
Digital Health for Patients Undergoing Cardiac Surgery: A Systematic Review
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Risk of Bias and Quality Assessment
3. Results
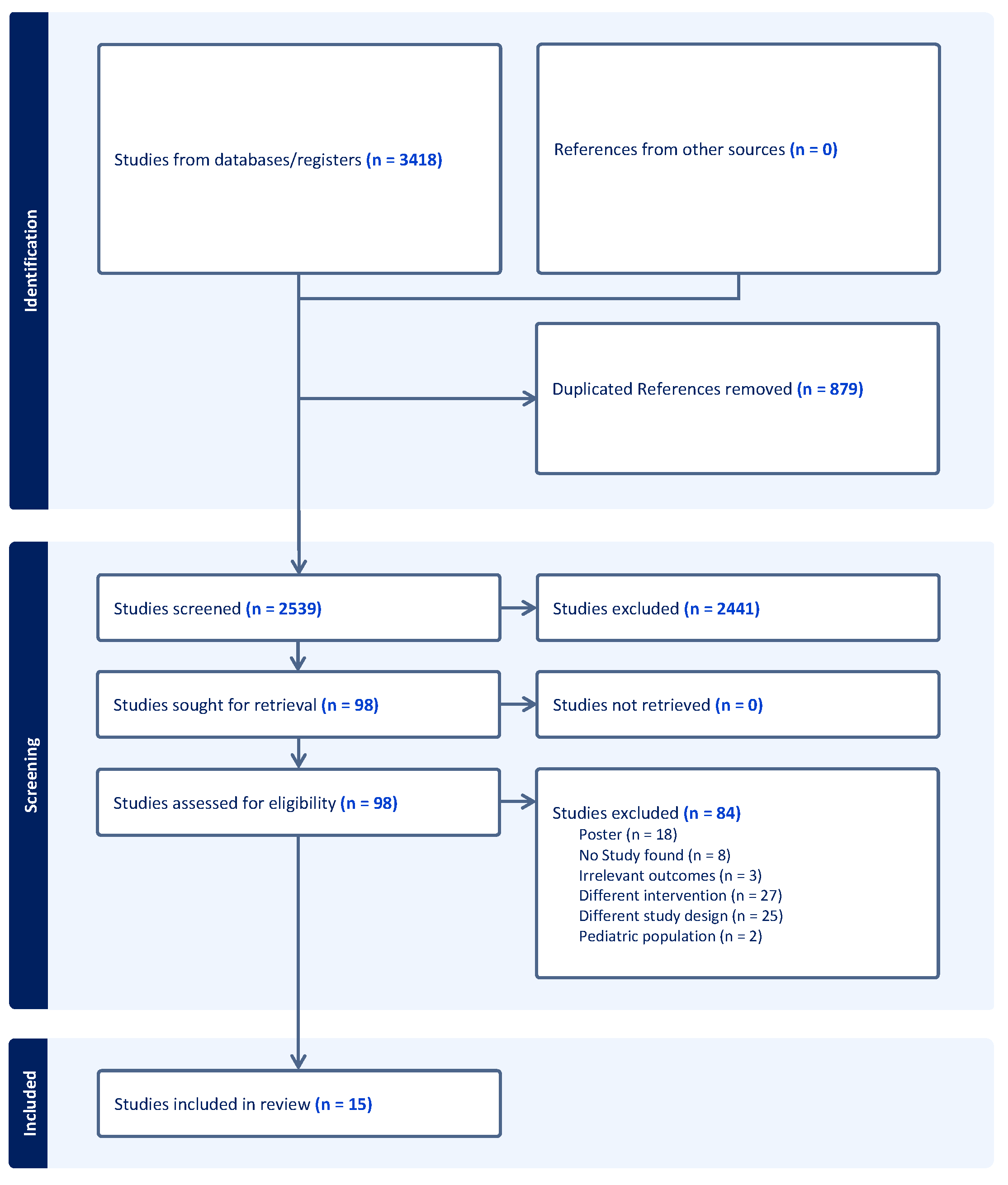
3.1. Literature Search
3.2. Digital Health Application
3.3. Risk of Bias and Quality Assessment
3.4. Randomized Control Trials
3.5. Nonrandomized Cohort Studies
3.6. Country of Origin
3.7. Data Synthesis
4. Discussion
4.1. Randomized Control Studies
4.2. NorRandomized Cohort Studies
4.3. Country of Origin
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; de Ferranti, S.; Després, J.P.; Fullerton, H.J.; et al. Heart Disease and Stroke Statistics-2016 Update: A Report From the American Heart Association. Circulation 2016, 133, e38–e360. [Google Scholar] [CrossRef]
- Doenst, T.; Kirov, H.; Moschovas, A.; Gonzalez-Lopez, D.; Safarov, R.; Diab, M.; Bargenda, S.; Faerber, G. Cardiac surgery 2017 reviewed. Clin. Res. Cardiol. 2018, 107, 1087–1102. [Google Scholar] [CrossRef]
- Vervoort, D.; Meuris, B.; Meyns, B.; Verbrugghe, P. Global cardiac surgery: Access to cardiac surgical care around the world. J. Thorac. Cardiovasc. Surg. 2020, 159, 987–996.e986. [Google Scholar] [CrossRef]
- Senst, B.; Kumar, A.; Diaz, R.R. Cardiac Surgery; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Açıkel, M.E.T. Evaluation of Depression and Anxiety in Coronary Artery Bypass Surgery Patients: A Prospective Clinical Study. Braz. J. Cardiovasc. Surg. 2019, 34, 389–395. [Google Scholar] [CrossRef]
- Curcio, N.; Philpot, L.; Bennett, M.; Felius, J.; Powers, M.B.; Edgerton, J.; Warren, A.M. Anxiety, depression, and healthcare utilization 1 year after cardiac surgery. Am. J. Surg. 2019, 218, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Vogel, B.A.; Leonhart, R.; Helmes, A.W. Communication matters: The impact of communication and participation in decision making on breast cancer patients’ depression and quality of life. Patient Educ. Couns. 2009, 77, 391–397. [Google Scholar] [CrossRef]
- Kao, C.K.; Liebovitz, D.M. Consumer Mobile Health Apps: Current State, Barriers, and Future Directions. PM R 2017, 9, S106–S115. [Google Scholar] [CrossRef]
- Sarkar, S.; MacLeod, J.; Hassan, A.; Brunt, K.R.; Palmer, K.; Légaré, J.F. Enhanced Telehealth Home-Monitoring Intervention for Vulnerable and Frail Patients after Cardiac Surgery (THE-FACS Pilot Intervention Study). BMC Geriatr. 2022, 22, 836. [Google Scholar] [CrossRef]
- Carlson, L.; O’Brien, J.; Gujral, N.; Chiang, V.; Del Nido, P.; Nathan, M. Digital solution for follow-up in congenital cardiac surgery. Cardiol. Young 2022, 32, 1032–1040. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.S.; Jie, C.; Joe, J.; Irani, Z.D.; Ganguli, S.; Kalva, S.P.; Wicky, S.; Wu, S. The impact of transvenous cardiac devices on vascular access patency in hemodialysis patients. Semin. Dial. 2013, 26, 728–732. [Google Scholar] [CrossRef] [PubMed]
