
Effect of Physiotherapy Treatment with Immersive Virtual Reality in Subjects with Stroke: A Protocol for a Randomized Controlled Trial
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
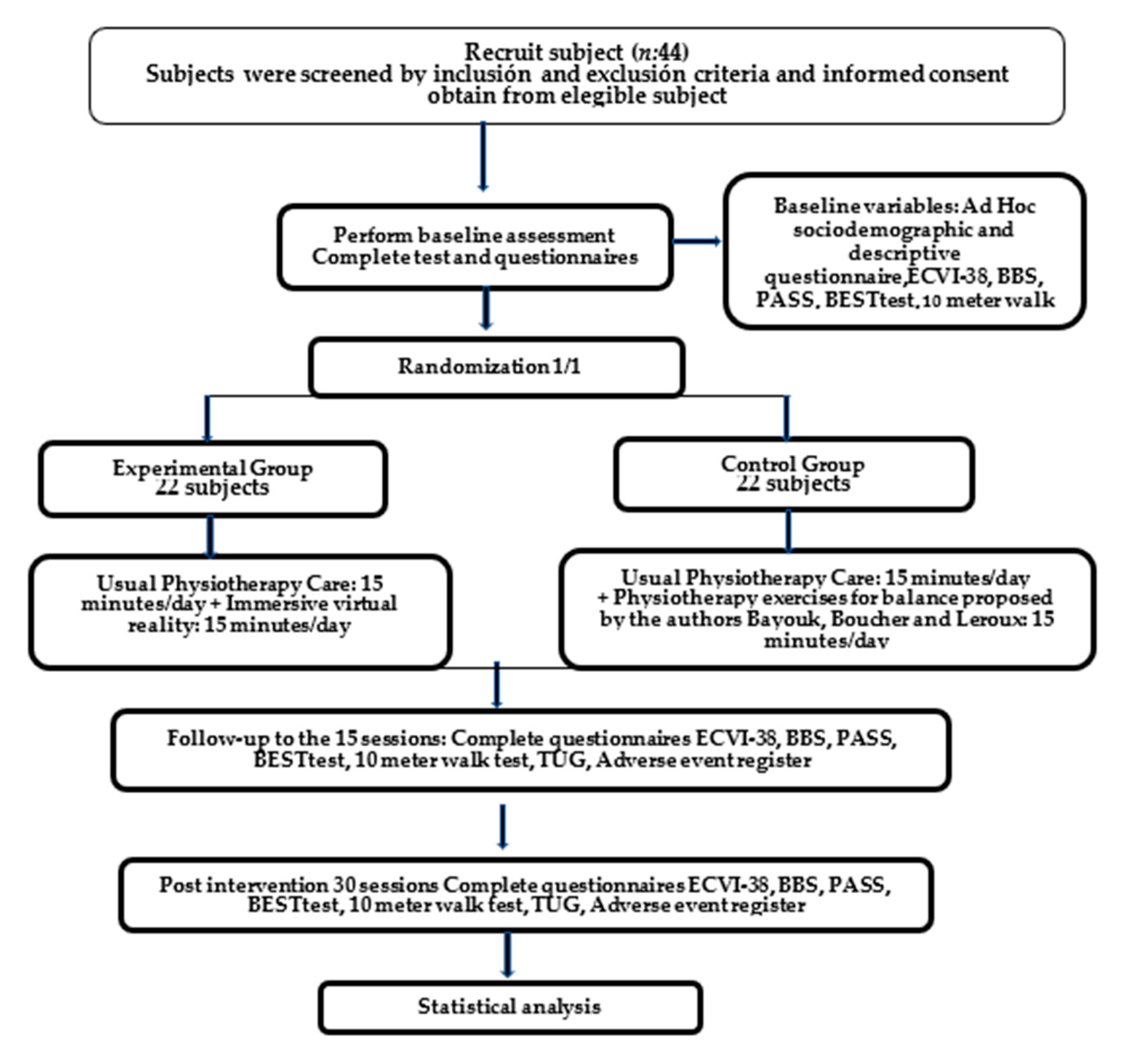
2.1. Study Design and Setting
2.2. Participants
2.3. Randomization of Subjects
2.4. Intervention Protocol/Procedure
2.5. Physiotherapists Training
2.6. Intervention
- -
- Stretching exercises lasting 30 s each, with a maximum duration of 5 min;
- -
- Joint mobilization exercises of the hip, knee and ankle of both lower extremities, which will be carried out passively and with a total duration of 5 min;
- -
- Exercises for the active mobilization of the spine (flexion, extension, turning, etc.) with a maximum duration of 5 min.
