
The Effectiveness of the Chronic Disease Self-Management Program in Improving Patients’ Self-Efficacy and Health-Related Behaviors: A Quasi-Experimental Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Participants
2.3. Measures
2.4. Translation and Readability Assessment
2.5. Procedures
2.6. Intervention Fidelity
2.7. Data Analysis
2.8. Ethical Approval
3. Results
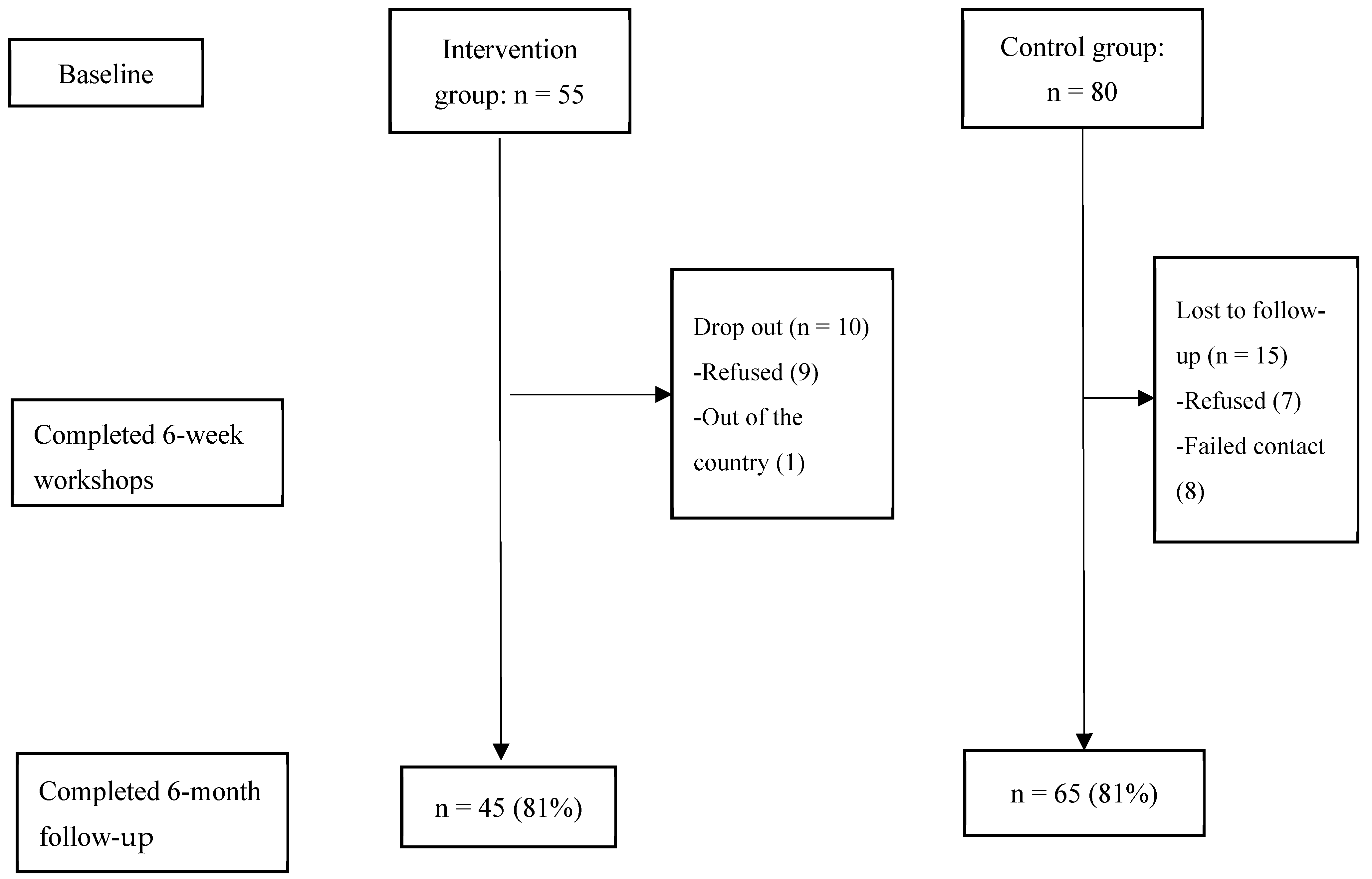
3.1. Enrollment and Demographics
3.2. Baseline Characteristics
3.3. Comparison between the Groups at 6 Months
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bahari, G. Prevalence and factors associated with psychological distress among family caregivers: A cross-sectional study. Perspect. Psychiatr. Care 2021, 57, 1960–1965. [Google Scholar] [CrossRef] [PubMed]
- Holman, H.R. The Relation of the Chronic Disease Epidemic to the Health Care Crisis. ACR Open Rheumatol. 2020, 2, 167–173. [Google Scholar] [CrossRef] [PubMed]
- AlQuaiz, A.M.; Kazi, A.; Almigbal, T.H.; AlHazmi, A.M.; Qureshi, R.; AlHabeeb, K.M. Factors Associated with an Unhealthy Lifestyle among Adults in Riyadh City, Saudi Arabia. Healthcare 2021, 9, 221. [Google Scholar] [CrossRef] [PubMed]
- Airhihenbuwa, C.O.; Tseng, T.-S.; Sutton, V.D.; Price, L. Global Perspectives on Improving Chronic Disease Prevention and Management in Diverse Settings. Prev. Chronic Dis. 2021, 18, E33. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.B.; Hashim, M.J.; King, J.K.; Govender, R.D.; Mustafa, H.; Al Kaabi, J. Epidemiology of Type 2 Diabetes–Global Burden of Disease and Forecasted Trends. J. Epidemiol. Glob. Health 2020, 10, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Mills, K.T.; Stefanescu, A.; He, J. The global epidemiology of hypertension. Nat. Rev. Nephrol. 2020, 16, 223–237. [Google Scholar] [CrossRef]
- Alyami, M.H.; Naser, A.Y.; Alyami, H.S.; Algahtani, T.S.; Alyami, A.H.; Alsalem, S.; Almansour, A.; Alswar, H.S.; Al Alhareth, A.M. Prevalence and Knowledge of Respiratory Symptoms Among the General Public in the Southern Area of Najran, Saudi Arabia: A Cross-Sectional Health Survey Study. Int. J. Gen. Med. 2023, 16, 4077–4090. [Google Scholar] [CrossRef] [PubMed]
- Powell-Wiley, T.M.; Poirier, C.P.; Burke, V.C.L.E.; Després, J.P.; Gordon-Larsen, P.; Lavie, C.J. Obesity and Cardiovascular Disease. Circulation 2021, 143, e984–e1010. [Google Scholar] [CrossRef] [PubMed]
- Gross, J.J.; Uusberg, H.; Uusberg, A. Mental illness and well-being: An affect regulation perspective. World Psychiatry 2019, 18, 130–139. [Google Scholar] [CrossRef]
