Systematizing Professional Knowledge of Medical Doctors and Teachers: Development of an Interdisciplinary Framework in the Context of Diagnostic Competences

 , ,
, ,
Abstract
:1. Introduction
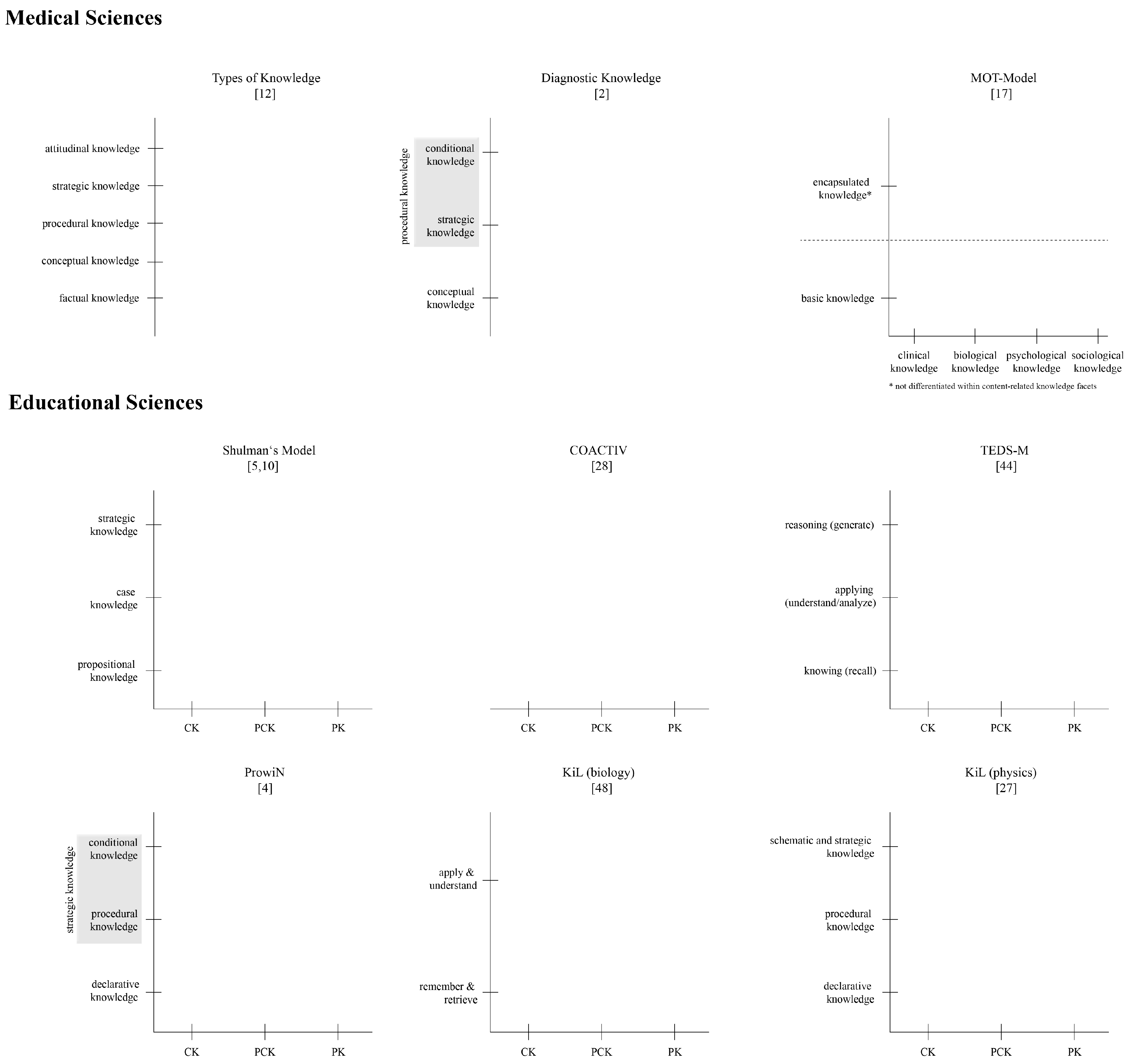
2. Recent Frameworks for Professional Knowledge in Medical and Educational Sciences
2.1. Medical Sciences
2.1.1. Types of Knowledge by Mayer
2.1.2. A Model of Diagnostic Knowledge
2.1.3. The MOT Model of Clinical Reasoning Processes
2.2. Educational Sciences
2.2.1. Content-Related Facets of Knowledge
2.2.2. Types of Professional Knowledge: Shulman’s Model and Realization in Different Projects
2.3. Summary
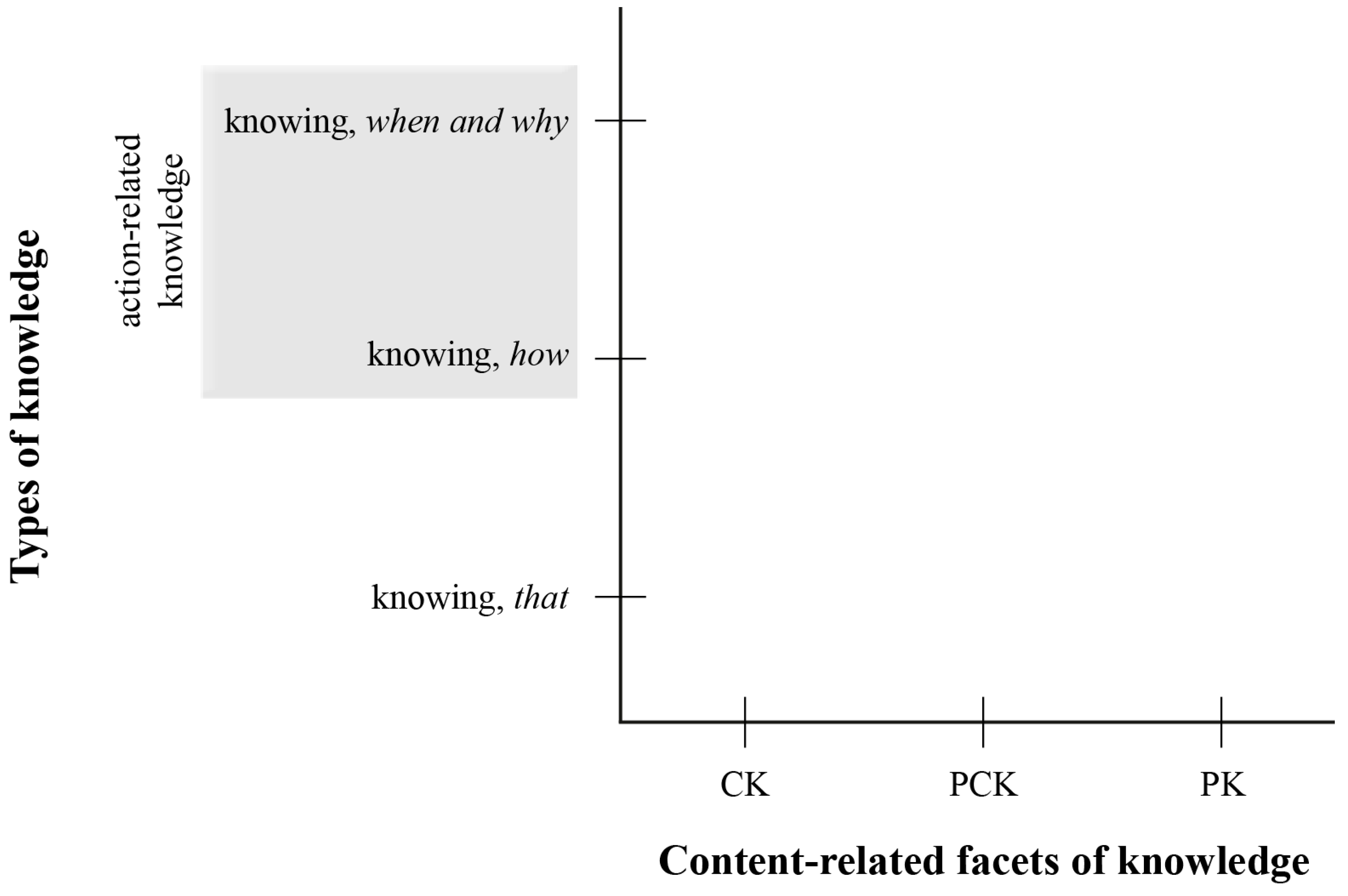
3. A Synthesis
3.1. Commonalities Between the Different Models Leading to a Two-dimensional Model
3.2. Domain-Specific Applications in the Context of Diagnosis
3.2.1. Medicine: Diagnosing Collaboratively During an Interprofessional Medical Ward Round
3.2.2. Mathematics: Diagnosing Individual Student’s Misconceptions Regarding Decimal Fractions
3.2.3. Biology: Diagnosing the Situation within Whole Class Lesson Settings
4. Concluding Discussion and Outlook
4.1. Role of the Knowledge Facets for Competent Acting and Transferability Between Domains
4.2. A Third Dimension: Links to Competence Development
4.3. Research Agenda
Author Contributions
Funding
Conflicts of Interest
References
- Blömeke, S.; Gustafsson, J.-E.; Shavelson, R.J. Beyond Dichotomies: Competence Viewed as a Continuum. Zeitschrift für Psychologie 2015, 223, 3–13. [Google Scholar] [CrossRef]
- Schmidmaier, R.; Eiber, S.; Ebersbach, R.; Schiller, M.; Hege, I.; Holzer, M.; Fischer, M.R. Learning the Facts in Medical School is not Enough: Which Factors Predict Successful Application of Procedural Knowledge in a Laboratory Setting? BMC Med. Educ. 2013, 13. [Google Scholar] [CrossRef] [PubMed]