2.7. Outcomes
2.8. Participant Timeline
2.9. Blinding
2.10. Data Collection Methods
2.11. Data Management and Statistical Analysis
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alvarez-Sabín, J.; Quintana, M.; Masjuan, J.; Oliva-Moreno, J.; Mar, J.; Gonzalez-Rojas, N.; Becerra, V.; Torres, C.; Yebenes, M. Economic Impact of Patients Admitted to Stroke Units in Spain. Eur. J. Health Econ. 2017, 18, 449–458. [Google Scholar] [CrossRef] [PubMed]
- Go, A.S.; Mozaffarian, D.; Roger, V.L.; Benjamin, E.J.; Berry, J.D.; Borden, W.B.; Bravata, D.M.; Dai, S.; Ford, E.S.; Fox, C.S.; et al. Heart Disease and Stroke Statistics—2013 Update: A Report from the American Heart Association. Circulation 2013, 127, e6–e245. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Stark, B.A.; Johnson, C.O.; Roth, G.A.; Bisignano, C.; Abady, G.G.; Abbasifard, M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abedi, V.; et al. Global, Regional, and National Burden of Stroke and Its Risk Factors, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Westlake, K.P.; Nagarajan, S.S. Functional Connectivity in Relation to Motor Performance and Recovery after Stroke. Front. Syst. Neurosci. 2011, 5, 8. [Google Scholar] [CrossRef]
- Xu, T.; Clemson, L.; O’Loughlin, K.L.; Lannin, N.; Dean, C.; Koh, G. Risk Factors for Falls in Community Stroke Survivors: A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2018, 99, 563–573. [Google Scholar] [CrossRef]
- Hun Jang, S.; Lee, J.-H.H.; Jang, S.H.; Lee, J.-H.H. Impact of Sensory Integration Training on Balance among Stroke Patients: Sensory Integration Training on Balance among Stroke Patients. Open. Med. 2016, 11, 330–335. [Google Scholar] [CrossRef] [PubMed]
- Campfens, S.F.; Zandvliet, S.B.; Meskers, C.G.M.; Schouten, A.C.; van Putten, M.J.A.M.; van der Kooij, H. Poor Motor Function Is Associated with Reduced Sensory Processing after Stroke. Exp. Brain Res. 2015, 233, 1339–1349. [Google Scholar] [CrossRef]
- Li, S.; Hummel, F.C.; Yue, G.H.; Li, S. Spasticity, Motor Recovery, and Neural Plasticity after Stroke. Front. Neurol. 2017, 3, 120. [Google Scholar] [CrossRef]
- Daly, J.J.; Ruff, R.L. Construction of Efficacious Gait and Upper Limb Functional Interventions Based on Brain Plasticity Evidence and Model-Based Measures For Stroke Patients. Sci. World J. 2007, 7, 2031–2045. [Google Scholar] [CrossRef]
- Kleim, J.A. Neural Plasticity and Neurorehabilitation: Teaching the New Brain Old Tricks. J. Commun. Disord. 2011, 44, 521–528. [Google Scholar] [CrossRef]
- Kleim, J.A.; Jones, T.A. Principles of Experience-Dependent Neural Plasticity: Implications for Rehabilitation after Brain Damage. J. Speech Lang. Hear. Res. 2008, 51, S225. [Google Scholar] [CrossRef] [PubMed]
