
Home-Based Intermittent Pneumatic Compression Therapy: The Impact in Chronic Leg Lymphedema in Patients Treated for Gynecologic Cancer

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Intervention
2.4. Outcome Measures
2.4.1. Inter-Limb Volume Difference Ratio
2.4.2. Quality of Life
2.4.3. Participant Satisfaction
2.5. Statistical Analysis
3. Results
3.1. General Characteristics
3.2. Time-Dependent Changes in Inter-Limb Volume Difference Ratio
3.3. Time-Dependent Changes in the Inter-Limb Volume Difference Ratio between the Subgroups
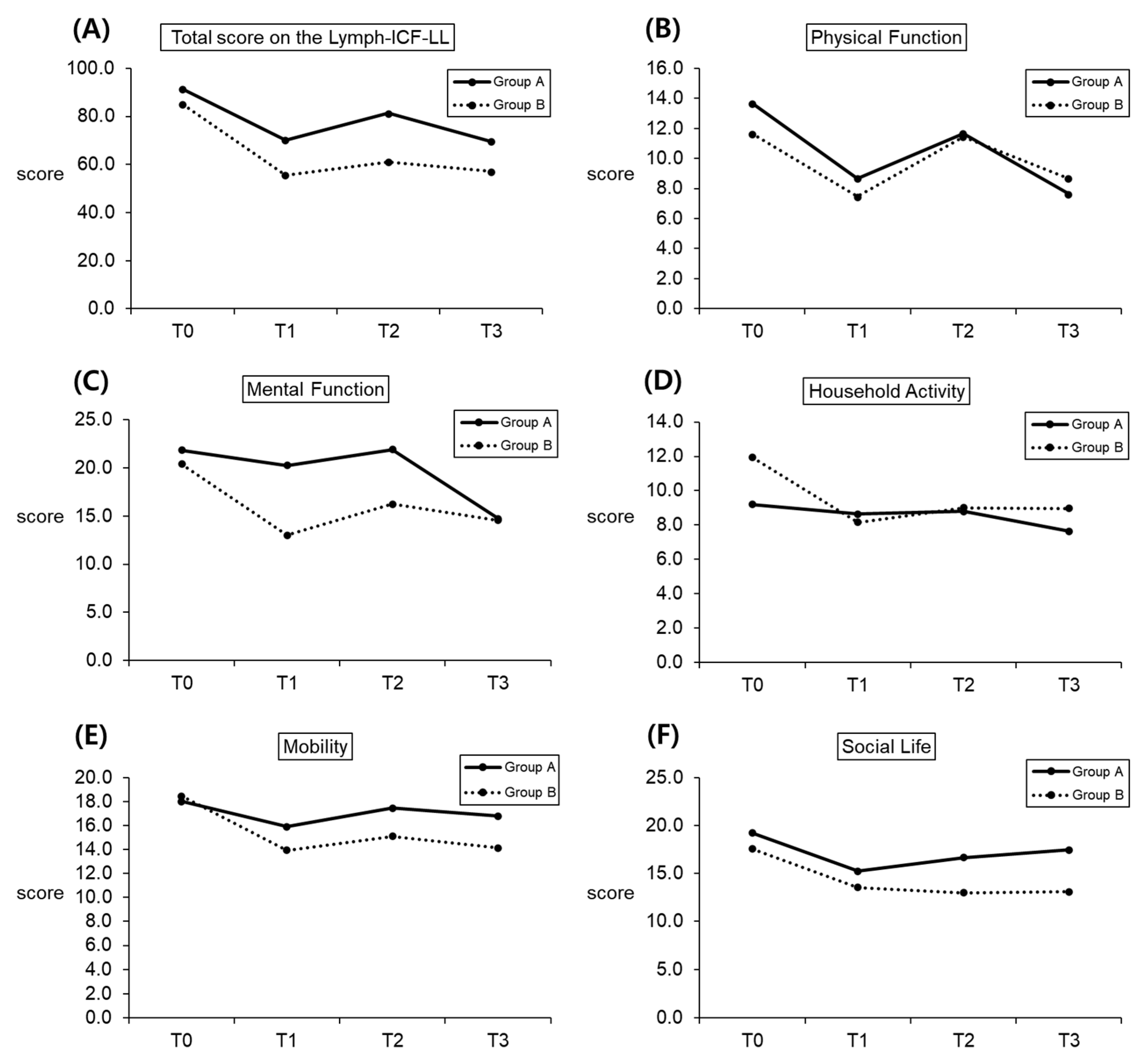
3.4. Time-Dependent Changes in the ICF Domain Scores
3.5. Time-Dependent Changes in the ICF Domain Scores between the Subgroups
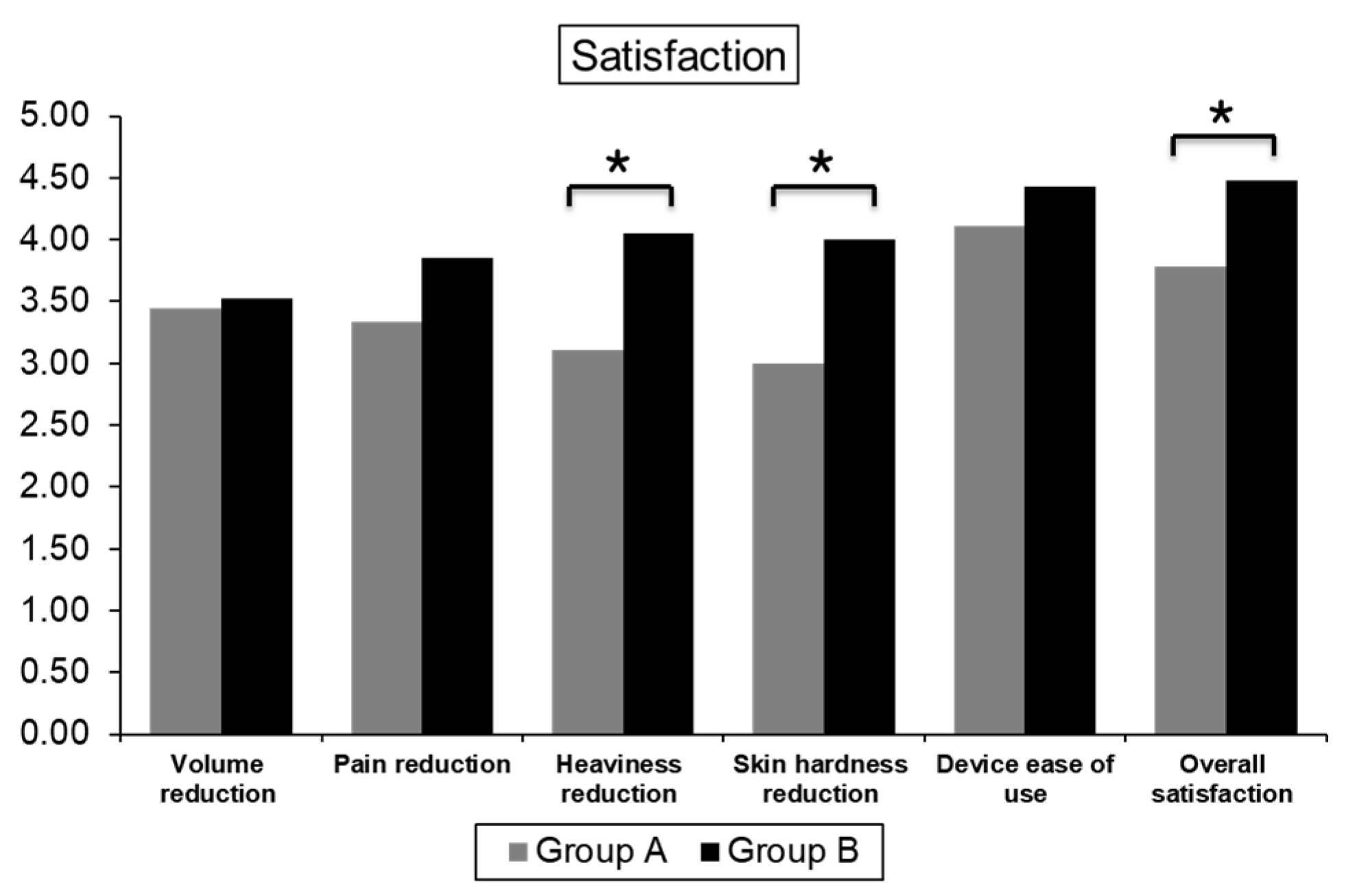
3.6. Satisfaction Scores
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zaleska, M.; Olszewski, W.L.; Durlik, M. The effectiveness of intermittent pneumatic compression in long-term therapy of lymphedema of lower limbs. Lymphat. Res. Biol. 2014, 12, 103–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanton, A.W.; Modi, S.; Mellor, R.H.; Levick, J.R.; Mortimer, P.S. Recent advances in breast cancer-related lymphedema of the arm: Lymphatic pump failure and predisposing factors. Lymphat. Res. Biol. 2009, 7, 29–45. [Google Scholar] [CrossRef] [PubMed]