- Conard, S. Best practices in digital health literacy. Int. J. Cardiol. 2019, 292, 277–279. [Google Scholar] [CrossRef]
- Lopez-Olivo, M.A.; Suarez-Almazor, M.E. Digital Patient Education and Decision Aids. Rheum. Dis. Clin. N. Am. 2019, 45, 245–256. [Google Scholar] [CrossRef] [PubMed]
- Kataria, S.; Ravindran, V. Digital health: A new dimension in rheumatology patient care. Rheumatol. Int. 2018, 38, 1949–1957. [Google Scholar] [CrossRef]
- Pal, K.; Dack, C.; Ross, J.; Michie, S.; May, C.; Stevenson, F.; Farmer, A.; Yardley, L.; Barnard, M.; Murray, E. Digital Health Interventions for Adults with Type 2 Diabetes: Qualitative Study of Patient Perspectives on Diabetes Self-Management Education and Support. J. Med. Internet Res. 2018, 20, e40. [Google Scholar] [CrossRef]
- Schnitman, G.; Wang, T.; Kundu, S.; Turkdogan, S.; Gotlieb, R.; How, J.; Gotlieb, W. The role of digital patient education in maternal health: A systematic review. Patient Educ. Couns. 2022, 105, 586–593. [Google Scholar] [CrossRef] [PubMed]
- Solvin, H.; Lippert, M.; Holmstrøm, H.; Elle, O.J.; Brun, H. Real-time Remote Expert-guided Echocardiography by Medical Students. Ultrasound. J. 2023, 15, 28. [Google Scholar] [CrossRef] [PubMed]
- Hasan, A.; Mohammed, Y.; Basiony, M.; Hanbazazh, M.; Samman, A.; Abdelaleem, M.F.; Nasr, M.; Abozeid, H.; Mohamed, H.I.; Faisal, M.; et al. Clinico-Pathological Features and Immunohistochemical Comparison of p16, p53, and Ki-67 Expression in Muscle-Invasive and Non-Muscle-Invasive Conventional Urothelial Bladder Carcinoma. Clin. Pract. 2023, 13, 806–819. [Google Scholar] [CrossRef]
- Chen, L.; Chen, M.; Li, Q.; Kumar, V.; Duan, Y.; Wu, K.A.; Pierce, T.T.; Samir, A.E. Machine Learning-Assisted Diagnostic System for Indeterminate Thyroid Nodules. Ultrasound. Med. Biol. 2022, 48, 1547–1554. [Google Scholar] [CrossRef]
- Asiedu, M.; Benjamin, A.; Singh, V.; Wang, S.; Wu, K.; Samir, A.; Kumar, V. A generative adversarial network for ultrasound signal enhancement by transforming low-voltage beamformed radio frequency data to high-voltage data. SPIE Med. Imaging 2022, 2022, 12038. [Google Scholar] [CrossRef]
- Peng, S.; Liu, Y.; Lv, W.; Liu, L.; Zhou, Q.; Yang, H.; Ren, J.; Liu, G.; Wang, X.; Zhang, X.; et al. Deep learning-based artificial intelligence model to assist thyroid nodule diagnosis and management: A multicentre diagnostic study. Lancet Digit. Health 2021, 3, e250–e259. [Google Scholar] [CrossRef]
- Walker, D.; Adebajo, A.; Bukhari, M. The benefits and challenges of providing patient education digitally. Rheumatology 2020, 59, 3591–3592. [Google Scholar] [CrossRef]
- Smith, B.; Magnani, J.W. New technologies, new disparities: The intersection of electronic health and digital health literacy. Int. J. Cardiol. 2019, 292, 280–282. [Google Scholar] [CrossRef] [PubMed]