- Alshareef, S.M.; Aldayel, A.Y.; AlKhathlan, M.A.; Alduaij, K.O.; Alshareef, F.G.; Al-Harthi, M.E.; Aldayel, A.A.; Shadid, A.M.; Bin Dahmash, A. Diabetic patients in Saudi Arabia. SciVee 2019, 40, 271–276. [Google Scholar] [CrossRef]
- Bahari, G.; Scafide, K.; Krall, J.; Mallinson, R.K.; Weinstein, A.A. Mediating role of self-efficacy in the relationship between family social support and hypertension self-care behaviours: A cross-sectional study of Saudi men with hypertension. Int. J. Nurs. Pract. 2019, 25, e12785. [Google Scholar] [CrossRef] [PubMed]
- Alasiri, A.A.; Mohammed, V. Healthcare Transformation in Saudi Arabia: An Overview Since the Launch of Vision 2030. Health Serv. Insights 2022, 15, 11786329221121214. [Google Scholar] [CrossRef] [PubMed]
- Catarino, M.; Charepe, Z.; Festas, C. Promotion of Self-Management of Chronic Disease in Children and Teenagers: Scoping Review. Healthcare 2021, 9, 1642. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Park, S.; Lee, K.-S. Relationship between Morbidity and Health Behavior in Chronic Diseases. J. Clin. Med. 2020, 9, 121. [Google Scholar] [CrossRef] [PubMed]
- Muscat, D.M.; Song, W.; Cvejic, E.; Ting, J.H.C.; Medlin, J.; Nutbeam, D. The Impact of the Chronic Disease Self-Management Program on Health Literacy: A Pre-Post Study Using a Multi-Dimensional Health Literacy Instrument. Int. J. Environ. Res. Public Health 2020, 17, 58. [Google Scholar] [CrossRef] [PubMed]
- Hudon, C.; Chouinard, M.-C.; Diadiou, F.; Bouliane, D.; Lambert, M.; Hudon, É. The Chronic Disease Self-Management Program: The experience of frequent users of health care services and peer leaders. Fam. Pract. 2016, 33, 167–171. [Google Scholar] [CrossRef] [PubMed]
- Tomioka, M.; Braun, K.L.; Compton, M.; Tanoue, L. Adapting Stanford’s Chronic Disease Self-Management Program to Hawaii’s Multicultural Population. Gerontologist 2012, 52, 121–132. [Google Scholar] [CrossRef]
- Luu, K.L.; Witkamp, F.E.; Nieboer, D.; Bakker, E.M.; Kranenburg, L.W.; van der Rijt, C.C.D.; Lorig, K.; van der Heide, A.; Rietjens, J.A.C. Effectiveness of the “Living with Cancer” peer self-management support program for persons with advanced cancer and their relatives: Study protocol of a non-randomized stepped wedge study. BMC Palliat. Care 2022, 21, 107. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef]
