
The Effects of Neurodevelopmental Treatment-Based Trunk Control Exercise on Gross Motor Function and Trunk Control in Children with Developmental Disabilities

Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Intervention
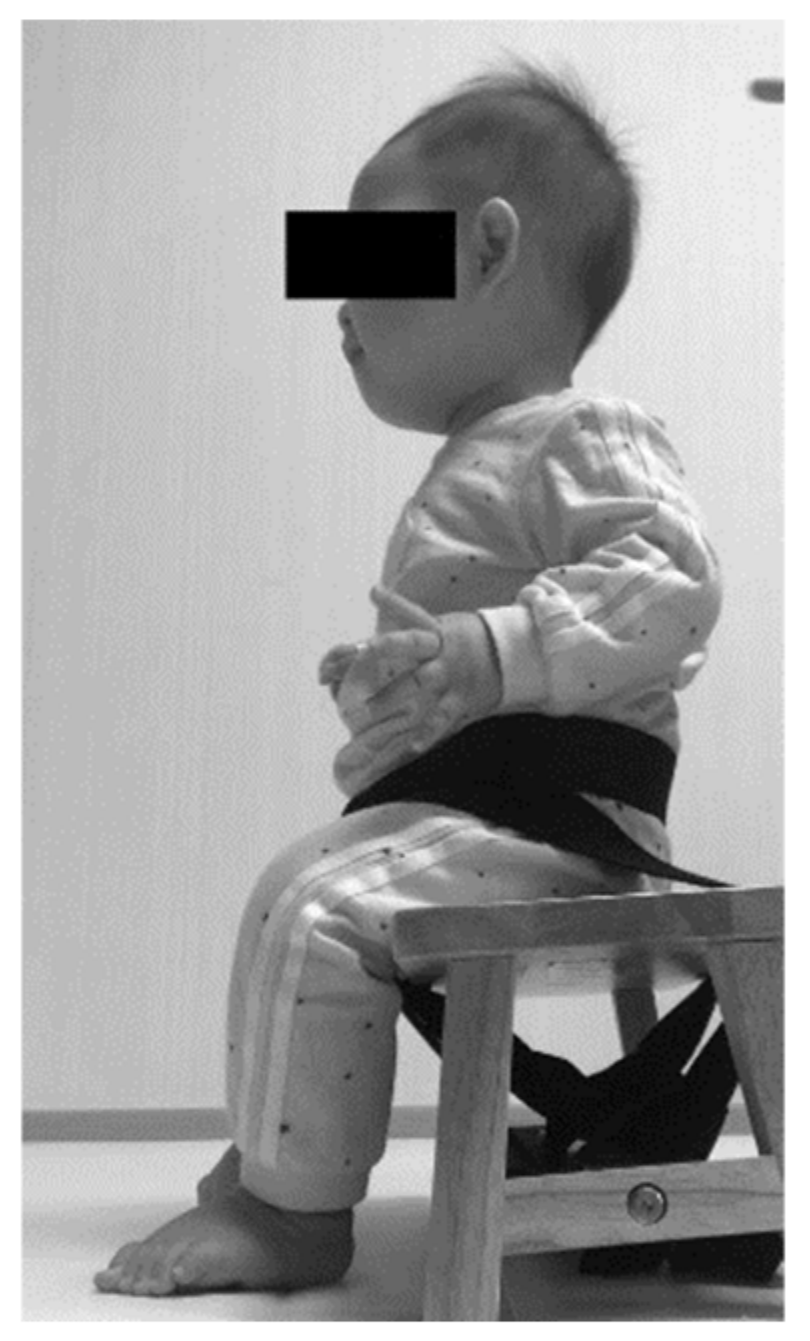
2.3.1. Neurodevelopmental Treatment-Based Trunk Control Exercise (NDT-TCE)
2.3.2. Conventional Physiotherapy
2.4. Measurements
2.4.1. Gross Motor Function Measure-88 (GMFM-88)
2.4.2. Segmental Assessment of Trunk Control (SATCo)
2.5. Statistical Analysis
3. Results
3.1. General Characteristics of the Participants
3.2. Comparison of GMFM before and after Intervention within Groups
3.3. Comparison of Changes in SATCo Scores within and between Groups before and after Intervention (Scores: %)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kane, K.; Barden, J. Contributions of trunk muscles to anticipatory postural control in children with and without developmental coordination disorder. Hum. Mov. Sci. 2012, 31, 707–720. [Google Scholar] [CrossRef] [PubMed]
- Bertenthal, B.; Von Hofsten, C. Eye, head and trunk control: The foundation for manual development. Neurosci. Biobehav. Rev. 1998, 22, 515–520. [Google Scholar] [CrossRef] [PubMed]
- Rachwani, J.; Santamaria, V.; Saavedra, S.L.; Wood, S.; Porter, F.; Woollacott, M.H. Segmental trunk control acquisition and reaching in typically developing infants. Exp. Brain Res. 2013, 228, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Hsue, B.J.; Wang, Y.E.; Chen, Y.J. The movement patterns used to rise from a supine position by children with developmental delay and age-related differences in these. Res. Dev. Disabil. 2014, 35, 2205–2214. [Google Scholar] [CrossRef]
- Johnston, L.M.; Burns, Y.R.; Brauer, S.G.; Richardson, C.A. Differences in postural control and movement performance during goal directed reaching in children with developmental coordination disorder. Hum. Mov. Sci. 2002, 21, 583–601. [Google Scholar] [CrossRef]
- Inamdar, K.; Molinini, R.M.; Panibatla, S.T.; Chow, J.C.; Dusing, S.C. Physical therapy interventions to improve sitting ability in children with or at-risk for cerebral palsy: A systematic review and meta-analysis. Dev. Med. Child Neurol. 2021, 63, 396–406. [Google Scholar] [CrossRef]
- Dornelas, L.d.F.; Magalhães, L.D.C. Functional performance of school children diagnosed with developmental delay up to two years of age. Rev. Paul. Pediatr. 2016, 34, 78–85. [Google Scholar] [CrossRef]
- Pin, T.W.; Butler, P.B.; Cheung, H.-M.; Shum, S.L.-F. Relationship between segmental trunk control and gross motor development in typically developing infants aged from 4 to 12 months: A pilot study. BMC Pediatr. 2019, 19, 425. [Google Scholar] [CrossRef]