- Jandoo, T. WHO guidance for digital health: What it means for researchers. Digit. Health 2020, 6, 2055207619898984. [Google Scholar] [CrossRef]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, L.E.; Takahashi, R. A Resource for Developing an Evidence Synthesis Report for Policy-Making; Health Evidence Network Synthesis Report, No. 50; WHO Regional Office for Europe: Copenhagen, Danmark, 2017. [Google Scholar]
- Ben-Ali, W.; Lamarche, Y.; Carrier, M.; Demers, P.; Bouchard, D.; El-Hamamsy, I.; Cartier, R.; Pellerin, M.; Perrault, L.P. Use of Mobile-Based Application for Collection of Patient-Reported Outcomes in Cardiac Surgery. Innovations 2021, 16, 536–544. [Google Scholar] [CrossRef] [PubMed]
- Cook, D.J.; Moradkhani, A.; Douglas, K.S.; Prinsen, S.K.; Fischer, E.N.; Schroeder, D.R. Patient education self-management during surgical recovery: Combining mobile (iPad) and a content management system. Telemed. J. E Health 2014, 20, 312–317. [Google Scholar] [CrossRef]
- Dew, M.A.; Goycoolea, J.M.; Harris, R.C.; Lee, A.; Zomak, R.; Dunbar-Jacob, J.; Rotondi, A.; Griffith, B.P.; Kormos, R.L. An internet-based intervention to improve psychosocial outcomes in heart transplant recipients and family caregivers: Development and evaluation. J. Heart Lung Transplant. 2004, 23, 745–758. [Google Scholar] [CrossRef] [PubMed]
- Gomis-Pastor, M.; Mirabet Perez, S.; Roig Minguell, E.; Brossa Loidi, V.; Lopez Lopez, L.; Ros Abarca, S.; Galvez Tugas, E.; Mas-Malagarriga, N.; Mangues Bafalluy, M.A. Mobile Health to Improve Adherence and Patient Experience in Heart Transplantation Recipients: The mHeart Trial. Healthcare 2021, 9, 463. [Google Scholar] [CrossRef]
- Lunde, P.; Bye, A.; Bergland, A.; Grimsmo, J.; Jarstad, E.; Nilsson, B.B. Long-term follow-up with a smartphone application improves exercise capacity post cardiac rehabilitation: A randomized controlled trial. Eur. J. Prev. Cardiol. 2020, 27, 1782–1792. [Google Scholar] [CrossRef] [PubMed]
- Martorella, G.; Côté, J.; Racine, M.; Choinière, M. Web-based nursing intervention for self-management of pain after cardiac surgery: Pilot randomized controlled trial. J. Med. Internet Res. 2012, 14, e177. [Google Scholar] [CrossRef]
- Melholt, C.; Joensson, K.; Spindler, H.; Hansen, J.; Andreasen, J.J.; Nielsen, G.; Noergaard, A.; Tracey, A.; Thorup, C.; Kringelholt, R.; et al. Cardiac patients’ experiences with a telerehabilitation web portal: Implications for eHealth literacy. Patient. Educ. Couns. 2018, 101, 854–861. [Google Scholar] [CrossRef]
- Schuuring, M.J.; Backx, A.P.; Zwart, R.; Veelenturf, A.H.; Robbers-Visser, D.; Groenink, M.; Abu-Hanna, A.; Bruining, N.; Schijven, M.P.; Mulder, B.J.; et al. Mobile health in adults with congenital heart disease: Current use and future needs. Neth. Heart J. 2016, 24, 647–652. [Google Scholar] [CrossRef] [PubMed]