- Kerchner, K.; Fleischer, A.; Yosipovitch, G. Lower extremity lymphedema update: Pathophysiology, diagnosis, and treatment guidelines. J. Am. Acad. Dermatol. 2008, 59, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Szuba, A.; Achalu, R.; Rockson, S.G. Decongestive lymphatic therapy for patients with breast carcinoma-associated lymphedema. A randomized, prospective study of a role for adjunctive intermittent pneumatic compression. Cancer 2002, 95, 2260–2267. [Google Scholar] [CrossRef] [PubMed]
- Aschen, S.; Zampell, J.C.; Elhadad, S.; Weitman, E.; De Brot, M.; Mehrara, B.J. Regulation of adipogenesis by lymphatic fluid stasis: Part II. Expression of adipose differentiation genes. Plast. Reconstr. Surg. 2012, 129, 838–847. [Google Scholar] [CrossRef]
- Fialka-Moser, V.; Korpan, M.; Varela, E.; Ward, A.; Gutenbrunner, C.; Casillas, J.M.; Delarque, A.; Berteanu, M.; Christodoulou, N. The role of physical and rehabilitation medicine specialist in lymphoedema. Ann. Phys. Rehabil. Med. 2013, 56, 396–410. [Google Scholar] [CrossRef] [Green Version]
- Pedrosa, B.C.S.; Maia, J.N.; Ferreira, A.P.L.; de Araujo, M.; Montenegro, E.J.N.; da Silva, F.L.; de Castro, C.; Andrade, M.D.A. Functionality and quality of life of patients with unilateral lymphedema of a lower limb: A cross-sectional study. J. Vasc. Bras. 2019, 18, e20180066. [Google Scholar] [CrossRef] [Green Version]
