
Early Workplace Intervention to Improve the Work Ability of Employees with Musculoskeletal Disorders in a German University Hospital—Results of a Pilot Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Intervention
2.4. Data Collection and Measurements
2.5. Statistical Analyzes
3. Results
3.1. Sample Description
3.2. Participation and Satisfaction with the Worksite Intervention
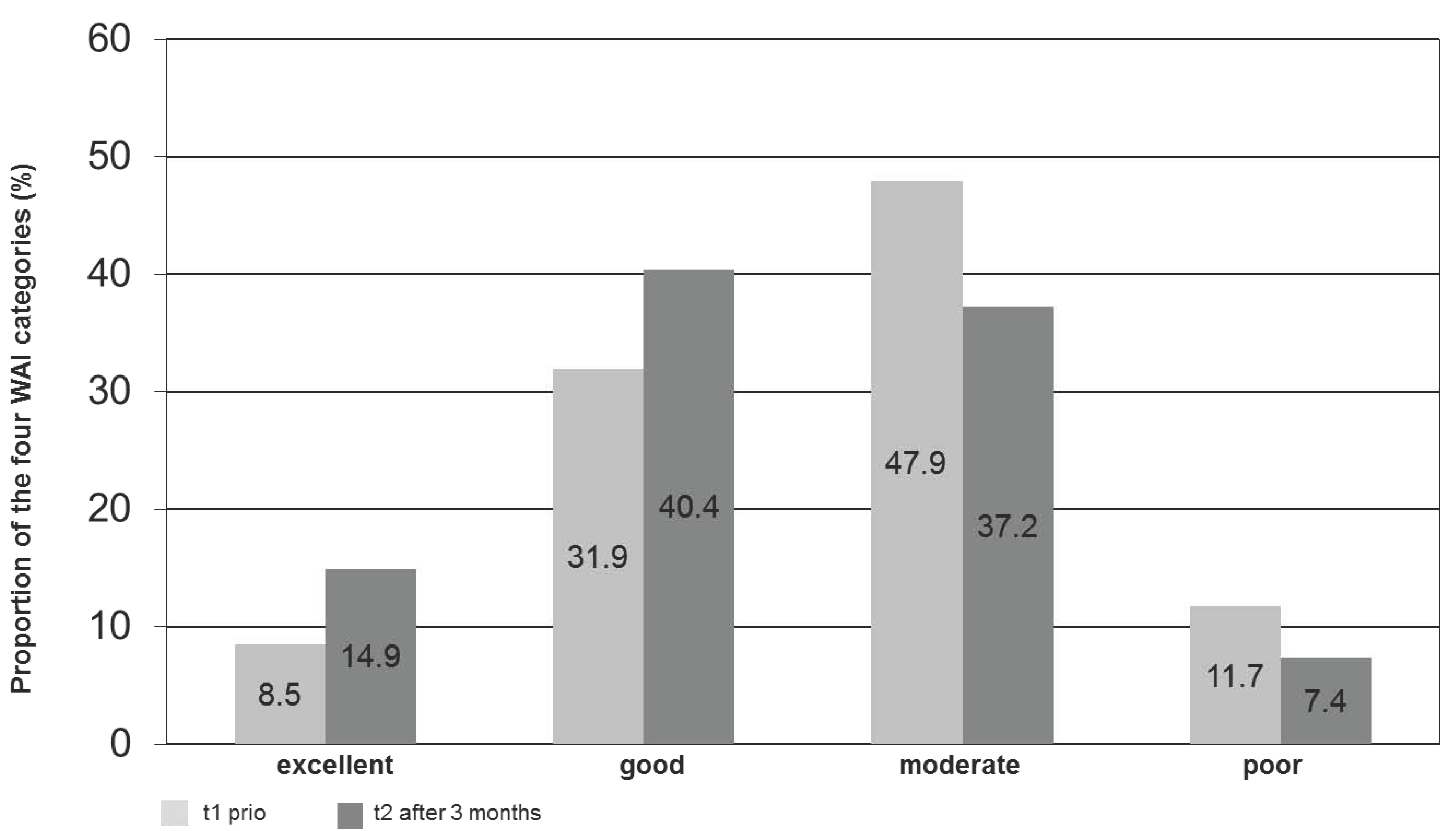
3.3. Workability, Prognosis of Gainful Employment and Sickness Absence
4. Discussion
4.1. Implementation
4.2. Need-Based Approach
4.3. Outcome
4.4. Strengths and Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| MSD | Musculoskeletal Disorders |
| RP | Rehabilitation Physician |
| CP | Company Physician |
| SPE-Scale | Subjective prognosis of gainful employment |
| WAI | Work Ability Index |
| WMR | Work-Related Medical Rehabilitation |
| WHP | Work Health Program |
| GDP | Gross Domestic Product |
| SES | Standardized Effect Size |
References
- Schulz, E.; Leidl, R.; König, H. The impact of ageing on hospital care and long-term care—The example of Germany. Health Policy 2004, 67, 57–74. [Google Scholar] [CrossRef]
- Szinovacz, M.E. Introduction: The aging workforce: Challenges for societies, employers, and older workers. J. Aging Soc. Policy 2011, 23, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Fehr, H.; Kallweit, M.; Kindermann, F. Pension reform with variable retirement age: A simulation analysis for Germany. J. Pension Econ. Finance 2012, 11, 389–417. [Google Scholar] [CrossRef]
- Bhattacharya, J.; Choudhry, K.; Lakdawalla, D. Chronic disease and severe disability among working-age populations. Med. Care 2008, 46, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Müller, A.; Weigl, M.; Heiden, B.; Glaser, J.; Angerer, P. Promoting work ability and well-being in hospital nursing: The interplay of age, job control, and successful ageing strategies. Work 2012, 41, 5137–5144. [Google Scholar] [PubMed]
- Scheidt-Nave, C. Chronische Erkrankungen—Epidemiologische Entwicklung und die Bedeutung für die öffentliche Gesundheit. Public Health Forum 2010, 18, 2–4. (In German) [Google Scholar] [CrossRef]
- Badura, B.; Ducki, A.; Schröder, H.; Klose, J.; Meyer, M. Fehlzeiten-Report 2014: Erfolgreiche Unternehmen von Morgen-Gesunde Zukunft Heute Gestalten; Springer: Berlin, Germany, 2014. (In German) [Google Scholar]
- Shaw, W.S.; Hartvigsen, J.; Woiszwillo, M.J.; Linton, S.J.; Reme, S.E. Psychological distress in acute low back pain: A review of measurement scales and levels of distress reported in the first two months after pain onset. Arch. Phys. Med. Rehabil. 2016. [Google Scholar] [CrossRef] [PubMed]
- Bevan, S. Economic impact of musculoskeletal disorders (MSDs) on work in Europe. Best Pract. Res. Clin. Rheumatol. 2015, 29, 356–373. [Google Scholar] [CrossRef] [PubMed]
