Evaluating the Effectiveness of Clinical Pharmacy Consultations on Nutrition, Physical Activity, and Sleep in Improving Patient-Reported Psychiatric Outcomes for Individuals with Mental Illnesses



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
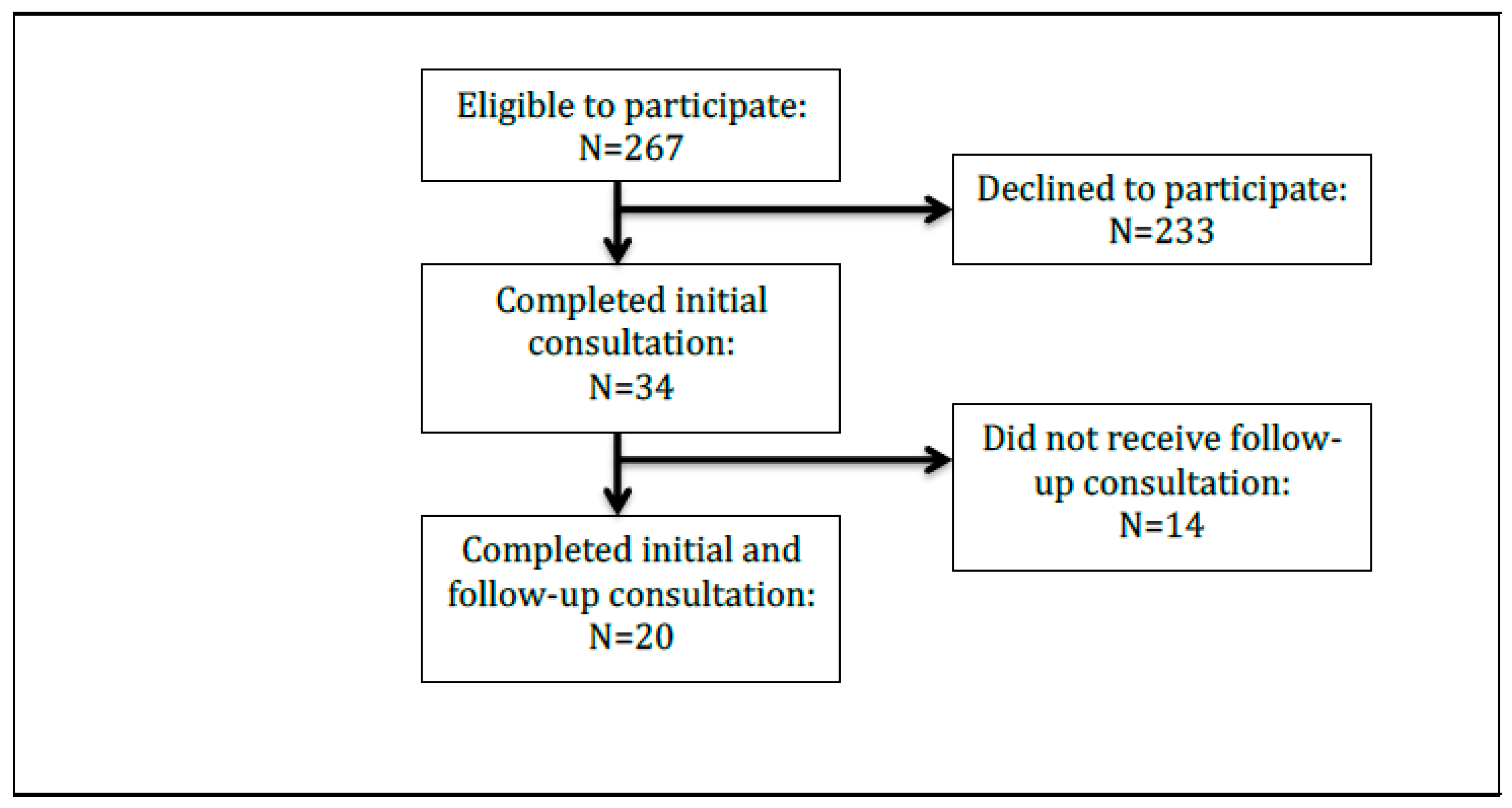
2.2. Study Sample
2.3. Initial Consultation (Intervention)
2.4. Physical and Mental Health Assessment
2.4.1. General Nutrition Counseling
- Assess patient dietary and supplement intake of essential nutrients required for optimal absorption, based on patient recall of a typical daily meal plan. Address apparent deficit(s) and make recommendations to supplement patient’s intake of these nutrients.