- AlOtaibi, S.S.; Almutairi, H.A.; Alotaibi, M.K.; Alharbi, K.; Bahari, G. Enhancing Nurses’ Disaster Management and Preparedness: Evaluating the Effectiveness of an Online Educational Program through a Quasi-Experimental Study. Risk Manag. Health Policy 2024, 17, 101–111. [Google Scholar] [CrossRef]
- Alshahrani, H.; Matrafi, N.; Qahtani, N.; Taliby, R.; Hassanein, M.; Rowilly, I. Mapping the Private Healthcare Sector in Riyadh Region: Size, Services, and Alignment with the Saudi Ministry of Health Priorities. Mater. Socio Medica 2023, 35, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Al-Sheddi, A.; Kamel, S.; Almeshal, A.S.; Assiri, A.M.; Kamel, S., Jr. Distribution of Primary Healthcare Centers Between 2017 and 2021 Across Saudi Arabia. Cureus 2023, 15, e41932. [Google Scholar] [CrossRef] [PubMed]
- Davis, S.L.; Johnson, A.H.; Lynch, T.; Gray, L.; Pryor, E.R.; Azuero, A.; Soistmann, H.C.; Phillips, S.R.; Rice, M. Inclusion of Effect Size Measures and Clinical Relevance in Research Papers. Nurs. Res. 2020, 70, 222–230. [Google Scholar] [CrossRef] [PubMed]
- Pullyblank, K.; Brunner, W.; Scribani, M.; Krupa, N.; Ory, M.G.; Smith, M.L. Recruitment and engagement in disease self-management programs: Special concerns for rural residents reporting depression and/or anxiety. Prev. Med. Rep. 2022, 26, 101761. [Google Scholar] [CrossRef] [PubMed]
- Leong, S.M.; Lei, W.I.; Chan, U.W. The Six-Month and One-Year Outcome of a Chronic Disease Self-Management Program among Older Adults in Macao: A Quasi-Experimental Study. SAGE Open Nurs. 2020, 6, 2377960820958231. [Google Scholar] [CrossRef] [PubMed]
- Bahari, G.; Kerari, A. Evaluating the Effectiveness of a Self-Management Program on Patients Living with Chronic Diseases. Risk Manag. Health Policy 2024, 17, 487–496. [Google Scholar] [CrossRef] [PubMed]
- Lorig, K.; Stewart, A.; Ritter, P.; González, V.; Laurent, D.; Lynch, J. Outcome Measures for Health Education and Other Health Care Interventions; SAGE Publications: Thousand Oaks, CA, USA, 1996; 99p. [Google Scholar]
- Marconcin, P.; Tomé, G.; Carnide, F.; Yázigi, F.; Campos, P.; Pais, S.; Espanha, M. Translation, cultural adaptation and validation of the self-efficacy to manage chronic disease 6-Item scale for European Portuguese. Acta Reumatol. Port. 2021, 46, 15–22. [Google Scholar] [PubMed]
- Han, H.R.; Lee, H.; Commodore-Mensah, Y.; Kim, M. Development and Validation of the Hypertension Self-Care Profile: A Practical Tool to Measure Hypertension Self-Care. J. Cardiovasc. Nurs. 2014, 29, E11–E20. [Google Scholar] [CrossRef] [PubMed]
