
Evaluation of Oral Amoxicillin/Clavulanate for Urinary Tract Infections Caused by Ceftriaxone Non-Susceptible Enterobacterales
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
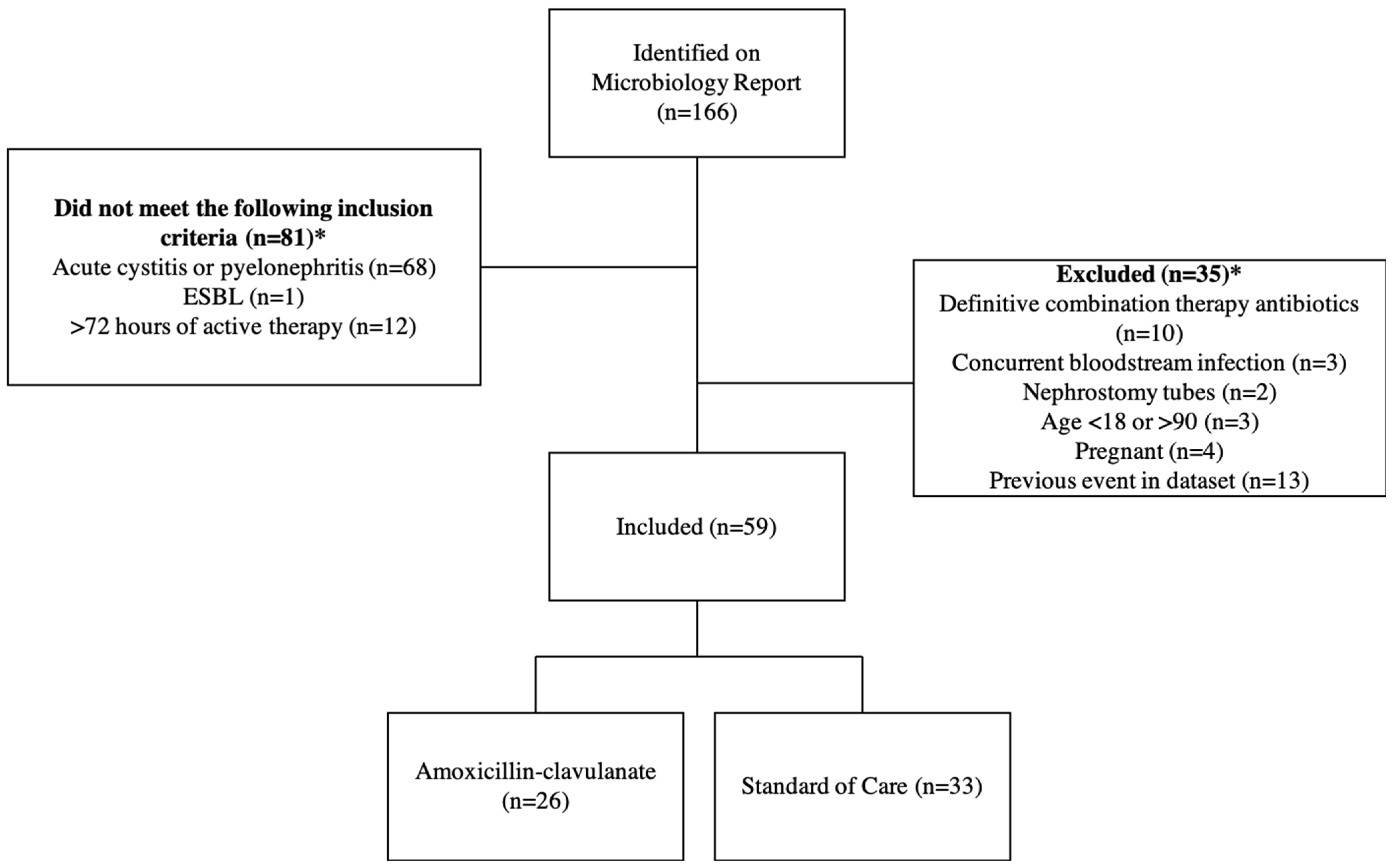
2.1. Patients
2.2. Definitions
2.3. Outcomes
2.4. Data Management and Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- ESBL-Producing Enterobacterales |HAI|, C.D.C. Available online: https://www.cdc.gov/hai/organisms/ESBL.html (accessed on 8 December 2022).