- Identify strategies (e.g., educate patient on integrating good food sources of essential nutrients or encourage tracking intake of essential nutrients) for achieving the Acceptable Macronutrient Distribution Range of 10–35% of healthy complete protein daily and creating individualized meal plans through open discussion, based on patient dietary restrictions, comorbidities, and financial barriers [12].
- Recommend smaller, more frequent meals throughout the day, when appropriate.
- Ensure alignment with prescribed medications for achieving optimal mental health status.
2.4.2. Serotonin-Targeting Psychotropic Medications
- Assess sources of complete protein, including all nine essential amino acids and L-tryptophan (e.g., meat, poultry, fish, dairy, eggs); sources containing all essential amino acids were deemed necessary for patients taking a serotonin-targeting psychotropic medication [17].
- Evaluate dietary intake of vitamins B6, B9, B12, and D3, as well as omega fatty acids for enzyme activation of tryptophan hydroxylase [17]. In cases where the patient reported dietary intolerance or avoidance of complete proteins, the pharmacist emphasized these precursors.
2.4.3. Norepinephrine and Dopamine-Targeting Psychotropic Medications
- Assess nutritional intake of essential amino acids phenylalanine and tyrosine, as well as vitamins B6, B9, B12, D3, and iron (for dopamine) for tyrosine hydroxylase activation.
- Encourage consumption of incomplete proteins containing phenylalanine and tyrosine (e.g., nuts, grains, beans, legumes, soy, or animal-based complete proteins).
2.4.4. Sleep Counseling
- Assess sleep quality and quantity based on the amount of patient-reported uninterrupted sleep received each night. Patients were advised to sleep at least seven hours per night, according to consensus guidelines [13].
- Educate on sleep hygiene, including the importance of maintaining a consistent routine (e.g., rising and going to bed at same time daily); removing distractions (i.e., computers, electronic devices, televisions, cellular phones); and avoiding large meals, physical activity, and stimulants (e.g., smoking, caffeine) before bedtime, per the Centers for Disease Control and Prevention recommendations [14].
2.4.5. Physical Activity Counseling
- Assess physical activity level. Patients were advised to engage in 150 minutes of physical activity each week per the Office of Disease Prevention and Health Promotion guidelines [15]. A personalized plan was created after the pharmacist and patient mutually agreed on a physical activity schedule that aligned with the patient’s normal routine (e.g., shorter sessions throughout the day if needed).
- Recommend consulting with their healthcare provider before starting a new program, and selecting physical activities of interest to help increase motivation and maintenance.
2.5. Follow-up Consultation (Intervention)
2.6. Data Collection and Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A: Call Scripts
- Serotonin helps with your mood. It is also what makes you feel happy. Your [medication name] needs serotonin to work.
- Norepinephrine helps with your response to stressful situations. It can also help with depression. Your [medication name] needs norepinephrine to work.
- Dopamine helps with your emotional response and mental focus. Your [medication name] needs dopamine to work.
- “I am going to ask you some questions about your diet to see if you are getting enough of the right foods for your body to build [serotonin/norepinephrine/dopamine].”
- “What does your daily meal plan look like?” Review with patient. Identify strengths within diet to build positive foundation. Identify/address cost-related barriers.
- “How often do you eat? It is recommended to eat every couple of hours during the day. Do not skip meals, particularly breakfast. When you eat, try to eat slowly over 30 minutes. It will allow your body time to absorb the nutrients better.”
- “Do you know which foods are classified as complete proteins? The greatest building blocks for [serotonin/norepinephrine] are things that you might already have in your kitchen. You can find them in beef, venison, buffalo, pork, fish, shellfish, cheese, cottage cheese, milk, yogurt, and eggs.”
- “Do you know which foods are classified as incomplete proteins? The building blocks for [norepinephrine/dopamine] are also found in your kitchen. In addition to eating complete proteins, it’s also important to eat incomplete proteins as well. You can find these in nuts, grains, beans, legumes, and soy.”
