
Steps towards Smarter Solutions in Optometry and Ophthalmology—Inter-Device Agreement of Subjective Methods to Assess the Refractive Errors of the Eye


Abstract
:1. Background
2. Methods
2.1. Subjects
2.2. Equipment
2.3. Experimental Procedures
2.4. Analysis
2.5. Statistics
3. Results
3.1. Descriptive Statistics
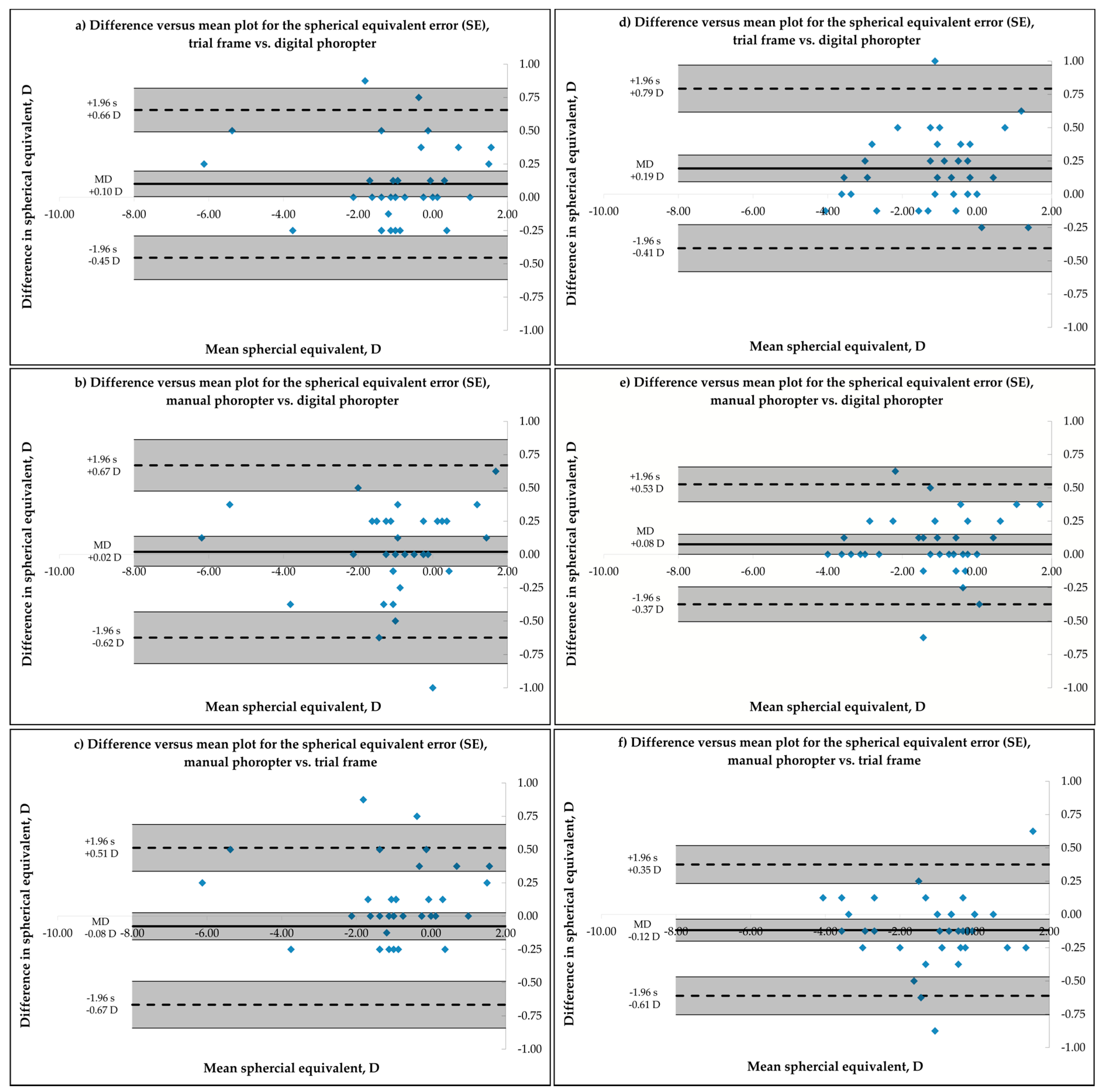
3.2. Bland-Altman Analysis for Inter-Device Agreement
3.3. Intra Class Correlation Analysis
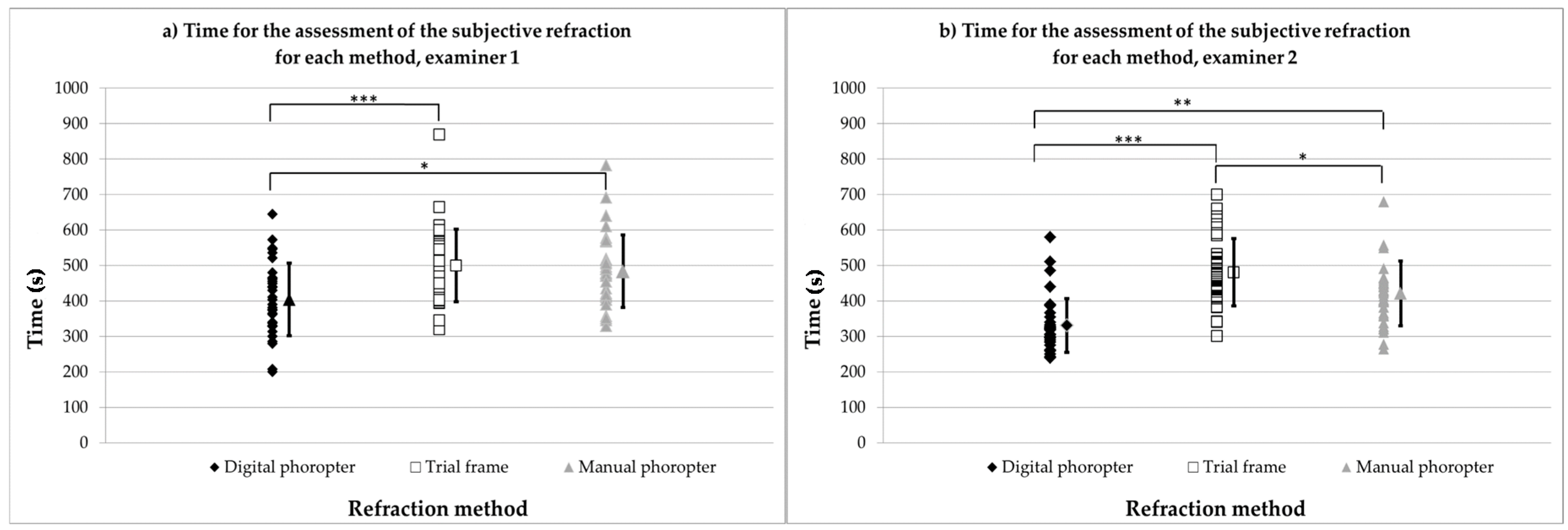
3.4. Time to Assess Subjective Refraction under Binocular Conditions
4. Discussion
4.1. Bland-Altman Analysis for Inter-Device Agreement
4.2. Intra Class Correlation Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Naidoo, K.S.; Leasher, J.; Bourne, R.R.; Flaxman, S.R.; Jonas, J.B.; Keeffe, J.; Limburg, H.; Pesudovs, K.; Price, H.; White, R.A.; et al. Global vision impairment and blindness due to uncorrected refractive error, 1990–2010. Ophthalmol. Vis. Sci. 2016, 93, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Vitale, S.; Ellwein, L.; Cotch, M.F.; Ferris, F.L.; Sperduto, R. Prevalence of refractive error in the United States, 1999–2004. Arch. Ophthalmol. 2008, 126, 1111–1119. [Google Scholar] [CrossRef] [PubMed]
- Solaka, N.; Modi, R.; Gaiser, H.; Pamplona, V.; Schafran, D.; He, R.; Moore, B.D. Comparison of a New Prototype of Netra-G Cell Phone-Based Refraction with Subjective Refraction. Available online: http://iovs.arvojournals.org/article.aspx?articleid=2268075 (accessed on 24 March 2016).