- Talan, D.A.; Takhar, S.S.; Krishnadasan, A.; Mower, W.R.; Pallin, D.J.; Garg, M.; Femling, J.; Rothman, R.E.; Moore, J.C.; Jones, A.E.; et al. Emergence of Extended-Spectrum β-Lactamase Urinary Tract Infections among Hospitalized Emergency Department Patients in the United States. Ann. Emerg. Med. 2021, 77, 32–43. [Google Scholar] [CrossRef] [PubMed]
- Ling, W.; Furuya-Kanamori, L.; Ezure, Y.; Harris, P.N.; Paterson, D.L. Adverse clinical outcomes associated with infections by Enterobacterales producing ESBL (ESBL-E): A systematic review and meta-analysis. JAC Antimicrob Resist. 2021, 3, dlab068. [Google Scholar] [CrossRef] [PubMed]
- Kaye, K.S.; Gupta, V.; Mulgirigama, A.; Joshi, A.V.; Scangarella-Oman, N.E.; Yu, K.; Ye, G.; Mitrani-Gold, F.S. Antimicrobial Resistance Trends in Urine Escherichia coli Isolates from Adult and Adolescent Females in the United States from 2011 to 2019: Rising ESBL Strains and Impact on Patient Management. Clin. Infect. Dis. 2021, 73, 1992–1999. [Google Scholar] [CrossRef] [PubMed]
- Aronin, S.I.; Dunne, M.W.; Kalvin, C.Y.; Watts, J.A.; Gupta, V. Increased rates of extended-spectrum beta-lactamase isolates in patients hospitalized with culture-positive urinary Enterobacterales in the United States: 2011–2020. J. Diagn. Microbiol. Infect. Dis. 2022, 103, 115717. [Google Scholar] [CrossRef] [PubMed]
- Tamma, P.; Aitken, S.; Bonomo, R.; Mathers, A.; van Duin, D.; Clancy, C. Infectious Diseases Society of America Antimicrobial-Resistant Treatment Guidance: Gram-Negative Bacterial Infections. Clin. Infect. Dis. 2022, 6, 2089–2114. [Google Scholar] [CrossRef] [PubMed]
- Rolinson, G.N. A review of the microbiology of amoxycillin/clavulanic acid over the 15 year period 1978–1993. J. Chemother. 1994, 6, 283–318. [Google Scholar] [CrossRef] [PubMed]
- Beytur, A.; Yakupogullari, Y.; Oguz, F.; Otlu, B.; Kaysadu, H. Oral amoxicillin-clavulanic Acid treatment in urinary tract infections caused by extended-spectrum Beta-lactamase-producing organisms. Jundishapur J. Microbiol. 2015, 8, e13792. [Google Scholar] [CrossRef] [PubMed]
- Flores-Mireles, A.L.; Walker, J.N.; Caparon, M.; Hultgren, S.J. Urinary tract infections: Epidemiology, mechanisms of infection and treatment options. Nat. Rev. Microbiol. 2015, 13, 269–294. [Google Scholar] [CrossRef]
- Nicolle, L.E.; Gupta, K.; Bradley, S.F.; Colgan, R.; DeMuri, G.P.; Drekonja, D.; Eckert, L.O.; Geerlings, S.E.; Köves, B.; Hooton, T.M.; et al. Clinical Practice Guideline for the Management of Asymptomatic Bacteriuria: 2019 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2019, 68, e83–e110. [Google Scholar] [CrossRef]
- Gupta, K.; Hooton, T.M.; Naber, K.G.; Wullt, B.; Colgan, R.; Miller, L.G.; Moran, G.J.; Nicolle, L.E.; Raz, R.; Schaeffer, A.J.; et al. Infectious Diseases Society of America; European Society for Microbiology and Infectious Diseases. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin. Infect. Dis. 2011, 52, e103–e120. [Google Scholar]
- Ramakrishnan, K.; Scheid, D.C. Diagnosis and management of acute pyelonephritis in adults. Am. Fam. Physician 2005, 71, 933–942. [Google Scholar]
- Centers for Disease Control and Prevention. People Who Are Immunocompromised. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-who-are-immunocompromised.html (accessed on 14 February 2023).
