1. Introduction
To date, particular emphasis has been placed upon data analysis mostly in the technological field. Digital technologies influence every single industry sector and the economy as a whole. Even though access to healthcare may vary across countries, communities, and individuals, it is considered to be one of the most important sectors in every economy. A stronger relationship between healthcare and digital technologies leads to a new era of e-health and a new way of managing the healthcare. E-health provides the opportunity to get data from patients, medical facilities, and hospitals to one place at the same time. It ensures the quality and safety of care, continuity of services, and cost containment. As it is known in variety of countries, e-health is one way to make work easier and more effective.
The adoption of the information and communication technologies in healthcare systems requires the cooperation between the management level of organizations as well as the practitioners who are the end users of the information and communication technologies. It involves users at different development and implementation phases, using project champions or other key staff, providing adequate training and support, and monitoring the system use in the early stages of implementation. Different factors influence the success or failure of the information and communication technologies’ implementation.
A poor quality of care and an inefficiency deriving from inconsistent processes puts the healthcare system at risk. One of the strategies that is supposed to make healthcare systems more durable is to invest in information and communication technologies. The information and communication technologies implemented in healthcare are widely known as the health information technologies, which include the electronic health records, telemedicine, and the computerised collections of all of the daily processes of the healthcare providers.
However, the adoption of a healthcare information system could become a failure when the human factor fails, therefore, the human factor should be one of the key elements in the management system. Nowadays, a managerial method exists that allows for a more efficient and effective use of all of the available resources. Despite of the fact that health information technologies are supposed to improve the quality and safety of care, healthcare access, and the optimisation of the cost of healthcare, not every new technology improves the health outcomes. The problem is the inability to predict whether new technology will be effective or not. Even though implemented technology could lower the everyday costs of healthcare institutions, the initial investment of it is high.
2. Literature Review
There are many studies exploring the healthcare sector. However, the management system of the healthcare facilities is often described only from the point of view of the carried out processes. Only a few of these studies are devoted to the information system applied in the healthcare facilities specifically. The following lines introduce these studies.
The studies that determine the implementation of the information and communication technologies in healthcare tend to provide general information on how the implementation of the information and communication technologies improve the whole system of providing healthcare (
Gastaldi and Corso 2012). One of the key elements of the successful information and communication technologies implementation is its payoff (
Devaraj and Kohli 2000). According to
Gagnon et al. (
2012), the information and communication technologies’ adoption is complex, multi-dimensional, and influenced by a variety of factors at individual and organisational levels.
The healthcare facility information system may become a useful instrument for knowing how to deal with a growing number of patients. It allows for managing operations including admissions and transfers, and the results of the laboratory test, and so on. The information system in the hospital may decrease the amount of work and, in this way, be able to assist in reducing the costs linked to these kinds of operations (
Sharon Ross and Venkatesh 2016).
Nowadays, big data has evolved as a monitoring tool for the information and communication technologies. As a tool for this, it detects the relevant patterns that were previously unknown. As the healthcare information systems are provided by a variety of producers, the big data analysis has to deal with the differences of the various system and database architecture; a key challenge is faced when synchronizing the data from various sources (
Chauhan et al. 2017). Real and efficient cooperation between healthcare facilities or even their organisational units is not possible (
Hammami et al. 2014;
Zdravković et al. 2014). The combination of data from different departments like laboratory, radiology, admission wards, and medicine supply store are needed. The differences in the databases and the format of the data of different departments makes it difficult to have interoperability and an exchange with all of these systems and the health information system (
Walker et al. 2005;
Middleton 2006;
Marchibroda 2007;
Jardim 2013). MongoDB, MarkLogic, and Apache Cassandra, known as one of the new database management systems, allow for data to be transferred between the traditional and new operating systems (
Wang et al. 2018).
The information and communication technologies used by all types of healthcare providers facilitate the electronic capture, storage of different kinds of patient data and also allows to share these data. It could be used to detect diseases at earlier stages, to manage specific individual and population health, and to detect healthcare fraud more efficiently (
Raghupathi 2014). Even though the information and communication technologies make the work easier, and healthcare professionals do not use all of its potential. Healthcare organisations are noticeably lagging behind in the adoption of these technologies (
Tole 2013). There are the barriers associated with the implementation of a healthcare information system. These barriers are usually connected to the organisational management and the interrelations (
Lluch 2011).
