Pilot Study on the Utility and Feasibility of a House-Call Checkup of the Medicine Cabinet



Abstract
:1. Introduction
2. Materials and Methods
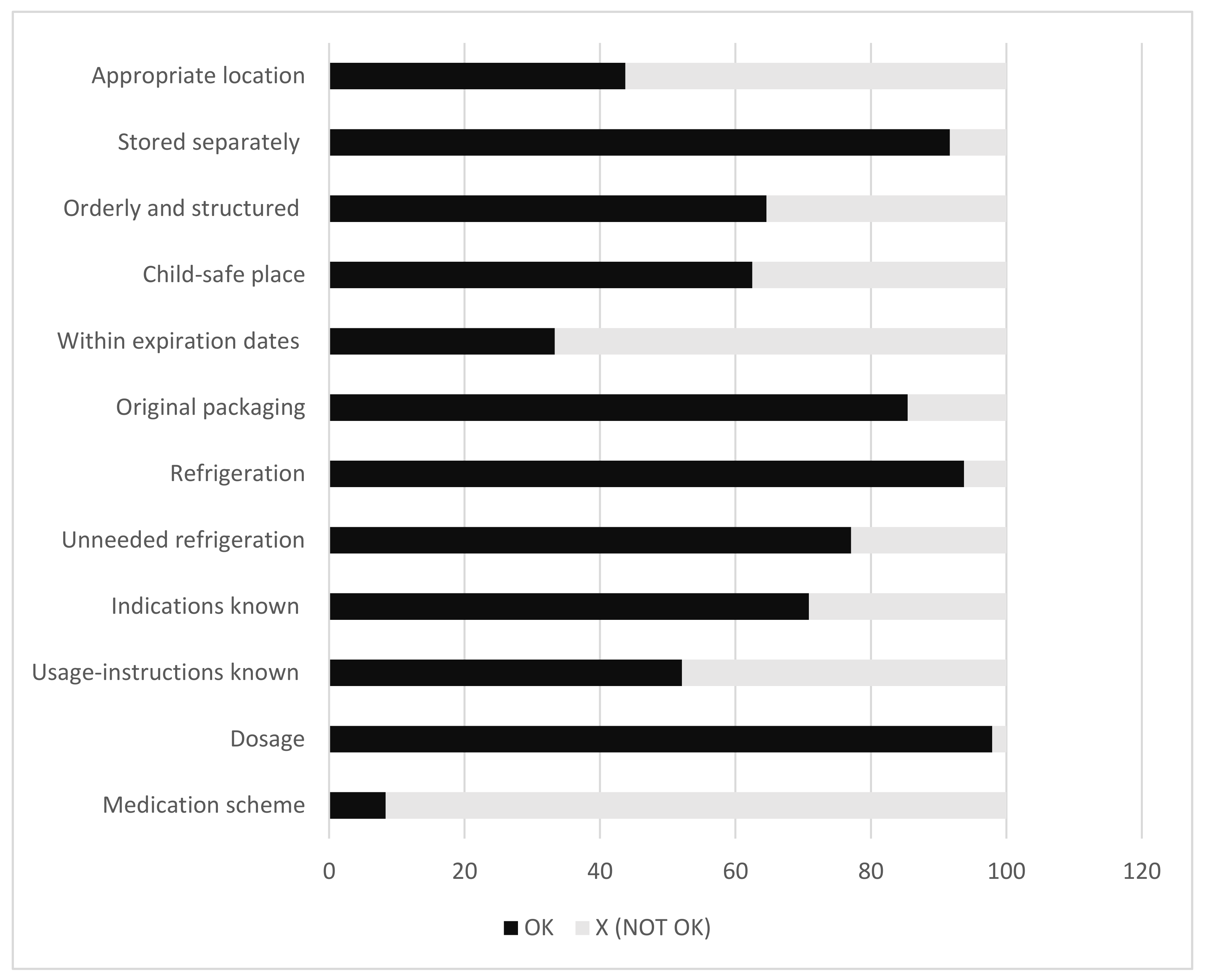
3. Results
4. Discussion and Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
| Question/Statement |
| Location |
| Where are medicines stored at home? |
| What kind of storage is used? |
| Are medicines stored in an orderly/structured way? |
| Is the medication kept out of the reach of children? |
| Refrigeration |
| Are medicines needing refrigeration present? |
| Are medicines that do not need refrigeration present in the refrigerator? |
| Medication |
| Are expired medicines present? |
| Are the products stored in their original packaging? |
| Are the indications of the medicines known? |
| Are you familiar about how the medication is used? |
| Medication scheme/plan |
| Are the patients aware what medicine should be taken at what moment? |
| Is a Medication scheme/plan present? |
References
- Tong, A.Y.; Peake, B.M.; Braund, R. Disposal practices for unused medications around the world. Environ. Int. 2011, 37, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.H.J.; Doshi, M.; Mason, N.A. Analysis of medications returned during a medication take-back event. Pharmacy (Basel) 2015, 3, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Ceaser, S.; Wurtz, R. Leftover antibiotics in the medicine cabinet. Ann. Intern. Med. 2000, 133, 74. [Google Scholar] [CrossRef] [PubMed]
- De Bolle, L.; Mehuys, E.; Adriaens, E.; Remon, J.P.; Van Bortel, L.; Christiaens, T. Home medication cabinets and self-medication: A source of potential health threats? Ann. Pharmacother. 2008, 42, 572–579. [Google Scholar] [CrossRef] [PubMed]
- Akici, A.; Aydin, V.; Kiroglu, A. Assessment of the association between drug disposal practices and drug use and storage behaviors. Saudi Pharm. J. 2017, 26, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.D.; Wood, D.M.; Dargan, P.I. Internet survey of home storage of paracetamol by individuals in the UK. QJM Mon. J. Assoc. Phys. 2013, 106, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Reddy, A.; de la Cruz, M.; Rodriguez, E.M.; Thames, J.; Wu, J.; Chisholm, G.; Liu, D.; Frisbee-Hume, S.; Yennurajalingam, S.; Hui, D.; et al. Patterns of storage, use, and disposal of opioids among cancer outpatients. Oncologist 2014, 19, 780–785. [Google Scholar] [CrossRef] [PubMed]
- Schillie, S.F.; Shehab, N.; Thomas, K.E.; Budnitz, D.S. Medication overdoses leading to emergency department visits among children. Am. J. Prev. Med. 2009, 37, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Fraeyman, J.; Peeters, L.; Van Hal, G.; Beutels, P.; De Meyer, G.R.; De Loof, H. Consumer choice between common generic and brand medicines in a country with a small generic market. J. Manag. Care Spec. Pharm. 2015, 21, 288–296. [Google Scholar] [CrossRef] [PubMed]