- Dewar, R.; Love, S.; Johnston, L.M. Exercise interventions improve postural control in children with cerebral palsy: A systematic review. Dev. Med. Child Neurol. 2015, 57, 504–520. [Google Scholar] [CrossRef]
- Choo, Y.Y.; Agarwal, P.; How, C.; Yeleswarapu, S. Developmental delay: Identification and management at primary care level. Singap. Med. J. 2019, 60, 119–123. [Google Scholar] [CrossRef]
- Brown, G.T.; Burns, S.A. The efficacy of neurodevelopmental treatment in paediatrics: A systematic review. Br. J. Occup. Ther. 2001, 64, 213–264. [Google Scholar] [CrossRef]
- Graham, J.V.; Eustace, C.; Brock, K.; Swain, E.; Irwin-Carruthers, S. The Bobath concept in contemporary clinical practice. Top. Stroke Rehabil. 2009, 16, 57–68. [Google Scholar] [CrossRef] [PubMed]
- Mayston, M. Bobath and Neuro Developmental Therapy: What is the future? Dev. Med. Child Neurol. 2016, 58, 994. [Google Scholar] [CrossRef] [PubMed]
- Velicković, T.D. Basic Principles of the Neurodevelopmental treatment (NDT) Bobath. Paediatr. Croat. 2002, 46 (Suppl. S1), 163. [Google Scholar]
- Arı, G.; Günel, M.K. A Randomised Controlled Study to Investigate Effects of Bobath Based Trunk Control Training on Motor Function of Children with Spastic Bilateral Cerebral Palsy. Int. J. Clin. Med. 2017, 8, 205. [Google Scholar] [CrossRef]
- Tekin, F.; Kavlak, E.; Cavlak, U.; Altug, F. Effectiveness of Neuro-Developmental Treatment (Bobath Concept) on postural control and balance in Cerebral Palsied children. J. Back Musculoskelet. Rehabil. 2018, 31, 397–403. [Google Scholar] [CrossRef]
- Labaf, S.; Shamsoddini, A.; Hollisaz, M.T.; Sobhani, V.; Shakibaee, A. Effects of Neurodevelopmental Therapy on Gross Motor Function in Children with Cerebral Palsy. Iran. J. Child Neurol. 2015, 9, 36–41. [Google Scholar]
- Lee, K.H.; Park, J.W.; Lee, H.J.; Nam, K.Y.; Park, T.J.; Kim, H.J.; Kwon, B.S. Efficacy of Intensive Neurodevelopmental Treatment for Children with Developmental Delay, With or Without Cerebral Palsy. Ann. Rehabil. Med. 2017, 41, 90–96. [Google Scholar] [CrossRef]
- Arndt, S.W.; Chandler, L.S.; Sweeney, J.K.; Sharkey, M.A.; McElroy, J.J. Effects of a Neurodevelopmental Treatment-Based Trunk Protocol for Infants with Posture and Movement Dysfunction. Pediatr. Phys. Ther. 2008, 20, 11–22. [Google Scholar] [CrossRef]
- Kyvelidou, A.; Harbourne, R.; Willett, S.L.; Stergiou, N. Sitting postural control in infants with typical development, motor delay, or cerebral palsy. Pediatr. Phys. Ther. 2013, 25, 46–51. [Google Scholar] [CrossRef]