- Gaiser, H.; Moore, B.; Pamplona, V.; Solaka, N.; Schafran, D.; Merrill, D.; Sharpe, N.; Geringer, J.; Raskar, R. Comparison of a Novel Cell Phone-Based Refraction Technique (Netra-G) with Subjective Refraction. Available online: http://iovs.arvojournals.org/article.aspx?articleid=2147023 (accessed on 24 March 2016).
- Bastawrous, A.; Leak, C.; Howard, F.; Kumar, V. Validation of near eye tool for refractive assessment (NETRA)—Pilot study. J. Mob. Technol. Med. 2012, 1, 6–16. [Google Scholar] [CrossRef]
- Ciuffreda, K.J.; Rosenfield, M. Evaluation of the SVOne: A handheld, smartphone-based autorefractor. Optom. Vis. Sci. 2015, 92, 1133–1139. [Google Scholar] [CrossRef] [PubMed]
- Opternative. Eye Exams from Home. Available online: https://www.opternative.com/ (accessed on 24 March 2016).
- EyeNetra Inc. NETRA—Refraction for Anyone Anywere. Available online: https://eyenetra.com/product-netra.html (accessed on 11 May 2016).
- Elliott, M.; Simpson, T.; Richter, D.; Fonn, D. Repeatability and accuracy of automated refraction: A comparison of the Nikon NRK-8000, the Nidek AR-1000, and subjective refraction. Optom. Vis. Sci. 1997, 74, 434–438. [Google Scholar] [CrossRef] [PubMed]
- Zadnik, K.; Mutti, D.O.; Adams, A.J. The repeatability of measurement of the ocular components. Investig. Ophthalmol. Vis. Sci. 1992, 33, 2325–2333. [Google Scholar]
- Sheedy, J.; Schanz, P.; Bullimore, M. Evaluation of an automated subjective refractor. Optom. Vis. Sci. 2004, 81, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Rosenfield, M.; Chiu, N.N. Repeatability of subjective and objective refraction. Optom. Vis. Sci. 1995, 72, 577–579. [Google Scholar] [CrossRef] [PubMed]
- Goss, D.A.; Grosvenor, T. Reliability of refraction—A literature review. J. Am. Optom. Assoc. 1996, 67, 619–630. [Google Scholar] [PubMed]
- Thibos, L.N.; Wheeler, W.; Horner, D. Power vectors: An application of fourier analysis to the description and statistical analysis of refractive error. Optom. Vis. Sci. 1997, 74, 367–375. [Google Scholar] [CrossRef] [PubMed]
- McAlinden, C.; Khadka, J.; Pesudovs, K. Statistical methods for conducting agreement (comparison of Clinical Tests) and precision (repeatability or Reproducibility) Studies in optometry and ophthalmology. Ophthalmic Physiol. Opt. 2011, 31, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Measurement error and correlation coefficients. BMJ 1996, 313, 41–42. [Google Scholar] [CrossRef] [PubMed]
- Bullimore, M.A.; Fusaro, R.E.; Adams, C.W. The repeatability of automated and clinician refraction. Optom. Vis. Sci. 1998, 75, 617–622. [Google Scholar] [CrossRef] [PubMed]
- Grein, H.-J.; Schmidt, O.; Ritsche, A. Reproducibility of subjective refraction measurement. Ophthalmologe 2014, 111, 1057–1064. [Google Scholar] [CrossRef] [PubMed]
- Collins, M.; Shaw, A.; Menkens, E.; Davis, B.; Franklin, R. The Effect of Pupil Size on Subjective Refraction with Irregular Corneas. Available online: http://iovs.arvojournals.org/article.aspx?articleid=2419314 (accessed on 11 May 2016).