- Snoek, J.A.; Prescott, E.I.; van der Velde, A.E.; Eijsvogels, T.M.H.; Mikkelsen, N.; Prins, L.F.; Bruins, W.; Meindersma, E.; González-Juanatey, J.R.; Peña-Gil, C.; et al. Effectiveness of Home-Based Mobile Guided Cardiac Rehabilitation as Alternative Strategy for Nonparticipation in Clinic-Based Cardiac Rehabilitation among Elderly Patients in Europe: A Randomized Clinical Trial. JAMA Cardiol. 2021, 6, 463–468. [Google Scholar] [CrossRef] [PubMed]
- Spindler, H.; Leerskov, K.; Joensson, K.; Nielsen, G.; Andreasen, J.J.; Dinesen, B. Conventional Rehabilitation Therapy Versus Telerehabilitation in Cardiac Patients: A Comparison of Motivation, Psychological Distress, and Quality of Life. Int. J. Environ. Res. Public Health 2019, 16, 512. [Google Scholar] [CrossRef]
- van Steenbergen, G.J.; van Veghel, D.; Ter Woorst, J.; van Lieshout, D.; Dekker, L. IMPROV-ED trial: eHealth programme for faster recovery and reduced healthcare utilisation after CABG. Neth. Heart J. 2021, 29, 80–87. [Google Scholar] [CrossRef]
- Vasankari, V.; Halonen, J.; Husu, P.; Vähä-Ypyä, H.; Tokola, K.; Suni, J.; Sievänen, H.; Anttila, V.; Airaksinen, J.; Vasankari, T.; et al. Personalised eHealth intervention to increase physical activity and reduce sedentary behaviour in rehabilitation after cardiac operations: Study protocol for the PACO randomised controlled trial (NCT03470246). BMJ Open Sport Exerc. Med. 2019, 5, e000539. [Google Scholar] [CrossRef]
- Widmer, R.J.; Allison, T.G.; Lerman, L.O.; Lerman, A. Digital Health Intervention as an Adjunct to Cardiac Rehabilitation Reduces Cardiovascular Risk Factors and Rehospitalizations. J. Cardiovasc. Transl. Res. 2015, 8, 283–292. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.; Liu, C.; Du, J.; Liu, H.; Zhang, H.; Zhao, Y.; Yang, L.; Li, X.; Li, J.; Wang, J.; et al. Smartphone-based application to improve medication adherence in patients after surgical coronary revascularization. Am. Heart J. 2020, 228, 17–26. [Google Scholar] [CrossRef]
- Venkatraman, V.; Ponder, M.; Gellad, Z.F.; Lad, S.P.; Christy, E.; Plichta, R.; Harrison, J.K.; Hughes, G.C.; Doberne, J. Feasibility study of a novel digital health platform for patients undergoing transcatheter aortic valve replacement. J. Card. Surg. 2022, 37, 2017–2022. [Google Scholar] [CrossRef]
- Venkatraman, V.; Lad, S.P.; Gellad, Z.F.; Heo, H.; Wu, K.A.; Dharmapurikar, R.; Liu, B.; Jung, S.-H.; Plichta, R.; Harrison, J.K.; et al. Improving Patient Outcomes with a Mobile Digital Health Platform for Patients Undergoing Transcatheter Aortic Valve Replacement (TAVR). J. Invasive Cardiol. 2023, 35. Available online: https://www.hmpgloballearningnetwork.com/site/jic/original-contribution/improving-patient-outcomes-mobile-digital-health-platform-patients (accessed on 25 August 2023).
- Selimen, D.; Andsoy, I.I. The importance of a holistic approach during the perioperative period. Aorn. J. 2011, 93, 482–487; quiz 488–490. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Miguel-Cruz, A. Technology adoption and diffusion in healthcare at onset of COVID-19 and beyond. Healthc. Manag. Forum. 2022, 35, 161–167. [Google Scholar] [CrossRef]