- Al-Asmari, A.I.; Al-Amoudi, D.H. The role of ethanol in fatalities in Jeddah, Saudi Arabia. Forensic Sci. Int. 2020, 316, 110464. [Google Scholar] [CrossRef]
- Devins, G.M.; Mandin, H.; Hons, R.B.; Burgess, E.D.; Klassen, J.; Taub, K.; Buckle, S. Illness intrusiveness and quality of life in end-stage renal disease: Comparison and stability across treatment modalities. Health Psychol. 1990, 9, 117–1142. [Google Scholar] [CrossRef]
- Kroenke, K.; Strine, T.W.; Spitzer, R.L.; Williams, J.B.; Berry, J.T.; Mokdad, A.H. The PHQ-8 as a measure of current depression in the general population. J. Affect. Disord. 2009, 114, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Sobers, N.P.; Hambleton, I.R.; Hassan, S.; Anderson, S.G.; Brathwaite-Graham, L.; Lewis, K.; Ferguson, T.S. Assessing the effectiveness and implementation of a chronic disease self-management programme in faith-based organisations in Barbados: Protocol for a cluster randomised parallel trial. BMJ Open 2021, 11, e050548. [Google Scholar] [CrossRef] [PubMed]
- Haslbeck, J.; Zanoni, S.; Hartung, U.; Klein, M.; Gabriel, E.; Eicher, M.; Schulz, P.J. Introducing the chronic disease self-management program in Switzerland and other German-speaking countries: Findings of a cross-border adaptation using a multiple-methods approach. BMC Health Serv. Res. 2015, 15, 576. [Google Scholar] [CrossRef] [PubMed]
- Hoong, J.M.; Koh, H.A.; Wong, K.; Lee, H.H. Effects of a community-based chronic disease self-management programme on chronic disease patients in Singapore. Chronic Illn. 2023, 19, 434–443. [Google Scholar] [CrossRef] [PubMed]
- Ritter, P.L.; Lorig, K.; Laurent, D.D. Characteristics of the Spanish- and English-Language Self-Efficacy to Manage Diabetes Scales. Diabetes Educ. 2016, 42, 167–177. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Hardin, H.K.; Zhou, L.; Fang, L.; Shi, P.; Robinson, K.M. Implementation and evaluation of the chronic-disease self-management program among Chinese immigrant older adults in the U.S. Geriatr. Nurs. 2014, 35, 448–450. [Google Scholar] [CrossRef]
- Hevey, D.; Wilson O’Raghallaigh, J.; O’Doherty, V.; Lonergan, K.; Marese, H.; Victoria, L.; Sinead, M.; Damien, L.; Niamh, L.; Kathy, M.; et al. Pre-post effectiveness evaluation of Chronic Disease Self-Management Program (CDSMP) participation on health, well-being and health service utilization. Chronic Illn. 2020, 16, 146–158. [Google Scholar] [CrossRef]
