

Applying Integrative Systems Methodology: The Case of Health Care Organizations
1
Institute of Management and Strategy, University of St. Gallen (HSG), 9000 St. Gallen, Switzerland
2
Landeskrankenhaus Klagenfurt, A-9020 Klagenfurt, Austria
*
Author to whom correspondence should be addressed.
Systems 2024, 12(4), 140; https://doi.org/10.3390/systems12040140
Submission received: 28 February 2024
/
Revised: 12 April 2024
/
Accepted: 17 April 2024
/
Published: 22 April 2024
(This article belongs to the Special Issue The Systems Thinking Approach to Strategic Management)
Abstract
:Systems thinking has a lot to offer to the field of strategizing. Calls for a greater use of the Systems Approaches to management are increasingly being advanced in the world of organizations, public and private. Yet, practical implementation of such postulates is lagging. This article aims to demonstrate the potential of systems thinking in shaping strategy in management and organization. It builds on a framework known as Integrative Systems Methodology, a circular set of established components of strategic processes: all elements of the methodology are covered, from finding purpose and goals, modeling, and diagnosing to the design of strategies and change. Along this path, complementary methodologies are combined to cope with high environmental complexity. In the present case, these are the systems methodologies of Organizational Cybernetics (namely Viable System Model) and System Dynamics. The layout of the treatise is conceptual in nature. Nevertheless, long-term empirical evidence from a set of real-world organizations-one center and several peripheral healthcare entities-is presented to make the methodology tangible: theoretically grounded and experientially corroborated. The case study we are introducing is from health care, concretely: an oncological care system. Structural patterns are elicited, which are isomorphic, applicable to any health care system. From a conceptual-theoretical stance, crucial factors conducive to continuous organizational learning are elaborated. Professionals can benefit from acquiring new ways of coping with the ever-increasing complexity.
1. Call for Cybersystemics
The strategic management of organizations faces growing challenges. The environments are showing increased uncertainty, interconnectedness, and dynamics. Crises are manifold from local to global. And issues are often intransparent, given their complexity. Problems at all levels of organizations and society abound. Consequently, calls and arguments for using cybersystemics—methods based on systems theory and cybernetics—to cope with these complex challenges have become frequent.
Advocates argue that the systems approach delivers problem-solving methods or methodologies that excel the other (“non-systemic”) approaches, in contexts of complexity [1,2,3]. Among the major advantages attributed to systemic methodologies, is that they provide holistic, integrative perspectives, combine analysis with synthesis and supply vehicles for transdisciplinary inquiry. Critics interject that the systems approach is too abstract, too general, and does not provide any handles for triggering change in the real world (e.g., [4,5]. These arguments have been superseded. Systemic methodologies have shown their potential to analyze problems and to influence the dynamics of social systems (e.g., [6,7,8,9,10,11]. Other criticisms maintain that managerial cybernetics is mechanistic and reductionist [12]. That view ignores the fact that cybernetics of organizations exists, which addresses social systems with their self-organizing, self-conscious properties [13,14].
One must add that the theoretical basis underlying cybersystemic methodologies is well-established, already by the founding fathers of system theory and cybernetics [15]. To take one more recent example, for many, the eminent systems scientist Mike Jackson attributes “enormous explanatory power compared with the usual analyses carried out in organizational theory” to the Viable System Model (VSM), a much-used instrument of organizational diagnosis and design, which rests upon the science of cybernetics [16] (p. 174).
This article is a contribution to systemic strategizing. It is based on our earlier work, of which it is a logical continuation, in particular [17]. The present, novel version is an improved, but also abridged record of the Integrative Systems Methodology [18,19]. The paper has been reframed and improved, and it leads to new insights, for example in its focus on application, while the piece from 2017 covered the conceptual–methodological aspect in greater detail. Our work adheres to an evolutionary concept of theory-building, which adopts a long-term perspective, and rests on gradual improvement and cumulative knowledge building.
The title of this article may seem too general. However, in search of invariant patterns, we are using models crafted for the discovery of invariances. Our assumption is one that is characteristic of systems theory, namely that certain structural phenomena, in the sense of isomorphisms, apply to many objects of a set or, more specifically, class. According to Beer’s theory, the structure of the VSM specifies the necessary and sufficient preconditions for viability of any organization. That includes health care organizations of any type. If that theory holds, then the VSM is appropriate for a structural diagnosis of any one of these.
The text is organized as follows. A methodological framework will be presented: Integrative Systems Methodology (ISM), with the lead distinction Content/Context. The next two sections are dedicated to each one of these dimensions. First the content loop with five subsections addressing Purpose and Goals, Modeling, Diagnosis, Design, Change. Second, the context loop, following the same categories, but in a more condensed form. The chiefly analytical article is then concluded with a final synthesis.
2. Methodological Framework
2.1. Concepts and Sources
We will make use of the conceptual framework of Integrative Systems Methodology (ISM). This is a systemic framework designed to help managers in coping with organizational complexity, or, more precisely, to attain requisite variety in relation to confronted problems.
“Variety” is a measure and a synonym for “Complexity”, simplified but useful. The concept of “Requisite Variety” stems from the cybernetician Ross W. Ashby. The condensed version of Ashby’s Law of Requisite Variety is “Only variety absorbs variety” [20]. (The verb “absorb” was substituted for the original “destroy”, by Stafford Beer [21] (p. 89). We decided to use this concept of “complexity”, because it fits the needs of management-related applications, and because it is the conceptual basis for the theory of the VSM, which is a basis for this article. However, we would point out that there are many concepts of complexity. Gell-Mann [22] discusses those grounded in physics and information theory. Mitchell [23] provides definitions of “complex system” in the tradition of research into complex adaptive systems. Rescher [24] gives a systematic overview of the concepts of complexity from multiple perspectives. He reflects on the managerial topic of coping with complexity, raising a fundamental issue: “problem complexity outpaces solution complexity” (p. 177).
The article’s focus is on the long term, and therewith at the vantage point of strategic and normative management. The attribute “systemic” is used in this context to denote that the framework is grounded in systems theory and cybernetics, the science dedicated to holistic or integrative management in the face of organizational complexity. The management of complexity is a pivotal topic in Organizational Cybernetics and systems thinking (e.g., [2,21,25,26,27,28,29,30,31].
The ISM framework is a vehicle for combining qualitative and quantitative methods of dealing with organizational complexity. This framework has been tested in several settings, some of which are documented in published case studies (e.g., [18,19,32].
There are other “multimethodological” frameworks with similar aims [17,30]. In positioning ISM among the variety of pertinent approaches, two aspects stand out. Firstly, it addresses the need of organizational and human agents to achieve requisite variety, i.e., a repertory of potential behaviors that is commensurate with the variety of the situation or the agents it is confronted with. Secondly, ISM, albeit being open to the inclusion of different methods both quantitative and qualitative, has been focusing on two highly complementary methodologies that are combined in a rigorous manner. One is the Viable System Model (VSM), a product of Organizational Cybernetics [2,21,31,33], and the other one being System Dynamics (SD), which is a discipline and methodology of dynamic modeling and simulation [34,35,36,37]. Both are at the core of the methodological repertory grounded in system theory and cybernetics. These two aspects indicate the use of ISM in the context of the case to be studied here. A briefing on both SD and VSM can be found in the Appendix A.
2.2. Integrative Systems Methodology
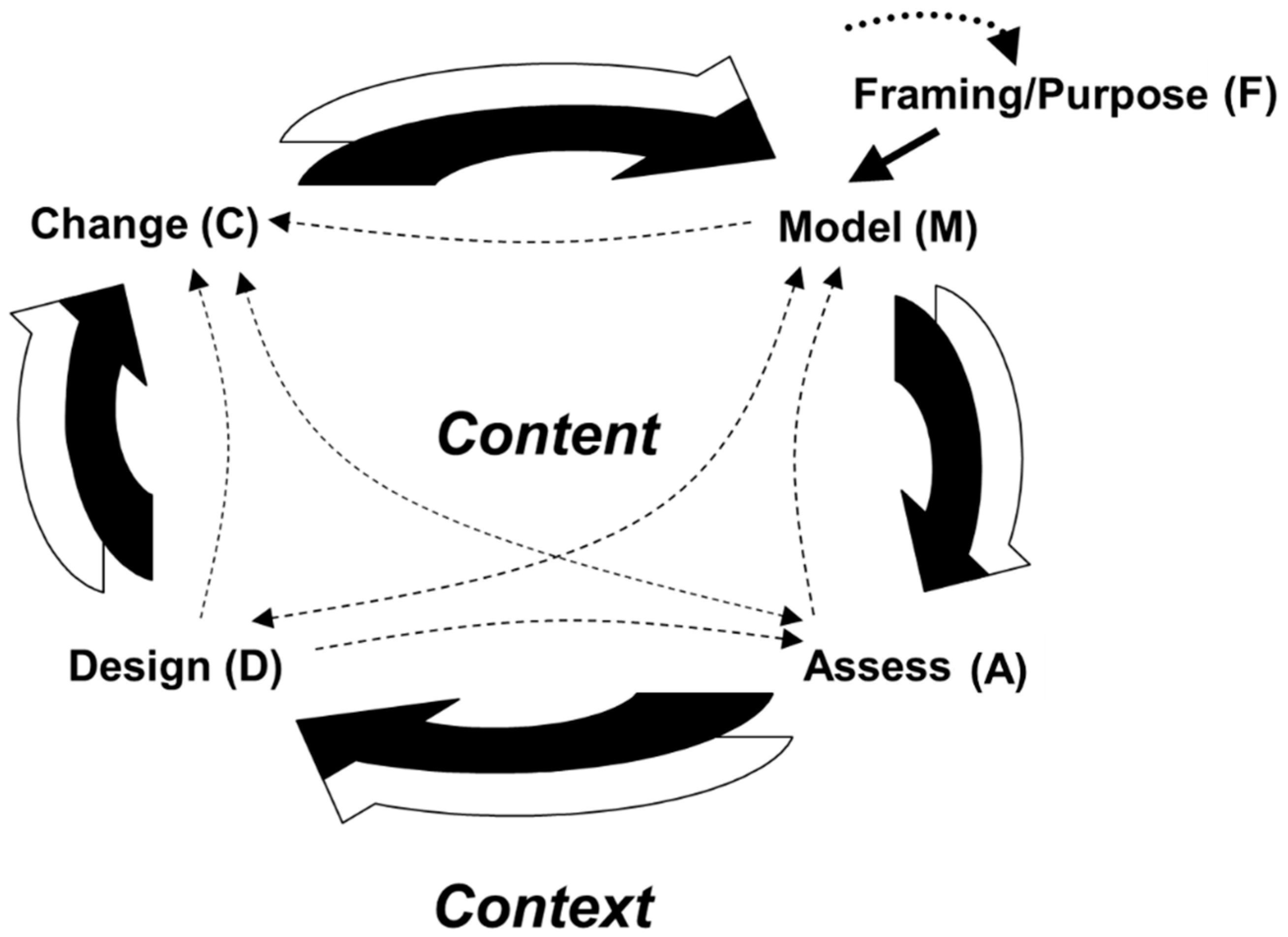
Integrative System Methodology (ISM) is a heuristic framework. “Heuristic” can best be translated as “the art of finding”. Stafford Beer defines “heuristic”, a contraction of “heuristic method”, as “a set of instructions for searching out an unknown goal by exploration, which continuously or repeatedly evaluates progress according to some known criterion” [31] (p. 402). ISM enables problem solvers to enhance their behavioral repertoire (cybernetically: “variety”; [20]) in coping with complex issues or problems. When dealing with complex phenomena, the procedure typically adopted follows a set of steps forming a circular shape (Figure 1). The point of origin is a perspective, i.e., a conceptual frame of the issue at hand, and, for dealing with it, a purpose or “overall goal”, followed by a set of phases:
- -
- Modeling (formal or informal representation of the issue under study)
- -
- Assessment (diagnosis, evaluation of current situation)
- -
- Design (strategies, structures, etc., needed to solve the problem or improve the situation)
- -
- Change (of the system).