- Kunter, M.; Klusmann, U.; Baumert, J.; Richter, D.; Voss, T.; Hachfeld, A. Professional Competence of Teachers: Effects on Instructional Quality and Student Development. J. Educ. Psychol. 2013, 105, 805–820. [Google Scholar] [CrossRef]
- Tepner, O.; Borowski, A.; Dollny, S.; Fischer, H.E.; Jüttner, M.; Kirschner, S.; Leutner, D.; Neuhaus, B.J.; Sandmann, A.; Sumfleth, E.; Thillmann, H.; Wirth, J. Modell zur Entwicklung von Testitems zur Erfassung des Professionswissens von Lehrkräften in den Naturwissenschaften. Zeitschrift für Didaktik der Naturwissenschaften 2012, 18, 7–28. [Google Scholar]
- Shulman, L.S. Knowledge and Teaching of the New Reform. Harv. Educ. Rev. 1987, 57, 1–22. [Google Scholar] [CrossRef]
- Helmke, A. Unterrichtsqualität und Lehrerprofessionalität. Diagnose, Evaluation und Verbesserung des Unterrichts; Klett: Seelze-Velber, Germany, 2014. [Google Scholar]
- Schmidt, H.G.; Rikers, R.M.J.P. How Expertise Develops in Medicine: Knowledge Encapsulation and Illness Script Formation. Med. Educ. 2007, 41, 1133–1139. [Google Scholar] [CrossRef] [PubMed]
- Alexander, P.A.; Schallert, D.L.; Hare, V.C. Coming to Terms: How Researchers in Learning and Literacy Talk about Knowledge. Rev. Educ. Res. 1991, 61, 315–343. [Google Scholar] [CrossRef]
- De jong, T.; Ferguson-Hessler, M.G.M. Types and Qualities of Knowledge. Educ. Psychol. 1996, 31, 105–113. [Google Scholar] [CrossRef]
- Shulman, L.S. Those Who Understand: Knowledge Growth in Teaching. Educ. Res. 1986, 15, 4–14. [Google Scholar] [CrossRef]
- Lin, F.-L.; Rowland, T. Pre-Service and In-Service Mathematics Teachers’ Knowledge and Professional Development. In The Second Handbook of Research on the Psychology of Mathematics Education; Gutiérrez, Á., Leder, G.C., Paolo, B., Eds.; Sense Publishers: Rotterdam, The Netherlands, 2016; pp. 483–520. [Google Scholar]