- Tullar, J.M.; Brewer, S.; Amick, B.C., III; Irvin, E.; Mahood, Q.; Pompeii, L.A.; Wang, A.; Van Eerd, D.; Gimeno, D.; Evanoff, B. Occupational safety and health interventions to reduce musculoskeletal symptoms in the health care sector. J. Occup. Rehabil. 2010, 20, 199–219. [Google Scholar] [CrossRef] [PubMed]
- Caruso, C.C.; Waters, T.R. A review of work schedule issues and musculoskeletal disorders with an emphasis on the healthcare sector. Ind. Health 2008, 46, 523–534. [Google Scholar] [CrossRef] [PubMed]
- Hüther, M.; Naegele, G. Demografiepolitik und Demografiestrategie—Was notwendig ist. In Demografiepolitik; Springer: Berlin, Germany, 2013; pp. 365–378. (In German) [Google Scholar]
- Schmidt, C.; Bauer, J.; Schmidt, K.; Bauer, M. Betriebliches Gesundheitsmanagement im Krankenhaus: Strukturen, Prozesse und das Arbeiten im Team gesundheitsfördernd Gestalten; MWV: Berlin, Germany, 2015. (In German) [Google Scholar]
- Palmer, K.T.; Harris, E.C.; Linaker, C.; Barker, M.; Lawrence, W.; Cooper, C.; Coggon, D. Effectiveness of community- and workplace-based interventions to manage musculoskeletal-related sickness absence and job loss: A systematic review. Rheumatology (Oxford) 2012, 51, 230–242. [Google Scholar] [CrossRef] [PubMed]
- Arnetz, B.B.; Sjögren, B.; Rydéhn, B.; Meisel, R. Early workplace intervention for employees with musculoskeletal-related absenteeism: A prospective controlled intervention study. J. Occup. Environ. Med. 2003, 45, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Meffert, C.; Mittag, O.; Jackel, W.H. Work place health promotion programmes of the statutory German Pension Insurance. Rehabilitation (Stuttg) 2013, 52, 391–398. [Google Scholar] [PubMed]
- Van Oostrom, S.H.; Driessen, M.T.; De Vet, H.; Franche, R.; Schonstein, E.; Loisel, P.; van Mechelen, W.; Anema, J.R. Workplace interventions for preventing work disability. Cochrane Database Syst. Rev. 2009. [Google Scholar] [CrossRef]
- Schaafsma, F.G.; Whelan, K.; van der Beek, A.J.; van der Es-Lambeek, L.C.; Ojajärvi, A.; Verbeek, J.H. Physical conditioning as part of a return to work strategy to reduce sickness absence for workers with back pain. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef]
- Waddell, G.; Burton, A.K.; Kendall, N.A. Vocational Rehabilitation—What Works, for Whom, and When? (Report for the Vocational Rehabilitation Task Group); TSO: London, UK, 2008. [Google Scholar]
- Wåhlin, C.; Ekberg, K.; Persson, J.; Bernfort, L.; Öberg, B. Evaluation of self-reported work ability and usefulness of interventions among sick-listed patients. J. Occup. Rehabil. 2013, 23, 32–43. [Google Scholar] [CrossRef] [PubMed]
- Schonstein, E.; Kenny, D.T.; Keating, J.L.; Koes, B.W. Work conditioning, work hardening and functional restoration for workers with back and neck pain. Cochrane Database Syst. Rev. 2003. [Google Scholar] [CrossRef]