For details, see [18,38].
![Systems 12 00140 g001]()
Figure 1.
An Integrative Systems Methodology for dealing with complex issues—process diagram.

This scheme was inspired by earlier works of the cybernetician Raúl Espejo [39] and associates (e.g., [40]), namely his Cybernetic Methodology, and by the postulate to study content, context and process of change, as formulated by the organization scientist Andrew Pettigrew [41] (p. 50).
From dealing with complex organizational processes, such as the one developed here, an important insight has emerged: in rather complex cases, the process and the problem solution must be developed at two levels, content, and organizational context. If one works only on the content, the problem solution will probably be realized defectively. If only context is considered, a dearth of knowledge for providing good solutions will likely occur. To distinguish the two dimensions, the arrows in Figure 1 are two-colored. The process is denoted by these arrows. It has a long-term perspective, i.e., it is a process of strategizing.
With “content” we are referring to the activities or operations of the system under study, and with “context” we are referring to the structural and cultural frame into which it is embedded. Content is about what the system “does”, context is about how it organizes itself (or how it is organized). Both dimensions require different conceptual tools for dealing with complexity. In the following we will use two systemic methodologies, System Dynamics modelling at the content level, and cybernetic modelling for context. An overview of these complementary methodologies is given in the Appendix A.
In the following, the abbreviations used for the phases in the diagram—F (Framing), M (Modeling), A (Assessment), D (Design), C (Change)—will be used to denote the sections of the case study.
2.3. Epistemological Aspects
The relevance of systems thinking for the practice of strategizing has been demonstrated for many years and has become visible in case studies [43,44], including the one presented here. The theoretical harvest of that practice is manifested in several dimensions. The theory of strategic management can benefit from the insertion of systemic methods in its methodical repertoire.
The Integrative Systems Methodology which we are drawing from here has proven useful in dealing with issues requiring a long-term perspective, such as strategy and normative management [18,19]. In line with the growing need for multimethodological approaches [30], users of ISM have followed a logic of integrating complementary methods, e.g., from Organizational Cybernetics and System Dynamics [45]. We know, from informal contacts with former students, that this approach is gaining momentum, but we cannot prove it. The ISM framework is highly abstract. We have not been in a position to pursue its implications for practice systematically.
Epistemologically, the discipline of strategy adheres to the theory of correspondence, which defines truth as the maximal accord of model and reality. The systemic perspective adds to the theory of consensus, which relies on the assumption that a statement is true, if it is generally accepted between the parties involved. The multi-agent approach used here in modeling to elicit the relevant perspectives (Table 1) provides a handy method, which could also be transposed to diagnosis and design.
Ontologically, the systemic methods rest on the assumption that the characteristics of social systems are complexity, inter-relatedness, uncertainty, and nonlinearity. These aspects are present in all phases of systemic strategy-making. This will also be apparent in the following case study.
3. Case Study Part I–Framing (F)
This is an abridged version of a long case study published earlier (Schwaninger & Klocker 2017a) [46], which covered applications of both the Viable System Model and System Dynamics in an organization for health care. This version does not contain an account of the SD application, which is contained in [47].
The case is about a group of pioneers, led by DDr. Johann Klocker (JK), who developed a system of oncological care covering the entire state of Carinthia in Austria. The case ranges from 1985, when JK started building the system from scratch, to 2015, when JK formally retired. In fact, he is still clinically active in that oncological care system (OCS) now (2023). Near the mid-eighties, JK was put in charge of building an oncological care unit situated in the department of internal medicine at the central hospital (Landeskrankenhaus, in short “LKH”) in Klagenfurt, the capital of Carinthia, one of the nine federal states of Austria. Over the ensuing 30+ years, JK pioneered and directed the development of an OCS covering the whole state and involving 10 hospitals as well as multiple local physicians. He managed that system over all these years and is the main source of information for this case study. JK called on this author (MS), who is an organization scientist, to help him conceptually, as a consultant and coach, a role that he continues to hold (until 2015 and beyond). According to JK, much of the successful evolution of that health care system is due to that cooperation. Normally, MS did not appear in front of the staff of the unit, except at certain internal conferences and workshops, for talks and discussions related to the organization and leadership of the system under development.
Over several decades, health care systems all over the world have been grappling with a formidable challenge. The issue was providing an integral kind of care, with the patient at the center, rather than technology or doctors. Traditionally, over the last four or five decades, hospitals had increasingly suffered from an orientation that hinged on over-specialization and splintered forms of organization. This orientation threatened the quality of medical care because patients tended to be treated in a fragmentary way. The perspective on sick people is as if they were conglomerates of organs that can be treated in isolation. The focus was on symptoms. Health care systems often lack the ability to deal with syndromes that can have multiple causes with complex interrelationships. Normally, the main concern is applying high technology and advanced medication, instead of warranting patients’ quality of life.
These deficits have provoked calls for a holistic kind of treatment. The systemic, integrative properties of such an approach to medicine had been under-researched because it transcends the silos of research organizations.
Hence, our research question is “how must health care systems be designed to achieve viability, or, more concretely, to become both efficient and effective while also maintaining their identity in the long run?” The issue here is building a system that provides patient-centered care of excellent quality and at a bearable cost. It became clear soon that the new OCS would necessarily use all available therapeutic modalities and infrastructure, in a sequential or combined mode, customized to each specific case. It would rather be a networked knowledge organization, not a hierarchy of silos as many of the extant health care systems.
In this article, we will explore an exemplar of a long-term process aimed at achieving a holistic system design of a viable health organization.
3.1. Framing: Purpose and Overall Goals (F)
JK and the directors of the state health authority, with the directors of the LKH Klagenfurt, shared a common vision. They defined the purpose of Oncology Carinthia as a health system that should provide the highest possible level of oncological care covering the whole country. They then agreed upon three general goals:
- (a)
- Guarantee of excellent oncological care in the context of the central hospital, using all the resources available within that powerful institution.
- (b)
- Provision of fast and high-level care for oncological patients all over the federal state, i.e., also outside the capital—in small towns and in the countryside, as far as possible “on the spot”.
- (c)
- An increasingly preventive orientation of oncological medicine in Carinthia.
Shortly thereafter, in a conversation between JK and the general manager of the LKH towards the end of 1984, the two agreed on the build-up of an oncological care unit centered in Klagenfurt. This would comprehend an allotment of beds for intensive therapeutic situations as well as an ambulatory where patients could be treated, and, once therapy was concluded, receive aftercare.
Subsequently, the LKH management endowed JK with the mission of building a consultation service involving other hospitals.
3.2. Mapping the System at the Outset (M)
Carinthia covers an area of 9500 square kilometers and had about 500,000 inhabitants at the time. The socio-geographic structure was “healthy”, with no excessive urban concentrations. Besides the capital Klagenfurt (86,000 inhabitants in 1985, 102,000 in 2022), several district centers exhibited their own lively economic, social, and cultural activities. Altogether, Carinthia had 13 hospitals potentially apt to be included in a network for oncological care; 10 became part of it. The number of independent physicians included about 20 internists, of which only one specialized in oncology. Many of them were also candidates for joining the network, to provide supportive care.
4. Case Study Part II–Content Level
The development of the OCS, from its build-up to maturity, spanned the years 1985 to 2015. This phase includes the formation and evolution of the oncological care system, and its successful operation over a quarter of a century: a long history of dealing with complex challenges.
4.1. Vision to Models (M)
Under the keyword “content”, the substantive issues and decisions concerning the establishment of the OCS will be addressed. This is about “what the system does” and how it functions.