- Javid, S.H.; Anderson, B.O. Mounting evidence against complex decongestive therapy as a first-line treatment for early lymphedema. J. Clin. Oncol. 2013, 31, 3737–3738. [Google Scholar] [CrossRef]
- Chang, D.W.; Masia, J.; Garza, R., 3rd; Skoracki, R.; Neligan, P.C. Lymphedema: Surgical and Medical Therapy. Plast. Reconstr. Surg. 2016, 138, 209s–218s. [Google Scholar] [CrossRef]
- Rockson, S.G.; Miller, L.T.; Senie, R.; Brennan, M.J.; Casley-Smith, J.R.; Foldi, E.; Foldi, M.; Gamble, G.L.; Kasseroller, R.G.; Leduc, A.; et al. American Cancer Society Lymphedema Workshop. Workgroup III: Diagnosis and management of lymphedema. Cancer 1998, 83, 2882–2885. [Google Scholar] [CrossRef]
- Kim, Y.B.; Hwang, J.H.; Kim, T.W.; Chang, H.J.; Lee, S.G. Would complex decongestive therapy reveal long term effect and lymphoscintigraphy predict the outcome of lower-limb lymphedema related to gynecologic cancer treatment? Gynecol. Oncol. 2012, 127, 638–642. [Google Scholar] [CrossRef] [PubMed]
- Korpan, M.I.; Crevenna, R.; Fialka-Moser, V. Lymphedema: A therapeutic approach in the treatment and rehabilitation of cancer patients. Am. J. Phys. Med. Rehabil. 2011, 90, S69–S75. [Google Scholar] [CrossRef] [PubMed]
- Badger, C.M.; Peacock, J.L.; Mortimer, P.S. A randomized, controlled, parallel-group clinical trial comparing multilayer bandaging followed by hosiery versus hosiery alone in the treatment of patients with lymphedema of the limb. Cancer 2000, 88, 2832–2837. [Google Scholar] [CrossRef]