- Barbosa, V.M.; Campbell, S.; Smith, E.; Berbaum, M. Comparison of test of infant motor performance (TIMP) item responses among children with cerebral palsy, developmental delay, and typical development. Am. J. Occup. Ther. 2005, 59, 446–456. [Google Scholar] [CrossRef] [PubMed]
- Berger, S.E.; Harbourne, R.T.; Guallpa Lliguichuzhca, C.L. Sit Still and Pay Attention! Trunk Movement and Attentional Resources in Infants with Typical and Delayed Development. Phys. Occup. Ther. Pediatr. 2019, 39, 48–59. [Google Scholar] [CrossRef] [PubMed]
- Russell, D.J.; Rosenbaum, P.L.; Cadman, D.T.; Gowland, C.; Hardy, S.; Jarvis, S. The gross motor function measure: A means to evaluate the effects of physical therapy. Dev. Med. Child Neurol. 1989, 31, 341–352. [Google Scholar] [CrossRef] [PubMed]
- Ko, J.; Kim, M. Inter-rater Reliability of the K-GMFM-88 and the GMPM for Children with Cerebral Palsy. Ann. Rehabil. Med. 2012, 36, 233–239. [Google Scholar] [CrossRef]
- Alotaibi, M.; Long, T.; Kennedy, E.; Bavishi, S. The efficacy of GMFM-88 and GMFM-66 to detect changes in gross motor function in children with cerebral palsy (CP): A literature review. Disabil. Rehabil. 2014, 36, 617–627. [Google Scholar] [CrossRef]
- Butler, P.B.; Saavedra, S.; Sofranac, M.; Jarvis, S.E.; Woollacott, M.H. Refinement, reliability, and validity of the segmental assessment of trunk control. Pediatr. Phys. Ther. 2010, 22, 246–257. [Google Scholar] [CrossRef]
- Pin, T.W.; Butler, P.B.; Cheung, H.-M.; Shum, S.L.-F. Segmental Assessment of Trunk Control in infants from 4 to 9 months of age- a psychometric study. BMC Pediatr. 2018, 18, 182. [Google Scholar] [CrossRef]
- Sah, A.K.; Balaji, G.K.; Agrahara, S. Effects of Task-oriented Activities Based on Neurodevelopmental Therapy Principles on Trunk Control, Balance, and Gross Motor Function in Children with Spastic Diplegic Cerebral Palsy: A Single-blinded Randomized Clinical Trial. J. Pediatr. Neurosci. 2019, 14, 120–126. [Google Scholar]
- Ahmed, M.; Azeim, F.H.; Ragaa, E.; Raouf, A. The Problem Solving Strategy of Poor Core Stability in Children with Cerebral Palsy: A Clinical Trial. J. Pediatr. Neonatal. Care 2014, 1, 37. [Google Scholar]
- Ardolino, E.; Flores, M.; Manella, K. Gross Motor Outcomes After Dynamic Weight-Bearing in 2 Children with Trunk Hypotonia: A Case Series. Pediatr. Phys. Ther. 2017, 29, 360–364. [Google Scholar] [CrossRef]