Early on, JK and MS drew a first model, using the methodology of qualitative System Dynamics, to provide an overview of the most important factors making up the system in focus, and their dynamic interrelationships. Their aim was first to understand and assess “how the system ticks”. Secondly, they wanted to discover priorities and levers for the design of the system.
They attempted to elicit the relevant perspectives on the system in focus. The schema in Table 1 distinguishes the main stakeholder groups (“interest groups”) and their goals with respect to the system in focus. Then, the key factors, i.e., aspects that are critical for the attainment of these goals, are ascertained.
The goals and key factors in this stakeholder analysis stand for components, potential variables or parameters that may constitute a model of the system under study, such as the one in Figure 2: that is a causal loop diagram (CLD). CLDs are devices stemming from System Dynamics, a methodology for modelling and simulation, going back to Prof. Jay Forrester; see [34,37,48]. These are diagrams for qualitative representations giving a first idea of the dynamics of a system, e.g., an organization.
In the diagram, arrows denote causal relationships, and signs show the directions of these relationships. All arrows that carry a negative sign denote that the two connected variables point in opposite directions: e.g., more personnel turnover leads to less productivity (and less personnel turnover leads to more productivity). All arrows not provided with signs implicitly show connections of variables pointing in the same direction, e.g., more quality of care entails higher success of care. To make generally correct the statement “X and Y move in the same [opposite] direction”, a more precise formulation is necessary: “If X increases, Y increases above [below] what it would have been” [49]. The diagram shows nine reinforcing (“R”) and three balancing (“B”) loops. The polarity of a loop is the result of multiplication of all signs in that loop. Loops with even numbers of negative signs are always reinforcing (e.g., Loop R1 [zero minuses]: “+” * ”+” = “+”; Loop R8 [two minuses]: “+” * ”−“ * ”−” * “+” …). Loops with uneven numbers of negative signs are always balancing (e.g., Loop B1: “+” * “−“ * “+” = “−“). Reinforcing loops promote either an increase or decrease, both of which, if not attenuated at some point, will entail destabilization eventually. Balancing loops lead to attenuation, and potentially to equilibrium. The benefit of distinguishing these two kinds of loops is that those dynamics can be ident—ified which make the system develop on the one hand, and which lead to a balance of the system on the other hand. For technical details, see [37].
The number of reinforcing loops (nine) is higher than that of the balancing loops (three), because Oncology Carinthia is still in an early phase, heading for development. The interpretation of these loops uncovers meaningful interconnections. For example: R1 is the core loop, a “motor”, where a patient’s quality of life is a function of quality of care entailing successful care. The quality of life for patients dynamizes the success of care because patients can contribute more to the healing process, and to a positively spirited milieu.
4.2. Assessment/Diagnosis (A, D)
The idea of the champions was, first of all, to set the norm to enable an excellent level of care (including quality, reliability and high speed). Strategically, that care had to be delivered locally, i.e., be as decentralized as possible, and central only where absolutely necessary, with intelligent use of all available resources.
There were problems ahead:
- Resistance of medical departments that should join the effort;
- Weak know-how and lack of interest among the peripheral hospitals;
- Deficits of knowledge among the independent physicians;
- Fear among doctors and nursing staff of increasing demands and uncertainties;
- Low motivation among staff;
- No formal authority among oncologists about parties that should be included;
- Scarce budgetary means;
- Limited personnel capacity in the central oncology unit;
- Low interest, among authorities, in preventive care.
In the face of these issues, the challenges presented themselves as follows:
- Winning the cooperation of medical departments at the Klagenfurt and peripheral hospitals;
- Multiply know how and enhance knowledge-building in the peripheral hospitals;
- Involve and link multiple resources;
- Create robust and nimble structures to enhance the viability of the oncological care system;
- Information management—make data and information available for the control of therapies and the creation of new therapy options;
- Balance decentralized and centralized care;
- Balance the efficiency of care operations and the effectiveness of care strategies.
In sum, the venture ahead was very demanding: a high diversity of tasks had to be achieved, distributed human and technical capacities had to be networked skillfully, flexibility was to be built, and the restriction of high scarcity of resources had to be considered.
4.3. Design and Change (D, C)
The diagram in Figure 2 above reveals tangible dynamic features. The next question is “which are the levers to improve the system in line with the purpose and goals as defined at the outset?”.
Model analysis directed our attention to three main levers, (a) psycho-hygiene for the staff, (b) structures, information systems and knowledge management, and (c) leadership (bold parameters in Figure 3). The kinds of interventions chosen thereupon were not a result of the CLD per se, but they emerged in the champions’ ongoing discussion of challenges and pertinent responses. The CLD made the “mechanisms” driving the system under study transparent. Hence, it was a vehicle for keeping that discourse going. In the ensuing efforts the identified levers were put into practice in sophisticated ways, as will be shown.
These levers have the character of strategic parameters with great potential:
- (a)
- Psycho-hygiene: The staff in oncological care are subject to a stress load that tends to be greater than in other professions. Therefore, introducing psycho-hygienic measures was crucial, to sustain and foster the psychic health of people, adopting both preventive and restitutive measures.
- (b)
- Structure, information system and knowledge management: Structure is a powerful device that was considered crucial for strengthening the quality of care, coordination, and team cohesion. In addition, information systems and knowledge management were prominent in strengthening research.
- (c)
- Leadership: Ultimately everything in an organization is subject to the influence of leadership and hinges on its quality. Motivation as well as coordination and cohesion were identified as two main aspects to be strengthened by that driver. Coordination and cohesion then impinge strongly on cooperation. Equally crucial was a major effort to win the cooperation of all necessary parties.
5. Case Study Part III–Context Level
5.1. Master Structure (D)
Under the keyword “context”, the issues of structure and leadership in the OCS will be addressed. These concern the aspects which define how the system under study is directed and organized (or organizes itself) to make viable “what the system does”.
The structural diagnosis and design of the OCS was of primary importance in the evolution of that system. Structure is not merely the expression of a state, for it changes behavior. And change was needed if the OCS was going to take shape. Structure and other levers were the components we could manipulate directly. Many of the factors that constitute the competencies of the organization could be influenced only indirectly. This becomes visible when following the arrows in Figure 4. For example, leadership cannot influence quality of care directly, but indirectly, e.g., by strengthening the motivation of the staff.
Soon after embarking on the new venture, we used a powerful cybersystemic device of organizational diagnosis and design, already introduced above: Stafford Beer’s Viable System Model (in short “VSM”; [2,21,31,33]). That model is extraordinary in that it claims to define not only the necessary but also sufficient structural preconditions for the viability of any organization. The model has been tested in multiple case studies, for an overview see [27,50], and in two surveys [50,51]. After Beer’s original works, other authors have made methodological contributions to facilitate the application of the VSM, e.g., [40,52,53,54,55,56,57]. A remarkable contribution to the application of the VSM in the health sector is [58].
To facilitate comprehension of the model, the following description is supplemented by a graphic in the Appendix A. As a theory, the VSM is distinctive in several respects, in view of the claim it makes. This theoretical claim is as follows:
A social system is viable if, and only if, its structure fulfils several requirements, which the theory specifies. Concretely, according to the model, an organization is viable if, and only if it disposes of five component managerial subsystems and their interrelationships, as set forth by the theory:
- (1)
- Component 1. Management of a basic subsystem (an “operation”).
- (2)
- Component 2. Coordination of subsystems, attenuation of oscillations between them.
- (3)
- Component 3. Integrative management of a collective of subsystems.
- (4)
- Component 3*. Auditing and monitoring channel.
- (5)
- Component 4. Management for the long term, relationships with the overall environment.
- (6)
- Component 5. Normative management, corporate ethos.
Any deficit in this structure will inevitably prejudice the viability of the organization. It must be added that the structure, outlined here only in a rudimentary form, is recursive: also, subsystems (e.g., divisions) and super systems (e.g., a holding) should be structured in accordance with the same principles. This theory has strong implications. It opens a new perspective on organizational diagnosis and design: any deficiencies in this system, such as missing functions, insufficient capacity of the functions or faulty interaction between them impair or endanger the viability of the organization.
The exceptional strength of the claim of the VSM lies in that not only necessary but sufficient structural preconditions for the viability of a social system are established, according to the theory of the VSM. To the best of the author’s knowledge, no other organizational theory makes a claim as strong as this one.
One would expect that evidence has been found that contradicts the VSM’s claims. The surprising fact is, however, that the model has not been falsified. On the contrary, it has been corroborated by the growing empirical evidence from VSM applications (see above).
The VSM is a device for both diagnosis and design. In the case discussed here, it was rather used in the design mode, than in the diagnostic mode, because the OCS was constructed from zero upward.
Figure 4 visualizes the structure of the OCS as implemented within three years. The power of recursive organization design is visible from the diagram: the organization unfolds its capacity to absorb environmental complexity along the fronts where that complexity emerges. Thus, the organization can respond effectively.
The circles represent primary units, i.e., basic units with their regulatory capacity at different organizational levels, Oncology Carinthia, Oncology Regional Hospital, etc. The structure is recursive: colored versions of the structural components of a viable system (as listed above) are shown in each one of the primary units. The fundamental structure repeats itself along the different planes. A verbal and mathematical representation of the VSM can be found in [11].
In Table 2, a schema is presented which reflects a paragon for the structure of Oncology Carinthia, as designed and implemented for putting the strategy in place.
A system in focus is a unit of oncological care at any level of recursion. In other words, the overall health system is outside the influence of JK and will only marginally affect his area of responsibility. At the first level (recursion w), the system in focus is the whole OCS of Carinthia. At the next recursion level (x), it is the oncology in a region, e.g., Klagenfurt, Villach or Wolfsberg, where it is centered around the central district hospital (LKH) and other local clinics. Finally, at recursion level y, the system in focus is an oncology station such as a tumor ambulatory or a subsystem of the internist’s ward.
