
Economic Evaluation of the Thai Diagnostic Autism Scale for Autism Spectrum Disorder Diagnosis in Children Aged 1–5 Years Old

Abstract
:1. Introduction
2. Materials and Methods
2.1. Overall Description
2.2. Intervention and Comparator
2.3. Model Structure and Assumptions
2.4. Model Validation
2.5. Model Inputs
2.5.1. The Performance of TDAS and Probabilities of Being Diagnosed
2.5.2. Transitional Probabilities and Relative Risk of Death in Patients with ASD
2.5.3. Costs and Health Utility
2.6. Data Analysis
3. Results
3.1. Base-Case and Scenario Analysis Findings
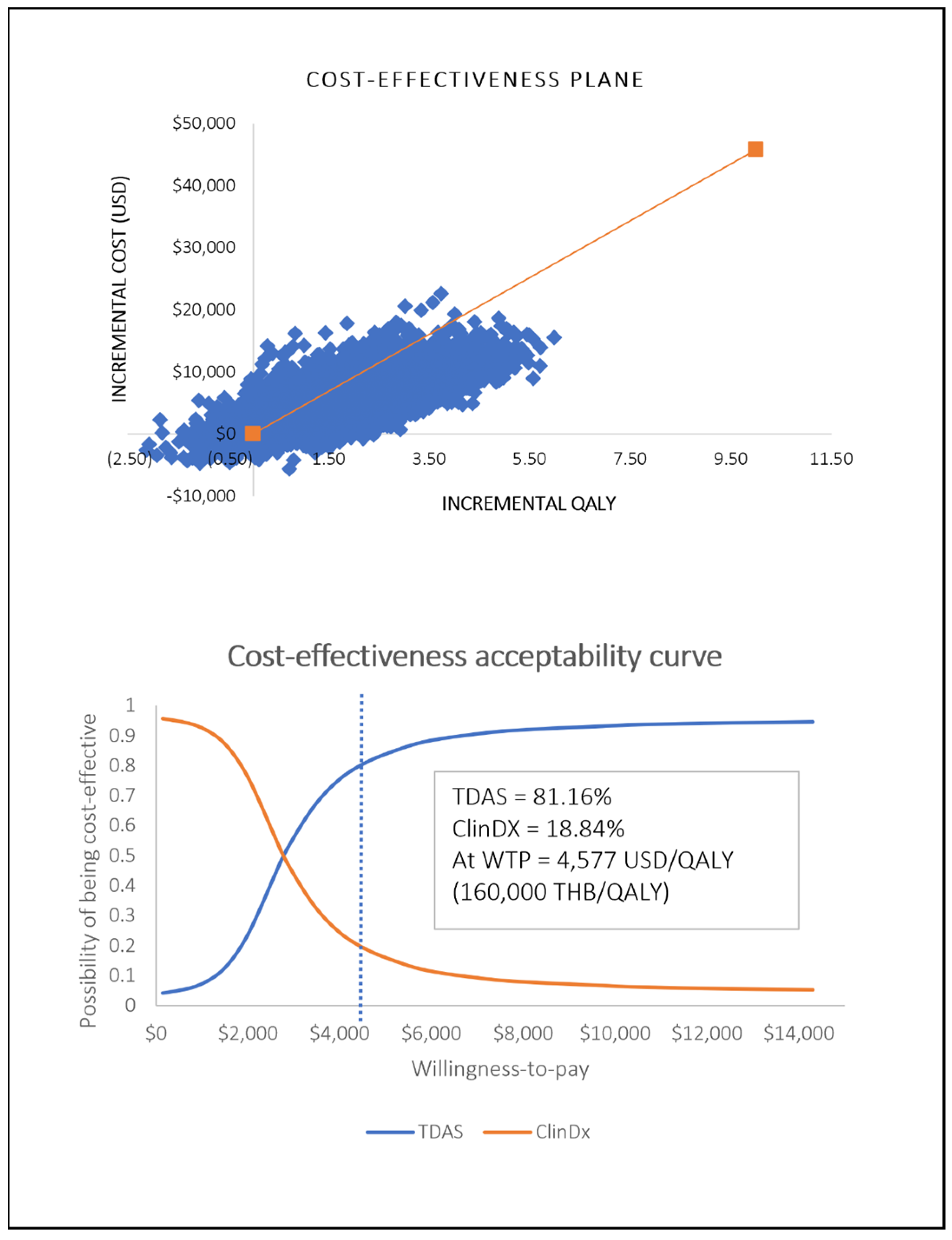
3.2. Sensitivity Analysis
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hodges, H.; Fealko, C.; Soares, N. Autism spectrum disorder: Definition, epidemiology, causes, and clinical evaluation. Transl. Pediatr. 2020, 9, S55–S65. [Google Scholar] [CrossRef] [PubMed]
- Tian, J.; Gao, X.; Yang, L. Repetitive Restricted Behaviors in Autism Spectrum Disorder: From Mechanism to Development of Therapeutics. Front. Neurosci. 2022, 16, 780407. [Google Scholar] [CrossRef] [PubMed]
- Grzadzinski, R.; Amso, D.; Landa, R.; Watson, L.; Guralnick, M.; Zwaigenbaum, L.; Deak, G.; Estes, A.; Brian, J.; Bath, K.; et al. Pre-symptomatic intervention for autism spectrum disorder (ASD): Defining a research agenda. J. Neurodev. Disord. 2021, 13, 49. [Google Scholar] [CrossRef]
- Geschwind, D.H. Genetics of autism spectrum disorders. Trends Cogn. Sci. 2011, 15, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Hallmayer, J.; Cleveland, S.; Torres, A.; Phillips, J.; Cohen, B.; Torigoe, T.; Miller, J.; Fedele, A.; Collins, J.; Smith, K.; et al. Genetic heritability and shared environmental factors among twin pairs with autism. Arch. Gen. Psychiatry 2011, 68, 1095–1102. [Google Scholar] [CrossRef] [PubMed]
- Gardener, H.; Spiegelman, D.; Buka, S.L. Prenatal risk factors for autism: Comprehensive meta-analysis. Br. J. Psychiatry 2009, 195, 7–14. [Google Scholar] [CrossRef]
- Zeidan, J.; Fombonne, E.; Scorah, J.; Ibrahim, A.; Durkin, M.S.; Saxena, S.; Yusuf, A.; Shih, A.; Elsabbagh, M. Global prevalence of autism: A systematic review update. Autism Res. 2022, 15, 778–790. [Google Scholar] [CrossRef]
- Poolsuppasit, S.; Panyayong, B.; Liknapichitkul, D.; Serisathien, P.; Chutha, W. Holistic care for Thai autism. J. Ment. Health Care Thail. 2005, 13, 10–16. [Google Scholar]
- Ben-Itzchak, E.; Zachor, D.A. The effects of intellectual functioning and autism severity on outcome of early behavioral intervention for children with autism. Res. Dev. Disabil. 2007, 28, 287–303. [Google Scholar] [CrossRef]
- Lord, C.; Rutter, M. Autism Diagnostic Observation ScheduleTM, 2nd ed.; Western Psychological Services: Los Angeles, CA, USA, 2012. [Google Scholar]
- Schopler, E.; Van Bourgondien, M.E.; Wellma, G.J.; Love, S.R. Childhood Autism Rating ScaleTM, 2nd ed.; Western Psychological Services: Los Angeles, CA, USA, 2010. [Google Scholar]
- Rutter, M.; LeCouteur, A.; Lord, C. Autism Diagnostic Interview-Revised; Western Psychological Services: Los Angeles, CA, USA, 2003. [Google Scholar]