- Mayer, R.E. Applying the Science of Learning to Medical Education. Med. Educ. 2010, 44, 543–549. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.W.; Krathwohl, D.R. A Taxonomy for Learning, Teaching, and Assessing. A Revision of Bloom’s Taxonomy of Educational Objectives; Longman: New York, NY, USA, 2001. [Google Scholar]
- Kopp, V.; Stark, R.; Fischer, M.R. Fostering Diagnostic Knowledge through Computer-Supported, Case-Based Worked Examples: Effects of Erroneous Examples and Feedback. Med. Educ. 2008, 42, 823–829. [Google Scholar] [CrossRef] [PubMed]
- Van Gog, T.; Paas, F.; van Merriёnboer, J.J.G. Process-Oriented Worked Examples: Improving Transfer Performance through Enhanced Understanding. Instr. Sci. 2004, 32, 83–98. [Google Scholar] [CrossRef]
- Kopp, V.; Stark, R.; Kühne-Eversmann, L.; Fischer, M.R. Do Worked Examples Foster Medical Students’ Diagnostic Knowledge of Hyperthyroidism? Med. Educ. 2009, 43, 1210–1217. [Google Scholar] [CrossRef] [PubMed]
- Charlin, B.; Lubarsky, S.; Millette, B.; Crevier, F.; Audétat, M.-C.; Charbonneau, A.; CaireFon, N.; Hoff, L.; Bourdy, C. Clinical Reasoning Processes: Unravelling Complexity through Graphical Representation. Med. Educ. 2012, 46, 454–463. [Google Scholar] [CrossRef] [PubMed]
- Abell, S.K. Research on Science Teacher Knowledge. In Handbook of Research on Science Education; Abell, S.K., Lederman, N.G., Eds.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 2007; pp. 1105–1149. [Google Scholar]
- Abell, S.K. Twenty Years Later: Does Pedagogical Content Knowledge Remain a Useful Idea? Int. J. Sci. Educ. 2008, 30, 1405–1416. [Google Scholar] [CrossRef]
- Baumert, J.; Kunter, M. The COACTIV Model of Teachers’ Professional Competence. In Cognitive Activation in the Mathematics Classroom and Professional Competence of Teachers: Results from the COACTIV Project; Kunter, M., Baumert, J., Blum, W., Klusmann, U., Krauss, S., Neubrand, M., Eds.; Springer: New York, NY, USA, 2013; pp. 25–48. [Google Scholar]