Basic units are the individual hospitals, but individual local oncologists also can have such a function, normally at recursion x, when they assume full responsibility for the therapy or aftercare of a patient. In the case of recursion y, the structure is based on teams, or systems of interaction, if we take—with Luhmann [59]—communications as the primary components of systems. The basic unit here (recursion z) is not a doctor or a patient, but a connection of four components, namely, patient and family, doctor and nurse. Each one is an integral part of the therapy team, but none is only a member of that unit. Doctors and nurses are also members of other similar teams, just as the patient and the family are at the same time members of other social systems.
To highlight some of the features outlined in Table 2, we will mainly comment on the innovative aspects, and will revert to all four recursion levels.
Component 1: A remarkable feature of the local management (Component 1) in recursion y is a reversal of the conventional arrangement: the management function, i.e., the primary regulatory responsibility, is with patient and family. This corresponds to the emancipatory idea of valorizing the role of the patient, who becomes the main agent pursuing his or her health. Making this philosophy real requires—despite this declaration about structure—that the medical and nursing staff take a different view than is common in most healthcare systems. The patient is not a passive object to be manipulated according to expert considerations, but a force aligned with the joint quest for a successful treatment. This novel view did not emerge by itself. The champions played a crucial part in conveying the inherent values, via discourse and acting by example.
Component 2: A crucial role in coordination (Component 2) is with the tumor boards and councils (recursion x). These are virtual units. In many of the processes at the OCS, virtual forms of organization are adopted at the team level. Teams in the OCS are flexible in that they are formed as changing casts drawn from resource pools that exist in different locations. The resources are there, but the teams materialize in response to changing needs. They work across space, time, and organizational boundaries [60], reverting to personal contact, other communication media (mainly electronic connections), and information systems (e.g., tumor database)), in which the medical cases are discussed, with themes ranging from diagnosis to therapy. The cases treated by a tumor board vary in number and size; usually the therapies are defined by these boards. The Tumor Council is a kind of individualized Tumor Board (see below).
Other group initiatives are the oncology circle at recursion w and the coordination meetings of radiologists, hematologists, and pathologists at recursion x. This principle greatly increases the efficiency of oncological care. Finally, standard therapies, training, messaging, and the doctors’ letters edited by the Klagenfurt oncologists fulfil an important coordinative function.
Component 3: The executive management always involves oncologists and nursing staff. Only at the last recursion—z, which is not elaborated in detail, in Table 1—are the managers are patients and family.
The connection between local and executive managements (Components 1 and 3), at different recursions, makes use of the precious but very limited capacity of that vertical channel. Here is where the negotiation and control of goals as well as the allocation of resources, in addition to important feedback mechanisms and participation, take place.
Hospitals that do not have their own specialized oncologists benefit from a new service installed as a mobile unit. This is a resource of recursion w deployed for the hospitals at recursion x. The oncologists from Klagenfurt visit the peripheral hospitals. Until 2015, the journeys of the oncologists were almost entirely substituted by a teleconferencing system. The visits take place in a constant rhythm of one week (LKH Villach, LKH Wolfsberg, KH St. Veit) or two weeks (hospitals Spittal and Friesach), all others occurring as needed. The oncologists participate in the respective local tumor boards and now and then, if indicated, in the local tumor ambulatories. In this way they make their expertise available, therewith contributing to the quality of the decentralized operations. The idea here is that the doctor comes to the patient rather than the patient “feeding the system”. This concept is also constitutive for the profession of barefoot doctors in India. In addition, the mobile doctors are a vehicle for knowledge transfer, and indeed, the oncological know-how at the periphery has made great progress over the years. Meanwhile, the LKH Villach, LKH Wolfsberg and KH in St. Veit have hired their own oncologists. However, the regular teleconferences continue to take place.
Component 3*: The audit channel (Component 3*) comprehends direct forms of access to the basic units, e.g., at recursion w, the visits to local oncology units. At recursions x and y, the medical visits are crucial, because they give the professionals a first-hand impression of the local care situation, and the individual state of the patient. Also, informal communication and cohesion-building socio-cultural activities play a crucial role here at all levels.
Among the cohesion-building measures are the coffee breaks in the wards, the “onco-lunches” that gather OCS people of Klagenfurt and beyond, and the yearly oncology symposia which bring together oncologists from all over the state plus colleagues from the neighbor state Styria. These events fulfil both coordination and auditing functions. In certain cases, they might also contribute to the intelligence function.
Component 4: This intelligence function fulfils tasks ranging into the long term and the wider environment. These tasks are, in the first place, the concern of the OCS leader’s team, whose members are involved in the strategic development at all three levels of recursion: at recursion w as the pioneers and masterminds, at recursions x and y in support roles. In the latter, it is the managers/leaders of these recursions who are the designers of the long-term future of their units, making up development plans and providing their staffs with education for the future. The development of therapy strategies, going hand in hand with research activities and international activities in knowledge networks, is mainly in the hands of the OCS leaders at recursion w.
Component 5: Finally, the system’s identity, manifested in the ethos of the system, with normative management has become a systemic braid that connects members and organizational cultures of all recursion planes. Shared values, principles, vision, and mission are the same for all three recursion levels, but they need different people to enforce and exemplify them, namely, the leaders at each level.
In this structure, as shown in Table 2, one and the same unit often fulfils different roles with respect to the management components. For example, on recursion w the management team is active in both functions, executive management (Component 3) and strategic management (Component 4).
The structure outlined here is a network, and so it need not be emphasized that the activities therein involve various forms of networking and communication, from formal to informal and from personal to electronic. That network is crucial for the alignment of the views of multiple purposeful actors with different goals and interests. And it enables building a shared corpus of knowledge over time. Much of that knowledge is tacit know-how [61], embodied in the people and teams of the organization.
5.2. Team Organization (D)
In addition to the “master structure” just described, we will now delve, in more detail, into one crucial organizational feature mentioned, the teams at various levels. These are of three kinds.
First, the Therapy Team is the nucleus of the structure. These self-regulating teams are formed around each patient, as the primary units at recursion z. The care here is accomplished by the patient, his or her family, a medical doctor, and a nurse. Besides its therapeutic function, the team also engages in prevention, as far as possible. While the patient and family are members of that team only, the doctor and nurse are normally also part of other teams, around other patients. They are always virtually present in each of these teams, but physically present only at certain times.
Second, the Tumor Board at recursion x is a platform that manages the continuous flow of cases to be dealt with in each hospital. It also plays a role in the building of local knowledge. A Tumor Board is formed by members of different organizational units of different recursions (x and y, or even x, y and z). A Tumor Board meets regularly to investigate the current cases under treatment. The local oncologist, if extant—and if not, a mobile oncologist from the hub—as well as members of specialist departments (Surgery, Gynecology, Hematology, etc.), constitute that body. Whenever indicated, representatives of Therapy Teams join the Board. The interaction in Tumor Boards is supported by the latest communication technologies, for example if (additional) oncologists from the hub need to be involved selectively. The leadership of the Board is in the hands of an oncologist.
In the oncology at Klagenfurt (LKH)—recursion x—more than one Tumor Board has been formed. Cancer patients have their treatment across different specialized wards, gynecology and pneumology being two prominent examples. One of the oncologists moves from the LKH oncology unit to these departments, where he or she participates in visits to cancer patients, in this way forming a local Tumor Board, together with the local doctors in charge. This approach was later copied in the largest of the peripheral clinics, as it developed internal capacity for oncology.