- Kadry, N.; Natarajan, M.; Bein, E.; Kim, P.; Farley, J. Discordant Clinical and Microbiological Outcomes Are Associated with Late Clinical Relapse in Clinical Trials for Complicated Urinary Tract Infections. Clin. Infect. Dis. 2023, 76, 1768–1775. [Google Scholar] [CrossRef]
- Sutton, J.D.; Stevens, V.W.; Chang, N.-C.N.; Khader, K.; Timbrook, T.T.; Spivak, E.S. Oral β-Lactam Antibiotics vs. Fluoroquinolones or Trimethoprim-Sulfamethoxazole for Definitive Treatment of Enterobacterales Bacteremia from a Urine Source. JAMA 2020, 3, e2020166. [Google Scholar] [CrossRef] [PubMed]
- Saad, S.; Mina, N.; Lee, C.; Afra, K. Oral beta-lactam step down in bacteremic E. coli urinary tract infections. BMC Infect. Dis. 2020, 20, 785. [Google Scholar] [CrossRef]
- Mack, T.; Hiles, J.J.; Wrin, J.; Desai, A. Use of Fluoroquinolones or Sulfamethoxazole-Trimethoprim Compared to Β-Lactams for Oral Step-Down Therapy in Hospitalized Patients with Uncomplicated Enterobacterales Bacteremia. Ann. Pharmacother. 2023, 57, 251–258. [Google Scholar] [CrossRef]
- Anderson, D.T.; Albrecht, B.; Jones, K.A.; Jacob, J.T.; Sexton, M.E.; Wiley, Z.; Dube, W.C.; Lee, B.; Suchindran, S. Efficacy of Noncarbapenem β-Lactams Compared to Carbapenems for Extended-Spectrum β-Lactamase–Producing Enterobacterales Urinary Tract Infections. Open Forum. Infect. Dis. 2022, 9, ofac034. [Google Scholar] [CrossRef]
- Sharara, S.L.; Amoah, J.; Pana, Z.D.; Simner, P.J.; Cosgrove, S.E.; Tamma, P.D. Is Piperacillin-Tazobactam Effective for the Treatment of Pyelonephritis Caused by Extended-Spectrum β-Lactamase–Producing Organisms? Clin. Infect. Dis. 2020, 71, e331–e337. [Google Scholar] [CrossRef] [PubMed]
- Dunne, M.W.; Aronin, S.I.; Das, A.F.; Akinapelli, K.; Zelasky, M.T.; Puttagunta, S.; Boucher, H.W. Sulopenem or Ciprofloxacin for the Treatment of Uncomplicated Urinary Tract Infections in Women: A Phase 3, Randomized Trial. Clin. Infect. Dis. 2023, 77, 66–77. [Google Scholar] [CrossRef] [PubMed]
- Cattrall JW, S.; Asín-Prieto, E.; Freeman, J.; Troconiz, I.F.; Kirby, A. A pharmacokinetic-pharmacodynamic assessment of oral antibiotics for pyelonephritis. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 2311–2321. [Google Scholar] [CrossRef]
- Bunnell, K.; Duong, A.; Ringsred, T.; Mian, A.; Bhathena, S. Aminopenicillins for treatment of ampicillin-resistant enterococcal urinary tract infections. Am. J. Health-Syst. Pharm. 2022, 79, 1056–1065. [Google Scholar] [CrossRef]
- Ponte, C.; Gracia, M.; Giménez, M.-J.; Aguilar, L.; Maín, C.M.; Carpintero, Y.; Huelves, L.; Carcas, A.; del Prado, G.; Soriano, F. Urinary Concentrations and Bactericidal Activity against Amoxicillin-Nonsusceptible Strains of Escherichia coli with Single-Dose, Oral, Sustained-Release Amoxicillin/Clavulanic Acid: A Phase I, Open-Label, Noncomparative Clinical Trial in Healthy Volunteers. Clin. Ther. 2005, 27, 1043–1049. [Google Scholar] [PubMed]
- Cole, K.A.; Kenney, R.M.; Perri, M.B.; Dumkow, L.E.; Samuel, L.P.; Zervos, M.J.; Davis, S.L. Outcomes of Aminopenicillin Therapy for Vancomycin-Resistant Enterococcal Urinary Tract Infections. Antimicrob. Agents Chemother. 2015, 59, 7362–7366. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.J.; Cherabuddi, K.; Shultz, J.; Borgert, S.; Ramphal, R.; Klinker, K.P. Ampicillin for the treatment of complicated urinary tract infections caused by vancomycin–resistant Enterococcus spp (VRE): A single-center university hospital experience. Int. J. Antimicrob. Agents 2018, 57, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Richey, E.M.; Waters, P.W.; Jovic, M.; Rakhman, C. Treatment of ampicillin-resistant Enterococcus faecium urinary tract infections. Fed. Pract. 2015, 32, 20–23. [Google Scholar] [PubMed]
- JMI Laboratories, Inc. SENTRY Antimicrobial Surveillance. Available online: https://sentry-mvp.jmilabs.com/app/sentry-public (accessed on 1 February 2023).