- Gentili, A.; Failla, G.; Melnyk, A.; Puleo, V.; Tanna, G.L.D.; Ricciardi, W.; Cascini, F. The cost-effectiveness of digital health interventions: A systematic review of the literature. Front. Public Health 2022, 10, 787135. [Google Scholar] [CrossRef] [PubMed]
- Quisel, T.; Foschini, L.; Zbikowski, S.M.; Juusola, J.L. The Association between Medication Adherence for Chronic Conditions and Digital Health Activity Tracking: Retrospective Analysis. J. Med. Internet Res. 2019, 21, e11486. [Google Scholar] [CrossRef] [PubMed]
- Mair, V.; Breda, A.P.; Nunes, M.E.; Matos, L.D. Evaluating compliance to a cardiac rehabilitation program in a private general hospital. Einstein 2013, 11, 278–284. [Google Scholar] [CrossRef]
- Hoogma, D.F.; Croonen, R.; Al Tmimi, L.; Tournoy, J.; Verbrugghe, P.; Fieuws, S.; Rex, S. Association between improved compliance with enhanced recovery after cardiac surgery guidelines and postoperative outcomes: A retrospective study. J. Thorac. Cardiovasc. Surg. 2022. [Google Scholar] [CrossRef]
- Marston, H.R.; Musselwhite, C.B.A. Improving Older People’s Lives Through Digital Technology and Practices. Gerontol. Geriatr. Med. 2021, 7, 23337214211036255. [Google Scholar] [CrossRef]
- Abernethy, A.; Adams, L.; Barrett, M.; Bechtel, C.; Brennan, P.; Butte, A.; Faulkner, J.; Fontaine, E.; Friedhoff, S.; Halamka, J.; et al. The Promise of Digital Health: Then, Now, and the Future. NAM Perspect 2022, 2022. [Google Scholar] [CrossRef]
- Alharbi, F. The Use of Digital Healthcare Platforms During the COVID-19 Pandemic: The Consumer Perspective. Acta. Inform. Med. 2021, 29, 51–58. [Google Scholar] [CrossRef]
- Krishnaswami, A.; Beavers, C.; Dorsch, M.P.; Dodson, J.A.; Masterson Creber, R.; Kitsiou, S.; Goyal, P.; Maurer, M.S.; Wenger, N.K.; Croy, D.S.; et al. Gerotechnology for Older Adults with Cardiovascular Diseases: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 76, 2650–2670. [Google Scholar] [CrossRef]


{kind=link}
| Study | Year | Study Design | Surgery Type | Study Population | Total Number of Enrolled or Analyzed | Intervention Name | Country |
|---|---|---|---|---|---|---|---|
| Application | |||||||
| Venkatraman 2022 [41] | 2022 | Cohort study | TAVR | Adult patients undergoing TAVR | 69 | ManageMySurgery (MMS) | USA |
| Gomis-Pastor 2021 [30] | 2021 | RCT | Heart transplant | Post Heart Transplant | 134 | mHeart | Spain |
| Ben-Ali 2021 [27] | 2021 | Cohort study | elective cardiac surgery | Adult patients | 1108 | SeamlessMD | Canada |
| Cook 2014 [28] | 2014 | Cohort study | elective cardiac surgery | Over 50 | 149 | MayoClinicHealthConnection | USA |
| Snoek 2021 [35] | 2021 | RCT | PCI | Patients 65 years or older who declined participation in center-based cardiac rehabilitation | 179 | Unnamed | 5 European Countries |