- Blömeke, S.; Kaiser, G.; Lehmann, R. (Eds.) Professionelle Kompetenz angehender Lehrerinnen und Lehrer. Wissen, Überzeugungen und Lerngelegenheiten deutscher Mathematikstudierender und -referendare. Erste Ergebnisse zur Wirksamkeit der Lehrerausbildung; Waxmann: Münster, NY, USA, 2008. [Google Scholar]
- Fischer, H.E.; Borowski, A.; Tepner, O. Professional Knowledge of Science Teachers. In Second International Handbook of Science Education; Fraser, B.J., Tobin, K., McRobbie, C.J., Eds.; Springer: Berlin, Germany, 2012; pp. 435–448. [Google Scholar]
- Jüttner, M.; Boone, W.; Park, S.; Neuhaus, B.J. Development and Use of a Test Instrument to Measure Biology Teachers’ Content Knowledge (CK) and Pedagogical Content Knowledge (PCK). Educ. Assess. Eval. Account. 2013, 25, 45–67. [Google Scholar] [CrossRef]
- Depaepe, F.; Verschaffel, L.; Kelchtermans, G. Pedagogical Content Knowledge: A Systematic Review of the Way in Which The Concept has Pervaded Mathematics Educational Research. Teach. Teach. Educ. 2013, 34, 12–25. [Google Scholar] [CrossRef]
- Schmelzing, S.; van Driel, J.H.; Jüttner, M.; Brandenbusch, S.; Sandmann, A.; Neuhaus, B.J. Development, Evaluation, and Validation of a Paper-and-Pencil Test for Measuring Two Componentes of Biology Teachers’ Pedagogical Content Knowledge Concerning the “Cardiovascular System”. Int. J. Sci. Math. Educ. 2013, 11, 1369–1390. [Google Scholar] [CrossRef]
- Blömeke, S.; Kaiser, G.; Lehmann, R. (Eds.) TEDS-M 2008. Professionelle Kompetenz und Lerngelegenheiten angehender Mathematiklehrkräfte für die Sekundarstufe I im internationalen Vergleich; Waxmann: Münster, NY, USA, 2010. [Google Scholar]
- Harms, U.; Neumann, K. Aims and Models of Mathematics and Science Education. Available online: http://www.ipn.uni-kiel.de/de/forschung/forschungsberichte/FB_B1final2.pdf (accessed on 31 January 2015).