- Yuen, T.; Carter, M.T.; Szatmari, P.; Ungar, W.J. Cost-Effectiveness of Universal or High-Risk Screening Compared to Surveillance Monitoring in Autism Spectrum Disorder. J. Autism Dev. Disord. 2018, 48, 2968–2979. [Google Scholar] [CrossRef]
- Piccininni, C.; Bisnaire, L.; Penner, M. Cost-effectiveness of Wait Time Reduction for Intensive Behavioral Intervention Services in Ontario, Canada. JAMA Pediatr. 2017, 171, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Penner, M.; Rayar, M.; Bashir, N.; Roberts, S.W.; Hancock-Howard, R.L.; Coyte, P.C. Cost-Effectiveness Analysis Comparing Pre-diagnosis Autism Spectrum Disorder (ASD)-Targeted Intervention with Ontario’s Autism Intervention Program. J. Autism Dev. Disord. 2015, 45, 2833–2847. [Google Scholar] [CrossRef] [PubMed]
- Department of Mental Health Ministry of Public Health. A Clinical Practice Guideline for the Care of Four Major Psychiatric Diseases in Children and Adolescents (Intellectual Disability, Autism, Attention Deficit, an Learning Disabilities) for the Public Health Service Network; The Agricultural Co-Operative Federation of Thailand Limited: Bangkok, Thailand, 2016. [Google Scholar]
- Tangviriyapaiboon, D.; Kawilapat, S.; Sirithongthaworn, S.; Apikomonkon, H.; Suyakong, C.; Srikummoon, P.; Thumronglaohapun, S.; Traisathit, P. The Optimal Cut-Off Point for Thai Diagnostic Autism Scale and Probability Prediction of Autism Spectrum Disorder Diagnosis in Suspected Children. Healthcare 2022, 10, 1868. [Google Scholar] [CrossRef] [PubMed]
- Tangviriyapaiboon, D.; Sirithongthaworn, S.; Apikomonkon, H.; Suyakong, C.; Srikummoon, P.; Kawilapat, S.; Traisathit, P. Development and psychometric evaluation of a Thai Diagnostic Autism Scale for the early diagnosis of Autism Spectrum Disorder. Autism Res. 2022, 15, 317–327. [Google Scholar] [CrossRef] [PubMed]
- Department of Mental Health Ministry of Public Health. Thai Early Developmental Assessment for Intervention: TEDA4I; Chumnumsahakornkarnkasat of Thailand: Bangkok, Thailand, 2020. [Google Scholar]
- Sirithongthaworn, S. The Development of Developmental Surveillance and Promotion Manual; DSPM. J. Psychiatr. Assoc. Thail. 2018, 63, 3–12. [Google Scholar]
- Panyayong, B. The validation of the pervasive developmental. J. Ment. Health Thail. 2012, 18, 36–44. [Google Scholar]
- Pornnoppadol, C.; Thongngen, A.; Gaevalin, A.; Sangratanayont, D. Development of the Pervasive Developmental Disorders Screening Questionnaire. J. Psychiatr. Assoc. Thail. 2002, 47, 75–96. [Google Scholar]
- Guideline Development Working Group. Guideline for Health Technology Assessment in Thailand Updated Edition: 2019; Ministry of Public Health: Nonthaburi, Thailand, 2021.
- Husereau, D.; Drummond, M.; Augustovski, F.; de Bekker-Grob, E.; Briggs, A.H.; Carswell, C.; Caulley, L.; Chaiyakunapruk, N.; Greenberg, D.; Loder, E.; et al. Consolidated Health Economic Evaluation Reporting Standards (CHEERS) 2022 Explanation and Elaboration: A Report of the ISPOR CHEERS II Good Practices Task Force. Value Health 2022, 25, 10–31. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5); American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders: Diagnostic Criteria for Research; World Health Organization: Geneva, Switzerland, 1993. [Google Scholar]