According to
Sharon Ross and Venkatesh (
2016), the implementation of e-health is influenced by different types of factors. The key factors for the implementation of e-health are the legislation and recognised standards. As the whole process of adoption depends on the purpose that the information system is used for, it is necessary to split the factors between these processes. The authors have diverse opinions on what the most important factors are for the management systems. These factors are the innovation source (
Archer et al. 2011;
Boonstra and Broekhuis 2010;
Sharon Ross and Venkatesh 2016), evidence of strength and quality (
Boonstra and Broekhuis 2010;
Benavides-Vaello et al. 2013;
Broens et al. 2007;
Demaerschalk et al. 2009;
Fontaine et al. 2010;
Stolee et al. 2010;
Sharon Ross and Venkatesh 2016), adaptability (
Sharon Ross and Venkatesh 2016;
Archer et al. 2011;
Boonstra and Broekhuis 2010;
Demaerschalk et al. 2009;
Gagnon et al. 2012;
Fontaine et al. 2010;
Gagnon et al. 2014;
Goldstein et al. 2014;
Kukafka et al. 2003;
Lu et al. 2005;
Ludwick and Doucette 2009), (
McGinn et al. 2011), triability (
Sharon Ross and Venkatesh 2016;
McGinn et al. 2011), complexity (
Boonstra and Broekhuis 2010;
Goldstein et al. 2014;
Lu et al. 2005;
Mack et al. 2009;
McGinn et al. 2011), design quality and packaging (
Boonstra and Broekhuis 2010;
Broens et al. 2007;
Lau et al. 2012;
Sharon Ross and Venkatesh 2016), patient needs and resources (
Jarvis-Selinger et al. 2008;
Jennett et al. 2004;
Lu et al. 2005;
McGinn et al. 2011)], networks and communication (
Sharon Ross and Venkatesh 2016;
Demaerschalk et al. 2009;
Jennett et al. 2004;
Lluch 2011;
Ludwick and Doucette 2009), and culture (
Sharon Ross and Venkatesh 2016;
Demaerschalk et al. 2009;
Lau et al. 2012).
Efficient hospital management may lead to a deduction in the administration costs and reductions of progressive loans (
Cline and Luiz 2013). The proposed solution to manage the stock more efficient is the kanban logic (
Jaana et al. 2011). In a hospital in Seville, Spain, the adoption of the kanban system facilitates the order systems in the hospital. Therefore, it can be said that it helps to improve the managerial system. It shortens the time needed to order the materials in the hospital.
Other processes that may be optimised by using the kanban system are the processes in the warehouse of the hospital. The study by
Jaana et al. (
2011) compares the efficiency of a hospital before and after maintaining of the kanban system. The result of maintaining this system is that the quantities of ordered stocks were reduced by up to 80%. (
Persona et al. 2008). The analysis of the costs linked to the implementation of the healthcare information system shows that the optimal healthcare information system applications should be implemented. Usually, the implementation of the information and communication technologies in the healthcare facilities is limited to the use of computers. The evidence of the successfully implemented health information technology, organisational changes, and costs are missing (
Lluch 2011).
Only a few authors have studied the impact of smart healthcare digitalisation in healthcare facilities through the exploration and exploitation their assets. In the study by
Gastaldi and Corso (
2012), the authors affirm that digitisation allows for the efficient use of hospital assets, which may improve the overall quality of the healthcare they provide. The analysis (
Saluvan and Ozonoff 2018) has shown that the functional healthcare information systems relate to improved quality and patient safety.
From the so-called institute of medicine, the National Academy of Medicine,
Gelijns and Halm (
1991) has studied the benefits and cost of healthcare in the context of the diffusion of new technology. An investment in technology that prevents disease may eliminate the costs required for the diagnosis and treatment needed in the case of an insufficient preventive process. The approaches that do not distinguish between the impacts of new and existing technologies are problematic. A highly cost-efficient technology in one situation can be exceedingly inefficient in others. Increased costs due to new technologies may increase the savings of the healthcare resources. This increase in the savings of resources may higher be in some clinical uses than the cost of technology.
