
StopApp: Using the Behaviour Change Wheel to Develop an App to Increase Uptake and Attendance at NHS Stop Smoking Services


Abstract
:1. Introduction
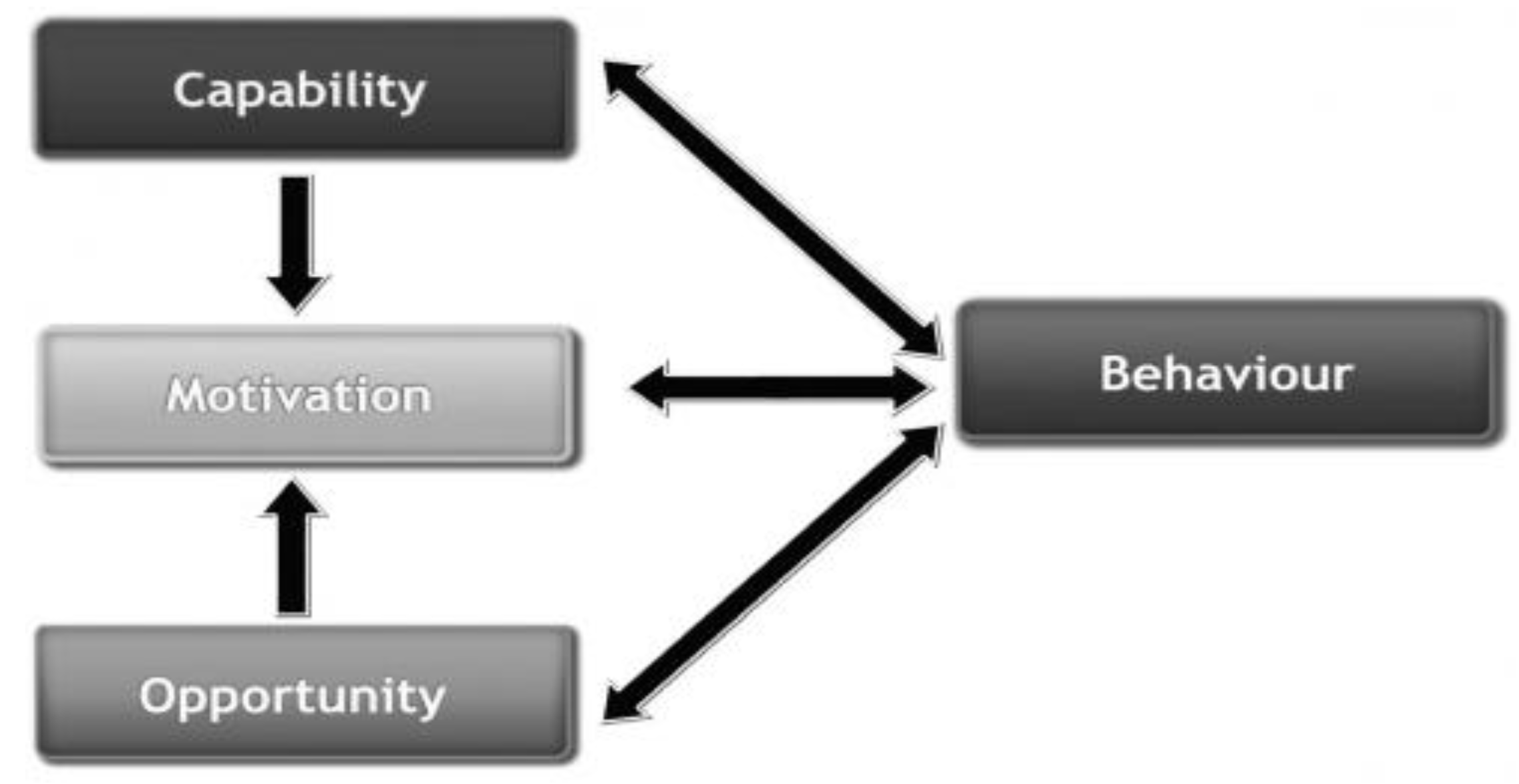
2. A Theoretically Driven Behaviour Change Intervention
3. Aim
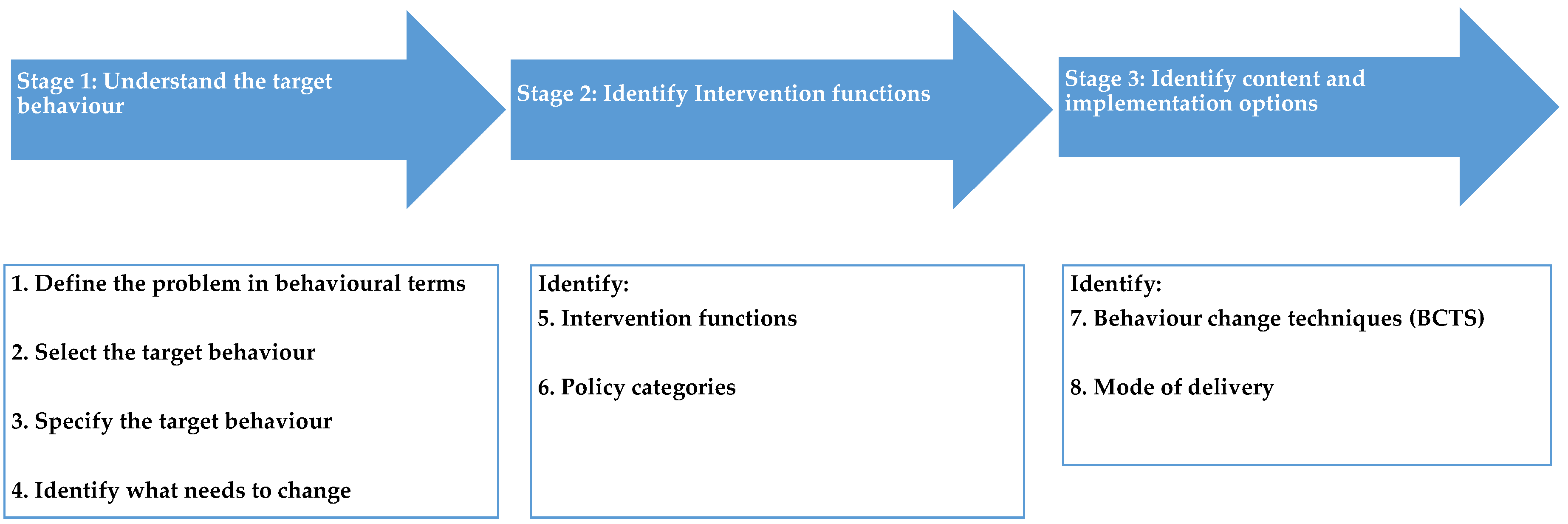
4. Experimental Section and Results
4.1. Stage 1—Understand the Behaviour and Identify What Needs to Change
4.1.1. Step 1—Define the Problem in Behavioural Terms
4.1.2. Step 2—Selecting the Target Behaviour
- ■
- Smokers to book an initial stop smoking advisor appointment.
- ■
- Smokers to attend a stop smoking advisor appointment.
- ■
- Healthcare professionals to (i) signpost and (ii) refer smokers to SSS.
- ■
- Other professionals who come into contact with people who smoke, e.g., housing officers, to signpost or refer smokers to SSS.
- ■
- Hospital staff to operate an opt-out referral system to SSS.