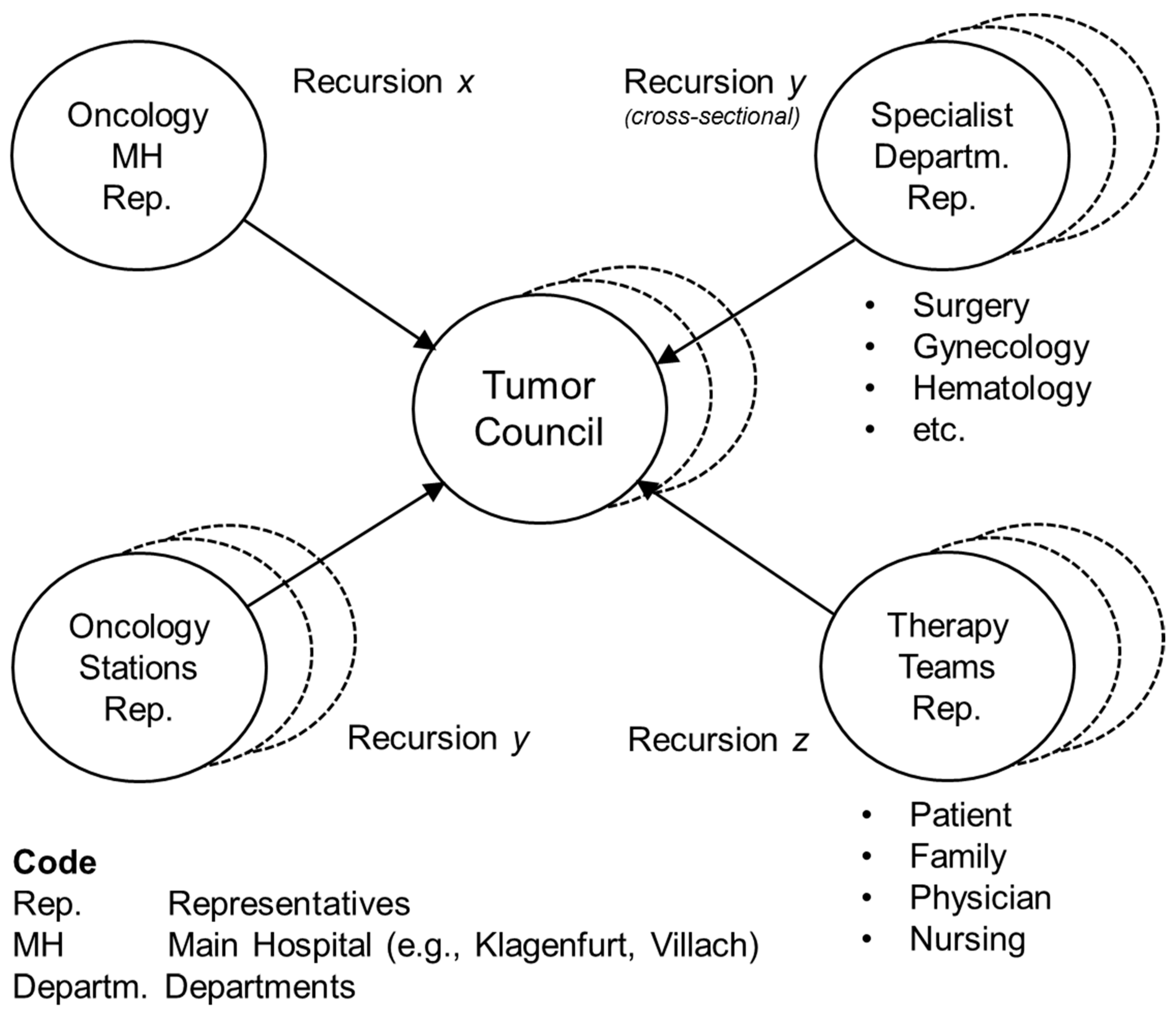
Finally, the Tumor Council is an entity that forms itself spontaneously, if a case needs a level of attention that goes beyond the possibilities of the Tumor Board. The composition of these bodies varies according to three criteria: (a) An oncologist is always present. (b) The responsible doctor (“patron”) and normally the nurse in charge of the case are present. (c) Other specialists are on the team as needed. See Figure 5. A Tumor Council can be summoned whenever a doctor or nurse from a specialist department needs assistance in dealing with a difficult case. In that case, an oncologist visits the respective ward, where he gathers with the local medical and nursing staff, and most importantly, the patient, in an on-site inspection (“ad hoc meeting”). Hence, the Tumor Council bundles distributed resources flexibly and effectively, and is a major factor for the quality of care.
These virtual teams are of a non-hierarchical (“heterarchical”) type [27,62]. They have proven to be efficient and powerful: they enhance the quality of care, an optimal use of available resources, and contribute towards the growth of the body of knowledge.
The arrows denote the provenience and inclusion, in the council, of members of different organizational groups; the multiple communications in the group are not especially represented. The diagram visualizes that the members of several recursions, normally two (x and y), possibly three (x, y, z) are part of such a body. The composition of the council varies as a function of the cases to be treated. The specialized departments are of the support function type, and they are represented as the cases demand.
Leadership of the council rests with a member of the oncology team of the hospital (e.g., Klagenfurt). If there is no local oncologist, a “mobile doctor” from OCS will be part of the team (either in person or electronically mediated), but only in a professional lead role, not in a formal one, such as the head or speaker of the group. Furthermore, the oncology stations (internal, tumor ambulatory, and any other stations with tumor patients) and if necessary certain specialists (e.g., surgeon, hematologist), are included.
Therapy teams are at the next recursion level (z). They are represented by the professionals just mentioned. However, certain cases do exist where a therapy team may be called onto a tumor council, normally via representation, for example in case an independent physician in charge of follow-up or support care needs the opinions of other professionals. When the presence of a patient is deemed necessary, the doctors may visit him at his station, and that patient himself becomes part of that council.
Also, an increase in the cohesion of those dealing with cancer and the cooperativeness across disciplines and departments has been clearly observable. Cultural events are regularly planned to support this process. For example, once a year, a gathering of medical and nursing staff from the oncology units in Carinthia and Styria, the neighboring state, takes place. The purpose of these events is exchanging ideas and getting informed about new developments in the field. Similar events take place, on a smaller scale, for the Carinthian staff, normally combined with a concert.
The tumor boards and councils are instances of decentralization. Nevertheless, certain technical resources (e.g., laser canons) could not be decentralized ad libitum due to financial constraints. Additional details about the team structures can be found in [11].
6. Case Part IV–The Evolution of Oncology Carinthia (C)
Taking a broad view on the evolution of Oncology Carinthia, we can discern remarkable changes which have shaped that system:
Gradually, doctors confronted with tumor instances came to understand the advantage of close cooperation with the oncological care unit established at LKH Klagenfurt, consisting of an internist-oncologist and a radiologist-oncologist. Even those who had rejected the new approach initially, moved on to cooperative and even supportive behavior.
The consecutive structural changes were set rather organically than mechanistically. They had considerable consequences. In the central oncology care unit, a team developed that was highly productive and continuously improved the quality of care. In addition, the specialists there transferred oncological know how to the decentralized oncology wards. These peripheral units gradually built their own skills and capabilities. The culture of a knowledge organization emerged, showing a high level of cohesiveness and stunning achievements.
At the level of partly organizational, partly product and technology innovations, many novelties were developed, e.g., a day clinic, mobile units, online meetings, tele-consulting. Overall, the social-organizational innovations—viable system, therapy teams, cross-sectional teams, virtual organization, transdisciplinary collaboration—were much more important than the product and technology ones. They made the latter possible in the first place, and their impact was much greater. Ultimately, the OCU success story has been written by social and organizational innovations.
The concept of virtual teams was introduced. Doctors increasingly took part in tumor boards, invoked councils, and conferred with the oncology hub. The 7 × 24 on-call service was a major factor in building trust and gave security when a doctor took on a treatment. The concept of mobile units added a new dimension in providing high-quality care covering the whole state. The introduction of these units and the virtual team approach added enormous flexibility to the provision of service capacity.
In this way, a growing share of the departments, as well in the LKHs as at the KHs, were integrated into the OCS. Increasingly tumor boards were established. The oncology champions were surprisingly active in research, participating in congresses and professional networks. Following the principle “as central as necessary and as decentralized as possible”, intensive-care patients were medicated at LKHs, under rigorous supervision of the oncological experts, while easy-to-manage cases could be treated at the clinic closest to their homes, frequently in the ambulant mode: a patient-friendly, but also a very economical way to provide oncological care. Altogether, an excellent level of care relative to the scientific state-of-the art was realized at Oncology Carinthia: the OCS had become an effective health care system.
7. Results
Our study demonstrates two things concerning the power of the systemically guided interventions accounted for in this paper. At the content level it shows the huge potential of service industries for increasing quality and productivity, even in cases of severe resource restrictions. A potential realized by sound diagnosis and clever operative decisions, supported by systemic methods and tools. At the context level, our study makes the strength of a holistic system design palpable. We were successful in conceiving Oncology Carinthia as a viable and adaptive whole, by supporting the evolution of the OCS conceptually and methodologically.
The first result is the organization design that has been accomplished. It is conceived around the patient as the focal point, with all features of a network organization. Patients and their families, often factored out from organizational plans, are the prime agents of the system in Oncology Carinthia. Both are crucial in the process of recovery. The central hospital and 10 more clinics, as well as registered doctors, are part of the care network, with a pivotal oncology unit as the main knowledge hub and coordinating agent. Among the innovative features of the structure are cross-sectional teams, transdisciplinary collaboration, a concept of mobile units that brings doctors to the patient (physically or online) rather than the other way around, and networks both inside and across the hospitals. The care process covers all phases from prevention to medical treatment to follow-up care and psychosocial accompaniment. It follows essentially a salutogenic orientation. One of the strengths of the arrangement is that both the design and management of the process are governed conceptually, with a heavy dose of theory. The implementation is an infinite learning process. In sum, an intricate, systemic path of dealing with the enormous complexity at hand has been discovered.
A second result is the stunning performance of the OCS. Despite an extreme scarcity of financial resources, both the quality and success of oncological care have been increased. The system under study has become a showcase of holistic medical treatment that has evoked sustained interest in professional circles all over Europe and beyond.
Third, Oncology Carinthia stands as an exemplar for the successful management of expertise. The influence of organizing and managing in general on the evolution of the system has become tangible. Yet it has not provoked the likely conflict between medical and managerial logics, which often deteriorates the qualification of professionals [63]. Instead, it brought to fruition a constructive force for the system’s viability. The reason is twofold: On the one hand, management in this case has never become a pathologically autopoietic system [31]. On the contrary, it has been instrumental in pursuing the purpose of the whole system in focus: a state-wide, excellent level of care, enabled by transdisciplinary collaboration. On the other hand, management including leadership was radically decentralized and integrated or “dissolved” into heterarchical, mobile, and virtual structures. This has entailed a powerful rise in the repertoires of behavior (“variety” in the cybernetic sense) at all levels of the organization, enabling multiple agents to cope with complexity forcefully. Oncology Carinthia has become more agile in both time and space.
The concerns and needs raised initially (see above) were met fully by the organization developed within roughly ten years (1985 to 1995): by then, the new system was running at “full steam”. In fact, the outcomes exceeded all expectations. A major factor was the substantial freedom granted to the champions by the state health authority of Carinthia.
Some of the results were unexpected: for example, the evidence that a) organizational structures can be nimble and robust at the same time, and b) a more complex structure is not necessarily more expensive; it can even be more economical.
The results referred to here are not an endpoint. On the contrary, the OCS team has seen itself confronted with new challenges along the way. Over time, competencies evolved, and structures had to develop as well. Transformations of structure took place for meeting new needs: for example, the establishment of two transdisciplinary units, a central ambulance, and an oncological ward for special cases, as well as the foundation of an intensive care unit for oncology.