- Egner, U.; Schliehe, F.; Streibelt, M. Work related medical rehabilitation, MBOR—A process model in medical rehabilitation. Rehabilitation (Stuttg) 2011, 50, 143–144. [Google Scholar] [CrossRef] [PubMed]
- Bethge, M.; Löffler, S.; Schwarz, B.; Vogel, H.; Schwarze, M.; Neuderth, S. Gelingt die Umsetzung des Anforderungsprofils zur Durchführung der medizinisch-beruflich orientierten Rehabilitation? Rehabilitation 2013, 53, 184–190. (In German) [Google Scholar] [CrossRef] [PubMed]
- Bethge, M.; Löffler, S.; Schwarz, B.; Vogel, H.; Schwarze, M.; Neuderth, S. Besondere berufliche Problemlagen: Spielen sie eine Rolle beim Zugang in die medizinisch-beruflich orientierte Rehabilitation? Rehabilitation 2014, 53, 49–55. (In German) [Google Scholar] [CrossRef] [PubMed]
- Buschmann-Steinhage, R.; Brüggemann, S. Veränderungstrends in der medizinischen Rehabilitation der gesetzlichen Rentenversicherung. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2011, 54, 404–410. (In German) [Google Scholar] [CrossRef] [PubMed]
- Hillert, A.; Müller-Fahrnow, W.; Radoschewski, F. Medizinisch-beruflich orientierte Rehabilitation. In Grundlagen und Klinische Praxis Köln; Deutscher Ärzte-Verlag: Berlin, Germany, 2009. (In German) [Google Scholar]
- Gerdau-Heitmann, C.; Gutenbrunner, C.; Miede, J.; Schwarze, M. Umsetzung des Erwerbsbezugs in der medizinischen Rehabilitation-Analyse von Routinedaten der Deutschen Rentenversicherung Braunschweig-Hannover. Phys. Med. Rehabil. Kurortmed. 2014. (In German) [Google Scholar] [CrossRef]
- Tuomi, K.; Ilmarinen, J.; Jahkola, A.; Katajarinne, L.; Tulkki, A. Work Ability Index, 2nd ed.; Finnish Institute of Occupational Health: Helsinki, Finland, 1998. [Google Scholar]
- Ilmarinen, J. The ageing workforce—Challenges for occupational health. Occup. Med. (Lond.) 2006, 56, 362–364. [Google Scholar] [CrossRef] [PubMed]
- Ilmarinen, J. Promoting Active Ageing in the Workplace; European Agency for Safety and Health at Work: Bilbao, Spain, 2012. [Google Scholar]
- Amler, N.; Felder, S.; Mau, W.; Merkesdal, S.; Schöffski, O. Instrumente zur Messung von Effekten einer Frühintervention auf den Erhalt bzw. die Wiederherstellung der Arbeitsfähigkeit in Deutschland—Stellungnahme einer interdisziplinären Arbeitsgruppe. Das Gesundheitswesen 2015. (In German) [Google Scholar] [CrossRef] [PubMed]
- Gutenbrunner, C.; Schwarze, M. JobReha-bedarfsgerechte arbeitsplatzbezogene Rehabilitation: Systematische Modellentwicklung. Phys. Med. Rehabil. Kurortmed. 2011, 21, 234–241. (In German) [Google Scholar] [CrossRef]
- Teumer, F.; Wassmus, A.; Cyganski, L.; Teichler, N.; Gutenbrunner, C.; Schwarze, M. Gesundheitsökonomische Evaluation der JobReha bei Volkswagen Nutzfahrzeuge Hannover. ASUpraxis Arbeitsmed. Sozialmed. Umweltmed. 2010, 45, 102–104. [Google Scholar]
- Neugebauer, T.; Bethge, M.; Egen, C.; Burzlaff, P.; Schriek, S.; Miede, J.; Gutenbrunner, C.; Schwarze, M. Evaluation einer arbeitsplatzorientierten Maßnahme nach dem Modell der JobReha für MitarbeiterInnen einer Universitätsklinik. DRV Schriften 2013, 101, 318–319. (In German) [Google Scholar]