The quality of healthcare and all of the services provided by the healthcare institutions is expressed by the satisfaction of the patients. Therefore, the outcome of the healthcare institutions is satisfaction with the services (
Gastaldi and Corso 2012). The determination of the hospital’s healthcare level is (
Ratnaningtyas and Surendro 2013) influenced by the information quality. Hence, the quality of information is the key element in the healthcare facility. The reduction of information variance in the healthcare process may be reached using one of the methods for improving the quality of information—Six Sigma. An investment in information technology leads to organisational profitability. There is evidence that a combination of business process re-engineering and investment affects profitability (
Devaraj and Kohli 2000). However, the results of the digitalisation processes are diverse, as errors often occur during the implementation phase, but a good management system is inevitable (
Sharon Ross and Venkatesh 2016).
Demographic development leads to a structural shortage of health professionals. The adoption of the information and communication technologies in healthcare is lagging behind other sectors. A development in the software will bring the nursing information to the location where the nurses actually are (
Bakker 2002). The authors Haluza and
Jungwirth (
2015) affirm that the information and communication technologies offer a huge opportunity to face the challenges of aging societies. The information and communication technologies may be used for everyday assistance that offers independence and self-care to the patients with different kinds of disabilities. The healthcare costs continue to rise as technological progress is its main driver. As healthcare resources are limited, the main point of the necessary analysis is to decide whether older less expensive treatments are not enough to cover the present needs of the patients (
Hentschker and Wübker 2016).
3. Methodology
The whole data set consists of 51 healthcare facilities throughout the whole Slovak Republic. Each organisation is assigned a fundamental attribute showing the legal form of the institution.
The data comes from the survey, “An Evaluation of the Management of the Information Systems (IS) and Technologies (IT) in Hospitals (Gesiti – Hospitals)”, from the Technical University of Košice, Slovakia, conducted in 2014. Its collection is assigned to the period of 2011 to 2013.
The elementary division of the healthcare facilities is according to their legal form—the following six types of legal forms are applied for all of the healthcare facilities in the Slovak Republic:
119—non-profit organisation;
121—joint-stock company;
301—state-owned enterprise;
321—budgetary organisation;
331—public-benefit organisation; and
382—public institution.
The codes applied for the individual legal forms of the organisations come from the dial of the Statistical Office of the Slovak Republic. These codes are applied in all of the tables in the paper.
The explored questions relate to the research of the information and communication technologies in the form of health information systems, as well as their investment into them in relation to the usage of the database types. The elementary hypothesis is that the healthcare facilities do not efficiently use the information systems in terms of the not absolutely complete usage of the information system features or their usage in an inappropriate way. Further research is aimed at finding of the means that are used in relation to these information systems.
The fundamental analytic approach is the self-organising map or is sometimes called the self-organising feature map. It is a type of artificial neural network, displaying a discrete representation of the input database. In this case, the two-dimensional method has been selected. The rectangular shape of the self-organising maps has been applied (
Kohonen 1982).
The whole analysis is done in an R statistical environment and the self-organising maps are produced using the kohonen package.
4. Results
The elementary division of the explored healthcare facilities in the Slovak Republic reveal that, according to their legal form, there are 20 public-benefit organisations, 17 non-profit organisations, 6 joint-stock companies, 3 state-owned enterprises, 3 public institutions, and 2 budget organisations. Based on this division, the rest of the analysis was carried out.
Firstly, there is a small introduction to the research and development in the questionnaire. The first three tables are devoted to this entrance to the topic, and subsequently, the three main sections, namely, technological innovations, investment into information and communication technologies, and usage of database systems. Finally, the section regarding the usage of the database systems concludes the results chapter.
4.1. Technological Innovations
Technological innovations are the main issue of the first subchapter of the analysis outcome.
Table 1 demonstrates the activities of research and development in the period from 2011 to 2013.
There have been 34 research and development activities among all of the healthcare facilities in total, of which 25 of them are ongoing and 9 are occasional or have already ended.
The importance of these activities is perceived variously on four levels ascending from low through to medium, and to high importance, with a possibility of no relevancy. The results are shown in
Table 2.