4.1.3. Step 3—Specify the Target Behaviour
4.1.4. Step 4—Understanding the Target Behaviour and Understanding What Needs to Change
Literature Review
Questionnaires with Smokers and ex-Smokers
4.2. Stage 2—Identify Intervention Options
4.2.1. Step 5—Identify Appropriate Intervention Functions
4.2.2. Step 6—Identify Policy Categories
4.3. Stage 3—Identify Content and Implementation Options
4.3.1. Step 7—Identifying Behaviour Change Techniques (BCTs)
4.3.2. Step 8—Determining the Mode of Delivery
Telephone Interviews with Stop Smoking Advisors
Telephone Interviews with Non-NHS Community Services
4.4. The StopApp Intervention
5. Discussion
A Web App Intervention
6. An Instant Booking System
7. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Action on Smoking & Health: Smoking statistics 2015. Available online: http://www.ash.org.uk/files/documents/ASH_93.pdf (accessed on 18 May 2015).
- Health & Social Care Information Centre (2015). Statistics on Smoking: England 2015. Available online: http://www.hscic.gov.uk/catalogue/PUB17526/stat-smok-eng-2015-rep.pdf (accessed on 1 June 2015).
- Health & Social Care Information Centre (2014). Statistics on NHS Stop Smoking Services in England: 1 April 2013 to 31 March 2014. Available online: http://www.hscic.gov.uk/article/2021/Website-Search?productid=17735&q=stop+smoking+services&sort=Relevance&size=10&page=1&area=both#top (accessed on 18 August 2015).
- West, R. Stop smoking Services: Increased Chances of Quitting. NCSCT Briefing #8; National Centre for Smoking Cessation and Training: London, UK, 2012. [Google Scholar]
- Kmietowicz, Z. Action is needed to boost uptake of stop smoking services, say campaigners. BMJ 2015. [Google Scholar] [CrossRef] [PubMed]
- Hajek, P.; Etter, J.; Benowitz, N.; Eissenberg, T.; McRobbie, H. Electronic cigarettes: Review of use, content, safety, effects on smokers and potential for harm and benefit. Addiction 2014, 109, 1801–1810. [Google Scholar] [CrossRef] [PubMed]
- West, R.; Brown, J. Electronic cigarettes: Fact and faction. Br. J. Gen. Pract. 2014, 64, 442–443. [Google Scholar] [CrossRef] [PubMed]
- Furber, A. Electronic cigarettes: Reasons to be cautious. Thorax 2015, 70, 307–308. [Google Scholar] [CrossRef] [PubMed]
- Borland, R.; Partos, T.R.; Yong, H.H.; Cummings, K.M.; Hyland, A. How much unsuccessful quitting activity is going on among adult smokers? Data from the International Tobacco Control 4-Country cohort survey. Addiction 2012, 107, 673–682. [Google Scholar] [CrossRef] [PubMed]
- Office of National Statistics 2014: Statistical bulletin: Integrated Household Survey, January to December 2014: Experimental Statistics. Available online: http://www.ons.gov.uk/ons/rel/integrated-household-survey/integrated-household-survey/january-to-december-2014/stb-ihs-jan-dec-2014.html (accessed on 18 May 2015).