- Kunter, M.; Baumert, J.; Blum, W.; Klusmann, U.; Krauss, S.; Neubrand, M. (Eds.) Cognitive Activation in the Mathematics Classroom and Professional Competence of Teachers. Results from the COACTIV Project; Springer: New York, NY, USA, 2013. [Google Scholar]
- The Preparing Gap: Teacher Education for Middle School Mathematics in Six Countries (MT21 Report). Available online: https://www.educ.msu.edu/content/downloads/sites/usteds/MT21Report.pdf (accessed on 17 January 2018).
- Hill, H.C.; Rowan, B.; Ball, D.L. Effects of Teachers’ Mathematical Knowledge for Teaching on Student Achievement. Am. Educ. Res. J. 2005, 42, 371–406. [Google Scholar] [CrossRef]
- Kennedy, M.M. Education Reform and Subject Matter Knowledge. J. Res. Sci. Teach. 1998, 35, 249–263. [Google Scholar] [CrossRef]
- Hill, H.C.; Schilling, S.G.; Ball, D.L. Developing Measures of Teachers’ Mathematics Knowledge for Teaching. Elem. Sch. J. 2004, 105, 11–30. [Google Scholar] [CrossRef] [Green Version]
- Gess-Newsome, J. Pedagogical Content Knowledge: An Introduction and Orientation. In Examining Pedagogical Content Knowledge: The Construct and Its Implications for Science Education; Gess-Newsome, J., Lederman, N.G., Eds.; Kluwer Academic: Dordrecht, The Netherlands, 1999; pp. 3–17. [Google Scholar]
- Park, S.; Oliver, J.S. Revisiting the Conceptualisation of Pedagogical Content Knowledge (PCK): PCK as a Conceptual Tool to Understand Teachers as Professionals. Res. Sci. Educ. 2008, 38, 261–284. [Google Scholar] [CrossRef]
- König, J.; Seifert, A. (Eds.) Lehramtsstudierende erwerben pädagogisches Professionswissen; Waxmann: Münster, NY, USA, 2012. [Google Scholar]
- Lenske, G.; Thillmann, H.; Wirth, J.; Dicke, T.; Leutner, D. Pädagogisch-psychologisches Professionswissen von Lehrkräften: Evaluation des ProwiN-Tests. Zeitschrift für Erziehungswissenschaft 2015, 18, 225–245. [Google Scholar] [CrossRef]
- Voss, T.; Kunter, M. Teachers’ General Pedagogical/Psychological Knowledge. In Cognitive Activation in the Mathematics Classroom and Professional Competence of Teachers: Results from the COACTIV Project; Kunter, M., Baumert, J., Blum, W., Klusmann, U., Krauss, S., Neubrand, M., Eds.; Springer: New York, NY, USA, 2013; pp. 207–228. [Google Scholar]
- Lindmeier, A.M.; Heinze, A.; Reiss, K. Eine Machbarkeitsstudie zur Operationalisierung aktionsbezogener Kompetenz von Mathematiklehrkräften mit videobasierten Maßen. Journal für Mathematik-Didaktik 2013, 34, 99–119. [Google Scholar] [CrossRef]
- Lefstein, A.; Snell, J. Professional Vision and the Politics of Teacher Learning. Teach. Teach. Educ. 2011, 27, 505–514. [Google Scholar] [CrossRef]
- Seidel, T.; Blomberg, G.; Stürmer, K. “Observer”—Validierung eines videobasierten Instruments zur Erfassung der professionellen Wahrnehmung von Unterricht. Zeitschrift für Pädagogik 2010, 56, 296–306. [Google Scholar]
- Stürmer, K.; Seidel, T.; Schäfer, S. Changes in Professional Vision in the Context of Practice: Preservice Teachers’ Professional Vision Changes Following Practical Experience: A Video-Based Approach in University-Based Teacher Education. Gruppendynamik und Organisationsberatung 2013, 44, 339–355. [Google Scholar] [CrossRef]
- Krauss, S.; Blum, W.; Brunner, M.; Neubrand, M.; Baumert, J.; Kunter, M.; Besser, M.; Elsner, J. Mathematics Teachers’ Domain-Specific Professional Knowledge: Conceptualization and Test Construction in COACTIV. In Cognitive Activation in the Mathematics Classroom and Professional Competence of Teachers: Results from the COACTIV Project; Kunter, M., Baumert, J., Blum, W., Klusmann, U., Krauss, S., Neubrand, M., Eds.; Springer: New York, NY, USA, 2013; pp. 147–174. [Google Scholar]