- DeCarlo, D.K.; McGwin, G.; Searcey, K.; Gao, L.; Snow, M.; Waterbor, J.; Owsley, C. Trial frame refraction versus autorefraction among new patients in a low-vision clinic. Investig. Ophthalmol. Vis. Sci. 2013, 54, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Segura, F.; Sanchez-Cano, A.; Lopez de la Fuente, C.; Fuentes-Broto, L.; Pinilla, I. Evaluation of patient visual comfort and repeatability of refractive values in non-presbyopic healthy eyes. Int. J. Ophthalmol. 2015, 8, 1031–1036. [Google Scholar] [PubMed]
- Pujol, J.; Ondategui-Parra, J.C.; Badiella, L.; Otero, C.; Vilaseca, M.; Aldaba, M. Spherical subjective refraction with a novel 3D virtual reality based system. J. Optom. 2016. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Examiner 1 for n = 36 Subjects | Examiner 2 for n = 38 Subjects | ||||||
|---|---|---|---|---|---|---|---|
| Mean Value (D) | ±1 Standard Deviation (D) | ±1 Standard Error (D) | Mean Value (D) | ±1 Standard Deviation (D) | ±1 Standard Error (D) | ||
| trial frame | SE | −0.92 | 1.57 | 0.26 | −1.07 | 1.38 | 0.22 |
| J0 | 0.01 | 0.31 | 0.05 | 0.03 | 0.35 | 0.06 | |
| J45 | 0.00 | 0.21 | 0.04 | 0.02 | 0.22 | 0.04 | |
| manual phoropter | SE | −0.99 | 1.59 | 0.27 | −1.17 | 1.38 | 0.22 |
| J0 | 0.02 | 0.34 | 0.06 | 0.00 | 0.36 | 0.06 | |
| J45 | −0.01 | 0.20 | 0.03 | 0.00 | 0.26 | 0.04 | |
| digital phoropter | SE | −1.02 | 1.57 | 0.26 | −1.24 | 1.36 | 0.22 |
| J0 | 0.01 | 0.32 | 0.05 | 0.02 | 0.36 | 0.06 | |
| J45 | 0.01 | 0.20 | 0.03 | 0.00 | 0.24 | 0.04 | |
| Examiner 1 (n = 36) | |||||
| Mean Difference (D) | 95% Limit of Agreement (D) | 95% CI for Upper Limit (D) | 95% CI for Lower Limit (D) | ||
| trial frame vs. digital phoropter | SE | 0.10 | ± 0.56 | 0.49 to 0.82 | −0.29 to −0.62 |
| J0 | 0.00 | ± 0.14 | 0.11 to 019 | −0.10 to −0.18 | |
| J45 | −0.01 | ± 0.14 | 0.09 to 0.17 | −0.11 to −0.19 | |
| manual phoropter vs. digital phoropter | SE | 0.06 | ± 0.65 | 0.63 to 1.01 | −0.43 to −0.82 |
| J0 | 0.01 | ± 0.21 | 0.16 to 0.29 | −0.14 to −0.27 | |
| J45 | −0.02 | ± 0.18 | 0.11 to 0.22 | −0.14 to −0.25 | |
| manual phoropter vs. trial frame | SE | −0.04 | ± 0.59 | 0.56 to 0.91 | −0.64 to −0.99 |
| J0 | 0.01 | ± 0.19 | 0.14 to 0.26 | −0.12 to −0.24 | |
| J45 | −0.01 | ± 0.15 | 0.10 to 0.19 | −0.11 to −0.20 | |
| Examiner 2 (n = 38) | |||||
| Mean Difference (D) | 95% Limit of Agreement (D) | 95% CI for Upper Limit (D) | 95% CI for Lower Limit (D) | ||
| trial frame vs. digital phoropter | SE | 0.19 | ± 0.60 | 0.62 to 0.97 | −0.23 to −0.58 |
| J0 | 0.00 | ± 0.20 | 0.14 to 0.25 | −0.14 to −0.25 | |
| J45 | 0.01 | ± 0.18 | 0.14 to 0.24 | −0.11 to −0.21 | |