- West, R.; May, S.; West, M.; Croghan, E.; McEwen, A. Performance of English stop smoking services in first 10 years: Analysis of service monitoring data. BMJ 2013, 347, f4921. [Google Scholar] [CrossRef] [PubMed]
- Langley, T.; Szatkowski, L.; Lewis, S.; McNeill, A.; Gilmore, A.B.; Salway, R.; Sims, M. The freeze on mass media campaigns in England: A natural experiment of the impact of tobacco control campaigns on quitting behaviour. Addiction 2014, 109, 995–1002. [Google Scholar] [CrossRef] [PubMed]
- Matcham, F.; McNally, L.; Vogt, F. A pilot randomized controlled trial to increase smoking cessation by maintaining National Health Service Stop Smoking Service attendance. Br. J. Health Psychol. 2014, 19, 795–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, R.L.; Coleman, T.; Antoniak, M.; Stocks, J.; Fergus, A.; Britton, J.; Lewis, S.A. The effect of proactively identifying smokers and offering smoking cessation support in primary care populations: A cluster-randomized trial. Addiction 2008, 103, 998–1006. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, H.; Sutton, S.; Morris, R.; Parrot, S.; Galton, S.; Nazareth, I. Evaluating the effectiveness of using personal tailored risk information and taster sessions to increase the uptake of smoking cessation services: Study protocol for a randomised controlled trial. Trials 2012, 13. [Google Scholar] [CrossRef] [PubMed]
- Webb, T.; Joseph, J.; Yardley, L.; Michie, S. Using the Internet to Promote Health Behaviour Change: A Systematic Review and Meta-analysis of the Impact of Theoretical Basis, Use of Behaviour Change Techniques, and Mode of Delivery on Efficacy. J. Med. Intern. Res. 2010, 12. [Google Scholar] [CrossRef] [PubMed]
- Redding, C.A.; Prochaska, J.O.; Armstrong, K.; Rossi, J.S.; Hoeppner, B.B.; Sun, X.; Kobayashi, H.; Yin, H.Q.; Coviello, D.; Evers, K.; et al. Randomized trial outcomes of a TTM-tailored condom use and smoking intervention in urban adolescent females. Health Educ. Res. 2015, 30, 162–178. [Google Scholar] [CrossRef] [PubMed]
- Evers, K.E.; Paiva, A.L.; Johnson, J.L.; Cummins, C.O.; Prochaska, J.O.; Prochaska, J.M.; Padula, J.; Gökbayrak, N.S. Results of a transtheoretical model-based alcohol, tobacco and other drug intervention in middle schools. Addict. Behav. 2012, 37, 1009–1018. [Google Scholar] [CrossRef] [PubMed]
- Abraham, C. Mapping modifiable mechanisms in health promotion research: A commentary on Sniehotta, Presseau, and Araújo-Soares. Health Psychol. Rev. 2015, 9, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; van Stralen, M.M.; West, W. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The behaviour change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behaviour change interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Atkins, L.; West, R. The Behaviour Change Wheel A Guide to Designing Interventions; Silverback Publishing: London, UK, 2014; pp. 978–971. [Google Scholar]
- Curtis, K.E.; Lahiri, S.; Brown, K.E. Targeting Parents for Childhood Weight Management: Development of a Theory-Driven and User-Centered Healthy Eating App. JMIR mHealth uHealth 2015, 3. [Google Scholar] [CrossRef] [PubMed]
- Borland, R.; Yong, H.H.; Balmford, J.; Cooper, J.; Cummings, K.M.; O’Connor, R.J.; McNeill, A.; Zanna, M.P.; Fong, G.T. Motivational factors predict quit attempts but not maintenance of smoking cessation: Findings from the International Tobacco Control Four country project. Nicotine Tob. Res. 2010, 12 (Suppl.), S4–S11. [Google Scholar] [CrossRef] [PubMed]