Only five activities are declared by the healthcare facilities to have a high importance for them. It is a very interesting finding, because it points to a quite low level of prioritisation of their own activities. Such an approach can lead to degradation of the overall research and development importance. Subsequently 17 of the activities are stated to have medium importance and 9 of them are assigned low importance.
The importance can be evaluated also for gain of the external findings. It is revealed in the subsequent
Table 3.
This outcome demonstrates that gaining an external knowledge is of greater importance for the explored organisations. Whilst only five of them stated that external knowledge has a low importance for them, nine expressed their opinion that it possesses a high importance, and 16 stayed at a medium level. Not relevant is at a level of three.
There are also several questions involved in the questionnaire related to investment into this field. The intensive usage of the information and communication technologies is an assumption of the future improvement of the competition ability of the particular hospital, among the others. All of the respondents agreed with this statement, only four did not know what it would bring. Also, the usage of information and communication technologies increases the added value of the services provided by the healthcare facilities. Only one respondent expressed that the mentioned usage does not deliver any added value. The usage of information and communication technologies is fully supported by the headquarters of the healthcare facilities and it is declared to be an important factor of the efficiency of improving processes. Again, only one respondent said that it is not determined whether it helps or not. All of the others agreed with this statement.
A considerably different situation is the field of financing the information and communication technologies.
Table 4 demonstrates the presence of financial problems in the process of implementing new technologies.
A majority of the healthcare facilities are affected by financial problems. Almost each case related to financial problems is based on a lack of financial resources. Only one is associated with a widening of the network, one has a complicated and very long-lasting process of procurement, one case is characteristic in a way that financial sources are sufficient only to solve critical states, another case feels an absence of the widening needs, and, finally, one case is represented by the long-term problems with upgrades of the system.
Another issue related to the implementation of the information and communication technologies is the qualification of the employees that are responsible for it.
Table 5 demonstrates this problem.
Although the implementation process does not run ideally, a majority of the healthcare facilities declare that the staff have the sufficient qualification required to implement the information and communication technologies.
Another important point is to remain in a flow of the modern trend. This is managed by several activities, which belongs among a participation in fairs, meetings with the healthcare sector representatives, and the presence of innovation networks. The mechanisms to monitor the external elements are visualised in
Table 6.
Plenty of the healthcare facilities agree with the statement that there are mechanisms that were mentioned monitor external elements. Often as a response to the type of external element is the presence of stands at fairs, and meeting with representatives of the healthcare sector. Regarding the innovation networks, only five healthcare facilities are joint in these networks.
The questionnaire also asks for the type of external elements that are observed. They are visible in
Table 7.
Besides these possibilities, only one different option of the monitored external element was mentioned, and that is website traffic. As it is clearly seen from the previous table, none of the surveyed elements are observed by an unknown majority of healthcare facilities. This is a very crucial point, because it brings new light to the knowledge of how respondents work in this field. The worst situation is from a competitive aspect, where the activities done by the competing entities are observed only by five respondents, whilst 23 of them express no intention in this. From the point of view of technology, only nine respondents look for new information in this field, whilst 19 of them express no interest in the development of technological potential. The only almost balanced situation is in an observation of the client confidence, where 13 healthcare facilities monitor this external element and 15 do not pay attention to this issue.
4.2. Investment into Information and Communication Technologies
The second section of the analysis related to research and development is devoted to the investment into information and communication technologies.
One of the questions involved in this section of the questionnaire is linked to the potential field that can be innovated through the improvement of the information and communication technologies, in order to increase a competing ability of the healthcare facilities.
Table 8 demonstrates the answers of the respondents.
It is partially alarming that there are still the two healthcare facilities that does have no idea how the information and communication technologies can help them in the competing environment. Fortunately, a majority of the entities have a clue how to access the innovations.
Another question asks the respondents whether the mentioned investments are efficiently used and whether its return is satisfactory. The subsequent
Table 9 demonstrates the attitudes of the healthcare facilities for this issue.