- Angwenyi, V.; Bunders-Aelen, J.; Criel, B.; Lazarus, J.V.; Aantjes, C. An evaluation of self-management outcomes among chronic care patients in community home-based care programmes in rural Malawi: A 12-month follow-up study. Health Soc. Care Community 2020, 29, 353–368. [Google Scholar] [CrossRef]
- Lorig, K. Chronic Disease Self-Management Program: Insights from the Eye of the Storm. Front. Public Health 2015, 2, 253. [Google Scholar] [CrossRef]
- Wilson, M.G.; DeJoy, D.M.; Vandenberg, R.J.; Padilla, H.M.; Haynes, N.J.; Zuercher, H.; Corso, P.; Lorig, K.; Smith, M.L. Translating CDSMP to the Workplace: Results of the Live Healthy Work Healthy Program. Am. J. Health Promot. 2021, 35, 491–502. [Google Scholar] [CrossRef] [PubMed]
- Andrade, C. The Limitations of Quasi-Experimental Studies, and Methods for Data Analysis When a Quasi-Experimental Research Design Is Unavoidable. Indian J. Psychol. Med. 2021, 43, 451–452. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Intervention (n = 45) | Control (n = 65) | x2/t-Value | |
|---|---|---|---|
| Mean Age (SD) | 43.40 (6.94) | 48.97 (14.58) | 2.76 *** |
| Sex | 5.23 * | ||
| Female (%) | 50 | 50 | |
| Male (%) | 29.2 | 70.8 | |
| Education | 8.43 ** | ||
| Higher Education (%) | 46.3 | 53.7 | |
| Lower Education (%) | 72.3 | 27.7 | |
| Income | 30.43 *** | ||
| <9000 Riyals (%) | 22.2 | 77.8 | |
| >9000 Riyals (%) | 72.5 | 27.5 | |
| Mean Medication Numbers (SD) | 2 (1.19) | 3.35 (2.30) | 3.77 ** |
| Mean History of Chronic Diseases in Years (SD) | 9.95 (8.60) | 9.29 (7.21) | 0.40 |
| Comorbidity | |||
| Living with One Chronic Disease (%) | 47.2 | 52.8 | 2.37 |
| Living with ≥One Chronic Disease (%) | 29 | 71 | |
| Disease Management Support | 10.03 ** | ||
| Family Support (%) | 21.1 | 78.9 | |
| By the Patient (%) | 53.8 | 46.2 |
| Outcome Measures | Mean (SD) | t-Value | |
|---|---|---|---|
| Intervention | Control | ||
| Self-Management Behaviors (range 19–76) $ | 47.65 (9.73) | 50.25 (9.90) | 0.99 |
| Self-Efficacy (range 6–60) $ | 34.72 (13.64) | 33.10 (11.75) | 1.68 |
| Health-Related Outcomes | |||
| Cognitive Symptom Management (range 0–30) $ | 13.60 (4.69) | 12.26 (6.40) | 1.88 |
| Illness Intrusiveness (range 13–91) $ | 57.25 (16.52) | 51.36 (15.67) | 1.56 |
| Pain Severity (range 5–38) § | 20.04 (6.36) | 17.08 (8.24) | 1.95 |
| Depressive Symptom (range 0–24) § | 9.27 (2.98) | 6.41 (5.77) | 2.82 ** |
| Outcome Measure | Group | Mean | S.E. | 95% CI | F-Value |
|---|---|---|---|---|---|
| Self-Management Behaviors (range 19–76) $ | Intervention | 54.38 | 0.97 | 52.45–56.30 | 11.17 ** |
| Control | 49.84 | 0.82 | 48.21–51.46 | ||