- Roddy, E.; Antoniak, M.; Britton, J.; Molyneux, A.; Lewis, S. Barriers and motivators to gaining access to smoking cessation services amongst deprived smokers—a qualitative study. BMC Health Serv. Res. 2006, 6. [Google Scholar] [CrossRef] [PubMed]
- McEwen, A.; Condliffe, L.; Gilbert, A. Promoting engagement with a Stop Smoking Service via pro-active telephone calls. Patient Educ. Couns. 2010, 80, 277–279. [Google Scholar] [CrossRef] [PubMed]
- Ussher, M.; Etter, J.F.; West, R. Perceived barriers to and benefits of attending a stop smoking course during pregnancy. Patient Educ. Couns. 2006, 61, 467–472. [Google Scholar] [CrossRef] [PubMed]
- Vogt, F.; Hall, S.; Marteau, T.M. Examining why smokers do not want behavioural support with stopping smoking. Patient Educ. Couns. 2010, 79, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Murray, R.L.; Bauld, L.; Hackshaw, L.E.; McNeill, A. Improving access to smoking cessation services for disadvantaged groups: A systematic review. J. Public Health 2009, 31, 258–277. [Google Scholar] [CrossRef] [PubMed]
- Benson, F.E.; Stronks, K.; Willemsen, M.C.; Bogaerts, N.M.; Nierkens, V. Wanting to attend isn’t just wanting to quit: Why some disadvantaged smokers regularly attend smoking cessation behavioural therapy while others do not: A qualitative study. BMC Public Health 2014, 14, 695. [Google Scholar] [CrossRef] [PubMed]
- Copeland, A.L.; Businelle, M.S.; Stewart, D.W.; Patterson, S.M.; Rash, C.J.; Carney, C.E. Identifying Barriers to Entering Smoking Cessation Treatment Among Socioeconomically Disadvantaged Smokers. J. Smok. Cessat. 2010, 5, 164–171. [Google Scholar] [CrossRef]
- Dobbie, F.; Hiscock, R.; Leonardi-Bee, J.; Murray, S.; Shahab, L.; Aveyard, P.; Coleman, T.; McEwen, A.; McRobbie, H.; Purves, R.; et al. Evaluating long-term outcomes of NHS Stop Smoking Services (ELONS): A prospective cohort study. Health Tech. Assess 2015, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jamison, J.; Sutton, S.; Gilbert, H. Delivering Tailored Smoking Cessation Support via Mobile Phone Text Messaging: A Feasibility and Acceptability Evaluation of the Quittext Program. J. Appl. Biobehav. Res. 2012, 17, 38–58. [Google Scholar] [CrossRef]
- Brown, B.; Michie, S.; Geraghty, A.W.A.; Miller, S.; Yardley, L.; Gardner, B.; Shahab, L.; Stapleton, J.A.; West, R. A pilot study of StopAdvisor: A theory-based interactive internet-based smoking cessation intervention aimed across the social spectrum. Addict. Behav. 2012, 37, 1365–1370. [Google Scholar] [CrossRef] [PubMed]
- Naughton, F.; Jamison, J.; Boase, S.; Sloan, M.; Gilbert, H.; Prevost, T.; Mason, D.; Smith, S.; Brimicombe, J.; Evans, R.; et al. Randomized controlled trial to assess the short-term effectiveness of tailored web- and text-based facilitation of smoking cessation in primary care (iQuit in Practice). Addiction 2013, 109, 1184–1193. [Google Scholar] [CrossRef] [PubMed]
- Sadasivam, R.S.; Volz, E.M.; Kinney, R.L.; Rao, S.R.; Houston, T.K. Share2Quit: Web-Based Peer-Driven Referrals for Smoking Cessation. JMIR Res. Protoc. 2013, 2. [Google Scholar] [CrossRef] [PubMed]
- Kotz, D.; Brown, J.; West, R. Predictive validity of the Motivation To Stop Scale (MTSS): A single-item measure of motivation to stop smoking. Drug Alcohol Depen. 2013, 128, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Local Government Association (2014). MECC Making every contact count—Taking every opportunity to improve health and wellbeing. Available online: http://www.local.gov.uk/web/guest/publications/-/journal_content/56/10180/6578160/PUBLICATION (accessed on 18 May 2015).