| manual phoropter vs. digital phoropter | SE | 0.08 | ± 0.45 | 0.40 to 0.66 | −0.24 to −0.51 |
| J0 | −0.02 | ± 0.16 | 0.10 to 0.19 | −0.14 to −0.23 | |
| J45 | 0.00 | ± 0.17 | 0.11 to 0.22 | −0.12 to −0.22 | |
| manual phoropter vs. trial frame | SE | −0.12 | ± 0.49 | 0.23 to 0.52 | −0.47 to −0.75 |
| J0 | −0.02 | ± 0.22 | 0.13 to 0.26 | −0.18 to −0.30 | |
| J45 | −0.02 | ± 0.18 | 0.11 to 0.21 | −0.15 to 0.25 | |
| Examiner 1 (n = 36) | |||||
| ICC | 95% CI | p | |||
| Lower | Lower | ||||
| trial frame vs. digital phoropter | SE | 0.992 | 0.984 | 0.996 | <0.01 |
| J0 | 0.985 | 0.97 | 0.992 | <0.01 | |
| J45 | 0.965 | 0.932 | 0.982 | <0.01 | |
| manual phoropter vs. digital phoropter | SE | 0.989 | 0.978 | 0.994 | <0.01 |
| J0 | 0.967 | 0.935 | 0.963 | <0.01 | |
| J45 | 0.932 | 0.866 | 0.965 | <0.01 | |
| manual phoropter vs. trial frame | SE | 0.991 | 0.982 | 0.995 | <0.01 |
| J0 | 0.974 | 0.949 | 0.987 | <0.01 | |
| J45 | 0.958 | 0.917 | 0.978 | <0.01 | |
| Examiner 2 (n = 38) | |||||
| ICC | 95% CI | p | |||
| Lower | Lower | ||||
| trial frame vs. digital phoropter | SE | 0.987 | 0.975 | 0.993 | <0.01 |
| J0 | 0.978 | 0.958 | 0.989 | <0.01 | |
| J45 | 0.953 | 0.91 | 0.976 | <0.01 | |
| manual phoropter vs. digital phoropter | SE | 0.993 | 0.986 | 0.996 | <0.01 |
| J0 | 0.985 | 0.971 | 0.992 | <0.01 | |
| J45 | 0.963 | 0.928 | 0.981 | <0.01 | |
| manual phoropter vs. trial frame | SE | 0.991 | 0.84 | 0.996 | <0.01 |
| J0 | 0.971 | 0.944 | 0.985 | <0.01 | |
| J45 | 0.953 | 0.909 | 0.975 | <0.01 | |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ohlendorf, A.; Leube, A.; Wahl, S. Steps towards Smarter Solutions in Optometry and Ophthalmology—Inter-Device Agreement of Subjective Methods to Assess the Refractive Errors of the Eye. Healthcare 2016, 4, 41. https://doi.org/10.3390/healthcare4030041
Ohlendorf A, Leube A, Wahl S. Steps towards Smarter Solutions in Optometry and Ophthalmology—Inter-Device Agreement of Subjective Methods to Assess the Refractive Errors of the Eye. Healthcare. 2016; 4(3):41. https://doi.org/10.3390/healthcare4030041
Chicago/Turabian StyleOhlendorf, Arne, Alexander Leube, and Siegfried Wahl. 2016. "Steps towards Smarter Solutions in Optometry and Ophthalmology—Inter-Device Agreement of Subjective Methods to Assess the Refractive Errors of the Eye" Healthcare 4, no. 3: 41. https://doi.org/10.3390/healthcare4030041
APA StyleOhlendorf, A., Leube, A., & Wahl, S. (2016). Steps towards Smarter Solutions in Optometry and Ophthalmology—Inter-Device Agreement of Subjective Methods to Assess the Refractive Errors of the Eye. Healthcare, 4(3), 41. https://doi.org/10.3390/healthcare4030041