- “How many servings of protein do you eat in a day? Now that we know what types of protein you eat, it is important to talk about how much you consume to make sure you are getting enough to allow your medications to work their best.” Review with patient. Identify methods to achieve 3–4 servings of healthy protein daily intake.
- “What else is included on your meal plan?” Based on patient’s medication regimen, the pharmacist will follow the appropriate script below:
- “When we think about serotonin building blocks, key vitamins play an important role as well. Vitamin B6 is a great nutritional source of this vitamin, and is found in whole grains, vegetables, and nuts. Vitamin B12 is found in meats, fish, liver, and milk. Folic acid and Vitamin D3 are often found in fortified foods like dairy products, orange juice, and yogurt. Omega-3 Fatty Acids are found in fish, dairy products, and grains.”
- “When we think about norepinephrine building blocks, key vitamins play an important role as well. Folic acid is often found in fortified foods like dairy products, orange juice, and yogurt. Vitamin B12 is found in meats, fish, liver, and milk.”
- “When we think about dopamine building blocks, key vitamins play an important role as well. Vitamin B6 is a great nutritional source of this vitamin, and is found in whole grains, vegetables, and nuts. Folic acid is often found in fortified foods like dairy products, orange juice, and yogurt. Vitamin B12 is found in meats, fish, liver, and milk. Iron is also a key player. It is found in beans, leafy greens, and fortified cereals.”
- “How many hours of sleep do you get on average per night?” Adults 18 to 60 years should sleep at least seven hours per night.
- “Do you have trouble with sleeping?” If patient answers yes, ask for more details. Review relevant sleep hygiene tips (online: https://www.cdc.gov/sleep/about_sleep/sleep_hygiene.html).
- “How would you describe your physical activity? Being physically active is important not only for heart health, but also for mental health. It is recommended to be physically active for 30 minutes a day, five times a week. Another option is to break it up. If you have a busy schedule, try dividing your time into two or three segments of 10 to 15 minutes per day. Do not start a new exercise program without talking with their doctor first.” Ask the patient what types of physical activity they like to do. Motivational counseling.
References
- Kessler, R.C.; Angermeyer, M.; Anthony, J.C.; DEGraaf, R.; Demyttenaere, K.; Gasquet, I.; DEGirolamo, G.; Gluzman, S.; Gureje, O.; Haro, J.M.; et al. Lifetime prevalence and age-of-onset distributions of mental disorders in the World Health Organization’s World Mental Health Survey Initiative. World Psychiatry 2007, 6, 168–176. [Google Scholar] [PubMed]
- National Institute of Mental Health. Available online: https://www.nimh.nih.gov/health/statistics/mental-illness.shtml (accessed on 8 August 2018).
- Results from the 2016 National Survey on Drug Use and Health. Available online: https://www.samhsa.gov/data/sites/default/files/NSDUH-FFR1-2016/NSDUH-FFR1-2016.htm (accessed on 8 August 2018).
- National Association of State Mental Health Program Directors. Available online: https://www.nasmhpd.org/sites/default/files/Mortality%20and%20Morbidity%20Final%20Report%208.18.08.pdf (accessed on 8 August 2018).
- Reeves, W.; Strine, T.; Pratt, L.; Thompson, W.; Ahluwalia, I.; Dhingra, S.; McKnight-Eily, L.; Harrison, L.; D’Angelo, D.V.; Williams, L.; et al. CDC Report: Mental Illness Surveillance Among Adults in the United States. MMWR Morb. Mortal. Wkly. Rep. 2011, 60, 1–32. [Google Scholar]
- Kline, C. The bidirectional relationship between exercise and sleep: Implications for exercise adherence and sleep improvement. Am. J. Lifestyle Med. 2014, 8, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Lopresti, A.L.; Hood, S.D.; Drummond, P.D. A review of lifestyle factors that contribute to important pathways associated with major depression: Diet, sleep and exercise. J. Affect. Disord. 2013, 148, 12–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rössler, W. Nutrition, sleep, physical exercise: Impact on mental health. J. Eur. Psychol. 2016, 33, S12. [Google Scholar] [CrossRef]
- Mayo Clinic. Available online: https://www.mayoclinic.org/diseases-conditions/depression/in-depth/depression-and-exercise/art-20046495 (accessed on 8 August 2018).