- Hughes, L.; McIlvar, M.; McEwen, A. How to advise and refer inpatients who smoke. Nursing Times 2013, 109, 14,16,18. [Google Scholar] [PubMed]
- Guy, R.; Hocking, J.; Wand, H.; Hammad, S.S. How Effective Are Short Message Service Reminders at Increasing Clinic Attendance? A Meta-Analysis and Systematic Review. Health Serv. Res. 2012, 47. [Google Scholar] [CrossRef] [PubMed]
- Atun, A.R.; Sittampalam, S.R.; Mohan, A. Uses and Benefits of SMS in Healthcare Delivery; Tanaka Business School, Imperial College: London, UK, 2005. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Target Behaviour | Smokers to Book and Attend an Initial Appointment at a Stop Smoking Service in Warwickshire |
|---|---|
| Who needs to perform the behaviour? | Anyone who smokes |
| What do they need to do differently to achieve the desired change? | They need to know that the stop smoking service exists |
| They need to know how to book an appointment | |
| They need the opportunity to book an appointment | |
| They need to understand what the stop smoking services offers | |
| They need to know when and how to attend an appointment | |
| When do they need to do it? | As soon as motivation/intention to stop smoking is increased |
| Where do they need to do it? | Anywhere they have access to the intervention via mobile phone, tablet or computer. |
| How often do they need to do it? | Once to book and once to attend initial appointment. It is then the role of the SSS to encourage continued attendance |
| With whom do they need to do it? | On their own or with support from a health/community professional |
| COM-B | Relevant TDF | Description of What Needs Addressing in the Intervention Based on Data Collected/Literature | Intervention Functions | Policy Categories | Behaviour Change Techniques (BCTs) Identified | |
|---|---|---|---|---|---|---|
| Capability | Psychological Capability | Knowledge | 1. A lack of knowledge about the benefits of the service—knowledge about what it does, how it has helped others, what it offers beyond what people may already know, that you are offered more than one appointment. | Education Persuasion Modeling Incentivization (NRT) | Communication/Marketing Service provision Designing the physical/social environment | 5.2 Salience of Consequences 5.3 Information about social/environmental consequences 6.2 Social comparison 9.3 Comparative imagining of future outcomes 10.1 Material incentive 16.3 Vicarious Consequences |
| 2. A lack of knowledge about the ethos (approach), non-judgmental, not just about health risks, supports realistic expectations, time is offered for support (not just quick prescription), how it engages people. | Education Persuasion Modeling | 5.3 Information about social/environmental consequences 6.2 Social comparison | ||||
| 3. A lack of knowledge about access—knowing the service exists, where it is, when you can go, how to get an appointment. | Education Enablement Environmental restructuring | 4.1 Instruction on how to perform the behaviour | ||||