- Schwarze, M.; Spallek, M.; Korallus, C.; Manecke, I.; Teumer, F.; Wrbitzky, R.; Gutenbrunner, C.; Rebe, T. Advantages of the JobReha discharge letter: An instrument for improving the communication interface in occupational rehabilitation. Int. Arch. Occup. Environ. Health 2013, 86, 699–708. [Google Scholar] [CrossRef] [PubMed]
- Oesch, P.; Meyer, K.; Jansen, B.; Kool, J. Functional Capacity Evaluation: Performance of patients with chronic non-specific low back pain without waddell signs. J. Occup. Rehabil. 2015, 25, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Isernhagen, S.J. Functional capacity evaluation: Rationale, procedure, utility of the kinesiophysical approach. J. Occup. Rehabil. 1992, 2, 157–168. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, J.; Lamprecht, F.; Wittmann, W. Zufriedenheit mit der stationären Versorgung. Entwicklung eines Fragebogens und erste Validitätsuntersuchungen. Psychother. Med. Psychol. 1989, 39, 248–255. (In German) [Google Scholar]
- Jedryka-Góral, A.; Bugajska, J.; Łastowiecka, E.; Najmiec, A.; Rell-Bakalarska, M.; Bownik, I.; Michalak, J.M.; Kochmański, M. Work ability in ageing workers suffering from chronic diseases. Int. J. Occup. Saf. Ergon. 2006, 12, 17–30. [Google Scholar] [CrossRef] [PubMed]
- Mittag, O.; Glaser-Moller, N.; Ekkernkamp, M.; Matthis, C.; Heon-Klin, V.; Raspe, A.; Raspe, H. Predictive validity of a brief scale measuring the subjective prognosis of gainful employment (SPE-scale) in a cohort of blue collar workers with low back pain or functional syndroms of Internal Medicine. Soz.-Präventivmed. 2003, 48, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Goetzel, R.Z.; Ozminkowski, R.J. The health and cost benefits of work site health-promotion programs. Annu. Rev. Public Health 2008, 29, 303–323. [Google Scholar] [CrossRef] [PubMed]
- Koppelaar, E.; Knibbe, J.J.; Miedema, H.S.; Burdorf, A. Determinants of implementation of primary preventive interventions on patient handling in healthcare: A systematic review. Occup. Environ. Med. 2009, 66, 353–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Völter-Mahlknecht, S.F.; Rieger, M.A. Patientenversorgung an der Schnittstelle von Rehabilitation und Betriebsärzten. Systematische Literaturübersicht zur Versorgungsgestaltung. Dtsch. Med. Wochenschr. 2014, 139, 1609–1614. (In German) [Google Scholar] [PubMed]
- Olbrich, D.; Beblo, A.; Passeik-Hartmann, D. Zur Bedeutung des Work Ability Index (WAI) im GUSI-Präventionsprogramm für Versicherte der Deutschen Rentenversicherung Bund und Westfalen. Available online: http://www.bsafb.de/fileadmin/downloads/pa_21_12_2010/pa21_12_2010_zur_bedeutung_des_WAI_im_GUSI_Praeventionsprogramm_fuer_versicherte_der_DRV_bund_und_westfalen.pdf (accessed on 31 August 2016).
