
Potential Factors Associated with Healthcare Utilization for Balance Problems in Community-Dwelling Adults within the United States: A Narrative Review

{kind=link}
Abstract
:1. Introduction
1.1. Background
1.2. Burden on Healthcare
1.3. Healthcare Utilization
1.4. Objective and Significance
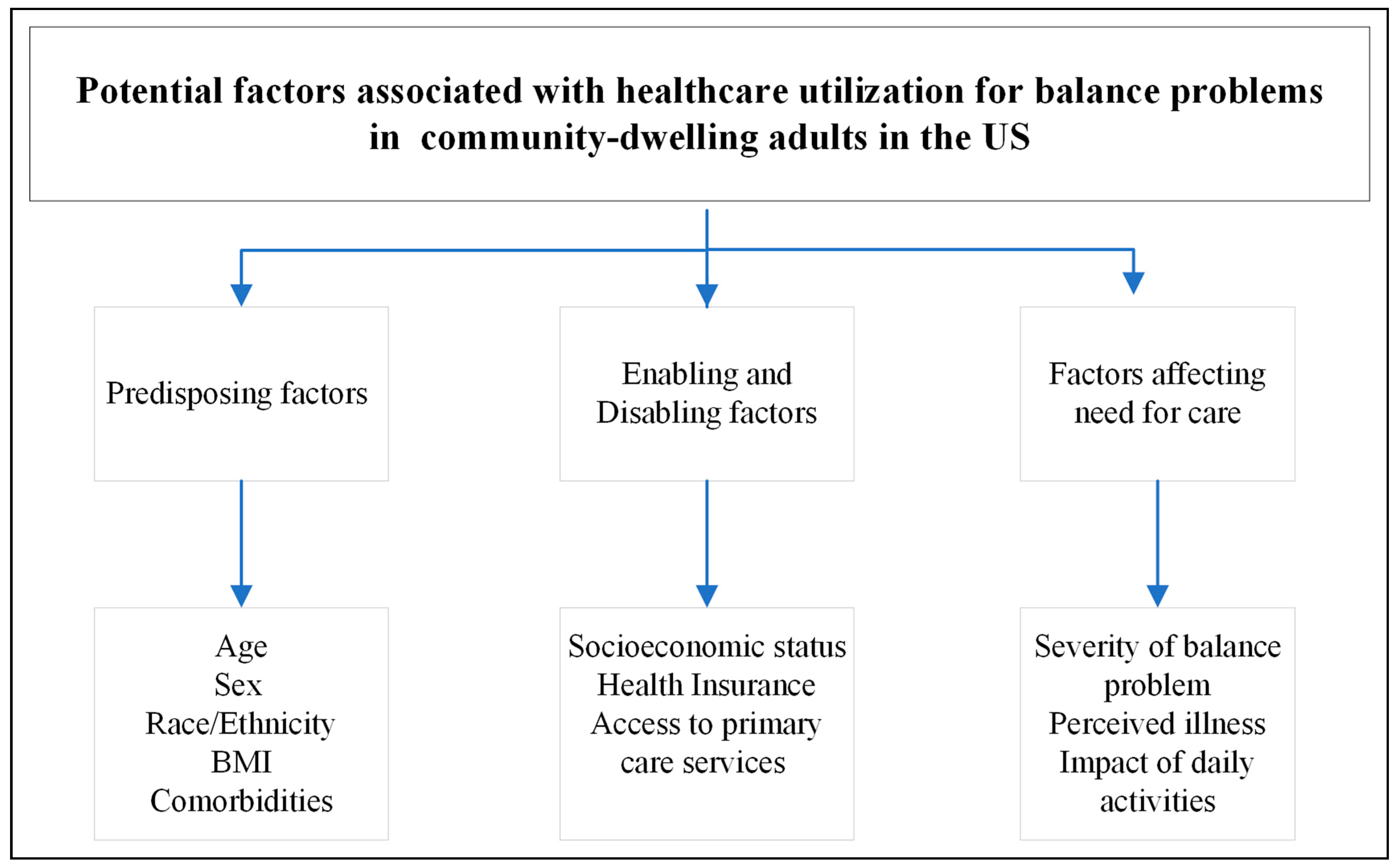
2. Framework
3. Predisposing Factors
3.1. Age
3.2. Sex
3.3. Race/Ethnicity
3.4. Body Mass Index (BMI)
3.5. Comorbidities
4. Enabling and Disabling Factors
4.1. Socioeconomic Status
4.2. Health Insurance
4.3. Access to Primary Care Services
5. Factors Affecting Need for Care
5.1. Severity of Balance Problem
5.2. Perceived Illness
5.3. Impact on Daily Activities
6. Conclusions
7. Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shumway-Cook, A.; Woollacott, M. Motor Control: Theory and Practical Applications; Lippincott, Williams & Wilkins: Philadelphia, PA, USA, 2001. [Google Scholar]
- Vestibular Disorders Association; Ann Watson, M.; Owen Black, F.; Crowson, M. The Human Balance System. VeDA. Available online: https://vestibular.org/article/what-is-vestibular/the-human-balance-system/the-human-balance-system-how-do-we-maintain-our-balance/ (accessed on 27 October 2022).