| Opportunity | Physical Opportunity | Environmental context and resources | Perception that time is a barrier- finding the time and the availability of appointments at correct time. Perception that SSS are not easy to access Mode of delivery of invitation—want to be invited face to face (app will be, but not part of content per se) Ease and privacy of booking via app | Enablement Education Environmental restructuring | 4.1 Instruction on how to perform the behaviour 7.1 Prompts/cues | |
| Social Opportunity | Social influences | Perception that no one has used SSS successfully Stigma and blame Others around you Encouragement from health professionals | Education Persuasion Modeling Environmental restructuring | 5.3 Information about social/environmental consequences 5.6 Information about emotional consequences 6.2 Social Comparison 6.3 Information about others’ approval 11.2 Reduce negative emotions | ||
| Motivation | Reflective Motivation | Professional/social role and identity | Don’t like the idea of needing or seeking help/belief that smokers should quit on their own Using SSS is a sign of weakness I can do it if I want/need to Disappointment with self if failed | Education Persuasion | 5.5 Anticipated Regret 5.6 Information about emotional consequences 11.2 Reduce Negative Emotions (see example below) 13.2 Framing/Re-framing 13.5 Identity associated with changed behaviour 15.3 Focus on past success | |
| Beliefs about capabilities | Don’t need support/help/SSS to successfully give up smoking—Already aware of the risks, have quit before, Would access services if was unsure could do it alone | Education Persuasion | 5.3 Information about social/environmental consequences 5.6 Information about emotional consequences | |||
| Optimism | 1. I don’t need help—Unrealistic Optimism | Education Persuasion Modeling | 6.2 Social Comparison 15.1 Verbal persuasion about capability | |||
| Beliefs about consequences | Knowing what to expect, what support, after ‘treatment’, how they would help, more than just NRT, time of appointments, confidentiality Expectation they will be nagged, fear of being judged. SSS don’t offer more than they already know Lack of knowledge of successful outcomes Non-committal—not committed to stopping smoking just the appointment Not knowing if you could go back if needed Beliefs that SSS don’t work—ineffective, it will not help me stop smoking | Education Persuasion Modeling | 5.3 Information about social/environmental consequences 5.6 Information about emotional consequences 6.2 Social Comparison 13.2 Framing/Re-framing | |||
| Intentions | N/A | |||||
| Automatic Motivation | Reinforcement | Lack of knowledge about free prescriptions —would go to SSS if they offered incentives such as free prescriptions, etc. | Education Incentivization | 10.1 Material incentive | ||
| Emotion | Fear of failing—the fear of failing stops me accessing SSS, it’s too difficult, disappointed in self if fail. Sign of weakness | Education Modelling Persuasion Incentivization | 5.6 Information about emotional consequences 10.5 Social reward 11.2 Reduce negative emotions 5.2 Salience of consequences 13.2 Framing/reframing | |||
| BCT # | BCT Label | BCT Definition | Examples of How this Is Represented in the App |
|---|---|---|---|
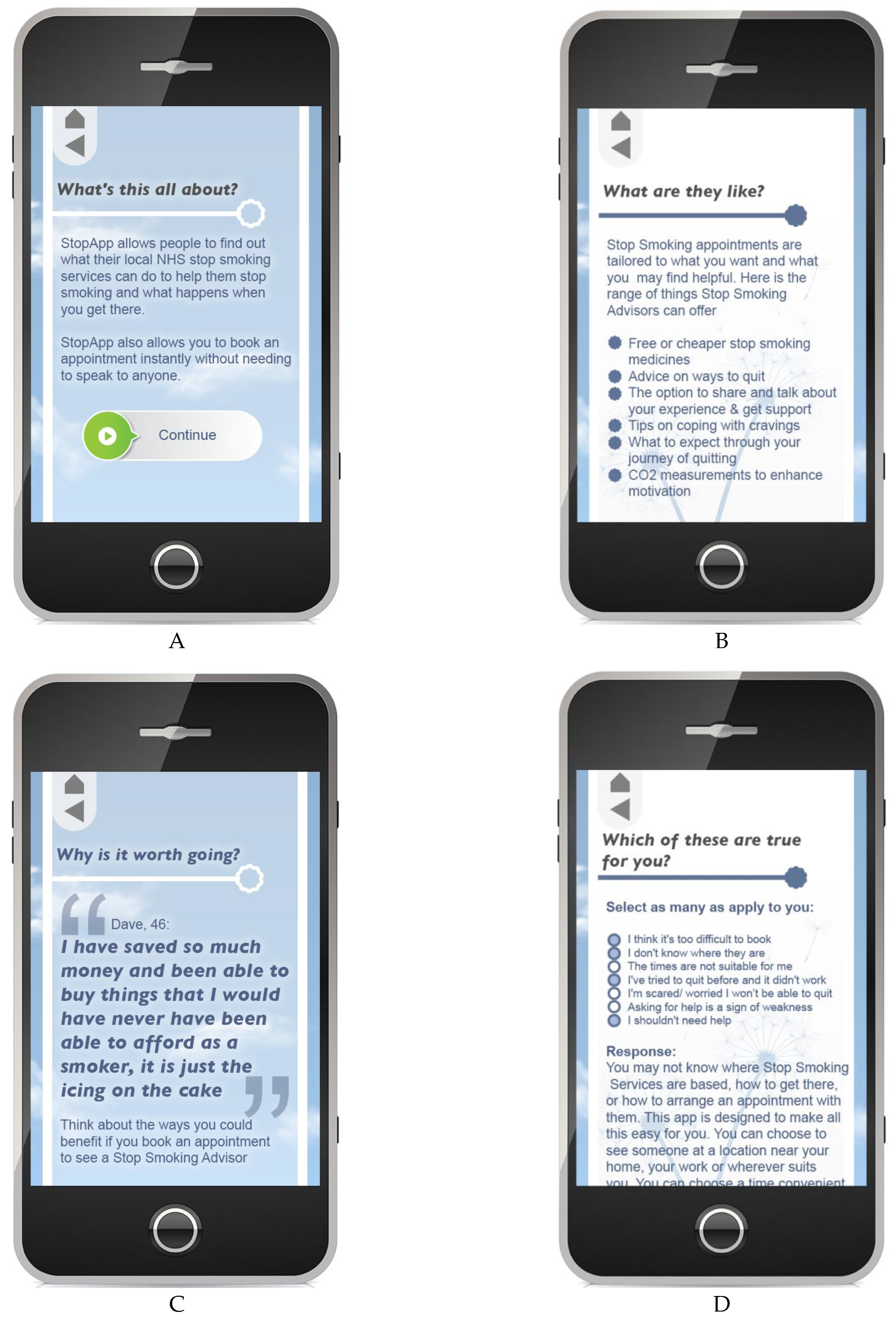