- The National Kidney Foundation. 6 Tips to Help Spring Clean Your Medicine Cabinet. Available online: https://www.kidney.org/transplantation/transaction/TC/Spring14/6-Tips-Help-SpringClean-Your-Medicine-Cabinet (accessed on 5 June 2018).
- FDA. 3 Spring Cleaning Tips. Available online: https://www.fda.gov/ForConsumers/ByAudience/ForWomen/WomensHealthTopics/ucm551446.htm (accessed on 5 June 2018).
- Anonymous. Drugs past their expiration date. JAMA 2016, 315, 510–511. [Google Scholar] [CrossRef]
- Truong, H.A.; Layson-Wolf, C.; de Bittner, M.R.; Owen, J.A.; Haupt, S. Perceptions of patients on medicare part d medication therapy management services. J. Am. Pharm. Assoc. 2009, 49, 392–398. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Sample | Location | Storage | Use | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| House-Call Number | Age † | Children | Appropriate Location | Stored Separately | Orderly and Structured ∆ | Child-Safe Place | Within Expiration Dates | Original Packaging | Refrigeration | Unneeded Refrigeration | Indications Known § | Usage-Instructions Known § | Dosage Known | Medication Scheme |
| 1 | 3 | C | X | OK | OK | OK | X | OK | OK | OK | OK | OK+ | OK | X |
| 2 | 3 | C | X | X | OK | OK | X | OK | OK | OK | OK+ | OK+ | OK | X |
| 3 | 2 | B | OK | OK | X | X | X | OK | OK | OK | X | OK+ | OK | X |
| 4 | 2 | B | X | OK | OK | OK | X | OK | OK | X | OK+ | X | OK | X |
| 5 | 2 | B | OK | OK | X | OK | X | OK | OK | X | X | OK+ | OK | X |
| 6 | 3 | C | X | OK | X | OK | X | OK | OK | OK | X | X | OK | X |
| 7 | 2 | B | OK | OK | OK− | X | X | OK | OK | OK | OK+ | X | OK | X |
| 8 | 3 | C | OK | OK | OK− | X | X | X | X | OK | OK | OK | OK | X |
| 9 | 2 | C | X | X | OK− | OK | OK | OK | OK | X | OK | OK+ | OK | X |
| 10 | 3 | C | X | OK | OK− | X | OK | OK | OK | OK | OK+ | X | OK | X |
| 11 | 3 | C | X | OK | X | X | X | OK | OK | OK | X | X | OK | X |
| 12 | 1 | C | OK | OK | X | OK | OK | X | OK | OK | OK | OK+ | OK | X |
| 13 | 1 | A | OK | OK | OK | OK | X | OK | OK | OK | OK | OK+ | OK | X |
| 14 | 1 | A | OK | OK | OK− | X | OK | X | OK | OK | OK | OK+ | OK | X |
| 15 | 2 | C | OK | OK | OK− | OK | OK | OK | OK | OK | OK | OK+ | OK | X |
| 16 | 2 | A | X | X | X | OK | X | OK | OK | OK | X | X | OK | X |
| 17 | 1 | A | OK | OK | X | OK | X | OK | X | OK | OK | X | OK | X |
| 18 | 2 | B | OK | OK | OK | X | OK | OK | OK | X | OK | OK | OK | OK |
| 19 | 1 | A | OK | OK | OK | OK | X | OK | OK | OK | OK | OK+ | OK | X |