- Flores, M.P.; Mitchell, K.P.; Bickley, C.P.; Da Silva, C.P.P. Psychometric Properties of Segmental Assessment of Trunk Control in Infants and Toddlers with Down Syndrome. Pediatr. Phys. Ther. 2020, 32, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Abd El-Nabie, W.A.E.; Saleh, M.S.M. Trunk and pelvic alignment in relation to postural control in children with cerebral palsy. J. Back Musculoskelet. Rehabil. 2019, 32, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Heyrman, L.; Molenaers, G.; Desloovere, K.; Verheyden, G.; De Cat, J.; Monbaliu, E.; Feys, H. A clinical tool to measure trunk control in children with cerebral palsy: The Trunk Control Measurement Scale. Res. Dev. Disabil. 2011, 32, 2624–2635. [Google Scholar] [CrossRef] [PubMed]
- Cholewicki, J.; Panjabi, M.M.; Khachatryan, A. Stabilizing function of trunk flexor-extensor muscles around a neutral spine posture. Spine 1997, 22, 2207–2212. [Google Scholar] [CrossRef]
- Sharma, S.; Begum, R. Effects of NDT Treatment Based Trunk Protocol on Gross Motor Function of Spastic CP Children. Indian J. Physiother. Occup. Ther. 2019, 13, 186. [Google Scholar] [CrossRef]
- Harries, N.; Kassirer, M.; Amichai, T.; Lahat, E. Changes over years in gross motor function of 3–8 year old children with cerebral palsy: Using the Gross Motor Function Measure (GMFM-88). Isr. Med. Assoc. J. 2004, 6, 408–411. [Google Scholar]
- Sung, I.Y.; Cho, S.C.; Lee, N.H. Scoring of Norms of the Gross Motor Function Measure (GMFM) in Normal Children. Ann. Rehabil. Med. 2002, 26, 7–402. [Google Scholar]
- Kwon, J.Y.; Chang, H.J.; Yoo, H.J. Clinical significance of change in gross motor function measure in children with cerebral palsy. J. Phys. Ther. Sci. 2020, 32, 462–467. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| General Characteristics | Experimental Group | Control Group | p-Value |
|---|---|---|---|
| N (Male/Female) | 12 (6/6) | 8 (5/3) | 0.927 |
| Mean age (months) (±SD) | 21.92 ± 12.27 | 32.75 ± 21.95 | 0.046 |
| Diagnosis | |||
| Unspecified (developmental disorder) | 3 | 1 | |
| Tetralogy of Fallot | 2 | - | |
| Brain damage | 1 | 1 | |
| Hypotonicity | 2 | - | |
| Lennox-Gastaut syndrome | 1 | - | |
| Coffin-Siris syndrome | - | 1 | |
| Down syndrome | - | 2 | |
| Chromosomal abnormality | 1 | 1 | |
| Suspected chromosomal abnormalities | 2 | - | |
| Cytomegaloviral disease | - | 1 | |
| Congenital toxoplasmosis | - | 1 | |
| Mean GMFCS level (±SD) | 3.75 ± 0.97 | 3.38 ± 1.30 | |
| I | - | - | |
| II | 1 | 3 | |
| III | 4 | 1 | |
| IV | 4 | 2 | |
| V | 3 | 2 | |
| Mean ± SD | |||||
|---|---|---|---|---|---|
| Pre-Intervention | Post-Intervention | z | p-Value (1) | ||
| GMFM A | Experimental group | 73.04 ± 26.00 | 87.73 ± 14.53 | −2.668 | 0.008 |
| Control group | 79.71 ± 29.22 | 85.29 ± 22.67 | −1.841 | 0.006 | |
| p-value (2) | 0.065 | ||||
| GMFM B | Experimental group | 41.67 ± 27.93 | 67.36 ± 27.99 | −3.064 | 0.002 |