- The diagnosis and treatment of peripheral lymphedema: 2020 Consensus Document of the International Society of Lymphology. Lymphology 2020, 53, 3–19. Available online: https://journals.librarypublishing.arizona.edu/lymph/article/id/4649/ (accessed on 23 July 2021).
- Brush, B.E.; Heldt, T.J. A device for relief of lymphedema. J. Am. Med. Assoc. 1955, 158, 34–35. [Google Scholar] [CrossRef] [PubMed]
- Baulieu, F.; Baulieu, J.L.; Vaillant, L.; Secchi, V.; Barsotti, J. Factorial analysis in radionuclide lymphography: Assessment of the effects of sequential pneumatic compression. Lymphology 1989, 22, 178–185. [Google Scholar] [PubMed]
- Hye, H.J.; Uk, K.T.; Woo, L.K.; Ik, K.D.; Boong, L.B. Sequential Intermittent Pneumatic Compression Therapy in Lymphedema. J. Korean Acad. Rehabil. Med. 1997, 21, 146–153. [Google Scholar]
- Dunn, N.; Williams, E.M.; Fishbourne, M.; Dolan, G.; Davies, J.H. Home management of lower limb lymphoedema with an intermittent pneumatic compression device: A feasibility study. Pilot Feasibility Study 2019, 5, 113. [Google Scholar] [CrossRef]
- Committee, E. The diagnosis and treatment of peripheral lymphedema: 2016 consensus document of the International Society of Lymphology. Lymphology 2016, 49, 170–184. Available online: https://journals.librarypublishing.arizona.edu/lymph/article/id/3838/ (accessed on 10 November 2018).