- Hoffman, G.; Franco, N.; Perloff, J.; Lynn, J.; Okoye, S.; Min, L. Incidence of and County Variation in Fall Injuries in US Residents Aged 65 Years or Older, 2016–2019. JAMA Netw. Open 2022, 5, e2148007. [Google Scholar] [CrossRef]
- Lin, H.W.; Bhattacharyya, N. Balance disorders in the elderly: Epidemiology and functional impact. Laryngoscope 2012, 122, 1858–1861. [Google Scholar] [CrossRef] [PubMed]
- Bergen, G.; Stevens, M.R.; Burns, E.R. Falls and Fall Injuries Among Adults Aged ≥65 Years–United States, 2014. MMWR Morb. Mortal Wkly. Rep. 2016, 65, 993–998. [Google Scholar] [CrossRef]
- NHANES. National Health and Nutrition Examination Survey. Center for Disease Control, USA. 2022. Available online: https://wwwn.cdc.gov/Nchs/Nhanes/limited_access/BAQ_K_R.htm (accessed on 29 November 2022).
- Aggarwal, N.T.; Bennett, D.A.; Bienias, J.L.; Mendes de Leon, C.F.; Morris, M.C.; Evans, D.A. The prevalence of dizziness and its association with functional disability in a biracial community population. J. Gerontol. A Biol. Sci. Med. Sci. 2000, 55, M288–M292. [Google Scholar] [CrossRef] [PubMed]
- Penger, M.; Strobl, R.; Grill, E. Country-specific and individual determinants of dizziness in Europe: Results from the Survey of Health Ageing and Retirement in Europe (SHARE). Public Health 2017, 149, 1–10. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Falls. WHO. Available online: https://www.who.int/news-room/fact-sheets/detail/falls (accessed on 20 October 2022).
- Agrawal, Y.C.J.; Della Santina, C.C.; Schubert, M.C.; Minor, L.B. Disorders of Balance and Vestibular Function in US Adults: Data From the National Health and Nutrition Examination Survey, 2001–2004. Arch. Intern. Med. 2009, 169, 938–944. [Google Scholar] [CrossRef] [PubMed]
- National Center for Injury Prevention and Control, 10 Leading Causes of Nonfatal Unintentional Emergency Department Visits, United States. CDC; 2020. Available online: https://wisqars.cdc.gov/cgi-bin/broker.exe (accessed on 27 October 2022).
- Burns, E.R.; Stevens, J.A.; Lee, R. The direct costs of fatal and non-fatal falls among older adults –United States. J. Saf. Res. 2016, 58, 99–103. [Google Scholar] [CrossRef]
- Office of Disease Prevention and Health Promotion, US Department of Health and Human Services. Healthy People 2030. Available online: https://health.gov/healthypeople/objectives-and-data/browse-objectives/sensory-or-communication-disorders/increase-proportion-adults-dizziness-or-balance-problems-who-have-been-referred-specialist-hoscd-11/data (accessed on 20 October 2022).