- Barlam, T.F.; Cosgrove, S.E.; Abbo, L.M.; MacDougall, C.; Schuetz, A.N.; Septimus, E.J.; Srinivasan, A.; Dellit, T.H.; Falck-Ytter, Y.T.; Fishman, N.O.; et al. Implementing an Antibiotic Stewardship Program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin. Infect. Dis. 2016, 62, e51–e77. [Google Scholar] [CrossRef]
- Coupat, C.; Pradier, C.; Degand, N.; Hofliger, P.; Pulcini, C. Selective reporting of antibiotic susceptibility data improves the appropriateness of intended antibiotic prescriptions in urinary tract infections: A case-vignette randomised study. Eur. J. Clin. Microbiol. Infect. Dis. 2013, 32, 627–636. [Google Scholar] [CrossRef]
- Rosenberg, J.M.; Levy, R.C.; Cicmanec, J.F.; Hedges, J.R.; Burke, B.M. Single-dose ceftriaxone treatment of urinary tract infections. Ann. Emerg. Med. 1985, 14, 970–972. [Google Scholar] [CrossRef]
- Iravani, A.; Richard, G.A. Single-dose ceftriaxone versus multiple-dose trimethoprim-sulfamethoxazole in the treatment of acute urinary tract infections. Antimicrob. Agents Chemother. 1985, 27, 158–161. [Google Scholar] [CrossRef]
- Stein, G.E. Single-dose treatment of acute cystitis with fosfomycin tromethamine. Ann. Pharmacother. 1998, 32, 215–219. [Google Scholar] [CrossRef]
- Goodlet, K.J.; Benhalima, F.Z.; Nailor, M.D. A Systematic Review of Single-Dose Aminoglycoside Therapy for Urinary Tract Infection: Is It Time to Resurrect an Old Strategy? Antimicrob. Agents Chemother. 2019, 63, e02165-18. [Google Scholar] [CrossRef]


{kind=link}
| Amoxicillin/ Clavulanate (n = 26) | Standard of Care (n = 33) | Total (n = 59) | p -Value | |
|---|---|---|---|---|
| Age (years), (mean (SD)) | 62.2 (18.0) | 58.2 (17.5) | 60.0 (17.7) | 0.396 |
| Male (n (%)) | 11 (42.3) | 9 (27.3) | 20 (33.9) | 0.226 |
| Race (n (%)) White Black/African American American Indian/Alaskan Asian Hispanic | 11 (42.3) 7 (26.9) 1 (3.8) 2 (7.7)5 (19.2) | 17 (51.5) 2 (6.1) 0 (0.0) 0 (0.0) 14 (42.4) | 28 (47.5) 9 (15.3) 1 (1.7) 2 (3.4)19 (32.2) | 0.014 |
| Infection Type (n (%)) Uncomplicated cystitis Complicated cystitis Uncomplicated pyelonephritis | 3 (11.5) 18 (69.2) 5 (19.2) | 4 (12.1) 15 (45.5) 14 (42.2) | 7 (11.9) 33 (55.9) 19 (32.2) | 0.142 |
| Inpatient at time of urine culture (n (%)) | 18 (69.2) | 18 (54.5) | 36 (61.0) | 0.251 |
| Urinary tract abnormalities (n (%)) | 12 (46.2) | 17 (51.5) | 29 (49.2) | 0.683 |
| Positive urine cultures within previous 12 months (n (%)) 0 1 2 3+ | 13 (50.0) 9 (34.6) 1 (3.8) 3 (11.5) | 8 (24.2) 13 (39.4) 3 (9.1) 9 (27.3) | 21 (35.6) 22 (37.3) 4 (6.8) 12 (20.3) | 0.160 |