| 2 | 4.1 Instruction on how to perform the behaviour | Advise or agree on how to perform the behaviour (includes ‘Skills training’) | Instructions in the app about how to find a service near home or work, how to then choose a date/time, and how to book. Information on how to attend (location, how to get there, etc.) (presented in Figure 3D) |
| 9 | 6.2 Social comparison | Draw attention to others’ performance to allow comparison with the person’s own performance | Stories from peers about success at SSS, not being judged, given right support, offered more than could do alone. |
| 11 | 7.1 Prompts/cues | Introduce or define environmental or social stimulus with the purpose of prompting or cueing the behaviour | Information about and provision of text reminders to attend appt. Option of support to make a plan to help people to get there |
| 13 | 9.3 Comparative imagining of future outcomes | Prompt or advise the imagining and comparing of future outcomes of changed versus unchanged behaviour | Positive stories from peers about life after smoking with prompt to consider own future outcomes (see Figure 3C) |
| 14 | 10.1 Material incentive | Inform that money, vouchers, or other valued objects will be delivered if and only if there has been effort and/or progress in performing the behaviour | Give the message that they can get free NRT from SSS (see Figure 3A). |
| 15 | 13.2 Framing/Re-framing | Suggest the deliberate adoption of a new perspective on behaviour (e.g., its purpose) in order to change cognitions or emotions about performing the behaviour | Stopping smoking is hard; even if do not want emotional support, SSS may provide NRT or practical ideas. Address belief that it is difficult/not practical to go—actually easy to book and access (partly addressed in Figure 3A,D) |
| 18 | 15.3 Focus on past success | Advise thinking about or listing previous successes in performing the behaviour (or parts of it) | The message that stopping smoking for any period is a success. Even applicable to periods of not smoking that are unintentional (e.g., long-haul flight). Each attempt is one step closer. Can learn a lot from previous attempts to quit that will help with stopping for good |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fulton, E.A.; Brown, K.E.; Kwah, K.L.; Wild, S. StopApp: Using the Behaviour Change Wheel to Develop an App to Increase Uptake and Attendance at NHS Stop Smoking Services. Healthcare 2016, 4, 31. https://doi.org/10.3390/healthcare4020031
Fulton EA, Brown KE, Kwah KL, Wild S. StopApp: Using the Behaviour Change Wheel to Develop an App to Increase Uptake and Attendance at NHS Stop Smoking Services. Healthcare. 2016; 4(2):31. https://doi.org/10.3390/healthcare4020031
Chicago/Turabian StyleFulton, Emily Anne, Katherine E. Brown, Kayleigh L. Kwah, and Sue Wild. 2016. "StopApp: Using the Behaviour Change Wheel to Develop an App to Increase Uptake and Attendance at NHS Stop Smoking Services" Healthcare 4, no. 2: 31. https://doi.org/10.3390/healthcare4020031
APA StyleFulton, E. A., Brown, K. E., Kwah, K. L., & Wild, S. (2016). StopApp: Using the Behaviour Change Wheel to Develop an App to Increase Uptake and Attendance at NHS Stop Smoking Services. Healthcare, 4(2), 31. https://doi.org/10.3390/healthcare4020031