| 20 | 2 | B | OK | OK | X | OK | X | OK | OK | OK | X | X | OK | X |
| 21 | 1 | C | X | OK | X | OK | X | OK | OK | OK | X | X | OK | X |
| 22 | 2 | B | X | OK | OK | X | X | OK | OK | OK | X | X | OK | X |
| 23 | 3 | C | X | OK | OK | X | X | OK | OK | OK | X | X | OK | OK |
| 24 | 1 | A | X | OK | OK | X | X | OK | OK | X | OK | OK | OK | X |
| 25 | 1 | B | OK | OK | X | OK | OK | X | OK | OK | X | X | OK | X |
| 26 | 2 | C | X | OK | X | X | X | OK | OK | OK | OK+ | X | OK | X |
| 27 | 2 | C | X | OK | OK− | X | OK | OK | OK | OK | X | X | X | X |
| 28 | 3 | C | X | OK | OK | OK | OK | OK | OK | OK | X | OK+ | OK | X |
| 29 | 2 | B | X | OK | X | OK | X | X | OK | OK | X | X | OK | X |
| 30 | 3 | C | OK | OK | OK | X | X | X | OK | X | OK | OK | OK | OK |
| 31 | 3 | C | X | OK | OK− | OK | X | OK | OK | OK | OK+ | X | OK | X |
| 32 | 2 | B | OK | OK | X | OK | X | OK | OK | X | OK+ | X | OK | X |
| 33 | 2 | B | X | OK | OK | X | OK | OK | OK | X | OK | OK+ | OK | X |
| 34 | 2 | B | X | OK | X | X | OK | OK | OK | OK | OK | OK+ | OK | X |
| 35 | 2 | B | OK | OK | OK | OK | OK | OK | OK | OK | OK | X | OK | X |
| 36 | 3 | C | OK | OK | OK− | X | OK | OK | OK | OK | OK+ | OK+ | OK | OK |
| 37 | 2 | C | X | OK | X | OK | X | OK | OK | X | OK+ | X | OK | X |
| 38 | 1 | A | OK | OK | OK | OK | X | OK | OK | OK | OK | OK | OK | X |
| 39 | 2 | B | X | OK | OK− | OK | X | OK | OK | OK | OK+ | OK | OK | X |
| 40 | 1 | C | X | OK | X | X | X | OK | OK | OK | OK+ | X | OK | X |
| 41 | 2 | A | OK | OK | OK | OK | X | OK | OK | OK | OK | OK | OK | X |
| 42 | 3 | C | X | OK | OK− | OK | X | OK | OK | X | OK | X | OK | X |
| 43 | 2 | B | X | OK | OK | OK | OK | OK | OK | OK | OK | OK | OK | X |
| 44 | 2 | B | X | OK | OK | X | X | OK | OK | OK | OK | OK | OK | X |
| 45 | 2 | B | X | OK | OK | OK | OK | OK | OK | OK | OK | OK+ | OK | X |
| 46 | 1 | A | OK | OK | X | OK | OK | OK | OK | OK | OK+ | X | OK | X |
| 47 | 1 | A | X | X | OK− | OK | X | OK | X | X | X | X | OK | X |
| 48 | 2 | B | OK | OK | OK− | OK | X | X | OK | OK | OK | OK | OK | X |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Janssen, L.; Pieters, L.; De Loof, H. Pilot Study on the Utility and Feasibility of a House-Call Checkup of the Medicine Cabinet. Pharmacy 2018, 6, 74. https://doi.org/10.3390/pharmacy6030074
Janssen L, Pieters L, De Loof H. Pilot Study on the Utility and Feasibility of a House-Call Checkup of the Medicine Cabinet. Pharmacy. 2018; 6(3):74. https://doi.org/10.3390/pharmacy6030074
Chicago/Turabian StyleJanssen, Lore, Luc Pieters, and Hans De Loof. 2018. "Pilot Study on the Utility and Feasibility of a House-Call Checkup of the Medicine Cabinet" Pharmacy 6, no. 3: 74. https://doi.org/10.3390/pharmacy6030074