| Control group | 54.36 ± 32.16 | 61.89 ± 34.03 | −2.524 | 0.012 | |
| p-value (2) | 0.002 | ||||
| GMFM C | Experimental group | 15.48 ± 28.18 | 33.73 ± 36.92 | −2.366 | 0.018 |
| Control group | 40.19 ± 34.50 | 47.66 ± 39.44 | −2.371 | 0.018 | |
| p-value (2) | 0.423 | ||||
| GMFM D | Experimental group | 5.98 ± 14.43 | 16.45 ± 26.25 | −2.207 | 0.027 |
| Control group | 16.35 ± 21.58 | 22.45 ± 24.32 | −1.826 | 0.068 | |
| p-value (2) | 0.861 | ||||
| GMFM E | Experimental group | 0.00 ± 0.00 | 2.02 ± 5.46 | −1.342 | 0.180 |
| Control group | 3.99 ± 6.85 | 6.95 ± 9.06 | −1.826 | 0.068 | |
| p-value (2) | 0.893 | ||||
| GMFM Total | Experimental group | 27.23 ± 16.82 | 40.96 ± 20.22 | −3.061 | 0.002 |
| Control group | 38.92 ± 22.46 | 44.84 ± 24.01 | −2.521 | 0.012 | |
| p-value (2) | 0.046 | ||||
| Mean ± SD | z | p-Value (1) | |||
|---|---|---|---|---|---|
| Pre-Intervention | Post-Intervention | ||||
| Static control | Experimental group | 4.92 ± 2.11 | 7.00 ± 1.13 | −3.097 | 0.002 |
| Control group | 5.63 ± 2.26 | 6.38 ± 2.00 | −2.121 | 0.034 | |
| p-value (2) | 0.004 | ||||
| Active control | Experimental group | 3.17 ± 2.76 | 6.33 ± 2.15 | −3.078 | 0.002 |
| Control group | 4.88 ± 2.48 | 5.63 ± 2.77 | −2.121 | 0.034 | |
| p-value (2) | 0.005 | ||||
| Reactive control | Experimental group | 0.83 ± 1.27 | 3.42 ± 3.29 | −2.384 | 0.017 |
| Control group | 0.88 ± 1.25 | 2.00 ± 2.27 | −1.841 | 0.066 | |
| p-value (2) | 0.239 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, M.; Kim, J.; Yu, C.; Lim, H. The Effects of Neurodevelopmental Treatment-Based Trunk Control Exercise on Gross Motor Function and Trunk Control in Children with Developmental Disabilities. Healthcare 2023, 11, 1446. https://doi.org/10.3390/healthcare11101446
Park M, Kim J, Yu C, Lim H. The Effects of Neurodevelopmental Treatment-Based Trunk Control Exercise on Gross Motor Function and Trunk Control in Children with Developmental Disabilities. Healthcare. 2023; 11(10):1446. https://doi.org/10.3390/healthcare11101446
Chicago/Turabian StylePark, Miho, Jeongseon Kim, Changseon Yu, and Hyoungwon Lim. 2023. "The Effects of Neurodevelopmental Treatment-Based Trunk Control Exercise on Gross Motor Function and Trunk Control in Children with Developmental Disabilities" Healthcare 11, no. 10: 1446. https://doi.org/10.3390/healthcare11101446
APA StylePark, M., Kim, J., Yu, C., & Lim, H. (2023). The Effects of Neurodevelopmental Treatment-Based Trunk Control Exercise on Gross Motor Function and Trunk Control in Children with Developmental Disabilities. Healthcare, 11(10), 1446. https://doi.org/10.3390/healthcare11101446