| van Steenbergen 2021 [37] | 2021 | RCT | coronary artery bypass | 280 | Unnamed | The Netherlands | |
| Lunde 2020 [31] | 2020 | RCT | N/A | Cardiac Rehab | 113 | Unnamed | Norway |
| Yu 2020 [40] | 2020 | RCT | CABG | 18 years of age or older, had been prescribed at least one secondary preventive oral medication within 2 weeks after surgery | 1000 | Heart Health Application | China |
| Vasankari 2019 [38] | 2019 | RCT | coronary artery bypass, valve replacement | Adult patient doing elective surgery | 540 | ExSed | Finland |
| Spindler 2019 [36] | 2019 | RCT | PCI | 18 years of age or above, a diagnosis of coronary artery bypass, valve surgery, heart failure or artery sclerosis, ability to understand Danish, and ability to use digital technology | 136 | Teledialog | Denmark |
| Schuuring 2016 [34] | 2016 | Cohort study | N/A | Congenital Heart Disease | 118 | Web-Based | The Netherlands |
| Widmer 2015 [39] | 2015 | RCT | PCI | Post Percutaneous Coronary Intervention (PCI) | 42 | personal health assistant | USA |
| Martorella 2012 [32] | 2012 | RCT | cardiac surgery requiring sternotomy | First surgery | 60 | Soulage Tavie | Canada |
| Web-Based | |||||||
| Melholt 2018 [33] | 2018 | Cohort study | N/A | Patients with ischemic heart disease or CHF | 49 | Active Heart | Norway |
| Dew 2004 [29] | 2004 | nonrandomized trial | Heart transplant | Patients post heart transplant | 64 | Heartnet | USA |
| Nonrandomized Cohort Studies | |||||||||
| MINORS | Venkatraman 2022 [41] | Melholt 2018 [33] | Schuuring 2016 [34] | Ben-Ali 2021 [27] | Cook 2014 [28] | Dew 2004 [29] | |||
| A clearly stated aim | 1 | 2 | 1 | 2 | 2 | 1 | |||
| Inclusion of consecutive patients | 2 | 1 | 1 | 2 | 2 | 2 | |||
| Prospective collection of data | 2 | 2 | 2 | 2 | 2 | 2 | |||
| Endpoints appropriate to the aim of the study | 2 | 2 | 2 | 2 | 2 | 2 | |||
| Unbiased assessment of study endpoint | 2 | 2 | 2 | 2 | 2 | 2 | |||
| Follow-up period appropriate to the aim of the study | 2 | 2 | 2 | 2 | 2 | 2 | |||
| Loss to follow up less than 5% | 0 | 0 | 2 | 0 | 0 | 2 | |||
| Prospective calculation of the study size | 2 | 2 | 2 | 1 | 1 | 2 | |||
| Total | 13 | 13 | 14 | 13 | 13 | 15 | |||
| Randomized Control Trials | |||||||||
| Joanna Briggs Institute critical appraisal | Gomis-Pastor 2021 [30] | van Steenbergen 2021 [37] | Snoek 2021 [35] | Lunde 2020 [31] | Yu 2020 [40] | Spindler 2019 [36] | Vasankari 2019 [38] | Widmer 2015 [39] | Martorella 2012 [32] |
| Were the two groups similar and recruited from the same population? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Were the exposures measured similarly to assign people to both exposed and unexposed groups? | Yes | Yes | Yes | Yes | Yes | Yes | Not Reported | Yes | Yes |
| Was the exposure measured in a valid and reliable way? | Yes | Not Reported | Yes | Yes | Yes | Yes | Not Reported | Yes | Yes |