It should be noted that the investment that has been brought into the information and communication technologies also involves investment in order to use and to implement the information systems. A majority of the surveyed healthcare facilities express no opinion about this statement. However, seven respondents were totally satisfied, and five of them were partially satisfied. On the other hand, five entities expressed partial dissatisfaction from these investments and one was totally dissatisfied. This outcome reveals that many healthcare facilities suggest that such an investment will not bring a positive effect for them in the future.
4.3. Usage of Database Systems
The last section of the results chapter is devoted to the usage of the database systems in the information systems of the healthcare facilities.
The first surveyed question relates to the usage of the central database itself.
Table 10 shows its state.
The focal point of the whole issue concerning the information systems lies in the usage of a central database. This represents the basement required in order to have an efficient information system nowadays. All of the entities, except for three public-benefit organisations, use the centralised type of database system. The remaining ones use the distributed type.
The timing of the future investment into to the hardware equipment for data storage is the topic of the next question. It is displayed in the succeeding
Table 11.
Most of the answers are stated as not relevant. This means that the healthcare facilities do not have a designed plan from a long-term point of view. The short-term plan is very rarely used in this field among the respondents. Financial planning for the period after 12 months is moderately difficult. It is also caused by the fact that the data storage devices represent a type of equipment that is subject to frequent changes.
4.4. Conformity of Variables
The found associations between the variables are visualised by self-organising maps. The usual structure of the analysis is applied—from the training process and the node counts through to the neighbour distance and the weight vectors, to the heat maps. The self-organising maps are produced by five dimensions in the both directions.
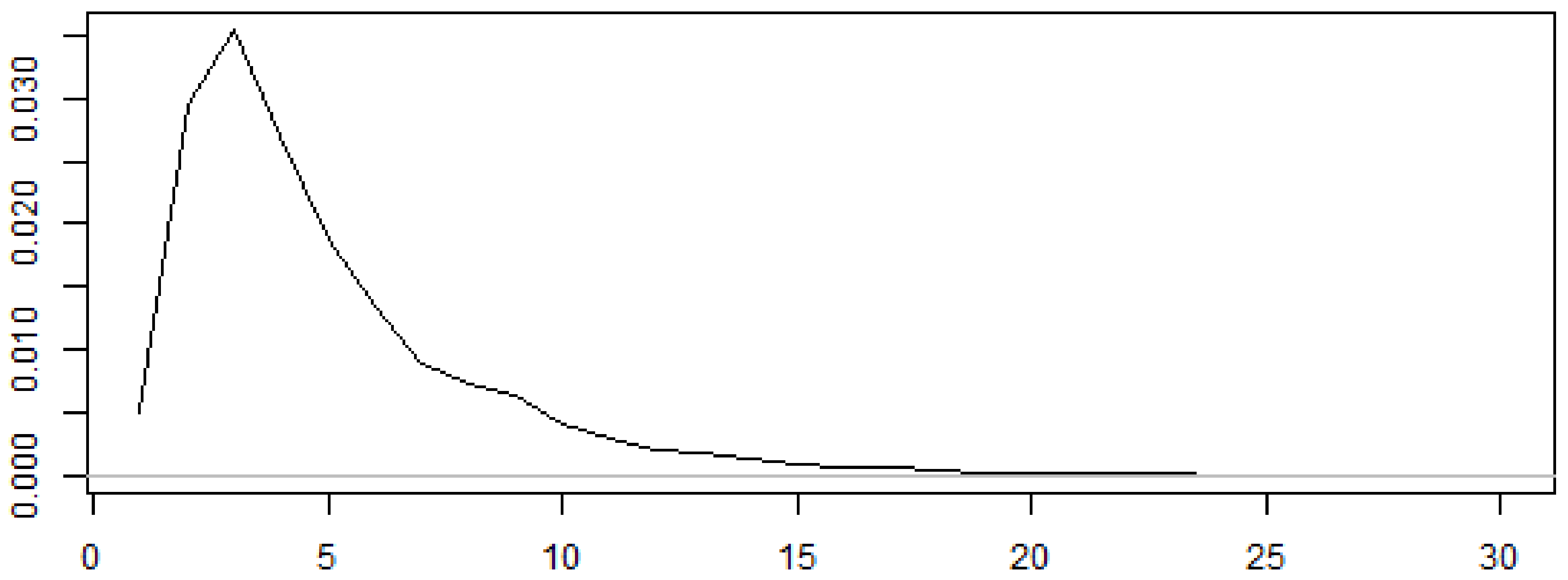
The training process is visualised by the following diagram in
Figure 1.