- Stanton, A.W.; Northfield, J.W.; Holroyd, B.; Mortimer, P.S.; Levick, J.R. Validation of an optoelectronic limb volumeter (Perometer). Lymphology 1997, 30, 77–97. [Google Scholar]
- Engelberger, R.P.; Blazek, C.; Amsler, F.; Keo, H.H.; Baumann, F.; Blättler, W.; Baumgartner, I.; Willenberg, T. Reproducibility and day time bias correction of optoelectronic leg volumetry: A prospective cohort study. BMC Med. Res. Methodol. 2011, 11, 138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devoogdt, N.; De Groef, A.; Hendrickx, A.; Damstra, R.; Christiaansen, A.; Geraerts, I.; Vervloesem, N.; Vergote, I.; Van Kampen, M. Lymphoedema Functioning, Disability and Health Questionnaire for Lower Limb Lymphoedema (Lymph-ICF-LL): Reliability and validity. Phys. Ther. 2014, 94, 705–721. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization; Regional Office for the Western Pacific. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; Health Communications Australia: Sydney, Australia, 2000. [Google Scholar]
- Brown, J.C.; Lin, L.L.; Segal, S.; Chu, C.S.; Haggerty, A.E.; Ko, E.M.; Schmitz, K.H. Physical activity, daily walking, and lower limb lymphedema associate with physical function among uterine cancer survivors. Support. Care Cancer 2014, 22, 3017–3025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fu, M.R.; Ridner, S.H.; Hu, S.H.; Stewart, B.R.; Cormier, J.N.; Armer, J.M. Psychosocial impact of lymphedema: A systematic review of literature from 2004 to 2011. Psychooncology 2013, 22, 1466–1484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ridner, S.H.; Dietrich, M.S.; Deng, J.; Ettema, S.L.; Murphy, B. Advanced pneumatic compression for treatment of lymphedema of the head and neck: A randomized wait-list controlled trial. Support. Care Cancer 2021, 29, 795–803. [Google Scholar] [CrossRef]
- Brayton, K.M.; Hirsch, A.T.; PJ, O.B.; Cheville, A.; Karaca-Mandic, P.; Rockson, S.G. Lymphedema prevalence and treatment benefits in cancer: Impact of a therapeutic intervention on health outcomes and costs. PLoS ONE 2014, 9, e114597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desai, S.S.; Shao, M. Superior Clinical, Quality of Life, Functional, and Health Economic Outcomes with Pneumatic Compression Therapy for Lymphedema. Ann. Vasc. Surg. 2020, 63, 298–306. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Parameters | Participants (n = 30) | Group A (n = 9) | Group B (n = 21) | p-Value | |
|---|---|---|---|---|---|
| Sex (female (%)) | 0/30 (100%) | 0/9 (100%) | 0/21 (100%) | ||
| Age (years, mean ± SD) | 56.47 ± 11.33 | 62.22 ± 6.02 | 54.00 ± 12.27 | 0.068 | |
| Height (cm, mean ± SD) | 159.95 ± 5.97 | 157.89 ± 6.19 | 160.83 ± 5.79 | 0.244 | |
| Initial BMI (kg/m2, mean ± SD) | 23.87 ± 3.33 | 24.39 ± 2.67 | 23.80 ± 3.02 | 0.158 | |
| Onset of lymphedema after surgery (years, mean ± SD) | 3.18 ± 2.58 | 3.23 ± 2.04 | 3.16 ± 3.21 | 0.782 | |