- de Rooij, I.J.M.M.; van de Port, I.G.L.L.; Meijer, J.-W.W.G. Effect of Virtual Reality Training on Balance and Gait Ability in Patients With Stroke: Systematic Review and Meta-Analysis. Phys. Ther. 2016, 96, 1905–1918. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Lo, W.L.A.; Mao, Y.R.; Ding, M.H.; Lin, Q.; Li, H.; Zhao, J.L.; Xu, Z.Q.; Bian, R.H.; Huang, D.F.; et al. Effect of Virtual Reality on Postural and Balance Control in Patients with Stroke: A Systematic Literature Review. Biomed. Res. Int. 2016, 2016, 7309272. [Google Scholar] [CrossRef] [PubMed]
- Lloréns, R.; Noé, E.; Colomer, C.; Alcañiz, M. Effectiveness, Usability, and Cost-Benefit of a Virtual Reality-Based Telerehabilitation Program for Balance Recovery after Stroke: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2015, 96, 418–425.e2. [Google Scholar] [CrossRef]
- Laver, K.E.; Lange, B.; George, S.; Deutsch, J.E.; Saposnik, G.; Crotty, M. Virtual Reality for Stroke Rehabilitation. Stroke 2017, 11, CD008349. [Google Scholar] [CrossRef]
- Cho, S.; Ku, J.; Cho, Y.K.; Kim, I.Y.; Kang, Y.J.; Jang, D.P.; Kim, S.I. Development of Virtual Reality Proprioceptive Rehabilitation System for Stroke Patients. Comput. Methods Programs Biomed. 2014, 113, 258–265. [Google Scholar] [CrossRef]
- Yasuda, K.; Muroi, D.; Ohira, M.; Iwata, H. Validation of an Immersive Virtual Reality System for Training near and Far Space Neglect in Individuals with Stroke: A Pilot Study. Top. Stroke Rehabil. 2017, 24, 533–538. [Google Scholar] [CrossRef]
- Garay-Sánchez, A.; Suarez-Serrano, C.; Ferrando-Margelí, M.; Jimenez-Rejano, J.J.; Marcén-Román, Y. Effects of Immersive and Non-Immersive Virtual Reality on the Static and Dynamic Balance of Stroke Patients: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 4473. [Google Scholar] [CrossRef]
- Cho, K.H.; Lee, W.H. Effect of Treadmill Training Based Real-World Video Recording on Balance and Gait in Chronic Stroke Patients: A Randomized Controlled Trial. Gait Posture 2014, 39, 523–528. [Google Scholar] [CrossRef]
- Kim, N.; Park, Y.; Lee, B.H. Effects of Community-Based Virtual Reality Treadmill Training on Balance Ability in Patients with Chronic Stroke. J. Phys. Ther. Sci. 2015, 27, 655–658. [Google Scholar] [CrossRef]
- Cortés-Pérez, I.; Nieto-Escamez, F.A.; Obrero-Gaitán, E. Immersive Virtual Reality in Stroke Patients as a New Approach for Reducing Postural Disabilities and Falls Risk: A Case Series. Brain Sci. 2020, 10, 296. [Google Scholar] [CrossRef] [PubMed]
- Huygelier, H.; Mattheus, E.; Vanden Abeele, V.; Van Ee, R.; Gillebert, C.R. The Use of the Term Virtual Reality in Post-Stroke Rehabilitation: A Scoping Review and Commentary. Psychol. Belg. 2021, 61, 145–162. [Google Scholar] [CrossRef] [PubMed]
- Sherman, W.; Craig, A. Understanding Virtual Reality, 2nd ed.; Morgan Kaufmann: Burlington, MA, USA, 2018; Available online: https://www.elsevier.com/books/understanding-virtual-reality/sherman/978-0-12-800965-9 (accessed on 24 April 2023).