We were not dealing with a machine, but with a social system. Hence, the design approach was both formal and informal. The results were emergent. Culture and structure were always “in progress”, adapting and evolving.
We have claimed that the OCS Carinthia has become a highly effective system of health care. Can this claim be upheld in view of empirical data? We consulted the Tumor Database Carinthia (“Tumorregister Kärnten”) in Klagenfurt, to examine if there was any evidence of medicinal effects of the OCS, over the period covered by our study. We received a long-term data series on the evolution of five-year survival rates, in Carinthia, for the five main entities of cancer indications (Figure 6). Five-year survival rates are the most important indicators of effectiveness in oncological care [64].
The axes in the five graphs show the period of survival after the treatment (from 1 to 5 years) and the percentage of patients surviving (1.00 being 100%). Each graph shows two curves, one for the period 2005–2004, the other for 2005–2013 (in case of stomach cancer for 2001–2006 and 2007–2013). The initial values n (number of patients) are as follows. prostate: 3828 (2005), 3819 (2005), lung: 2734 (1995), 2908 (2005), stomach: 783 (2001), 848 (2007), colorectal: 3259 (1995), 2953 (2005), breast: 3579 (1995), 3760 (2005).
The graphs tell us two things: a) for prostate, lung and stomach cancer, there is a highly significant improvement of the survival rates from the first to the second period. The respective p-values of the log-rank test are p < 0.0001 for the first indication, and p < 0.01 for the second and third indications. According to the null hypothesis, there is no difference between the two survival curves. Given the results of the log-rank test, the null hypothesis is refuted. (b) For colorectal cancer and breast cancer, there is a trend indicating improvement, even though the level of significance is less impressive. Here, p-values are at p < 0.1. This analysis testifies success, and that success could only be achieved through high quality of care. The numbers underpin the claim made above: the OCS became a highly effective health care organization.
8. Conclusions
What can be learnt from this case? In closing we shall try to condense our findings in a brief resumé, which cannot lay claim to being a full-fledged theory, but instead a set of crucial aspects conducive to ongoing learning. As these aspects have been tried and tested extensively over a long period, we dare to switch, at times, from the descriptive mode to “normative” propositions, i.e., suggestions of how things should be done in a high-quality OCS:
- (a)
- Ethos: The focus should be on the patient, with his or her family included. This means placing the patients and their quality of life at the center. Not only at the center, but also in command; the patient is the authority responsible for his or her health. For the doctors, nurses and other employees, a culture of the highest professional values, including unconditional commitment to patients, is the imperative to be adhered to. The principle of excellent care must pervade all activities. Goals must be high, and leaders need to energize the organization to attain them.
- (b)
- Systemic approach: Systemic thinking is a way of dealing competently with complex wholes. It enables systemic design for better organizations. The proposed thinking at the levels of both content and context forms a braid that enables a systemic process reaching from modelling to assessment to design to change. Unorthodox thinking, as our case showed, can produce management innovations that, although unwelcome at the beginning, go on to breed (unexpected) positive results and are adopted by the organization. To initiate and manage these innovations, powerful change agents are a sine qua non. Both an internal and external change agent were active, and in harmony. This may have been an important prerequisite for the successful performance of Oncology Carinthia [65].
- (c)
- Theory and practice: Practitioners are often theory averse. Therefore, we pursued another path, operating on a strong theoretical (and methodological) orientation, combining it with pragmatic, flexible implementation, and most important, with enduring dedication to the issues of health. This alternative path proved to be at the core of the success of Oncology Carinthia. The combination of theory-based and conceptually driven design, and reflexive, committed practice is mandatory for dealing effectively with complex organizational issues in a social system.
- (d)
- Methodology: We have tried to catalyze the dialectics of strategy and organization, proposing an integration of two system methodologies (SD and VSM) to facilitate dealing with the complex issues under study. These are not the only methodologies available, but they appear to be mature devices on which one can rely in the face of complexity. And they are complementary [45]. Much as with engineering, the chosen methods rely on the cyclic pair of reasoning and experimentation [66]. We have brought these methodologies together under the term Integrative Systems Methodology, a framework for systemic strategizing, i.e., for dealing with complexity in a long-term perspective.
- (e)
- Holistic organization design: The systemic approach provides highly effective heuristic devices and frameworks (e.g., VSM) for enhancing the viability and adaptiveness of organizations. Holistic design combines decentralization and centralization, as well as information flows from inside-out and outside-in, which is a better model than top-down and bottom-up. Structures can be nimble and robust at the same time, and a complex structure can be even more economical than a simplistic one. The systemic approach based on VSM, and other cybernetics-based structural models not discussed here. An example is Team Syntegrity, a systemic protocol for the interaction in large groups [67], and other cybersystemic models are remarkably effective in putting networks and virtual organizations in place, which absorb complexity pervasively. This proves to be the case here in an organization that is above all humanistic.
The main implication of our study is that these insights and teachings can also deliver value to other protagonists and “engineers” of health care systems. Even more, we trust that the organizational concepts discussed herein can convey lessons to organizers in any industry, showing them new paths of coping with complexity. As far as management scientists and students are concerned, the systemic approach—framework and methodology—documented in this reflexive case might potentially enhance their professional knowledge and repertoire.
All the aspects synthesized above are becoming ever more important, as the complexity of systems grows. The immediate results secured by organizations are less important than their viability in the long run. We have relied on the VSM to structure the OCS because that model defines not only the necessary but also the sufficient preconditions for such viability. Therefore, one can safely assume that the design we have proposed and implemented is not only successful, but it also has great potential for some time to come.
There are limitations to both the case and this chapter. As far as the case is concerned, even though the OCS has bred remarkable results as we have reported, Oncology Carinthia is not perfect; there is room for further improvement. For example, to date our successes at the preventive end are below our initial expectations. There is room for improvement here.
As far as this report is concerned, its chief limitation inheres in the difficulty of capturing the richness of 30 years of experience in a short document. For example, we cannot account for all the scenarios, the various what-ifs and so-what’s that emerged in the process. Also, little has been said about the relationships between Oncology Carinthia and its external stakeholders. Although we could write a book, a concise piece of work like this is more digestible.
Herewith, we have documented a combined application of SD and VSM in a long-term process of organizational transformation and learning. In another publication, we have explored a phase following the one described here [47]. There, the application of SD is documented more profoundly. While the present article shows an application of qualitative SD, the other paper conveys a full-fledged case of quantitative model-building related to an organizational process: the thoroughly validated model has the function of gauging a decision of the OCS management. The consequences of a planned budget cut are ascertained in terms of three indicators, economic performance, quality of care, and quality of work. The model delivers unexpected results. The assumption of the hospital management was that a budget cut would improve the profits. In contrast, the hypothesis of the oncologists, that the budget cut would impinge negatively on all three variables, was confirmed. That is what happened in the following five years, an instance of counterintuitive system behavior [64].
At the methodological level, we have shown that complementary methods are needed and must be combined to enable effective action in the face of organizational complexity. In this sense, we provide a synthesis of the methodologies of Organizational Cybernetics and System Dynamics. The need for such a combination derives from the remarkable complexity inherent in the case under study. We are proposing a methodologically rigorous synthesis in the context of Integrative Systems Methodology, an innovative device for coping with organizational complexity.
We have structured our study in line with the categories of Integrative Systems Methodology (ISM). This way we have provided a frame of useful distinctions for making the evolutionary process of the organization under study, the OCS, transparent. The schema of ISM also makes palpable the method for structuring the process in a robust fashion. As the frame is multidimensional, it enables a relatively “complete” set of interventions for coping with the complexity faced in the development of the OCS. For a deeper methodological reflection of ISM, see [19].
The ISM-framework has been used in multiple organizations. In the case under study, it has been applied over a long time; the results in terms of both efficiency and effectiveness have been outstanding. However, this finding is the smaller part of the theoretical harvest reaped from our study. Beyond the substantive results concerning the organization in focus, the data gathered from our inquiry lead to generic insights about organizational dynamics: insights that are applicable to a large class of organizations, not merely to this case study.
Author Contributions
M.S.: Conceptualization, methods, writing. J.K.: content, validation. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
Additional data available in [47].
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Appendix A.1. System Dynamics and Organizational Cybernetics–Complementarity and Synergy (For a More Profound Treatment of the Topic, see: [45])
System Dynamics (SD) and Organizational Cybernetics (OC), the Viable System Model (VSM) in particular, are two methodologies of the systems approach. The authors’ proposal is that SD and OC are complementary and can therefore be combined synergetically in concrete applications.