- Polanyi, M. Implizites Wissen; Suhrkamp: Frankfurt am Main, Germany, 1985. [Google Scholar]
- Blömeke, S.; Suhl, U.; Kaiser, G. Teacher Education Effectiveness: Quality and Equity of Future Primary Teachers’ Mathematics and Mathematics Pedagogical Content Knowledge. J. Teach. Educ. 2011, 62, 154–171. [Google Scholar] [CrossRef]
- König, J.; Blömeke, S.; Paine, L.; Schmidt, W.H.; Hsieh, F.-J. General Pedagogical Knowledge of Future Middle School Teachers: On the Complex Ecology of Teacher Education in the United States, Germany, and Taiwan. J. Teach. Educ. 2011, 62, 188–201. [Google Scholar] [CrossRef]
- Anderson, J.R. Acquisition of Cognitive Skill. Psychol. Rev. 1982, 89, 369–406. [Google Scholar] [CrossRef]
- Paris, S.G.; Lipson, M.Y.; Wixson, K.K. Becoming a Strategic Reader. Contemp. Educ. Psychol. 1983, 8, 293–316. [Google Scholar] [CrossRef]
- Großschedl, J.; Harms, U.; Kleickmann, T.; Glowinski, I. Preservice Biology Teachers’ Professional Knowledge: Structure and Learning Opportunities. J. Sci. Teach. Educ. 2015, 26, 291–318. [Google Scholar] [CrossRef]
- Dreher, A.; Lindmeier, A.; Heinze, A.; Niemand, C. What Kind of Content Knowledge do Secondary Mathematics Teachers Need? Journal für Mathematik-Didaktik 2018, 37, 131. [Google Scholar] [CrossRef]
- Heinze, A.; Dreher, A.; Lindmeier, A.; Niemand, C. Akademisches versus schulbezogenes Fachwissen—Ein differenzierteres Modell des fachspezifischen Professionswissens von angehenden Mathematiklehrkräften der Sekundarstufe. Zeitschrift für Erziehungswissenschaft 2016, 19, 329–349. [Google Scholar] [CrossRef]
- Krathwohl, D.R. A Revision of Bloom‘s Taxonomy: An Overview. Theor. Pract. 2002, 41, 212–218. [Google Scholar] [CrossRef]
- Hargreaves, D.H. The Production, Mediation and Use of Professional Knowledge among Teachers and Doctors: A Comparative Analysis. In Knowledge Management in the Learning Society; OECD Publishing: Paris, French, 2000; pp. 219–238. [Google Scholar]
- Wölfel, T.; Beltermann, E.; Lottspeich, C.; Vietz, E.; Fischer, M.R.; Schmidmaier, R. Medical Ward Round Competence in Internal Medicine—An Interview Study towards an Interprofessional Development of an Entrustable Professional Activity (EPA). BMC Med. Educ. 2016, 16. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.R. Skill Acquisition: Compilation of Weak-Method Problem Solutions. Psychol. Rev. 1987, 94, 192–210. [Google Scholar] [CrossRef]
- Helmke, A.; Lenske, G. Unterrichtsdiagnostik als Voraussetzung für Unterrichtsentwicklung. Beiträge zur Lehrerbildung 2013, 31, 214–233. [Google Scholar]
- Anderson, J.R.; Lebiere, C. (Eds.) The Atomic Components of Thought; Erlbaum: Mahwah, NJ, USA, 1998. [Google Scholar]
- VanLehn, K. Cognitive Skill Acquisition. Annu. Rev. Psychol. 1996, 47, 513–539. [Google Scholar] [CrossRef] [PubMed]
- Jüttner, M.; Neuhaus, B.J. Das Professionswissen von Biologielehrkräften: Ein Vergleich zwischen Biologielehrkräften, Biologen und Pädagogen. Zeitschriftfür Didaktik der Naturwissenschaften 2013, 19, 31–49. [Google Scholar]
- Krauss, S.; Baumert, J.; Blum, W. Secondary Mathematics Teachers’ Pedagogical Content Knowledge and Content Knowledge: Validation of the COACTIV Constructs. ZDM Math. Educ. 2008, 40, 873–892. [Google Scholar] [CrossRef]
