Uccello, M.; Malaguarnera, G.; Vacante, M.; Motta, M. Serum bone sialoprotein levels and bone metastases. J. Cancer Res. Ther. 2011, 7, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, A.; Alho, I.; Casimiro, S.; Costa, L. Bone remodeling markers and bone metastases: From cancer research to clinical implications. BoneKEy Rep. 2015, 4, 668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edge, S.B.; Compton, C.C. The American Joint Committee on Cancer: The 7th edition of the AJCC cancer staging manual and the future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | All Patients No. of Patients = 84 | Bone Invasion No. of Patients = 47 | No Bone Invasion No. of Patients = 37 | p Value 1 B vs. nB | |
|---|---|---|---|---|---|
| Age | |||||
| Years | Mean (SD) | 67.3 (11.0) | 69.3 (11.5) | 64.7 (9.9) | 0.055 |
| Gender | |||||
| Male | No. (%) | 52 (61.9%) | 26 (55.3%) | 26 (70.3%) | |
| Female | No. (%) | 32 (38.1%) | 21 (44.7%) | 11 (29.7%) | 0.182 |
| Smoking | Yes (%) | 43 (51.2%) | 21 (44.7%) | 22 (59.5%) | |
| No (%) | 41 (48.8%) | 26 (55.3%) | 15 (40.5%) | 0.195 | |
| Alcohol consumption | Yes (%) | 42 (50.0%) | 19 (40.4%) | 23 (62.2%) | |
| No (%) | 42 (50.0%) | 28 (59.6%) | 14 (37.8%) | 0.128 | |
| cT-classification | |||||
| T1-T2 | No. (%) | 22 (26.2%) | 8 (17%) | 14 (37.8%) | |
| T3 | No. (%) | 5 (6.0%) | 0 | 5 (13.5%) | |
| T4 | No. (%) | 57 (67.8%) | 39 (83%) | 18 (48.7%) | 0.007 |
| pT-classification | |||||
| T1-T2 | No. (%) | 28 (33.3%) | 0 | 27 (73%) | |
| T3 | No. (%) | 3 (3.6%) | 0 | 3 (8.1%) | |
| T4 | No. (%) | 53 (63.1%) | 47 (100%) | 7 (18.9%) | <0.001 * |
| pN-classification | |||||
| N0 | No. (%) | 41 (48.8%) | 18 (38.3%) | 23 (62.2%) | |
| N1 | No. (%) | 17 (20.2%) | 8 (17%) | 9 (24.3%) | |
| N2a-b | No. (%) | 22 (26.2%) | 18 (38.3%) | 4 (10.8%) | |
| N2c-N3 | No. (%) | 4 (4.8%) | 3 (6.4%) | 1 (2.7%) | 0.023 |
| FDG-PET | |||||
| SUVmax primary tumor | Median (IQR) | 14.1 (10.6–17.5) | 15.9 (11.1–18.9) | 13.0 (8.1–16.0) | 0.015 * |
| Variable | Histopathological Examination | ||
|---|---|---|---|
| Clinical examination | TP | FP | Sensitivity |
| 40 | 19 | 67.8% | |
| FN | TN | Specificity | |
| 7 | 18 | 72.0% | |
| Computed tomography (CT) | TP | FP | Sensitivity |
| 13 | 1 | 72.2% | |
| FN | TN | Specificity | |
| 5 | 11 | 91.6% | |
| Magnetic resonance imaging (MRI) | TP | FP | Sensitivity |
| 28 | 6 | 73.3% | |
| FN | TN | Specificity | |
| 8 | 19 | 76.0% | |
| SUVmax primary tumor < 9.5 | TP | FP | Sensitivity |
| 41 | 22 | 97.6% | |
| FN | TN | Specificity | |
| 1 | 10 | 31.2% | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stalder, S.A.; Schumann, P.; Lanzer, M.; Hüllner, M.W.; Rupp, N.J.; Broglie, M.A.; Morand, G.B. Value of SUVmax for the Prediction of Bone Invasion in Oral Squamous Cell Carcinoma. Biology 2020, 9, 23. https://doi.org/10.3390/biology9020023
Stalder SA, Schumann P, Lanzer M, Hüllner MW, Rupp NJ, Broglie MA, Morand GB. Value of SUVmax for the Prediction of Bone Invasion in Oral Squamous Cell Carcinoma. Biology. 2020; 9(2):23. https://doi.org/10.3390/biology9020023
Chicago/Turabian StyleStalder, Stephanie A., Paul Schumann, Martin Lanzer, Martin W. Hüllner, Niels J. Rupp, Martina A. Broglie, and Grégoire B. Morand. 2020. "Value of SUVmax for the Prediction of Bone Invasion in Oral Squamous Cell Carcinoma" Biology 9, no. 2: 23. https://doi.org/10.3390/biology9020023