The
x-axis demonstrates the number of iterations and the
y-axis indicates the minimum distance to the closest unit from all of the remaining units. As seen in
Figure 1, the training process converges after 23 iterations. It means that all of the involved entities are located next to each other after this number of iterations.
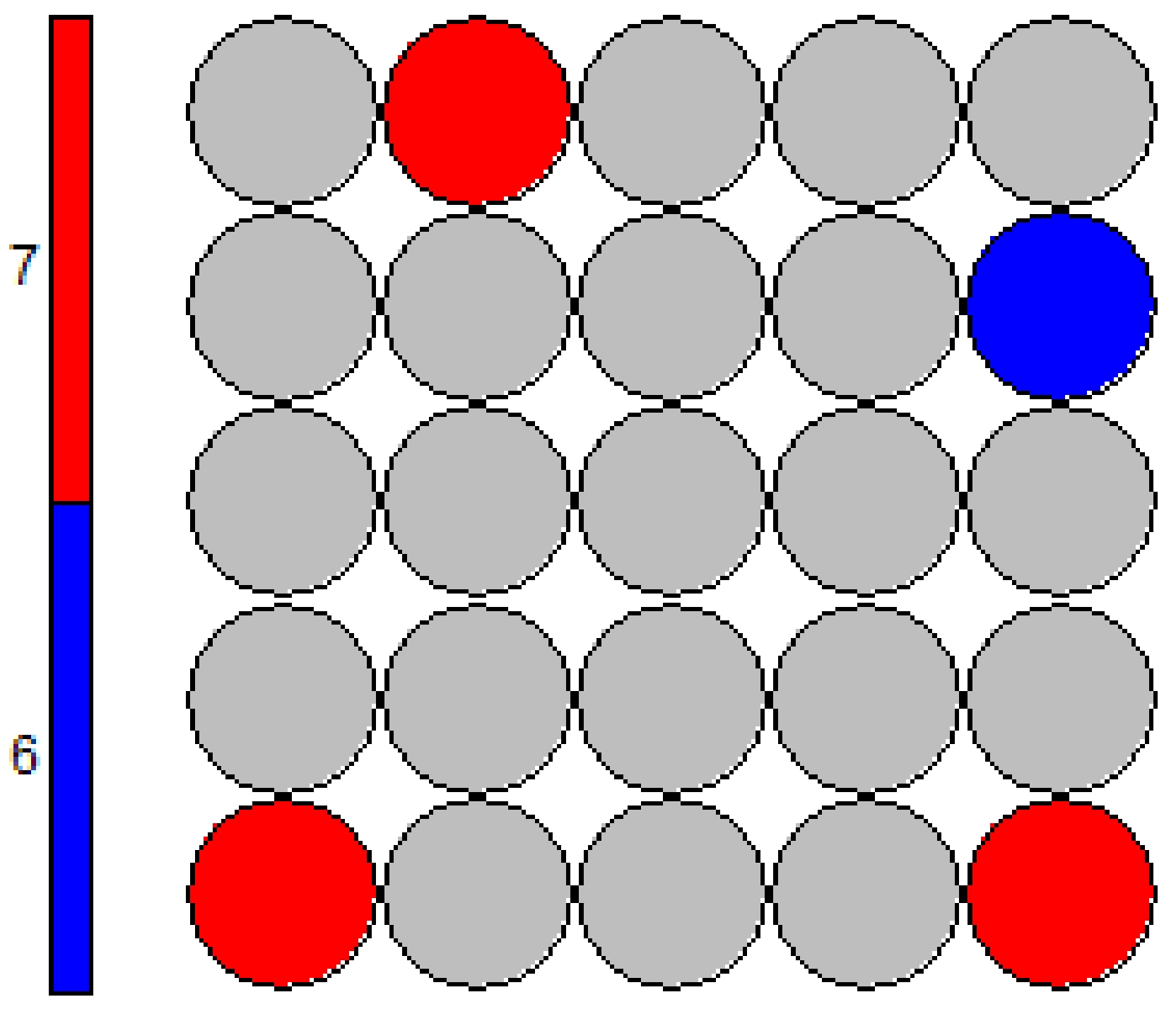
The node counts in
Figure 2 show the numbers of the different options selected by the respondents. In the following diagram, in
Figure 3, the neighbour distances are visible. The distances are rather short and the individual parts of the database are more similar than dissimilar. Only the three nodes are at the highest level of the distance measurement legend, and the sole node is at a level that lies a few degrees below it. A majority of the nodes are at an average level and at the levels situated a few degrees below it. This means that the answers of the respondents are partially differentiated for the same questions. This finding is based upon the differentiated replies for the individual survey queries. In the selection of this analysis, there were no questions that had answers that were consistent among the majority of the healthcare facilities.