- Finley, P.; Crismon, M.; Rush, A. Evaluating the impact of pharmacists in mental health: A systematic review. Pharmacotherapy 2003, 23, 1634–1644. [Google Scholar] [CrossRef] [PubMed]
- Parkerson, G.R., Jr.; Broadhead, W.E.; Tse, C.K. The Duke Health Profile. A 17-item measure of health and dysfunction. Med. Care 1990, 28, 1056–1072. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, R.R.; Cifelli, A.M.; Kostas, G.; Kim, I.-Y. Optimizing Protein Intake in Adults: Interpretation and Application of the Recommended Dietary Allowance Compared with the Acceptable Macronutrient Distribution Range. Adv. Nutr. 2017, 8, 266–275. [Google Scholar] [CrossRef] [Green Version]
- Watson, N.F.; Badr, M.S.; Belenky, G.; Bliwise, D.L.; Buxton, O.M.; Buysse, D.; Dinges, D.F.; Gangwisch, J.; Grandner, M.A.; Kushida, C.; et al. Recommended amount of sleep for a healthy adult: A joint consensus statement of the American Academy of Sleep Medicine and Sleep Research Society. Sleep 2015, 38, 843–844. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/sleep/about_sleep/sleep_hygiene.html (accessed on 8 August 2018).[Green Version]
- Office of Disease Promotion and Health Promotion. Available online: https://health.gov/paguidelines/guidelines/adults.aspx (accessed on 8 August 2018).
- Duke Community & Family Medicine. Available online: https://cfm.duke.edu/research/duke-health-measures (accessed on 26 September 2018).
- Bingham, J. What You Need to Know about Behavioral Health Medications. WellRx. Available online: https://news.wellrx.com/2017/07/24/what-you-need-to-know-about-behavioral-health-medications/ (accessed on 2 December 2018).
- REDCap. Available online: https://projectredcap.org/ (accessed on 13 December 2018).
- Simon, G.E.; VonKorff, M.; Rutter, C.; Wagner, E. Randomised trial of monitoring, feedback, and management of care by telephone to improve treatment of depression in primary care. BMJ 2000, 320, 550–554. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, J.M.; Alegría, M.; Prihoda, T.J.; Copeland, L.A.; Zeber, J.E. How the Relationship of Attitudes toward Mental Health Treatment and Service Use Differs by Age, Gender, Ethnicity/Race and Education. Soc. Psychiatry Psychiatr. Epidemiol. 2011, 46, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Ojeda, V.D.; McGuire, T.G. Gender and Racial/Ethnic Differences in Use of Outpatient Mental Health and Substance Use Services by Depressed Adults. Psychiatr. Q. 2006, 77, 211–222. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.S.; Lane, M.; Olfson, M.; Pincus, H.A.; Wells, K.B.; Kessler, R.C. Twelve-month Use of Mental Health Services in the United States: Results from the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 629–640. [Google Scholar] [CrossRef] [PubMed]
- Villatoro, A.P.; Mays, V.M.; Ponce, N.A.; Aneshensel, C.S. Perceived Need for Mental Health Care: The Intersection of Race, Ethnicity, Gender, and Socioeconomic Status. Soc. Ment. Health 2018, 8, 1–24. [Google Scholar] [CrossRef]
- Jang, Y.; Park, N.S.; Young Kang, S.; Chiriboga, D.A. Racial/Ethnic Differences in the Association between Symptoms of Depression and Self-rated Mental Health among Older Adults. Community Ment. Health J. 2014, 50, 325–330. [Google Scholar] [CrossRef]
- Anglin, D.M.; Albertic, P.M.; Link, B.G.; Phelan, J.C. Racial Differences in Beliefs about the Effectiveness and Necessity of Mental Health Treatment. Am. J. Community Psychol. 2008, 42, 17–24. [Google Scholar] [CrossRef]