- Sirithongthaworn, S.; Tangviriyapaiboon, D. Assessment of autism spectrum disorder among early childhood suspected of developmental delay or autism spectrum disorder: A pilot study in Chiang Mai. J. Ment. Health Thail. 2021, 29, 249–258. [Google Scholar]
- Catala-Lopez, F.; Hutton, B.; Page, M.J.; Driver, J.A.; Ridao, M.; Alonso-Arroyo, A.; Valencia, A.; Macias Saint-Gerons, D.; Tabares-Seisdedos, R. Mortality in Persons with Autism Spectrum Disorder or Attention-Deficit/Hyperactivity Disorder: A Systematic Review and Meta-analysis. JAMA Pediatr. 2022, 176, e216401. [Google Scholar] [CrossRef]
- Shiroiwa, T.; Ikeda, S.; Noto, S.; Fukuda, T.; Stolk, E. Valuation Survey of EQ-5D-Y Based on the International Common Protocol: Development of a Value Set in Japan. Med. Decis. Mak. 2021, 41, 597–606. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Input Parameters | Value (Standard Error) | Distribution | References |
|---|---|---|---|
| Probabilities for diagnostic phase (Decision tree model) | |||
| Probability of being test-positive for TDAS | 0.8990 (0.0339) | Beta | [27] |
| Probability of true positive for TDAS | 0.8286 (0.0368) | Beta | [17] |
| Probability of false positive for TDAS | 0.1961 (0.0556) | Beta | [17] |
| Probability of delayed diagnosis for TDAS | 0.0071 (0.0071) | Beta | A retrospective chart review from 5 hospitals |
| Probability of mild ASD for TDAS | 0.1111 (0.0786) | Dirichlet | |
| Probability of moderate ASD for TDAS | 0.5069 (0.0585) | Dirichlet | |
| Probability of severe ASD for TDAS | 0.3819 (0.0655) | Dirichlet | |
| Probability of being diagnosed with ASD for ClinDx | 0.6731 (0.0376) | Beta | [17] |
| Probability of delayed diagnosis for ClinDx | 0.2000 (0.0332) | Beta | A retrospective chart review from 5 hospitals |
| Probability of mild ASD for ClinDx | 0.0608 (0.0797) | Dirichlet | |
| Probability of moderate ASD for ClinDx | 0.3311 (0.0672) | Dirichlet | |
| Probability of severe ASD for ClinDx | 0.6081 (0.0515) | Dirichlet | |
| Probabilities for follow-up phase (Markov model) | |||
| Transitional probabilities from mild to moderate | 0.0620 (0.0538) | Beta | A retrospective chart review from 5 hospitals |
| Transitional probabilities from mild to severe | 0.0000 (0.0000) | Fixed | |
| Transitional probabilities from moderate to mild | 0.2643 (0.0226) | Beta | |
| Transitional probabilities from moderate to severe | 0.0218 (0.0087) | Beta | |
| Transitional probabilities from severe to mild | 0.0025 (0.0044) | Beta | |
| Transitional probabilities from severe to moderate | 0.2078 (0.1730) | Beta | |
| Relative risk of death in patients with ASD | 2.370 (0.0942) | Log-normal | [28] |
| Utility values | |||
| Utility for mild ASD | 0.8659 (0.0085) | Beta | A cross-sectional interview by EQ-5D-Y from 5 hospitals |