| Charlson Comorbidity Index (mean (SD)) | 4.5 (3.3) | 3.7 (1.9) | 4.1 (2.6) | 0.293 |
| Immunocompromised (n (%)) Renal Transplant | 3 (11.5) 1 (3.8) | 12 (36.4) 6 (18.2) | 15 (25.4) 7 (11.9) | 0.030 0.091 |
| Serum WBC (cells/uL) (mean (SD)) | 10.3 (5.8) | 9.7 (5.2) | 10.0 (5.4) | 0.673 |
| Serum lactate (mmol/L) (mean (SD)) | 2.0 (0.9) | 2.6 (1.3) | 2.4 (1.2) | 0.175 |
| Pyuria (n (%)) | 24 * (100.0) | 31 (93.9) | 55 (96.5) | 0.220 |
| Charlson Comorbidity Index (mean (SD)) | 4.5 (3.3) | 3.7 (1.9) | 4.1 (2.6) | 0.293 |
| Treatment duration (days) (mean (SD)) | 7.0 (2.7) | 9.3 (5.2) | 8.3 (5.0) | 0.085 |
| Active lead-in therapy ** (n (%)) | 6 (31.6) | 13 (65.0) | 19 (48.7) | 0.037 |
| Organism (n (%)) | ||||
| E. coli | 23 (88.5) | 25 (75.8) | 48 (81.4) | 0.214 |
| K. pneumoniae | 3 (11.5) | 8 (24.2) | 11 (18.6) | 0.362 |
| Amoxicillin/Clavulanate (n = 26) | Standard of Care (n = 33) | p-Value | |
|---|---|---|---|
| Clinical failure (n (%)) New symptoms Retreatment Both | 5 (19.2) 0 (0.0) 3 (11.5) 2 (7.7) | 10 (30.3) 3 (9.1) 6 (18.2) 1 (3.0) | 0.332 |
| Time to failure (days) (Mean (SD)) | 31.2 (23.8) | 35.0 (24.6) | 0.725 |
| Hospital length of stay (days), (Mean (SD)) | |||
| Admitted from Community | 2.9 (1.2) | 8.4 (8.9) | 0.053 |
| Inpatient at Diagnosis | 10.3 (9.8) | 19.7 (20.5) | 0.237 |
| Amoxicillin/Clavulanate-resistant organism (n (%)) | 3 (11.5) | 2 (6.1) | 0.453 |
| Carbapenem-resistant organism (n (%)) | 1 (3.8) | 0 (0.0) | 0.441 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salam, M.E.; Jeffres, M.; Molina, K.C.; Miller, M.A.; Huang, M.; Fish, D.N. Evaluation of Oral Amoxicillin/Clavulanate for Urinary Tract Infections Caused by Ceftriaxone Non-Susceptible Enterobacterales. Pharmacy 2024, 12, 60. https://doi.org/10.3390/pharmacy12020060
Salam ME, Jeffres M, Molina KC, Miller MA, Huang M, Fish DN. Evaluation of Oral Amoxicillin/Clavulanate for Urinary Tract Infections Caused by Ceftriaxone Non-Susceptible Enterobacterales. Pharmacy. 2024; 12(2):60. https://doi.org/10.3390/pharmacy12020060
Chicago/Turabian StyleSalam, Madison E., Meghan Jeffres, Kyle C. Molina, Matthew A. Miller, Misha Huang, and Douglas N. Fish. 2024. "Evaluation of Oral Amoxicillin/Clavulanate for Urinary Tract Infections Caused by Ceftriaxone Non-Susceptible Enterobacterales" Pharmacy 12, no. 2: 60. https://doi.org/10.3390/pharmacy12020060