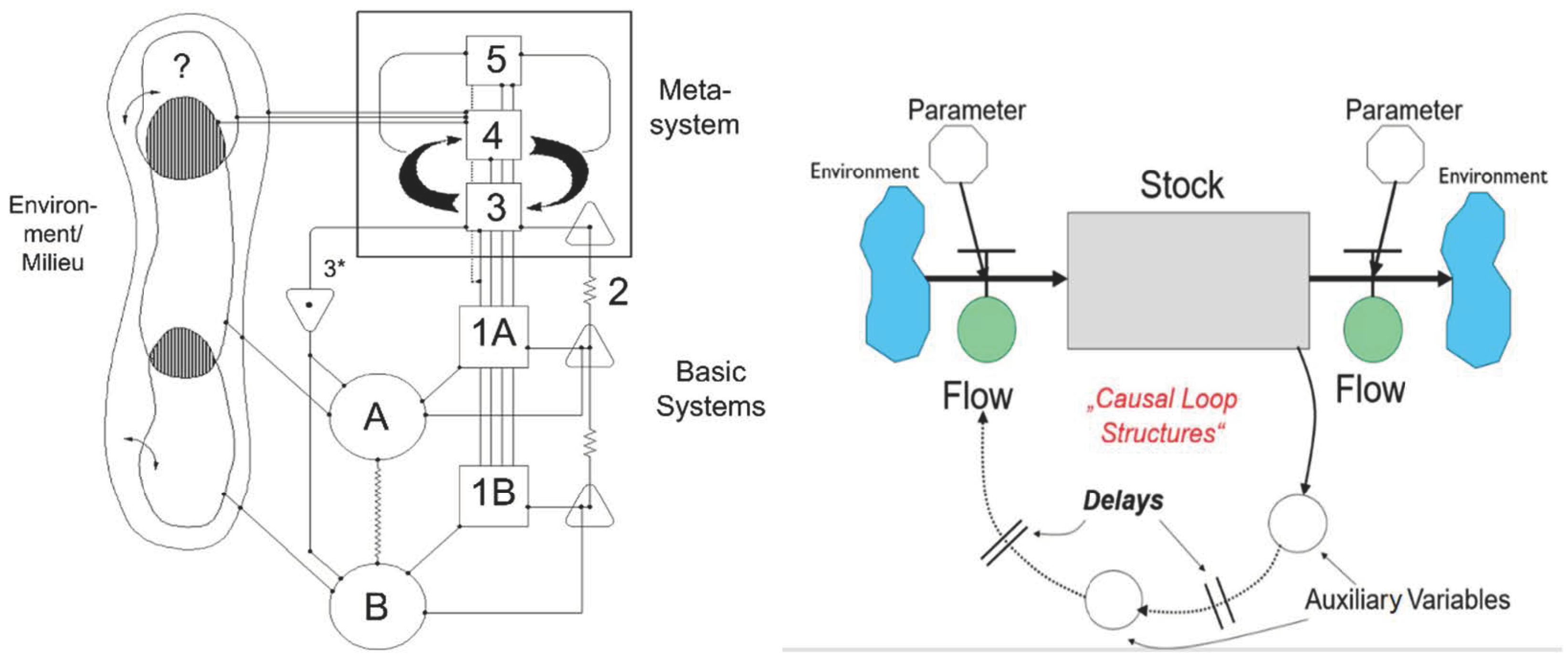
OC offers a model for the diagnosis and design of organizations of any kind—the Viable System Model (VSM). See Diagram A (Figure A1). The model defines the necessary and sufficient conditions for the viability of any social system, especially organizations.
SD is a discipline for the modeling, simulation and steering of complex, dynamic systems. See Diagram B (Figure A1). It provides a sophisticated, generic methodology to model the structure of such systems and to simulate their behavior.
Stylized versions of the two kinds of model:
Figure A1.
Diagram A: VSM (after Beer, passim). Diagram B: SD Model (after Forrester, passim).

The VSM is a structural model by which the degree of viability of an organization can be assessed. The model is applicable recursively to various levels of an organization, which show the same structure.
SD provides simulation models to capture and analyze the behavior of a system. Systems are normally analyzed with focus on concrete problems or issues, for example, surprising developments, systemic pathologies, etc.
Appendix A.2. Combining Complementary Methodologies
The combination or integration of the two complementary methodologies, SD and VSM, is prone to synergy. It can enable decision makers to be more effective in mastering complexity. This includes finding new ways of coping, via creativity and innovation. Other approaches or methodologies, e.g., Artificial Intelligence, can be integrated and be a powerful amplifier.
References
- Ulrich, H. Die Unternehmung als Produktives Soziales System: Grundlagen der Allgemeinen Unternehmungslehre; Haupt: Bern, Switzerland, 1968. [Google Scholar]
- Beer, S. Diagnosing the System for Organizations; Wiley: Chichester, UK, 1985. [Google Scholar]
- Bleicher, K. Das Konzept. In Integriertes Management; Campus, Frankfurt a.M.: New York, NY, USA, 2004. [Google Scholar]
- Berlinski, D. On Systems Analysis; MIT Press: Cambridge, MA, USA, 1976. [Google Scholar]
- Hanssmann, F. Einführung in die Systemforschung. Methodik der modellgestützten Entscheidungsvorbereitung; Oldenbourg: München, Germany, 1993. [Google Scholar]
- Ackoff, R.L. Creating the Corporate Future: Plan or Be Planned for; Wiley: New York, NY, USA, 1981. [Google Scholar]
- Checkland, P.B.; Scholes, J. Soft Systems Methodology in Action; New edition; Wiley: Chichester, UK, 2000. [Google Scholar]
- Türke, R.-E. Governance. In Systemic Foundation and Framework; Physica: Heidelberg, Germany, 2008. [Google Scholar]
- Homer, J. Models that Matter; Grapeseed Press: Barrytown, NY, USA, 2012. [Google Scholar]
- Ison, R. Systems Practice: How to Act. In Situations of Uncertainty and Complexity in a Climate-Change World, 2nd ed.; Springer: London, UK, 2017. [Google Scholar]
- Schwaninger, M. Making Change Happen: Recollections of a Systems Professional. Kybernetes 2012, 41, 348–367. [Google Scholar] [CrossRef]
- Ulrich, W. Critical Heuristics of Social Planning: A New Approach to Practical Philosophy; Haupt: Bern, Switzerland, 1983. [Google Scholar]
- Von Foerster, H. Observing Systems; Intersystems Publications: Seaside, CA, USA, 1984. [Google Scholar]
- Espejo, R.; Schuhmann, W.; Schwaninger, M.; Bilello, U. Organizational Transformation and Learning. In A Cybernetic Approach to Management; Wiley: Chichester, UK, 1996. [Google Scholar]
- Hammond, D. The Science of Synthesis: Exploring the Social Implications of General Systems Theory; University Press of Colorado: Boulder, CO, USA, 2003. [Google Scholar]
- Jackson, M.C. Systems Approaches to Management; Kluwer Academic/Plenum: New York, NY, USA, 2000. [Google Scholar]
- Schwaninger, M.; Klocker, J. Holistic Systems Design: The Oncology Carinthia Study. In Social Systems Engineering; García-Díaz, C., Olaya, C., Eds.; Wiley: Chichester, UK, 2018. [Google Scholar]
- Schwaninger, M. Methodologies in Conflict: Achieving Synergies between System Dynamics and Organizational Cybernetics. Syst. Res. Behav. Sci. 2004, 21, 411–431. [Google Scholar] [CrossRef]
- Schwaninger, M. An Integrative Systems Methodology for Dealing with Complex Issues. In GABEK VI—Sozial Verantwortliche Entscheidungsprozesse; Zelger, J., Müller, J., Plangge, S., Eds.; StudienVerlag: Innsbruck, Austria, 2013; pp. 177–196. [Google Scholar]
- Ashby, W.R. An Introduction to Cybernetics; Chapman & Hall: London, UK, 1956. [Google Scholar]
- Beer, S. The Heart of Enterprise; Wiley: Chichester, UK, 1979. [Google Scholar]
- Gell-Mann, M. What is Complexity? Remarks on simplicity and complexity. Complexity 1995, 1, 16–19. [Google Scholar] [CrossRef]
- Mitchell, M. Complexity. In A Guided Tour; Oxford University Press: New York, NY, USA, 2009. [Google Scholar]
- Rescher, N. Complexity. In A Philosophical Overview; Transaction Publishers: New Brunswick, NJ, USA; London, UK, 1998. [Google Scholar]
- Checkland, P.B. Systems Thinking, Systems Practice; Wiley: Chichester, UK, 1981. [Google Scholar]
- Griffin, D.; Shaw, P.; Stacey, R. Speaking of Complexity in Management Theory and Practice. Organ. Chaos Complex. 1998, 5, 315–339. [Google Scholar] [CrossRef]
- Schwaninger, M. Intelligent Organizations: Powerful Models for Systemic Management, 2nd ed.; Springer: Berlin/Heidelberg, Germany, 2009. [Google Scholar]
- Allen, P.; Maguire, S.; McKelvey, B. The SAGE Handbook of Complexity and Management; SAGE: London, UK, 2011. [Google Scholar]
- Stacey, R.D. Strategic Management and Organisational Dynamics the Challenge of Complexity to Ways of Thinking about Organisations; Financial Times Prentice Hall: Harlow, UK, 2011. [Google Scholar]
- Jackson, M.C. Critical Systems Thinking and the Management of Complexity; Wiley: Chichester, UK, 2019. [Google Scholar]
- Beer, S. The Brain of the Firm; Wiley: Chichester, UK, 1981. [Google Scholar]
- Weber, M.; Schwaninger, M. Transforming an Agricultural Trade Organization: A System-Dynamics-Based Intervention. Syst. Dyn. Rev. 2002, 18, 381–401. [Google Scholar] [CrossRef]
- Beer, S. The Viable System Model: Its Provenance, Development, Methodology and Pathology. J. Oper. Res. Soc. 1984, 35, 7–25. [Google Scholar] [CrossRef]
- Forrester, J.W. Industrial Dynamics; MIT Press: Cambridge, MA, USA, 1961. [Google Scholar]
- Forrester, J.W. Principles of Systems; Pegasus Communications: Waltham, MA, USA, 1968. [Google Scholar]
- Forrester, J.W. Counterintuitive Behavior of Social Systems. Technol. Rev. 1971, 73, 52–68. [Google Scholar]
- Sterman, J.D. Business Dynamics. In Systems Thinking and Modeling for a Complex World; Irwin/Mc Graw-Hill: Boston, MA, USA, 2000. [Google Scholar]
- Schwaninger, M. Integrative Systems Methodology: Heuristic for Requisite Variety. Int. Trans. Oper. Res. 1997, 4, 109–123. [Google Scholar] [CrossRef]
- Espejo, R. Management of Complexity in Problem Solving. In Organizational Fitness: Corporate Fitness through Management Cybernetics; Espejo, R., Schwaninger, M., Eds.; Campus Frankfurt: New York, NY, USA, 1993; pp. 67–92. [Google Scholar]
- Espejo, R.; Reyes, A. Organizational Systems. In Managing Complexity with the Viable System Model; Springer: Berlin/Heidelberg, Germany, 2011. [Google Scholar]
- Pettigrew, A.M. The Awakening Giant: Continuity and Change in Imperial Chemical Industries; Blackwell: Oxford, UK, 1985. [Google Scholar]
- Gomez, P.; Probst, G.J.B. Vernetztes Denken im Management; Die Orientierung (89); Schweizerische Volksbank: Bern, Switzerland, 1987. [Google Scholar]
- Christopher, W.F. Holistic Management: Managing What Matters for Company Success; Wiley: Hoboken, NJ, USA, 2007. [Google Scholar]
- Espinosa, A. Sustainable Self-Governance in Businesses and Society: The Viable System Model in Action; Francis & Taylor, Routledge: London, UK, 2023. [Google Scholar]
- Schwaninger, M.; Pérez Ríos, J. System dynamics and cybernetics: A synergetic pair. Syst. Dyn. Rev. 2008, 24, 145–174. [Google Scholar] [CrossRef]
- Schwaninger, M.; Klocker, J. Systemic Development of Health organizations: An Integrative Systems Methodology. In Innovative Health Systems for the 21st Century; Qudrat-Ullah, H., Tsasis, P., Eds.; Springer International: Cham, Switzerland; Wiley: Chichester, UK, 2017. [Google Scholar]