- Jimenez, D.E.; Bartels, S.J.; Cardenas, V.; Dhaliwal, S.S.; Alegría, M. Cultural Beliefs and Mental Health Treatment Preferences of Ethnically Diverse Older Adult Consumers in Primary Care. Am. J. Geriatr. Psychiatry 2012, 20, 533–542. [Google Scholar] [CrossRef] [Green Version]
- Taylor, R.J.; Woodward, A.T.; Chatters, L.M.; Mattis, J.S.; Jackson, J.B. Seeking Help from Clergy among Black Caribbeans in the United States. Race Soc. Probl. 2011, 3, 241–251. [Google Scholar] [CrossRef]
- Woodward, A.T.; Chatters, L.M.; Taylor, R.J.; Neighbors, H.W.; Jackson, J.S. Differences in Professional and Informal Help Seeking among Older African Americans. Black Caribbeans, and Non-Hispanic Whites. J. Soc. Soc. Work Res. 2010, 1, 124–139. [Google Scholar] [CrossRef]
- Cook, B.L.; Zuvekas, S.H.; Carson, N.; Wayne, G.F.; Vesper, A.; McGuire, T.G. Assessing Racial/Ethnic. Disparities in Treatment across Episodes of Mental Health Care. Health Serv. Res. 2014, 49, 206–221. [Google Scholar] [CrossRef]
- Morin, P.; Herrmman, F.; Ammann, P.; Uebelhart, B.; Rizzoli, R. A rapid self-administered food frequency questionnaire for the evaluation of dietary protein intake. Clin. Nutr. 2005, 24, 768–774. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.W.; Borowski, L.A.; Liu, B.; Galuska, D.A.; Signore, C.; Klabunde, C.; Huang, T.T.-K.; Krebs-Smith, S.M.; Frank, E.; Pronk, N.; et al. U.S. Primary Care Physicians’ Diet, Physical Activity, and Weight-Related Care of Adult Patients. Am. J. Prev. Med. 2011, 41, 33–42. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | N (%) |
|---|---|
| Age (in years) | |
| 20–30 | 4 (20) |
| 31–40 | 8 (40) |
| 41–50 | 6 (30) |
| ≥51 | 2 (10) |
| Gender | |
| Female | 12 (60) |
| Male | 8 (40) |
| Ethnicity | |
| Not Hispanic or Latino | 12 (60) |
| Race | |
| American Indian or Alaska Native | 0 (0) |
| White | 12 (60) |
| Asian | 0 (0) |
| Black or African American | 1 (5) |
| Unknown | 7 (35) |
| Profile Scale Scores | Baseline Mean (SD) | Follow up Mean (SD) | p-value |
|---|---|---|---|
| Physical | 54.5 (21.9) | 74.5 (17.9) | 0.007 |
| Mental | |||
| Anxiety | 49.6 (26.1) | 35.8 (17.7) | 0.025 |
| Depression | 53.5 (31.2) | 31.0 (18.3) | 0.001 |
| Anxiety-depression scale | 49.3 (31.8) | 29.3 (18.4) | 0.005 |
| Overall | 50.8 (29.7) | 32.0 (18.1) | 0.010 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bingham, J.; Axon, D.R.; Scovis, N.; Taylor, A.M. Evaluating the Effectiveness of Clinical Pharmacy Consultations on Nutrition, Physical Activity, and Sleep in Improving Patient-Reported Psychiatric Outcomes for Individuals with Mental Illnesses. Pharmacy 2019, 7, 2. https://doi.org/10.3390/pharmacy7010002
Bingham J, Axon DR, Scovis N, Taylor AM. Evaluating the Effectiveness of Clinical Pharmacy Consultations on Nutrition, Physical Activity, and Sleep in Improving Patient-Reported Psychiatric Outcomes for Individuals with Mental Illnesses. Pharmacy. 2019; 7(1):2. https://doi.org/10.3390/pharmacy7010002
Chicago/Turabian StyleBingham, Jennifer, David R. Axon, Nicole Scovis, and Ann M. Taylor. 2019. "Evaluating the Effectiveness of Clinical Pharmacy Consultations on Nutrition, Physical Activity, and Sleep in Improving Patient-Reported Psychiatric Outcomes for Individuals with Mental Illnesses" Pharmacy 7, no. 1: 2. https://doi.org/10.3390/pharmacy7010002