| Utility for moderate ASD | 0.8410 (0.0098) | Beta | |
| Utility for severe ASD | 0.7930 (0.0177) | Beta | |
| Direct medical cost (USD) | |||
| Cost of ASD treatment for an inpatient visit (mild) | 387 (88) | Gamma | A retrospective database analysis from 5 hospitals |
| Cost of ASD treatment for an inpatient visit (moderate) | 416 (38) | Gamma | |
| Cost of ASD treatment for an inpatient visit (severe) | 664 (53) | Gamma | |
| Proportion of patients having admission | 0.3460 (0.0280) | Beta | A cross-sectional interview from 5 hospitals |
| Proportion of patient hospitalized with mild ASD | 0.0585 (-) | Fixed | |
| Proportion of patient hospitalized with moderate ASD | 0.3032 (-) | Fixed | |
| Proportion of patient hospitalized with severe ASD | 0.6383 (-) | Fixed | |
| Cost of outpatient ASD treatment (mild) | 66 (11) | Gamma | A retrospective database analysis from 5 hospitals |
| Cost of outpatient ASD treatment (moderate) | 133 (7) | Gamma | |
| Cost of outpatient ASD treatment (severe) | 124 (12) | Gamma | |
| Cost of purchasing additional instruments (mild) | 11 (26) | Gamma | A cross-sectional interview from 5 hospitals |
| Cost of purchasing additional instruments (moderate) | 197 (24) | Gamma | |
| Cost of purchasing additional instruments (severe) | 199 (25) | Gamma | |
| Proportion of patients purchasing additional instruments (mild) | 0.5565 (-) | Fixed | |
| Proportion of patients purchasing additional instruments (moderate) | 0.6852 (-) | Fixed | |
| Proportion of patients purchasing additional instruments (severe) | 0.8966 (-) | Fixed | |
| Cost of additional activities for ASD (mild) | 1314 (246) | Gamma | |
| Cost of additional activities for ASD (moderate) | 1148 (188) | Gamma | |
| Cost of additional activities for ASD (severe) | 1152 (216) | Gamma | |
| Proportion of attending additional activities (mild) | 0.2114 (-) | Fixed | |
| Proportion of attending additional activities (moderate) | 0.2243 (-) | Fixed | |
| Proportion of attending additional activities (severe) | 0.4561 (-) | Fixed | |
| Direct non-medical cost (USD) | |||
| Travel cost per outpatient visit | 13 (0.9) | Gamma | A cross-sectional interview from 5 hospitals |
| Additional food cost per outpatient visit | 8 (0.5) | Gamma | |
| Accommodation cost per outpatient visit | 24 (3.6) | Gamma | |
| Proportion of patients with accommodation for outpatient | 0.60 (0.03) | Beta | |
| Average number of outpatient visits per year (mild) | 5.13 (0.49) | Gamma | |
| Average number of outpatient visits per year (moderate) | 4.89 (0.48) | Gamma | |
| Average number of outpatient visits per year (severe) | 6.65 (0.91) | Gamma | |
| Caregiver cost for accompanying patients to outpatient visit | 38 (3) | Gamma | |
| Travel cost per admission for patients | 48 (6) | Gamma | |
| Additional food cost per admission for patients | 9 (0.7) | Gamma | |
| Accommodation cost per admission for patients | 15 (1) | Gamma | |
| Proportion of patients with accommodation for admissions | 0.385 (0.078) | Beta | |