- Schwaninger, M.; Klocker, J. Efficiency versus Effectiveness in Hospitals: A Dynamic Simulation Approach. In Outcome-Based Performance Management in the Public Sector; Borgonovi, E., Anessi Pessina, E., Bianchi, C., Eds.; Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar]
- Senge, P.M. The Fifth Discipline. In The Art and Practice of the Learning Organization; Century Business: London, UK, 1990. [Google Scholar]
- Richardson, G. Problems in Causal Loop Diagrams Revisited. Syst. Dyn. Rev. 1997, 13, 247–252. [Google Scholar] [CrossRef]
- Schwaninger, M.; Scheef, C. Testing the Viable System Model. Theoretical Claim versus Empirical Evidence. Cybern. Syst. 2016, 47, 544–569. [Google Scholar] [CrossRef]
- Crisan Tran, C.I. Beers Viable System Model und die Lebensfähigkeit von Jungunternehmen: Eine Empirische Untersuchung. Ph.D. Dissertation, University of St. Gallen, St. Gallen, Switzerland, 2006. No. 3201. [Google Scholar]
- Malik, F. Strategie des Managements Komplexer Systeme ein Beitrag zur Management-Kybernetik Evolutionärer Systeme; Haupt: Bern, Switzerland, 1989. [Google Scholar]
- Clemson, B. Cybernetics: A New Management Tool; Abacus: Turnbridge Wells, UK, 1984. [Google Scholar]
- Hoverstadt, P. The Fractal Organization. In Creating Sustainable Organizations with the Viable System Model; Wiley: Chichester, UK, 2008. [Google Scholar]
- Pérez Ríos, J. Design and Diagnosis for Sustainable Organizations: The Viable System Method; Springer: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Lassl, W. The Viability of Organizations; Springer: Berlin/Heidelberg, Germany, 2019/20; Volumes 1–3.
- Pfiffner, M. The Neurology of Business: Implementing the Viable System Model; Springer: Cham, Switzerland, 2022. [Google Scholar]
- Erbsen, A. Krankheit im Zentrum Gestaltung von Krankheitsorientierten Spitalstrukturen aus Kybernetisch-Konstruktivistischer Sicht; Springer Fachmedien Wiesbaden: Wiesbaden, Germany, 2012. [Google Scholar]
- Luhmann, N. Social Systems; Stanford University Press: Stanford, CA, USA, 1995. [Google Scholar]
- Lipnack, J.; Stamps, J. Virtual Teams, 2nd ed.; Wiley: New York, NY, USA, 2000. [Google Scholar]
- Nonaka, I.; Takeuchi, H. The Knowledge-Creating Company; Oxford University Press: New York, NY, USA, 1995. [Google Scholar]
- McCulloch, W. Embodiments of Mind; MIT Press: Cambridge, MA, USA, 1965; new edition 1988. [Google Scholar]
- Boos, F.; Mitterer, G. Einführung in Das Systemische Management; Carl-Auer-Systeme Verlag: Heidelberg, Germany, 2014. [Google Scholar]
- Ziegler, A.; Lange, S.; Bender, R. Überlebenszeitanalyse: Der Log-Rang Test. Dtsch. Med. Wochenschr. 2007, 132, e39–e41. [Google Scholar] [CrossRef] [PubMed]
- Birkinshaw, J.; Hamel, G.; Mol, M.J. Management Innovation. Acad. Manag. Rev. 2008, 33, 825–845. [Google Scholar] [CrossRef]
- Golden, S.L. Compromised Exactness and the Rationality of Engineering. In Social Systems Engineering; Garcia-Díaz, C., Olaya, C., Eds.; Wiley: Chichester, UK, 2017. [Google Scholar]
- Beer, S. Beyond Dispute. In The Invention of Team Syntegrity; Wiley: Chichester, UK, 1994. [Google Scholar]
Figure 2.
Causal loop diagram showing the dynamics of the system in focus.

Figure 3.
Three main levers for the development of the oncological care system. Variables in brackets are “shadow variables”, used to avoid entanglements in the diagram. For example, <Leadership> is identical with Leadership).
Figure 3.
Three main levers for the development of the oncological care system. Variables in brackets are “shadow variables”, used to avoid entanglements in the diagram. For example, <Leadership> is identical with Leadership).

Figure 4.
Oncology Carinthia as a recursively structured system.

Figure 5.
The constitution of tumor councils as virtual organizations.

Figure 6.
Survival rates for main entities of cancer in Carinthia 1995–2013.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Stakeholders, goals, and key factors.
| Interest Groups | Goals | Key Factors |
|---|---|---|
| Patients & their Families | Be healthy Suffer little | Prevention Quality of life Quality of care |
| Champions of Oncological Care | Be excellent professionals Have an interesting job Realize their ideas Lead an effective team | Motivation Research & knowledge management Strong infrastructure Cooperation Effective coordination |
| Local Hospitals and Doctors | Qualify in oncology Become members of care network | Training Cooperation |
| Professional Staff | Have an interesting job Have a bearable job Become more qualified | Training Psychohygiene Cooperativeness of other units involved |
| State Authorities & Central Hospital Administration | Effectiveness of care system Efficiency of care system | Low incidence of cancer Cancer prevention Success of care High productivity Coordination |
| Public in General | Stay healthy | Social & ecological consciousness Quality of environment Healthy behavior |
Table 2.
Recursive distribution of tasks in the oncological care system.
| Recursion w: Oncology Carinthia | Recursion x: Oncology Regions (e.g., Oncology Klagenfurt) | Recursion y: Oncology Stations (e.g., Tumor Ambulance) | |
|---|---|---|---|
| Basic Units | Oncology Klagenfurt Oncology Villach Oncology Wolfsberg Oncology in 6 further hospitals | Oncological Ambulance, Oncology ward at internal station. n Local practitioners with oncological competence | N Teams (Interaction Systems, including patient & family, physician & nursing) n Local practitioners with oncological competence |
| Component 1: Local Management | Heads of basic units: Oncologists | Heads of station: oncologists or intemists | Patient & family |
| Component 2: Coordination | Standard therapies, tumor database, training, oncology circle, doctors’ letters, electronic messaging and conferences | Tumor database, tumor boards and councils, coordination sessions (Radiotherapy1Hematology/Pathology), standard therapies, training, doctors’ letters | Tumor councils, Standard therapy plans, daily station meeting, nursing guidelines, coffee break |
| Component 3: Executive Management | Lead Team OCS (2 oncologists, 1 internist-oncologist, 1 radiologist-oncologist) | Management team/local leaders (physicians & nursing staff; 9 persons) | Station leaders (physicians and nursing staff in charge) |
| Channel between Components 1 to 3 | Allocation of time and OCS staff, Management by Objectives, Definition/negotiation Std. Therapies | Allocation of time and personnel, design/negotiation of therapy plans | Assignments/requests, participation |
| Component 3*: Audit Channel | Visits to local oncology units, phone calls, messaging, Special studies, inquiries, Tests informal communication, cultural events | Medical visits, phone calls, messaging. informal communication | Medical visits, continualcontact1 conversations with patients. informal communication |
| Component 4: Organizational/ Development/ Strategic Management | OCS leaders team, therapy and prevention strategies, ongoing research, congresses and symposia, networks, strategy workshops | Development plan, future-oriented education, management team, leaders OCS | Station development plan, future-oriented education, leaders of station, leaders OCS, head internal station |
| Component 5: System Ethos/ Normative Management | Ethos OCS- Values, principles, vision and mission, mission, management framework OCS, leaders OCS | Values, principles, vision and mission, ethos OCS, management framework OCS, local management team, leaders OCS | mission, ethos OCS, leaders of station, leaders OCS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Schwaninger, M.; Klocker, J. Applying Integrative Systems Methodology: The Case of Health Care Organizations. Systems 2024, 12, 140. https://doi.org/10.3390/systems12040140
AMA Style
Schwaninger M, Klocker J. Applying Integrative Systems Methodology: The Case of Health Care Organizations. Systems. 2024; 12(4):140. https://doi.org/10.3390/systems12040140
Chicago/Turabian StyleSchwaninger, Markus, and Johann Klocker. 2024. "Applying Integrative Systems Methodology: The Case of Health Care Organizations" Systems 12, no. 4: 140. https://doi.org/10.3390/systems12040140
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.