| Self-Efficacy (range 6–60) $ | Intervention | 40.21 | 1.29 | 37.63–42.79 | 8.80 ** |
| Control | 34.88 | 1.10 | 32.69–37.06 | ||
| Health-related Outcomes | |||||
| Cognitive Symptom Management (range 0–30) $ | Intervention | 17.22 | 0.76 | 15.71–18.74 | 26.50 *** |
| Control | 12.27 | 0.64 | 10.99–13.55 | ||
| Illness Intrusiveness (range 13–91) $ | Intervention | 61.17 | 1.80 | 57.58–64.76 | 12.76 ** |
| Control | 51.65 | 1.52 | 48.63–54.68 | ||
| Pain Severity (range 5–38) § | Intervention | 14.20 | 0.88 | 12.45–15.95 | 8.22 ** |
| Control | 17.32 | 0.77 | 15.84–18.79 | ||
| Depressive Symptom (range 0–24) § | Intervention | 4.16 | 0.46 | 3.23–5.08 | 16.22 *** |
| Control | 7.35 | 0.39 | 6.57–8.12 |
| Outcome Measures | Intervention | Control | ||||
|---|---|---|---|---|---|---|
| Pretest Mean (SD) | Posttest Mean (SD) | t-Test | Pretest Mean (SD) | Posttest Mean (SD) | t-Test | |
| Self-Management Behaviors (range 19–76) $ | 47.65 (9.73) | 53.76 (8.03) | 3.91 *** | 50.25 (9.90) | 50.12 (8.85) | 0.35 |
| Self-Efficacy (range 6–60) $ | 34.72 (13.64) | 40.04 (12.95) | 1.98 * | 33.10 (11.75) | 33.95 (11.47) | 1.71 |
| Cognitive Symptom Management (range 0–30) $ | 13.60 (4.69) | 17.11 (5.60) | 4.10 *** | 12.26 (6.40) | 11.46 (6.52) | 0.48 |
| Illness Intrusiveness (range 13–91) $ | 57.25 (16.52) | 61.06 (17.27) | 2.28 * | 51.36 (15.67) | 49.83 (14.51) | 0.66 |
| Pain Severity (range 5–38) § | 20.04 (6.36) | 15.02 (3.46) | 4.52 *** | 17.08 (8.24) | 16.40 (8.57) | 0.65 |
| Depressive Symptom (range 0–24) § | 9.27 (2.98) | 5.06 (3.28) | 8.01 *** | 6.41 (5.77) | 6.53 (4.81) | 0.65 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kerari, A.; Bahari, G.; Alharbi, K.; Alenazi, L. The Effectiveness of the Chronic Disease Self-Management Program in Improving Patients’ Self-Efficacy and Health-Related Behaviors: A Quasi-Experimental Study. Healthcare 2024, 12, 778. https://doi.org/10.3390/healthcare12070778
Kerari A, Bahari G, Alharbi K, Alenazi L. The Effectiveness of the Chronic Disease Self-Management Program in Improving Patients’ Self-Efficacy and Health-Related Behaviors: A Quasi-Experimental Study. Healthcare. 2024; 12(7):778. https://doi.org/10.3390/healthcare12070778
Chicago/Turabian StyleKerari, Ali, Ghareeb Bahari, Kholoud Alharbi, and Latifah Alenazi. 2024. "The Effectiveness of the Chronic Disease Self-Management Program in Improving Patients’ Self-Efficacy and Health-Related Behaviors: A Quasi-Experimental Study" Healthcare 12, no. 7: 778. https://doi.org/10.3390/healthcare12070778