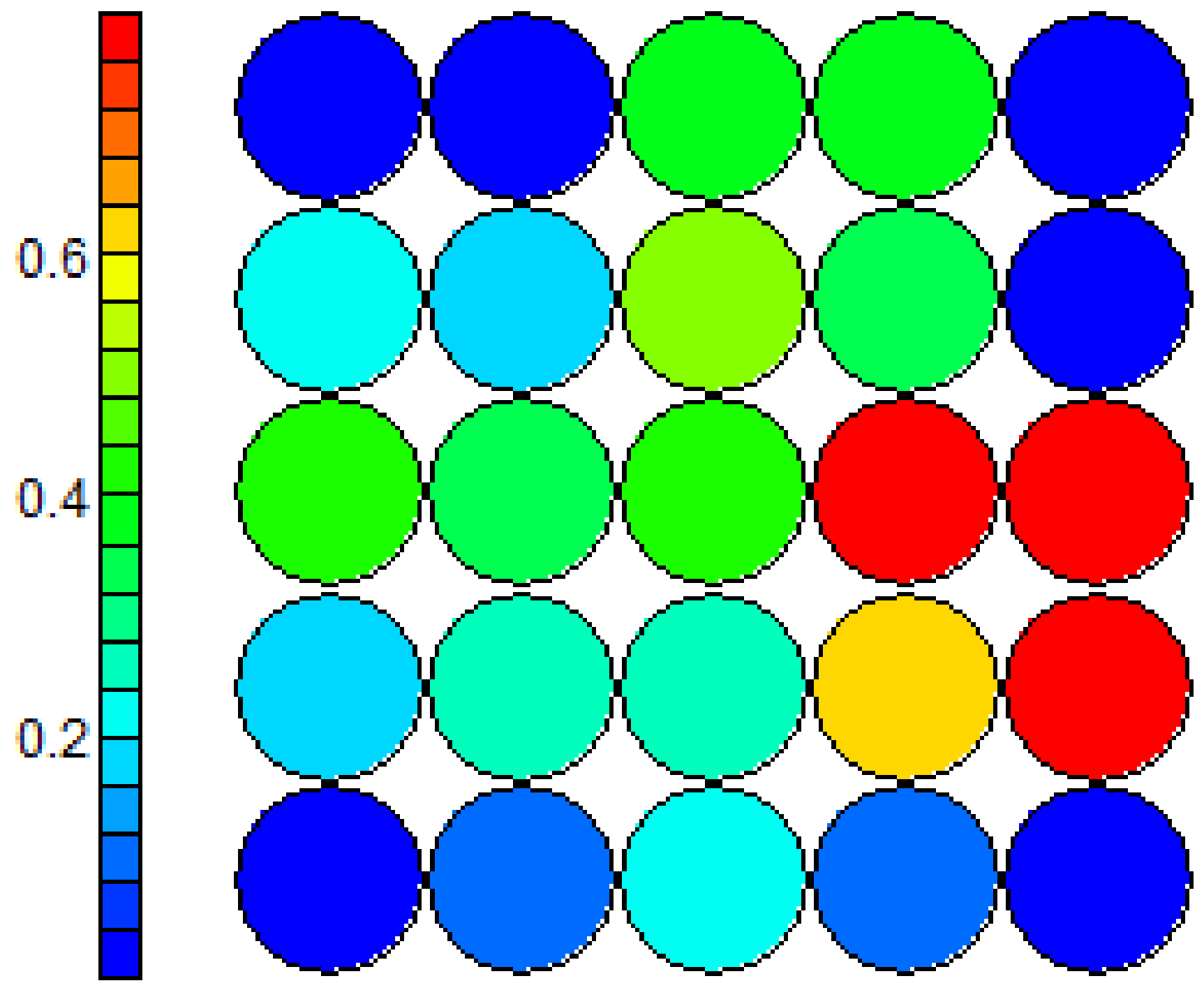
The heat maps in
Figure 4 and
Figure 5 demonstrate the distribution of the variables across the space. A comparison of these heat maps reveals another distribution of different answers from the survey. Here, it is visible that only minor alternations happen. Furthermore, only one movement is seen as the red circles from the first quadrant move to the third quadrant. Vice versa, this can be applied for the blue circles in the third quadrant too. This outcome demonstrates that there is little change between the two dimensions. It shows that the answers of the respondents are almost consistent.