| Mean duration of lymphedema (years, mean ± SD) | 15.46 ± 7.57 | 14.42 ± 7.92 | 15.91 ± 5.84 | 0.323 | |
| Affected side, N (%) | Right | 17 (56.7) | 4 (44.4) | 13 (61.9) | 0.376 |
| Left | 13 (43.3) | 5 (55.6) | 8 (38.1) | ||
| Chemotherapy, N (%) | 11 (36.7) | 3 (33.3) | 8 (38.1) | 0.804 | |
| Radiotherapy, N (%) | 11 (36.7) | 5 (55.6) | 6 (28.6) | 0.160 | |
| Cancer type, N (%) | |||||
| Ovarian cancer | 6 (20.0) | 2 (22.2) | 4 (19.0) | 0.842 | |
| Cervical cancer | 16 (53.3) | 4 (44.4) | 12 (57.1) | 0.523 | |
| Fallopian tube | 2 (6.7) | 0 (0) | 2 (9.5) | 0.338 | |
| Endometrial cancer | 6 (20.0) | 3 (33.3) | 3 (14.3) | 0.232 | |
| Outcome | T0 (n = 30) | T1 (n = 30) | T2 (n = 30) | T3 (n = 30) | χ2 (df) | p-Value |
|---|---|---|---|---|---|---|
| Mean (SD) | ||||||
| Distal limb volume difference ratio | 22.21 (17.67) | 22.07 (17.42) | 21.97 (18.07) | 23.19 (17.92) | 2.40 (3) | 0.494 |
| Proximal limb volume difference ratio | 23.86 (11.27) | 23.41 (11.49) | 23.63 (12.05) | 25.67 (13.43) | 6.85 (3) | 0.077 |
| Whole limb volume difference ratio | 23.15 (12.92) | 22.83 (12.77) | 23.03 (13.09) | 24.65 (13.98) | 4.92 (3) | 0.178 |
| Outcome | Group A (n = 9) | Group B (n = 21) | Mean Difference (95% CI) | p-Value | |||
|---|---|---|---|---|---|---|---|
| Mean (SD) | |||||||
| Distal limb volume difference ratio | |||||||
| △T0–T1 | −2.60 | (4.21) | 5.60 | (5.28) | −8.20 | (−11.90, −4.49) | <0.001 * |
| △T1–T2 | 1.37 | (3.76) | −3.54 | (5.42) | 4.91 | (1.40, 8.42) | 0.008 * |
| △T2–T3 | 0.75 | (4.23) | 2.32 | (7.86) | −1.57 | (−7.76, 4.61) | 0.584 |
| Proximal limb volume difference ratio | |||||||
| △T0–T1 | −1.91 | (3.87) | 2.97 | (4.53) | −4.88 | (−8.20, −1.56) | 0.006 * |
| △T1–T2 | 0.79 | (2.61) | −1.12 | (4.55) | 1.90 | (−0.78, 4.58) | 0.157 |
| △T2–T3 | 1.37 | (5.09) | 3.62 | (5.94) | −2.26 | (−6.62, 2.11) | 0.299 |
| Whole limb volume difference ratio | |||||||
| △T0–T1 | −2.22 | (2.96) | 4.10 | (4.01) | −6.33 | (−9.02, −3.64) | 0.000 * |
| △T1–T2 | 1.20 | (2.47) | −2.13 | (4.52) | 3.33 | (0.73, 5.94) | 0.014 |
| △T2–T3 | 0.97 | (2.47) | 3.17 | (6.55) | −2.20 | (−6.23, 1.82) | 0.272 |
| ICF Domain | RMANOVA (or Friedman Test) | Pairwise Comparisons (or Wilcoxon Signed-Rank Test) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) | |||||||||||
| T0 | T1 | T2 | T3 | p Value | T0 vs. T1 | T0 vs. T2 | T0 vs. T3 | T1 vs. T2 | T1 vs. T3 | T2 vs. T3 | |
| Total score | 92.57 (37.34) | 57.90 (29.33) | 65.49 (31.45) | 61.07 (34.20) | <0.001 * | <0.001 * | <0.001 * | <0.001 * | 0.048 * | 0.426 | 0.225 |
| Physical function | 12.03 (7.71) | 6.33 (5.47) | 9.33 (7.77) | 8.67 (8.33) | 0.013 | 0.001 * | 0.164 | 0.040 * | 0.009 * | 0.141 | 0.638 |
| Mental function | 28.27 (16.19) | 16.70 (16.14) | 18.73 (14.15) | 16.80 (14.30) | <0.001 * | <0.001 * | 0.004 * | <0.001 * | 0.204 | 0.809 | 0.313 |