| Travel cost per admission for caregivers | 63 (10) | Gamma | |
| Additional food cost per admission for caregivers | 80 (8) | Gamma | |
| Accommodation cost per admission for caregivers | 183 (48) | Gamma | |
| Caregiver cost for accompanying patients to admissions | 225 (105) | Gamma | |
| Average number of admissions per year | 1 (-) | Fixed | |
| Caregiver cost at home (USD) | |||
| Hired caregiver salary | 196 (32) | Gamma | A cross-sectional interview from 5 hospitals |
| Proportion of hired caregiver | 0.058 (-) | Fixed | |
| Unhired caregiver salary | 518 (53) | Gamma | |
| Proportion of unhired caregiver quitting a job (mild) | 0.1778 (-) | Fixed | |
| Proportion of unhired caregiver quitting a job (moderate) | 0.1348 (-) | Fixed | |
| Proportion of unhired caregiver quitting a job (severe) | 0.2364 (-) | Fixed | |
| Cost of TDAS and ClinDx | |||
| Cost of TDAS training (per provider) | 151 (±20%) | Gamma | Internal data from previous TDAS implementation |
| Cost of TDAS instruments at implementation | 323 (±20%) | Gamma | |
| Cost of TDAS maintenance per patient per year | 0.27 (±20%) | Gamma | |
| Cost of cloud services per patient per year | 1.43 (±20%) | Gamma | |
| Average labor cost for TDAS (per month) | 134 (±20%) | Gamma | An interview from healthcare providers |
| Average labor cost for ClinDx (per month) | 61 (±20%) | Gamma | |
| The number of ASD diagnoses (per week) | 2.0 (-) | Fixed | |
| Intervention | Undiscounted | Discounted | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Cost (USD) | QALY | Incremental Cost (USD) | Incremental QALY | ICER (USD/QALY) | Cost (USD) | QALY | Incremental Cost (USD) | Incremental QALY | ICER (USD/QALY) | |
| Base-case analysis | ||||||||||
| TDAS | 80,304 | 31.36 | 10,119 | 3.92 | 2579 | 43,231 | 15.55 | 5577 | 1.96 | 2852 |
| ClinDx | 70,185 | 27.43 | Reference | 37,654 | 13.59 | Reference | ||||
| Scenario analysis | ||||||||||
| TDAS | 80,293 | 31.36 | 10,408 | 3.84 | 2709 | 43,219 | 15.55 | 5907 | 1.91 | 3092 |
| ClinDx | 69,885 | 27.52 | Reference | 37,312 | 13.64 | Reference | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tangviriyapaiboon, D.; Permsuwan, U.; Pavasuthipaisit, C.; Sriminipun, A.; Dilokthornsakul, P. Economic Evaluation of the Thai Diagnostic Autism Scale for Autism Spectrum Disorder Diagnosis in Children Aged 1–5 Years Old. Healthcare 2024, 12, 782. https://doi.org/10.3390/healthcare12070782
Tangviriyapaiboon D, Permsuwan U, Pavasuthipaisit C, Sriminipun A, Dilokthornsakul P. Economic Evaluation of the Thai Diagnostic Autism Scale for Autism Spectrum Disorder Diagnosis in Children Aged 1–5 Years Old. Healthcare. 2024; 12(7):782. https://doi.org/10.3390/healthcare12070782
Chicago/Turabian StyleTangviriyapaiboon, Duangkamol, Unchalee Permsuwan, Chosita Pavasuthipaisit, Athithan Sriminipun, and Piyameth Dilokthornsakul. 2024. "Economic Evaluation of the Thai Diagnostic Autism Scale for Autism Spectrum Disorder Diagnosis in Children Aged 1–5 Years Old" Healthcare 12, no. 7: 782. https://doi.org/10.3390/healthcare12070782