- Lange, B.; Koenig, S.; Chang, C.; McConnell, E.; Suma, E.; Bolas, M.; Rizzo, A. Designing Informed Game-Based Rehabilitation Tasks Leveraging Advances in Virtual Reality. Disabil. Rehabil. 2012, 34, 1863–1870. [Google Scholar] [CrossRef] [PubMed]
- De Luca, R.; Torrisi, M.; Piccolo, A.; Bonfiglio, G.; Tomasello, P.; Naro, A.; Calabrò, R. Improving Post-Stroke Cognitive and Behavioral Abnormalities by Using Virtual Reality: A Case Report on a Novel Use of Nirvana. Appl. Neuropsychol. Adult 2018, 25, 581–585. [Google Scholar] [CrossRef]
- Schiza, E.; Matsangidou, M.; Neokleous, K.; Pattichis, C.S. Virtual Reality Applications for Neurological Disease: A Review. Front. Robot. AI 2019, 6, 100. [Google Scholar] [CrossRef]
- Høeg, E.R.; Povlsen, T.M.; Bruun-Pedersen, J.R.; Lange, B.; Nilsson, N.C.; Haugaard, K.B.; Faber, S.M.; Hansen, S.W.; Kimby, C.K.; Serafin, S. System Immersion in Virtual Reality-Based Rehabilitation of Motor Function in Older Adults: A Systematic Review and Meta-Analysis. Front. Virtual Real. 2021, 2, 647993. [Google Scholar] [CrossRef]
- Kim, A.; Darakjian, N.; Finley, J.M. Walking in Fully Immersive Virtual Environments: An Evaluation of Potential Adverse Effects in Older Adults and Individuals with Parkinson’s Disease. J. Neuroeng. Rehabil. 2017, 14, 16. [Google Scholar] [CrossRef]
- Ozkul, C.; Guclu-Gunduz, A.; Yazici, G.; Atalay Guzel, N.; Irkec, C. Effect of Immersive Virtual Reality on Balance, Mobility, and Fatigue in Patients with Multiple Sclerosis: A Single-Blinded Randomized Controlled Trial. Eur. J. Integr. Med. 2020, 35, 101092. [Google Scholar] [CrossRef]
- Bauer, A.C.M.; Andringa, G. The Potential of Immersive Virtual Reality for Cognitive Training in Elderly. Gerontology 2020, 66, 614–623. [Google Scholar] [CrossRef]
- Lima Rebêlo, F.; de Souza Silva, L.F.; Doná, F.; Sales Barreto, A.; de Souza Siqueira Quintans, J. Immersive Virtual Reality Is Effective in the Rehabilitation of Older Adults with Balance Disorders: A Randomized Clinical Trial. Exp. Gerontol. 2021, 149, 111308. [Google Scholar] [CrossRef]
- Muhla, F.; Clanché, F.; Duclos, K.; Meyer, P.; Maïaux, S.; Colnat-Coulbois, S.; Gauchard, G.C. Impact of Using Immersive Virtual Reality over Time and Steps in the Timed Up and Go Test in Elderly People. PLoS ONE 2020, 15, e0229594. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Bang, M.; Krivonos, D.; Schimek, H.; Naval, A. An Immersive Virtual Reality Exergame for People with Parkinson’s Disease. In Computers Helping People with Special Needs; Springer Science and Business Media Deutschland GmbH: Cham, Switzerland, 2020; Volume 12376, pp. 138–145. [Google Scholar]
- Lheureux, A.; Lebleu, J.; Frisque, C.; Sion, C.; Stoquart, G.; Warlop, T.; Detrembleur, C.; Lejeune, T. Immersive Virtual Reality to Restore Natural Long-Range Autocorrelations in Parkinson’s Disease Patients’ Gait During Treadmill Walking. Front. Physiol. 2020, 11, 572063. [Google Scholar] [CrossRef]