- Choi, N.G.; Choi, B.Y.; DiNitto, D.M.; Marti, C.N.; Kunik, M.E. Fall-related emergency department visits and hospitalizations among community-dwelling older adults: Examination of health problems and injury characteristics. BMC Geriatr. 2019, 19, 303. [Google Scholar] [CrossRef] [PubMed]
- Phillips, K.A.; Morrison, K.R.; Andersen, R.; Aday, L.A. Understanding the context of healthcare utilization: Assessing environmental and provider-related variables in the behavioral model of utilization. Health Serv. Res. 1998, 33 Pt 1, 571–596. [Google Scholar] [PubMed]
- Andersen, R.M. Revisiting the behavioral model and access to medical care: Does it matter? J. Health Soc. Behav. 1995, 36, 1–10. [Google Scholar] [CrossRef]
- Andersen, R.; Newman, J.F. Societal and individual determinants of medical care utilization in the United States. Milbank Mem. Fund. Q. Health Soc. 1973, 51, 95–124. [Google Scholar] [CrossRef] [PubMed]
- Peel, N.M.; Kassulke, D.J.; McClure, R.J. Population based study of hospitalised fall related injuries in older people. Inj. Prev. 2002, 8, 280–283. [Google Scholar] [CrossRef]
- Jacobs, M.M.; Ellis, C. Heterogeneity among women with stroke: Health, demographic and healthcare utilization differentials. BMC Womens Health 2021, 21, 160. [Google Scholar] [CrossRef]
- van den Bussche, H.; Kaduszkiewicz, H.; Schäfer, I.; Koller, D.; Hansen, H.; Scherer, M.; Schön, G. Overutilization of ambulatory medical care in the elderly German population?–An empirical study based on national insurance claims data and a review of foreign studies. BMC Health Serv. Res. 2016, 16, 129. [Google Scholar] [CrossRef] [PubMed]
- Daly, R.M.; Rosengren, B.E.; Alwis, G.; Ahlborg, H.G.; Sernbo, I.; Karlsson, M.K. Gender specific age-related changes in bone density, muscle strength and functional performance in the elderly: A-10 year prospective population-based study. BMC Geriatr. 2013, 13, 71. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.S.; Bishu, K.; Dismuke, C.E.; Egede, L.E. Sex differences in healthcare expenditures among adults with diabetes: Evidence from the medical expenditure panel survey, 2002–2011. BMC Health Serv. Res. 2017, 17, 259. [Google Scholar] [CrossRef] [PubMed]
- Dark, T.; Rust, G.; Sehres, G.; Harman, J.S. Racial Disparities in Healthcare Utilization Among Individuals with Cardiometabolic Risk Factors and Comorbid Anxiety Disorder. J. Racial Ethn. Health Disparities 2020, 7, 1234–1240. [Google Scholar] [CrossRef]
- Saadi, A.; Himmelstein, D.U.; Woolhandler, S.; Mejia, N.I. Racial disparities in neurologic health care access and utilization in the United States. Neurology 2017, 88, 2268–2275. [Google Scholar] [CrossRef]
- Jarman, M.P.; Sokas, C.; Dalton, M.K.; Castillo-Angeles, M.; Uribe-Leitz, T.; Heng, M.; von Keudell, A. Cooper, Z.; Salim, A. The impact of delayed management of fall-related hip fracture management on health outcomes for African American older adults. J. Trauma Acute Care Surg. 2021, 90, 942–950. [Google Scholar] [CrossRef]
- Edwards, C.H.; Aas, E.; Kinge, J.M. Body mass index and lifetime healthcare utilization. BMC Health Serv. Res. 2019, 19, 696. [Google Scholar] [CrossRef]
- Finkelstein, E.A.; Chen, H.; Prabhu, M.; Trogdon, J.G.; Corso, P.S. The relationship between obesity and injuries among U.S. adults. Am. J. Health Promot. 2007, 21, 460–468. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Hu, X.; Zhang, Q.; Zou, R. Diabetes mellitus and risk of falls in older adults: A systematic review and meta-analysis. Age Ageing 2016, 45, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Trevisan, C.; Crippa, A.; Ek, S.; Welmer, A.K.; Sergi, G.; Maggi, S.; Manzato, E.; Bea, J.W.; Cauley, J.A.; Decullier, E.; et al. Nutritional Status, Body Mass Index, and the Risk of Falls in Community-Dwelling Older Adults: A Systematic Review and Meta-Analysis. J. Am. Med. Dir. Assoc. 2019, 20, 569–582.e7. [Google Scholar] [CrossRef] [PubMed]