- Kleickmann, T.; Tröbst, S.; Heinze, A.; Bernholt, A.; Rink, R.; Kunter, M. Teacher Knowledge Experiment: Conditions of the Development of Pedagogical Content Knowledge. In Competence Assessment in Education: Research Models and Instruments; Leutner, D., Fleischer, J., Grünkorn, J., Klieme, E., Eds.; Springer: Cham, Switzerland, 2017; pp. 111–129. [Google Scholar]
- Baumert, J.; Kunter, M. The Effect of Content Knowledge and Pedagogical Content Knowledge on Instructional Quality and Student Achievement. In Cognitive Activation in the Mathematics Classroom and Professional Competence of Teachers: Results from the COACTIV Project; Kunter, M., Baumert, J., Blum, W., Klusmann, U., Krauss, S., Neubrand, M., Eds.; Springer: New York, NY, USA, 2013; pp. 175–206. [Google Scholar]
- Förtsch, C.; Werner, S.; von Kotzebue, L.; Neuhaus, B. Effects of Biology Teachers’ Professional Knowledge and Cognitive Activation on Students’ Achievement. Int. J. Sci. Educ. 2016, 38, 2642–2666. [Google Scholar] [CrossRef]
- Lenske, G.; Wagner, W.; Wirth, J.; Thillmann, H.; Cauet, E.; Liepertz, S.; Leutner, D. Die Bedeutung des pädagogisch-psychologischen Wissens für die Qualität der Klassenführung und den Lernzuwachs der Schüler/innen im Physikunterricht. Zeitschrift für Erziehungswissenschaft 2016, 19, 211–233. [Google Scholar] [CrossRef]
- Kahan, J.A.; Cooper, D.A.; Bethea, K.A. The Role of Mathematics Teachers’ Content Knowledge in their Teaching: A Framework for Research Applied to a Study of Student Teachers. J. Math. Teach. Educ. 2003, 6, 223–252. [Google Scholar] [CrossRef]
- Dicke, T.; Holzberger, D.; Kunina-Habenicht, O.; Linninger, C.; Schulze-Stocker, F. “Doppelter Praxisschock” auf dem Weg ins Lehramt? Verlauf und potenzielle Einflussfaktoren emotionaler Erschöpfung während des Vorbereitungsdienstes und nach dem Berufseintritt. Psychologie in Erziehung und Unterricht 2016, 63, 244. [Google Scholar] [CrossRef]
- Holzberger, D.; Philipp, A.; Kunter, M. How Teachers’ Self-Efficacy is related to Instructional Quality: A Longitudinal Analysis. J. Educ. Psychol. 2013, 105, 774–786. [Google Scholar] [CrossRef]
- Holzberger, D.; Philipp, A.; Kunter, M. Predicting Teachers’ Instructional Behaviors: The Interplay between Self-Efficacy and Intrinsic Needs. Contemp. Educ. Psychol. 2014, 39, 100–111. [Google Scholar] [CrossRef]
- Koehler, M.J.; Mishra, P. What is Technological Pedagogical Content Knowledge. Contemp. Issues Technol. Teach. Educ. 2009, 9, 60–70. [Google Scholar] [CrossRef]
- Epstein, R.M.; Hundert, E.M. Defining and Assessing Professional Competence. JAMA 2002, 287, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Klieme, E.; Leutner, D. Kompetenzmodelle zur Erfassung individueller Lernergebnisse und zur Bilanzierung von Bildungsprozessen: Beschreibung eines neu eingerichteten Schwerpunktprogramms der DFG. Zeitschrift für Pädagogik 2006, 52, 876–903. [Google Scholar]
- Koeppen, K.; Hartig, J.; Klieme, E.; Leutner, D. Current Issues in Competence Modeling and Assessment. Zeitschrift für Psychologie 2008, 216, 61–73. [Google Scholar] [CrossRef]
- Weinert, F.E. Concept of competence: A Conceptual Clarification. In Defining and Selecting Key Competencies; Rychen, D.S., Salganik, L.H., Eds.; Hogrefe and Huber: Seattle, WA, USA, 2001; pp. 45–65. [Google Scholar]
- Südkamp, A.; Praetorius, A.-K. (Eds.) Diagnostische Kompetenz von Lehrkräften; Waxmann: Münster, NY, USA, 2017. [Google Scholar]