- Reeuwijk, K.G.; Robroek, S.J.; Niessen, M.A.; Kraaijenhagen, R.A.; Vergouwe, Y.; Burdorf, A. The prognostic value of the work ability index for sickness absence among office workers. PLoS ONE 2015, 10, e0126969. [Google Scholar] [CrossRef] [PubMed]
- Gutenbrunner, C.; Egen, C.; Kahl, K.; Briest, J.; Tegtbur, U.; Miede, J.; Born, M. Entwicklung und Implementierung eines umfassenden Gesundheitsmanagements (Fit for Work and Life) für Mitarbeiter/innen eines Universitätsklinikums–ein Praxisbericht. Das Gesundheitswesen 2015. (In German) [Google Scholar] [CrossRef] [PubMed]
- Van den Berg, T.I.; Elders, L.A.; de Zwart, B.C.; Burdorf, A. The effects of work-related and individual factors on the Work Ability Index: A systematic review. Occup. Environ. Med. 2009, 66, 211–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | n (%) |
|---|---|
| Gender | |
| Female | 70 (60.3) |
| Men | 46 (39.7) |
| Age | |
| Average (years, SD) | 47 8.3 |
| Groups (years) | |
| <46 | 46 (39.7) |
| 46–50 | 25 (29.0) |
| >50 | 41 (35.3) |
| Range (years max–min) | 63–20 |
| Occupational groups/divisions | |
| Blue-collar workers (logistics, transport, kitchen, laundry) | 69 (59.5) |
| White-collar workers (funding, finance, patient-accounting office) | 47 (40.5) |
| Working conditions | |
| Shift work | 26 (22.8) |
| Display screen work | 51 (44.7) |
| Physically demanding work (high load) | 34 (29.8) |
| Time pressure (high load) | 37 (32.5) |
| Work Ability Index (n = 94) | |
| Excellent (44–49) | 8 (8.5) |
| Good (37–43) | 30 (31.9) |
| Moderate (28–36) | 45 (47.9) |
| Poor (7–27) | 11 (11.7) |
| Prognosis of gainful employment (SPE-scale) (n = 97) | |
| No risk | 49 (50.5) |
| Low risk | 26 (26,8) |
| Strong risk | 19 (19.6) |
| Very strong risk | 3 (3.1) |
| Days of sick leave During six months prior to intervention (days) | 13.0 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schwarze, M.; Egen, C.; Gutenbrunner, C.; Schriek, S. Early Workplace Intervention to Improve the Work Ability of Employees with Musculoskeletal Disorders in a German University Hospital—Results of a Pilot Study. Healthcare 2016, 4, 64. https://doi.org/10.3390/healthcare4030064
Schwarze M, Egen C, Gutenbrunner C, Schriek S. Early Workplace Intervention to Improve the Work Ability of Employees with Musculoskeletal Disorders in a German University Hospital—Results of a Pilot Study. Healthcare. 2016; 4(3):64. https://doi.org/10.3390/healthcare4030064
Chicago/Turabian StyleSchwarze, Monika, Christoph Egen, Christoph Gutenbrunner, and Stephanie Schriek. 2016. "Early Workplace Intervention to Improve the Work Ability of Employees with Musculoskeletal Disorders in a German University Hospital—Results of a Pilot Study" Healthcare 4, no. 3: 64. https://doi.org/10.3390/healthcare4030064