| Were strategies to deal with confounding factors stated? | Not Reported | Not Reported | Not Reported | Not Reported | Yes | No | Not Reported | Yes | No |
| Were the groups/participants free of the outcome at the start of the study (or at the moment of exposure)? | Yes | Not Reported | Yes | Yes | Yes | Yes | Not Reported | Yes | Yes |
| Were the outcomes measured in a valid and reliable way? | Yes | Not Reported | Yes | Yes | Yes | Yes | Not Reported | Yes | Yes |
| Was the follow-up time reported and sufficient to be long enough for outcomes to occur? | No | Not Reported | No | No | No | No | Not Reported | No | No |
| Was follow-up complete, and if not, were the reasons for the loss to follow up described and explored? | Yes | Not Reported | Yes | Yes | No | Not Reported | Not Reported | Yes | Yes |
| Were strategies to address incomplete follow-up utilized? | Not Reported | Not Reported | Yes | Yes | Yes | Yes | Not Reported | Yes | Yes |
| Was appropriate statistical analysis used? | Yes | Yes | Yes | Yes | Yes | Yes | Not Reported | Yes | Yes |
| Study | Intervention Name | Primary Objective | Secondary Objective | Primary Results | Secondary Results |
|---|---|---|---|---|---|
| Gomis-Pastor 2021 [30] | mHeart | medication adherence | medical knowledge | intervention improved med compliance | intervention increased knowledge about meds |
| van Steenbergen 2021 [37] | Unnamed | healthcare utilization | quality of life | reduced healthcare utilization | by improving quality of life, decreasing anxiety, and accelerating recovery |
| Snoek 2021 [35] | Unnamed | peak oxygen uptake (VO2peak) after 6 months | change in the amount of self-reported habitual physical activity was greater | peak oxygen uptake improved in the study group at 6 and 12 months | change in the amount of self-reported habitual physical activity was greater in the study group compared with the control group |
| Lunde 2020 [31] | unnamed | VO2, exercise performance | lipid panel | intervention increased VO2, exercise performance | intervention had no impact on lipid panel |
| Yu 2020 [40] | Heart Health Application | CABG secondary preventive medication adherence as measured by the MMAS-8 at the 6-month visit after randomization | secondary outcomes were mortality, major adverse cardiovascular and cerebrovascular events, cardiovascular rehospitalizations, self-reported secondary preventive medication use after 6-month follow-up, BP, BMI and self-reported smoking status | there were no significant differences in the primary outcome | there were no significant differences in the secondary clinical outcome measures |
| Spindler 2019 [36] | Teledialog | level of anxiety and depressive symptoms | quality of life experienced by patients | no significant differences between the two rehabilitation groups with regard to the level of anxiety and depressive symptoms | no significant differences between the two rehabilitation groups with regard to quality of life experienced by patients |