- Boshuizen, H.P.A.; van de Wiel, M.W.J.; Schmidt, H.G. What and How Advanced Medical Students Learn from Reasoning through Multiple Cases. Instr. Sci. 2012, 40, 755–768. [Google Scholar] [CrossRef]
- Custers, E.J.F.M.; Boshuizen, H.P.A.; Schmidt, H.G. The role of Illness Scripts in the Development of Medical Diagnostic Expertise: Results from an Interview Study. Cognit. Instruct. 1998, 16, 367–398. [Google Scholar] [CrossRef] [Green Version]
- Schank, R.C. Dynamic Memory Revisited; Cambridge Univ. Press: Cambridge, UK, 1999. [Google Scholar]
- Kollar, I.; Fischer, F.; Hesse, F.W. Collaboration Scripts—A Conceptual Analysis. Educ. Psychol. Rev. 2006, 18, 159–185. [Google Scholar] [CrossRef] [Green Version]
- Kolodner, J.L. (Ed.) Case-Based Learning; Springer: Boston, MA, USA, 1993. [Google Scholar]
- Rumelhart, D.E.; Ortony, A. The Representation of Knowledge in Memory. In Schooling and the Acquisition of Knowledge; Anderson, R.C., Spiro, R.J., Montague, W.E., Eds.; Erlbaum: Hillsdale, NJ, USA, 1977; pp. 99–135. [Google Scholar]



{kind=link}
{kind=link}
| Content-Related Facets of Knowledge | ||||
|---|---|---|---|---|
| Types of knowledge | CK | PCK | PK | |
| knowing when and why | Knowing, when and why subject-specific actions are executed. (KW-CK) | Knowing, when and why subject-specific instructional strategies are executed and knowing, when and why students’ errors within a certain topic are dealt with (KW-PCK) | Knowing, when and why subject-independent instructional strategies and the diagnostic process are executed (KW-PK) | |
| knowing how | Knowing, how subject-specific actions are executed (KH-CK) | Knowing, how subject-specific instructional strategies are executed and knowing, how students’ errors within a certain topic are dealt with (KH-PCK) | Knowing, how subject-independent instructional strategies and the diagnostic process are executed (KH-PK) | |
| knowing that | Knowledge about subject-specific terms, concepts, facts, and principles (KT-CK) | Knowledge about subject-specific instructional strategies and students’ errors within a certain topic (KT-PCK) | Knowledge about subject-independent instructional strategies and the diagnostic process (KT-PK) | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Förtsch, C.; Sommerhoff, D.; Fischer, F.; Fischer, M.R.; Girwidz, R.; Obersteiner, A.; Reiss, K.; Stürmer, K.; Siebeck, M.; Schmidmaier, R.; et al. Systematizing Professional Knowledge of Medical Doctors and Teachers: Development of an Interdisciplinary Framework in the Context of Diagnostic Competences. Educ. Sci. 2018, 8, 207. https://doi.org/10.3390/educsci8040207
Förtsch C, Sommerhoff D, Fischer F, Fischer MR, Girwidz R, Obersteiner A, Reiss K, Stürmer K, Siebeck M, Schmidmaier R, et al. Systematizing Professional Knowledge of Medical Doctors and Teachers: Development of an Interdisciplinary Framework in the Context of Diagnostic Competences. Education Sciences. 2018; 8(4):207. https://doi.org/10.3390/educsci8040207
Chicago/Turabian StyleFörtsch, Christian, Daniel Sommerhoff, Frank Fischer, Martin R. Fischer, Raimund Girwidz, Andreas Obersteiner, Kristina Reiss, Kathleen Stürmer, Matthias Siebeck, Ralf Schmidmaier, and et al. 2018. "Systematizing Professional Knowledge of Medical Doctors and Teachers: Development of an Interdisciplinary Framework in the Context of Diagnostic Competences" Education Sciences 8, no. 4: 207. https://doi.org/10.3390/educsci8040207