- van den Bussche, H.; Schön, G.; Kolonko, T.; Hansen, H.; Wegscheider, K.; Glaeske, G.; Koller, D. Patterns of ambulatory medical care utilization in elderly patients with special reference to chronic diseases and multimorbidity—Results from a claims data based observational study in Germany. BMC Geriatr. 2011, 11, 54. [Google Scholar] [CrossRef] [PubMed]
- Nilsagård, Y.; Gunn, H.; Freeman, J.; Hoang, P.; Lord, S.; Mazumder, R.; Cameron, M. Falls in people with MS–An individual data meta-analysis from studies from Australia, Sweden, United Kingdom and the United States. Mult. Scler. 2015, 21, 92–100. [Google Scholar] [CrossRef]
- Cameron, M.H.; Nilsagard, Y. Balance, gait, and falls in multiple sclerosis. Handb. Clin. Neurol. 2018, 159, 237–250. [Google Scholar] [CrossRef]
- Homann, C.N.; Homann, B.; Ivanic, G.; Urbanic-Purkart, T. Accidental Falls in Patients with Hyperkinetic Movement Disorders: A Systematic Review. Tremor. Other Hyperkinet. Mov. 2022, 12, 30. [Google Scholar] [CrossRef]
- Bloem, B.R.; Grimbergen, Y.A.; Cramer, M.; Willemsen, M.; Zwinderman, A.H. Prospective assessment of falls in Parkinson’s disease. J. Neurol. 2001, 248, 950–958. [Google Scholar] [CrossRef]
- Rudzińska, M.; Bukowczan, S.; Stożek, J.; Zajdel, K.; Mirek, E.; Chwała, W.; Wójcik-Pędziwiatr, M.; Banaszkiewicz, K.; Szczudlik, A. The incidence and risk factors of falls in Parkinson disease: Prospective study. Neurol. Neurochir. Pol. 2013, 47, 431–437. [Google Scholar] [CrossRef]
- Deandrea, S.; Lucenteforte, E.; Bravi, F.; Foschi, R.; La Vecchia, C.; Negri, E. Risk factors for falls in community-dwelling older people: A systematic review and meta-analysis. Epidemiology 2010, 21, 658–668. [Google Scholar] [CrossRef]
- Shalev, V.; Chodick, G.; Heymann, A.D.; Kokia, E. Gender differences in healthcare utilization and medical indicators among patients with diabetes. Public Health 2005, 119, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Minejima, E.; Wong-Beringer, A. Impact of Socioeconomic Status and Race on Sepsis Epidemiology and Outcomes. J. Appl. Lab. Med. 2021, 6, 194–209. [Google Scholar] [CrossRef] [PubMed]
- Frølich, A.; Ghith, N.; Schiøtz, M.; Jacobsen, R.; Stockmarr, A. Multimorbidity, healthcare utilization and socioeconomic status: A register-based study in Denmark. PLoS ONE 2019, 14, e0214183. [Google Scholar] [CrossRef] [PubMed]
- Grits, D.; Emara, A.K.; Klika, A.K.; Murray, T.G.; McLaughlin, J.P.; Piuzzi, N.S. Neighborhood Socioeconomic Disadvantage Associated with Increased Healthcare Utilization after Total Hip Arthroplasty. J. Arthroplast. 2022, 37, 1980–1986. [Google Scholar] [CrossRef]
- Singh, J.A.; Cleveland, J.D. Socioeconomic status and healthcare access are associated with healthcare utilization after knee arthroplasty: A U.S. national cohort study. Jt. Bone Spine 2020, 87, 157–162. [Google Scholar] [CrossRef]
- Freeman, J.D.; Kadiyala, S.; Bell, J.F.; Martin, D.P. The causal effect of health insurance on utilization and outcomes in adults: A systematic review of US studies. Med. Care 2008, 46, 1023–1032. [Google Scholar] [CrossRef]
- Cooper, J.N.; Koppera, S.; Boss, E.F.; Lind, M.N. Differences in Tonsillectomy Utilization by Race/Ethnicity, Type of Health Insurance, and Rurality. Acad. Pediatr. 2021, 21, 1031–1036. [Google Scholar] [CrossRef]