5. Discussion
The discussion of the analysis outcome is partially difficult. This is because the analysis is carried out on the survey data. In spite of this, the desired outcome creates a platform for further research. That is why it is considerably demanding to determine the explicit statements as a part of the analysis result.
In Poland, the usage of databases to collect information about patients is inevitable. The healthcare facilities in the Slovak Republic plan to invest in hardware equipment for data storage in the future. More than half of the hospitals do not have the central databases to store data. Without an appropriate data storage system, the data analysis cannot be provided efficiently enough to be beneficial. Even the general results show that innovating organisations have become leaders of their own sectors, but not all employees would agree with that. All of the respondents agree that innovation has a high cost in Poland. There is also a similar situation in the Slovak Republic. However, the innovation is not declared to be so significant, and hence, the cost devoted to it at such a level is not considered to be important. That is why a lesser amount of money is devoted to this activity in the Slovak Republic. The cost of innovation is a basic obstacle that negatively affects the adoption and the implementation of the innovative practices and activities in hospitals (
Piasecka et al. 2015).
The main priority field in Bulgaria is to implement innovations into organisations in the healthcare sector. The three main points of the innovation processes are computerising, using databases to store information about patients, and the automation of the healthcare facility management. This is a plan that the Slovak Republic should keep to closely. The computerising process in the terms of the mechanisation of the procedures, is done in an electronic way. As it can be seen, the data storage and the database systems are in the future and take the biggest part of the innovation (
Vassileva and Balloni 2014).
This study bears a considerable number of limitations. Perhaps the biggest limitation lies in the structure of the database. There is quite a high number of unavailable data involved in the database. This makes the carried out analyses more difficult. The usage of the survey data is always a demanding field of complexity regarding the obtained data. The respondents are not always willing to fulfil the requirements of the surveyor. Another limitation is the market size of the healthcare facilities in the Slovak Republic. There are only several main institutions with a network of minor supporting healthcare facilities. Moreover, there is the limitation of a lack of implementation of the explored points throughout the whole set of the involved institutions.
6. Conclusions
Big data facilitates the analysis of information from an increasing variety of sources, namely, structured and unstructured, from medical records, electronic monitoring, and other devices. The inability to use the information and communication technologies more efficiently puts the public healthcare sector at risk of becoming an unsustainable system. The hospital information system can handle an increased flow of patients, remove duplication and unnecessary procedures, and so on. Statistics and data mining techniques lead to a better understanding of the patients’ conditions. Information and communication technologies have increased the growth of digitisation globally in the recent period, which produces millions of bytes in the form of data each day. Many organisations work to develop models from data resources with an analytics approach for developmental purposes.
Regardless, there are benefits to be gained from automation, and the information and communication technologies are now widely known as the way to raise the level of provided healthcare. It just depends on the quality of information from this point of view.
The innovation process or the business process redesign in hospitals used to be expensive, not only on its own, but also because of the all of the processes connected to this procedure. The cost of innovation is the basic obstacle that negatively affects the adoption and implementation of innovative practices and activities in healthcare facilities. While businesses have analysed data for decades, recent developments in computing have opened new doors and unleashed the potential of big data.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}