- Morales-Gómez, S.; Elizagaray-García, I.; Yepes-Rojas, Ó.; de la Puente-Ranea, L.; Gil-Martínez, A. Effectiveness of Virtual Immersion Programmes in Patients with Parkinson’s Disease. A Systematic Review. Rev. Neurol. 2018, 66, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Peruzzi, A.; Cereatti, A.; della Croce, U.; Mirelman, A. Effects of a Virtual Reality and Treadmill Training on Gait of Subjects with Multiple Sclerosis: A Pilot Study. Mult. Scler. Relat. Disord. 2016, 5, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Huygelier, H.; Schraepen, B.; Lafosse, C.; Vaes, N.; Schillebeeckx, F.; Michiels, K.; Note, E.; Vanden Abeele, V.; van Ee, R.; Gillebert, C.R. An Immersive Virtual Reality Game to Train Spatial Attention Orientation after Stroke: A Feasibility Study. Appl. Neuropsychol. Adult 2022, 29, 915–935. [Google Scholar] [CrossRef]
- Mekbib, D.B.; Debeli, D.K.; Zhang, L.; Fang, S.; Shao, Y.; Yang, W.; Han, J.; Jiang, H.; Zhu, J.; Zhao, Z.; et al. A Novel Fully Immersive Virtual Reality Environment for Upper Extremity Rehabilitation in Patients with Stroke. Ann. N. Y. Acad. Sci. 2021, 1493, 75–89. [Google Scholar] [CrossRef]
- Bayouk, J.-F.; Boucher, J.P.; Leroux, A. Balance Training Following Stroke: Effects of Task-Oriented Exercises with and without Altered Sensory Input. Int. J. Rehabil. Res. 2006, 29, 51–59. [Google Scholar] [CrossRef]
- Chan, A.-W.; Tetzlaff, J.M.; Altman, D.G.; Laupacis, A.; Gøtzsche, P.C.; Krleža-Jerić, K.; Hróbjartsson, A.; Mann, H.; Dickersin, K.; Berlin, J.A.; et al. SPIRIT 2013 Statement: Defining Standard Protocol Items for Clinical Trials. Ann. Intern. Med. 2013, 158, 200–207. [Google Scholar] [CrossRef]
- Downs, S. The Berg Balance Scale. J. Physiother. 2015, 61, 46. [Google Scholar] [CrossRef]
- Romero, M.; Sánchez, A.; Marín, C.; Navarro, M.D.; Ferri, J.; Noé, E. Clinical Usefulness of the Spanish Version of the Mississippi Aphasia Screening Test (MASTsp): Validation in Stroke Patients. Neurologia 2012, 27, 216–224. [Google Scholar] [CrossRef]
- Arevalo-Rodriguez, I.; Smailagic, N.; Roqué-Figuls, M.; Ciapponi, A.; Sanchez-Perez, E.; Giannakou, A.; Pedraza, O.; Bonfill Cosp, X.; Cullum, S. Mini-Mental State Examination (MMSE) for the Early Detection of Dementia in People with Mild Cognitive Impairment (MCI). Cochrane Database Syst. Rev. 2021, 7, CD010783. [Google Scholar] [PubMed]
- Bonan, I.V.; Yelnik, A.P.; Colle, F.M.; Michaud, C.; Normand, E.; Panigot, B.; Roth, P.; Guichard, J.P.; Vicaut, E. Reliance on Visual Information after Stroke. Part II: Effectiveness of a Balance Rehabilitation Program with Visual Cue Deprivation after Stroke: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2004, 85, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Cabanas-Valdés, R.; Girabent-Farrés, M.; Cánovas-Vergé, D.; Caballero-Gómez, F.M.; Germán-Romero, A.; Bagur-Calafat, C. Spanish Translation and Validation of the Postural Assessment Scale for Stroke Patients (PASS) to Assess Balance and Postural Control in Adult Post-Stroke Patients. Rev. Neurol. 2015, 60, 151–158. [Google Scholar]
- Horak, F.B.; Wrisley, D.M.; Frank, J. The Balance Evaluation Systems Test (BESTest) to Differentiate Balance Deficits. Phys. Ther. 2009, 89, 484–498. [Google Scholar] [CrossRef] [PubMed]