| Vasankari 2019 [38] | ExSed | the change in mean daily step count between the baseline (preoperatively) and at 3 months from hospital discharge | improvement in self-perceived QoL | ||
| Widmer 2015 [39] | personal health assistant | changes in risk factors | rehospitalizations plus emergency department (ED) visits | significant reductions in weight and blood pressure | significant reductions in rehospitalizations/ED visits |
| Martorella 2012 [32] | Soulage Tavie | pain intensity, pain interference with daily activities, patients’ pain barriers, tendency to catastrophize in face of pain, and analgesic consumption | intervention group had less pain interference with breathing | intervention group consumed more opioid pain meds |
| Study | Intervention Name | Primary Objective | Secondary Objective | Primary Results | Secondary Results |
|---|---|---|---|---|---|
| Venkatraman 2022 [41] | ManageMySurgery (MMS) | user satisfaction | 73% of users found the application helpful | ||
| Ben-Ali 2021 [27] | SeamlessMD | user satisfaction | reduction in health service utilization | 94% of patients were satisfied with the app | 45% of patients used the app to avoid a phone call and 28% used the app to avoid a hospital visit |
| Melholt 2018 [33] | Active Heart | patient satisfaction, literacy skills | patients were satisfied with app and had self-reported improved literacy | ||
| Schuuring 2016 [34] | mHealth | use of mHealth, desire to use mHealth | only a minority of patients already used mHealth tools, but a majority would want to try | desire to use mHealth was not impacted by patients age | |
| Cook 2014 [28] | MayoClinicHealthConnection | use by age category | age did not have a significant effect on app use | ||
| Dew 2004 [29] | Heartnet | mental health, QoL, compliance | intervention reduced anxiety, depression and increased social QoL |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, K.A.; Kunte, S.; Rajkumar, S.; Venkatraman, V.; Kim, G.; Kaplan, S.; Anwar-Hashmi, S.O.; Doberne, J.; Nguyen, T.C.; Lad, S.P. Digital Health for Patients Undergoing Cardiac Surgery: A Systematic Review. Healthcare 2023, 11, 2411. https://doi.org/10.3390/healthcare11172411
Wu KA, Kunte S, Rajkumar S, Venkatraman V, Kim G, Kaplan S, Anwar-Hashmi SO, Doberne J, Nguyen TC, Lad SP. Digital Health for Patients Undergoing Cardiac Surgery: A Systematic Review. Healthcare. 2023; 11(17):2411. https://doi.org/10.3390/healthcare11172411
Chicago/Turabian StyleWu, Kevin A., Sameer Kunte, Shashank Rajkumar, Vishal Venkatraman, Grace Kim, Samantha Kaplan, Syed Omar Anwar-Hashmi, Julie Doberne, Tom C. Nguyen, and Shivanand P. Lad. 2023. "Digital Health for Patients Undergoing Cardiac Surgery: A Systematic Review" Healthcare 11, no. 17: 2411. https://doi.org/10.3390/healthcare11172411