- Dieleman, J.L.; Cao, J.; Chapin, A.; Chen, C.; Li, Z.; Liu, A.; Horst, C.; Kaldjian, A.; Matyasz, T.; Scott, K.W.; et al. US Health Care Spending by Payer and Health Condition, 1996–2016. JAMA 2020, 323, 863–884. [Google Scholar] [CrossRef]
- Corscadden, L.; Levesque, J.F.; Lewis, V.; Strumpf, E.; Breton, M.; Russell, G. Factors associated with multiple barriers to access to primary care: An international analysis. Int. J. Equity Health 2018, 17, 28. [Google Scholar] [CrossRef]
- Glass, D.P.; Kanter, M.H.; Jacobsen, S.J.; Minardi, P.M. The impact of improving access to primary care. J. Eval. Clin. Pract. 2017, 23, 1451–1458. [Google Scholar] [CrossRef]
- Goodwin, A.J.; Nadig, N.R.; McElligott, J.T.; Simpson, K.N.; Ford, D.W. Where You Live Matters: The Impact of Place of Residence on Severe Sepsis Incidence and Mortality. Chest 2016, 150, 829–836. [Google Scholar] [CrossRef]
- Murimi-Worstell, I.B.; Lin, D.H.; Kan, H.; Tierce, J.; Wang, X.; Nab, H.; Desta, B.; Alexander, G.C.; Hammond, E.R. Healthcare Utilization and Costs of Systemic Lupus Erythematosus by Disease Severity in the United States. J. Rheumatol. 2021, 48, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Kobelt, G.; Thompson, A.; Berg, J.; Gannedahl, M.; Eriksson, J.; Group, M.S.; Platform, E.M.S. New insights into the burden and costs of multiple sclerosis in Europe. Mult. Scler. 2017, 23, 1123–1136. [Google Scholar] [CrossRef] [PubMed]
- Na, L.; Hennessy, S.; Bogner, H.R.; Kurichi, J.E.; Stineman, M.; Streim, J.E.; Kwong, P.L.; Xie, D.; Pezzin, L.E. Disability stage and receipt of recommended care among elderly medicare beneficiaries. Disabil. Health J. 2017, 10, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Min, L.C.; Reuben, D.B.; Keeler, E.; Ganz, D.A.; Fung, C.H.; Shekelle, P.; Roth, C.P.; Wenger, N.S. Is patient-perceived severity of a geriatric condition related to better quality of care? Med. Care 2011, 49, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Scuccato, R. Falls in the elderly. Recent. Prog. Med. 2018, 109, 401–404. [Google Scholar] [CrossRef]
- Taburee, W.; Sirilak, S.; Khotcharrat, R.; Anekpunyakul, P.; Dilokthornsakul, P.; Lukkahatai, N.; Boongird, C. Health-Related Problems and Drivers of Health-Related Quality of Life Among Community-Dwelling Older Adults. J. Prim Care Community Health 2020, 11, 2150132720913724. [Google Scholar] [CrossRef]
- Boyé, N.D.; Mattace-Raso, F.U.; Van Lieshout, E.M.; Hartholt, K.A.; Van Beeck, E.F.; Van der Cammen, T.J. Physical performance and quality of life in single and recurrent fallers: Data from the Improving Medication Prescribing to Reduce Risk of Falls study. Geriatr. Gerontol. Int. 2015, 15, 350–355. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kapur, S.; Sakyi, K.S.; Lohia, P.; Goble, D.J. Potential Factors Associated with Healthcare Utilization for Balance Problems in Community-Dwelling Adults within the United States: A Narrative Review. Healthcare 2023, 11, 2398. https://doi.org/10.3390/healthcare11172398
Kapur S, Sakyi KS, Lohia P, Goble DJ. Potential Factors Associated with Healthcare Utilization for Balance Problems in Community-Dwelling Adults within the United States: A Narrative Review. Healthcare. 2023; 11(17):2398. https://doi.org/10.3390/healthcare11172398
Chicago/Turabian StyleKapur, Shweta, Kwame S. Sakyi, Prateek Lohia, and Daniel J. Goble. 2023. "Potential Factors Associated with Healthcare Utilization for Balance Problems in Community-Dwelling Adults within the United States: A Narrative Review" Healthcare 11, no. 17: 2398. https://doi.org/10.3390/healthcare11172398