- Chien, C.W.; Hu, M.H.; Tang, P.F.; Sheu, C.F.; Hsieh, C.L. A Comparison of Psychometric Properties of the Smart Balance Master System and the Postural Assessment Scale for Stroke in People Who Have Had Mild Stroke. Arch. Phys. Med. Rehabil. 2007, 88, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Hsueh, L.P.; Chen, K.L.; Chou, Y.T.; Wang, Y.H.; Hsieh, C.L. Individual-Level Responsiveness of the Original and Short-Form Postural Assessment Scale for Stroke Patients. Phys. Ther. 2013, 93, 1377–1382. [Google Scholar] [CrossRef]
- Liaw, L.J.; Hsieh, C.L.; Lo, S.K.; Chen, H.M.; Lee, S.; Lin, J.H. The Relative and Absolute Reliability of Two Balance Performance Measures in Chronic Stroke Patients. Disabil. Rehabil. 2008, 30, 656–661. [Google Scholar] [CrossRef] [PubMed]
- Chinsongkram, B.; Chaikeeree, N.; Saengsirisuwan, V.; Viriyatharakij, N.; Horak, F.B.; Boonsinsukh, R. Reliability and Validity of the Balance Evaluation Systems Test (BESTest) in People With Subacute Stroke. Phys. Ther. 2014, 94, 1632–1643. [Google Scholar] [CrossRef] [PubMed]
- Chan, P.P.; Si Tou, J.I.; Tse, M.M.; Ng, S.S. Reliability and Validity of the Timed Up and Go Test With a Motor Task in People With Chronic Stroke. Arch. Phys. Med. Rehabil. 2017, 98, 2213–2220. [Google Scholar] [CrossRef]
- Perera, S.; Mody, S.H.; Woodman, R.C.; Studenski, S.A. Meaningful Change and Responsiveness in Common Physical Performance Measures in Older Adults. J. Am. Geriatr. Soc. 2006, 54, 743–749. [Google Scholar] [CrossRef]
- Flansbjer, U.B.; Holmbäck, A.M.; Downham, D.; Patten, C.; Lexell, J. Reliability of Gait Performance Tests in Men and Women with Hemiparesis after Stroke. J. Rehabil. Med. 2005, 37, 75–82. [Google Scholar] [CrossRef]
- Fernández-Concepción, O.; Ramírez-Pérez, E.; Alvarez, M.A.; Buergo-Zuáznabar, M.A. Validation of the Stroke-Specific Quality of Life Scale (ECVI-38). Rev. Neurol. 2008, 46, 147–152. [Google Scholar] [PubMed]
- Tefertiller, C.; Hays, K.; Natale, A.; O’Dell, D.; Ketchum, J.; Sevigny, M.; Eagye, C.B.; Philippus, A.; Harrison-Felix, C. Results From a Randomized Controlled Trial to Address Balance Deficits After Traumatic Brain Injury. Arch. Phys. Med. Rehabil. 2019, 100, 1409–1416. [Google Scholar] [CrossRef] [PubMed]
- Bambirra, C.; Rodrigues, M.; Faria, C.; De Paula, F.R. Clinical Evaluation of Balance in Hemiparetic Adults: A Systematic Review. Fisioter. Em Mov. 2015, 28, 187–200. [Google Scholar] [CrossRef]
- Hwang, H.S.; Kim, J.H.; Choi, B.R. Comparison of the Effects of Visual Feedback Training and Unstable Surface Training on Static and Dynamic Balance in Patients with Stroke. J. Phys. Ther. Sci. 2017, 29, 1720–1722. [Google Scholar] [CrossRef]
- Cho, H.Y.; Kim, K. Effects of Action Observation Training with Auditory Stimulation on Static and Dynamic Balance in Chronic Stroke Patients. J. Stroke Cerebrovasc. Dis. 2020, 29, 104775. [Google Scholar] [CrossRef]
- Lee, M.; Son, J.; Kim, J.; Pyun, S.B.; Eun, S.D.; Yoon, B.C. Comparison of Individualized Virtual Reality- and Group-Based Rehabilitation in Older Adults with Chronic Stroke in Community Settings: A Pilot Randomized Controlled Trial. Eur. J. Integr. Med. 2016, 8, 738–746. [Google Scholar] [CrossRef]