| Household activity | 10.10 (7.12) | 5.27 (3.90) | 5.63 (4.08) | 5.47 (4.84) | 0.005 * | 0.001 * | 0.003 * | 0.001 * | 0.319 | 0.508 | 0.863 |
| Mobility | 22.90 (13.04) | 15.37 (9.56) | 17.17 (10.42) | 15.63 (9.61) | 0.001 * | 0.004 * | 0.008 * | 0.002 * | 0.262 | 0.866 | 0.226 |
| Social life | 19.27 (6.75) | 13.93 (7.20) | 14.63 (7.35) | 14.50 (8.79) | 0.003 * | 0.005 * | 0.004 * | 0.014 * | 0.436 | 0.569 | 0.906 |
| Outcome | Group A (n = 9) | Group B (n = 21) | p-Value | ||
|---|---|---|---|---|---|
| Mean (SD) | |||||
| Quality of life | |||||
| Total ICF score | |||||
| △T0–T1 | 21.22 | (32.90) | 40.43 | (42.59) | 0.239 |
| △T1–T2 | −11.22 | (23.76) | −5.86 | (18.22) | 0.505 |
| △T2–T3 | 11.67 | (24.25) | 0.95 | (14.85) | 0.245 |
| Physical function | |||||
| △T0–T1 | 5.00 | (8.32) | 5.57 | (7.12) | 0.849 |
| △T1–T2 | −3.00 | (5.00) | −2.57 | (4.91) | 0.829 |
| △T2–T3 | 2.33 | (7.70) | −0.05 | (6.02) | 0.369 |
| Mental function | |||||
| △T0–T1 | 4.33 | (13.67) | 14.67 | (15.14) | 0.135 |
| △T1–T2 | −5.00 | (9.11) | −0.76 | (12.54) | 0.319 |
| △T2–T3 | 9.89 | (11.17) | −1.48 | (10.27) | 0.014 |
| Household activity | |||||
| △T0–T1 | 3.11 | (5.11) | 5.57 | (7.71) | 0.468 |
| △T1–T2 | −0.22 | (5.47) | −0.43 | (2.42) | 0.475 |
| △T2–T3 | −0.44 | (5.92) | 0.43 | (3.96) | 0.964 |
| Mobility | |||||
| △T0–T1 | 4.78 | (7.71) | 8.71 | (14.96) | 0.541 |
| △T1–T2 | −1.56 | (10.51) | −1.90 | (7.96) | 0.633 |
| △T2–T3 | 0.67 | (6.08) | 1.90 | (7.18) | 0.510 |
| Social life | |||||
| △T0–T1 | 4.00 | (9.72) | 5.90 | (9.57) | 0.587 |
| △T1–T2 | −1.44 | (4.13) | −0.19 | (3.88) | 0.663 |
| △T2–T3 | −0.78 | (6.96) | 0.14 | (5.87) | 0.453 |
| Satisfaction | |||||
| Overall satisfaction | 3.78 | (0.83) | 4.48 | (0.68) | 0.031 * |
| Volume reduction | 3.44 | (0.88) | 3.53 | (1.17) | 0.760 |
| Pain reduction | 3.33 | (0.71) | 3.86 | (1.01) | 0.162 |
| Heaviness reduction | 3.11 | (0.78) | 4.05 | (0.86) | 0.012 * |
| Skin hardness reduction | 3.00 | (0.87) | 4.00 | (0.77) | 0.007 * |
| Device ease of use | 4.11 | (1.05) | 4.43 | (0.68) | 0.516 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.; Kim, S.; Lim, J.Y.; Hwang, C.M.; Ko, M.-H.; Hwang, J.H. Home-Based Intermittent Pneumatic Compression Therapy: The Impact in Chronic Leg Lymphedema in Patients Treated for Gynecologic Cancer. Healthcare 2022, 10, 638. https://doi.org/10.3390/healthcare10040638
Kim Y, Kim S, Lim JY, Hwang CM, Ko M-H, Hwang JH. Home-Based Intermittent Pneumatic Compression Therapy: The Impact in Chronic Leg Lymphedema in Patients Treated for Gynecologic Cancer. Healthcare. 2022; 10(4):638. https://doi.org/10.3390/healthcare10040638
Chicago/Turabian StyleKim, Yoon, Seonghee Kim, Ji Young Lim, Chea Min Hwang, Myoung-Hwan Ko, and Ji Hye Hwang. 2022. "Home-Based Intermittent Pneumatic Compression Therapy: The Impact in Chronic Leg Lymphedema in Patients Treated for Gynecologic Cancer" Healthcare 10, no. 4: 638. https://doi.org/10.3390/healthcare10040638