- Lloréns, R.; Gil-Gómez, J.A.; Alcañiz, M.; Colomer, C.; Noé, E. Improvement in Balance Using a Virtual Reality-Based Stepping Exercise: A Randomized Controlled Trial Involving Individuals with Chronic Stroke. Clin. Rehabil. 2015, 29, 261–268. [Google Scholar] [CrossRef] [PubMed]
- McEwen, D.; Taillon-Hobson, A.; Bilodeau, M.; Sveistrup, H.; Finestone, H. Virtual Reality Exercise Improves Mobility after Stroke: An Inpatient Randomized Controlled Trial. Stroke 2014, 45, 1853–1855. [Google Scholar] [CrossRef]
- Sheehy, L.; Taillon-Hobson, A.; Sveistrup, H.; Bilodeau, M.; Fergusson, D.; Levac, D.; Finestone, H. Does the Addition of Virtual Reality Training to a Standard Program of Inpatient Rehabilitation Improve Sitting Balance Ability and Function after Stroke? Protocol for a Single-Blind Randomized Controlled Trial. BMC Neurol. 2016, 16, 42. [Google Scholar] [CrossRef]
- Viñas-Diz, S.; Sobrido-Prieto, M. Virtual Reality for Therapeutic Purposes in Stroke: A Systematic Review. Neurologia 2016, 31, 255–277. [Google Scholar] [CrossRef]
- Saposnik, G.; Cohen, L.G.; Mamdani, M.; Pooyania, S.; Ploughman, M.; Cheung, D.; Shaw, J.; Hall, J.; Nord, P.; Dukelow, S.; et al. Efficacy and Safety of Non-Immersive Virtual Reality Exercising in Stroke Rehabilitation (EVREST): A Randomised, Multicentre, Single-Blind, Controlled Trial. Lancet Neurol. 2016, 15, 1019–1027. [Google Scholar] [CrossRef] [PubMed]
- Ögün, M.N.; Kurul, R.; Yaşar, M.F.; Turkoglu, S.A.; Avci, Ş.; Yildiz, N. Effect of Leap Motion-Based 3D Immersive Virtual Reality Usage on Upper Extremity Function in Ischemic Stroke Patients. Arq. Neuropsiquiatr. 2019, 77, 681–688. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, K.; Buchanan, A.; Cottrell, K.; Hughes, S.; Day, T.W.; John, N.W. Immersive Virtual Reality for the Cognitive Rehabilitation of Stroke Survivors. IEEE Trans. Neural Syst. Rehabil. Eng. 2022, 30, 719–728. [Google Scholar] [CrossRef] [PubMed]
- Domínguez-Téllez, P.; Moral-Muñoz, J.A.; Casado-Fernández, E.; Salazar, A.; Lucena-Antón, D. Effects of Virtual Reality on Balance and Gait in Stroke: A Systematic Review and Meta-Analysis. Rev. Neurol. 2019, 69, 223–234. [Google Scholar] [CrossRef]
- Maggio, M.G.; Latella, D.; Maresca, G.; Sciarrone, F.; Manuli, A.; Naro, A.; de Luca, R.; Calabrò, R.S. Virtual Reality and Cognitive Rehabilitation in People With Stroke: An Overview. J. Neurosci. Nurs. 2019, 51, 101–105. [Google Scholar] [CrossRef]
- Brassel, S.; Power, E.; Campbell, A.; Brunner, M.; Togher, L. Recommendations for the Design and Implementation of Virtual Reality for Acquired Brain Injury Rehabilitation: Systematic Review. J. Med. Internet Res. 2021, 23, e26344. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Intervention Protocol | |
|---|---|
| Control Group (CG) | Intervention Group (IG) |
| 15 min: physiotherapy treatment aimed at achieving functional improvement and increased postural control [44]. | 15 min: physiotherapy treatment aimed at achieving functional improvement and increased postural control [44]. |
| 15 min: static and dynamic balance training in sitting and standing according to Bayouk, Boucher and Leroux protocol [39]. | 15 min: static and dynamic balance training in sitting and standing through Immersive VR. |
| Exercises | Repetitions | Total Time |
|---|---|---|
| Stand with feet together for 10 s. | 8 repetitions | 2 min |
| Hold the tandem posture for 10 s. | 8 repetitions | 2 min |
| Get up from the chair without using arms. | 3 sets of 8 repetitions | 3 min |
| Walk forwards and backwards with one foot in front of the other. | 5 min | |
| Stay in monopodal support for 10 s. | 10 repetitions | 3 min |
| Outcome Domain | Measures Instrument | T0 | T1 | T2 |
|---|---|---|---|---|
| Sociodemographic and descriptive data | Ad Hoc questionnaire | X | ||
| Primary outcomes | ||||
| Static balance and functional mobility | PASS | X | X | X |
| BESTtest | X | X | X | |
| Dynamic balance and gait | 10 m walk test | X | X | X |
| TUG | X | X | X | |
| Secondary outcomes | ||||
| Quality of life | ECVI-38 | X | X | X |
| Adverse effects | Open questions | X | X |
| STUDY PERIOD | |||||
|---|---|---|---|---|---|
| Enrolment | Allocation | Post-Allocation | Closeout | ||
| Time points baseline | t | 0 | t15 | t30 | tx |
| Enrollment | |||||
| Eligibility screen | X | ||||
| Informed consent | X | ||||
| Allocation | X | ||||
| Assessments | |||||
| Baseline variables | X | ||||
| Post. Intervention and follow-up variables | X | X | X | ||
| Interventions | |||||
| IVR training group | X | X | |||
| Physical therapy with Bayouk, Boucher and Leroux exercises | X | X | |||
| Sociodemographic and descriptive data | Age | Years |
|---|---|---|
| Gender | Male/female | |
| BMI | Underweight/normal weight/overweight | |
| Hypertension | Yes/no | |
| Hypercholesterolemia | Yes /no | |
| Diabetes mellitus | Yes /no | |
| Tabaco habit | Yes /no | |
| Habitual consumption of stimulants or toxic substances | Yes /no | |
| Chronic drug use | Yes /no | |
| Mississippi Aphasia Screening Score | Score | |
| Mini-mental State Examination Score | Score | |
| Days of hospitalization | Number of days |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garay-Sánchez, A.; Marcén-Román, Y.; Ferrando-Margelí, M.; Franco-Sierra, M.Á.; Suarez-Serrano, C. Effect of Physiotherapy Treatment with Immersive Virtual Reality in Subjects with Stroke: A Protocol for a Randomized Controlled Trial. Healthcare 2023, 11, 1335. https://doi.org/10.3390/healthcare11091335
Garay-Sánchez A, Marcén-Román Y, Ferrando-Margelí M, Franco-Sierra MÁ, Suarez-Serrano C. Effect of Physiotherapy Treatment with Immersive Virtual Reality in Subjects with Stroke: A Protocol for a Randomized Controlled Trial. Healthcare. 2023; 11(9):1335. https://doi.org/10.3390/healthcare11091335
Chicago/Turabian StyleGaray-Sánchez, Aitor, Yolanda Marcén-Román, Mercedes Ferrando-Margelí, M. Ángeles Franco-Sierra, and Carmen Suarez-Serrano. 2023. "Effect of Physiotherapy Treatment with Immersive Virtual Reality in Subjects with Stroke: A Protocol for a Randomized Controlled Trial" Healthcare 11, no. 9: 1335. https://doi.org/10.3390/healthcare11091335